26 February 2022 : Review article
A Review of Current Clinical Concepts in the Pathophysiology, Etiology, Diagnosis, and Management of Hypercalcemia
Carolina Rodrigues Tonon1ABCDEF*, Taline Alisson Artemis Lazzarin Silva1ABCDEF, Filipe Welson Leal Pereira1ABDE, Diego Aparecido Rios Queiroz1ABDE, Edson Luiz Favero Junior1BD, Danilo MartinsDOI: 10.12659/MSM.935821
Med Sci Monit 2022; 28:e935821






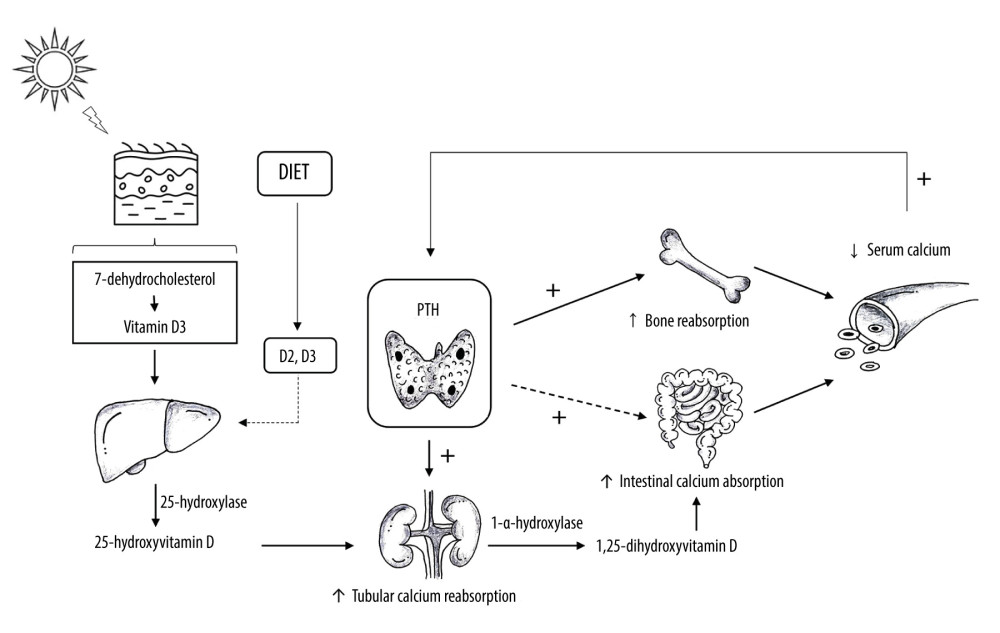
Figure 1 Calcium Homeostasis. Vitamin D is produced by the skin after exposure to ultraviolet B radiation and a small amount comes from diet. In the skin, vitamin D2 and D3 undergo hydroxylation in the liver by 25-hydroxylase, generating 25-hydroxyvitamin D (25[OH]D). In the kidneys, 1-α-hydroxylase converts 25[OH]D into 1,25-dihydroxyvitamin D (1,25[OH]2D). This form of vitamin D increases intestinal calcium absorption. Parathyroid hormone (PTH) is produced by the parathyroid glands. Decreased serum calcium concentration stimulates PTH release, which increases calcium bone absorption, renal calcium reabsorption, renal hydroxylation of 25[OH]D to 1,25[OH]2D, and, less importantly, intestinal calcium absorption. Created by the authors with Power Point, version 2013, manufactured by Microsoft.