23 August 2022: Meta-Analysis
Optimal Surgical Treatment Method for Anterior Cruciate Ligament Rupture: Results from a Network Meta-Analysis
Yudi Wu1CDEF, Yajia Li2BCD, Jia Guo2BC, Qianxiang Li34BC, Jianhuang Wu35BCD, Ziqin Cao5ABCDEF*, Yulin Song6ABCDEFDOI: 10.12659/MSM.937118
Med Sci Monit 2022; 28:e937118






Abstract
BACKGROUND: Previous studies have shown that primary repair (PR) and anterior cruciate ligament reconstruction (ACLR) can effectively treat ACL injuries. Our study aimed to compare different treatments of ACL tears, including autograft, allograft, hybrid graft ACLR, and PR, by assessing clinical outcomes and adverse events.
MATERIAL AND METHODS: PubMed, Cochrane Library, Embase, and CNKI databases were searched and a frequentist-framework network meta-analysis was used.
RESULTS: Overall, PR with augmentation was superior to ACLR only for activity recovery (WMD 0.28 95%CI [0.07 to 0.49]), and there was no significant difference shown between PR without augmentation and ACLR. ACLR with irradiated allograft was a poor option for the treatment of ACL rupture, showing the weakest subjective evaluations and functional outcomes and worst safety profile. PR with or without augmentation provided fairly good postoperative efficacy results and produced less postoperative knee laxity than irradiated allograft ACLR (PR: standardized mean difference [SMD] -1.27 [-1.80 to -0.74]; ACLR: SMD -1.36 [-1.88 to -0.83]). However, PR without augmentation showed a high failure rate compared with autograft ACLR (autograft vs PR without augmentation: risk ratio 0.29 [0.10 to 0.85]).
CONCLUSIONS: For surgical treatment of ACL rupture, irradiated allograft ACLR had the worst efficacy and safety and is not recommended. PR may be an ideal treatment method in terms of efficacy but it is related to a significantly higher revision risk if without augmentation. Autograft ACLR may be the preferred method currently available for most patients requiring surgical treatment of ACL rupture.
Keywords: Anterior Cruciate Ligament, Anterior Cruciate Ligament Injuries, anterior cruciate ligament reconstruction, autografts, Humans, Knee Joint, Network Meta-Analysis, Rupture
Background
Anterior cruciate ligament (ACL) injury is a common knee sports injury that often occurs during high-intensity physical exercise [1]. In addition, it is estimated that 1 in every 120 people of working age have ACL injuries [2]. The ACL is the main structure limiting the tibia’s anterior translation and internal rotation. In most cases, a tear or rupture is caused by excessive pivoting or anterior or valgus movement of the proximal tibia, rather than by direct contact [3].
Before the popularization of arthroscopy, the most common surgical option for treating ACL tears was open primary repair (PR). This provided good short-term outcomes but was associated with long-term problems, including high re-rupture and reoperation rates and postoperative complications [4–6]. These problems together with the development of ACL reconstruction (ACLR) led to a decline in the use of PR. However, with advances in arthroscopic technology, preoperative imaging, and surgical techniques, such as suture anchors and suture augmentation, PR is once again a viable option for ACL repair. More recent studies showed that compared with ACLR, PR had a comparable failure rate [7] and provided an earlier return of range of motion [8,9], most likely resulting from the less invasive nature of the surgery. It also has no donor site morbidity because of the lack of graft collection.
ACLR is regarded as the most accepted standard surgical therapy for active and symptomatic patients with ACL injury. There are 3 main approaches for ACLR based on graft type: autograft, allograft, and hybrid graft (combination of autograft and allograft) [10,11]. Autograft is the oldest and most common ACLR technique used because it has some unique advantages, such as the lowest rejection reaction and relatively high mechanical reliability [12]. In contrast, allograft ACLR causes no donor site morbidity but has a lower graft survival rate and a higher postoperative infection rate [3,13,14]. Hybrid graft ACLR provides a graft of suitable size, with clinical results comparable to that of autografts, and offers an alternative to autograft ACLR, especially for those patients whose tendons are damaged or undersized at harvest [15].
Despite several comparative studies, it is still unclear which is the best surgical method for ACL rupture. Previous meta-analyses have compared clinical outcomes of the different types of ACLR. The study by Li et al [16] showed the performance of the autograft and hybrid graft was similar in graft failure, graft diameter, and reoperation ratio. Meanwhile, the study by Sun et al [17] also revealed no difference in long-term outcomes and failure risk after cruciate ligament reconstruction with either autograft or synthetics; however, autografts were found to be inferior to synthetics in dealing with restoring knee joint stability and were associated with more complications. Several clinical trials have reported functional outcome scores and revision rates after PR [18–20]. However, there are few randomized controlled trials (RCTs) or systematic reviews that have compared the efficacy and safety of the various types of ACLR and PR.
In summary, we speculated that PR could also bring ideal therapeutic effects and potentially be superior to ACLR. This network meta-analysis was aimed to compare the clinical outcomes and adverse events of autograft, allograft, hybrid graft ACLR, and PR in the surgical treatment of ACL tears. This study was not focused on professional athletes.
