01 November 2020 : Review article
Long-Term Respiratory and Neurological Sequelae of COVID-19
Fuzhou Wang1ABCDEF, Richard M. Kream2ABCDEF, George B. Stefano23ABCDEF*DOI: 10.12659/MSM.928996
Med Sci Monit 2020; 26:e928996






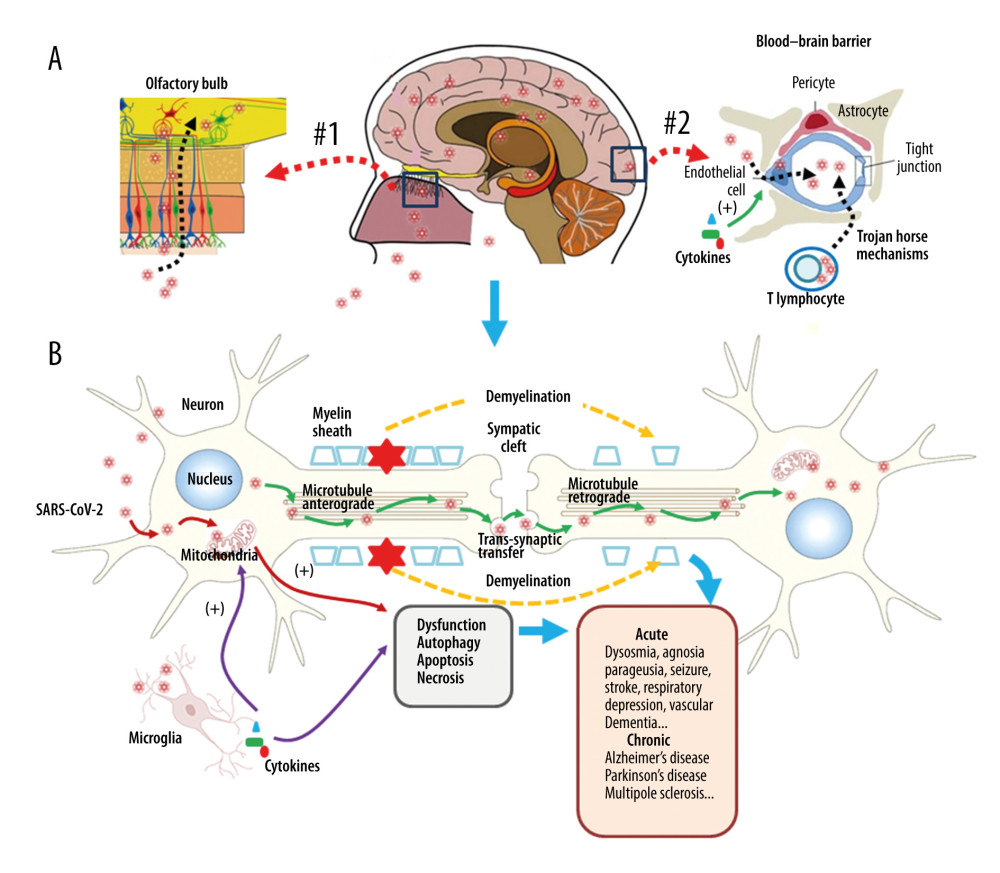
Figure 2 Neuronal injury associated with SARS-CoV-2 infection. SARS-CoV-2 enters into the central nervous system (CNS) through 2 major routes: the olfactory pathway (#1 in A), and the blood–brain barrier (BBB) pathway (#2 in A). The virus can migrate into the CNS directly by endocytosis with the assistance of inflammatory cytokine-induced increased vascular permeability and indirect transfer via a ‘Trojan horse’ mechanism. (B) After binding to its membrane receptor, ACE2, SARS-CoV-2 will be engulfed into neuronal cytosol and move to connect with cytosol-located angiotensin-converting enzyme 2 (ACE2). The viral RNAs enter the mitochondria or form into autophagolysosomes to initiate autophagy and/or apoptosis. Microglia and immune cells produce pro-inflammatory cytokines, which result in further abnormalities in mitochondrial function. When the virus enters the neurons, it combines with the axonal microtubules with anterograde and retrograde spread to the synapse and enters the next level of neurons by trans-synaptic transfer and endocytosis. Both the virus and the ‘cytokine storm’ can destroy the myelin sheath of neurons, resulting in acute and chronic neuropathology.