Material and Methods
DATA SOURCES AND SEARCHES:
This study was registered in the PRESPERO (registration no. CRD42021225778). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Network Meta-analysis (PRISMA-NMA) guidelines [21] were strictly followed throughout this study. MeSH keywords combined with a free words retrieval strategy was adopted to search the PubMed/Medline, Cochrane Library, Embase, and CNKI databases from January 1995 to July 2022. The specific query for PubMed/Medline was as follows: ((anterior cruciate ligament injury) OR (anterior cruciate ligament injury) OR (anterior cruciate ligament rupture) OR (anterior cruciate ligament tear) OR (ACL injury) OR (ACL rupture) OR (ACL tear) AND (ACL[MeSH Terms]) OR (anterior cruciate ligament[MeSH Terms]) AND (reconstruction) OR (transplantation) OR (repair) OR (primary repair) OR (suture)). The specific query for Cochrane Library was as follows: “MeSH descriptor.[Anterior Cruciate Ligament Injuries] explode all trees” OR “MeSH descriptor.[Anterior Cruciate Ligament] explode all trees” OR “(ACL injury): ti,ab,kw OR (ACL rupture): ti,ab,kw OR (ACL tear): ti,ab,kw” OR “(anterior cruciate ligament injury): ti,ab,kw OR (anterior cruciate ligament rupture): ti,ab,kw OR (anterior cruciate ligament tear): ti,ab,kw” AND “(reconstruction): ti,ab,kw OR (transplatation);: ti,ab,kw OR (repair): t,ab,kw OR (suture): ti,ab,kw OR (primary suture): ti,ab,kw”. The specific query for Embase was as follows: ((“anterior cruciate ligament injury”: ti, ab, kw OR “anterior cruciate ligament rupture”: ti, ab, kw OR “anterior cruciate ligament tear”: ti, ab, kw OR “ACL injury”: ti, ab, kw OR “ACL rupture”: ti, ab, kw OR “ACL tear”: ti, ab, kw) AND (“reconstruction”: ti, ab, kw OR “transplantation”: ti, ab, kw OR “repair”: ti, ab, kw OR “primary repair”: ti, ab, kw OR “suture”: ti, ab, kw)). The specific query for CNKI was as follows [in Chinese]: ((主题: 前交叉韧带损伤 + 前交叉韧带断裂 + 前交叉韧带撕裂 (精确) OR (主题: 前交叉韧带重建 + 前交叉韧带移植 + 前交叉韧带修复 + 前交叉韧带缝合 (精确)). A reference lists of identified articles were further reviewed to find additional eligible studies. No language restriction was set for the publication selection.
STUDY SELECTION:
A research protocol under the PICO principle was pre-drafted as follows: (1) Population: patients underwent ACL rupture and planned surgery; (2) intervention: surgical treatment for ACL rupture; (3) comparison: different surgical methods for ACL rupture; and (4) outcomes: postoperative subjective feelings of patients, recovery of postoperative activity, functional improvement, joint laxity, and treatment failure.
Based on the PICO protocol, studies that fulfilled all of the following criteria were included: (1) Patients underwent ACLR or PR to treat ACL tears; (2) study compared 2 or more different surgery methods; (3) study used an RCT design, non-RCT design, or cohort design (CHS); and (4) the following outcomes were reported: subjective evaluation improvement, functional rehabilitation, improvement of activity, postoperative knee laxity, or the incidence of revision surgery.
The exclusion criteria were as follows: (1) The study included the revision of ACL rupture; (2) low-quality of study; (3) studies with a non-prospective design; and (4) animal or vitro basic studies, observational studies, reviews (including systematic review and meta-analyses), meeting abstracts, letters, and those with inaccessible original study data.
We would also try to contact the corresponding authors for the studies lacking complete information, and those for which no response was received were excluded. The source of data was also requested from the corresponding author for the studies presenting outcomes only in figures but not in numeric datasets, and when no response was received, 2 authors would independently try to obtain the data by the measurements shown in the figures. When there was still no access to the raw data after the above attempts, the study was excluded.
DATA EXTRACTION AND QUALITY ASSESSMENT:
The study quality was assessed by 2 authors independently. Quality of method and bias risk for RCTs was assessed by using the Cochrane risk bias assessment tools [22]. The Newcastle-Ottawa Scale (NOS) [23] was used for the evaluation of the method quality of CHSs and non-RCTs. Three main domains – the selection of the study groups, comparability among different groups, and ascertainment of either the exposure or outcome of interest – were evaluated with a score from 0 to 9. All disputes were resolved during a discussion between the 2 authors. The following information was extracted from each included study: first author, year of publication, number of participants, average age, sex ratio, traumatic mechanism, method of surgery, average follow-up time, study design, and outcome.
OUTCOME MEASURES:
For the evaluation and comparison of the efficacy and safety of the surgical methods, the following outcome measurements were selected: postoperative subjective feelings of patients, recovery of postoperative activity, functional improvement, and safety endpoints.
For measuring postoperative function status, no restriction was placed on the types of questionnaires used in functional evaluation. The Lequesne Index was the first choice, followed by other functional measurement scales, including the Knee Injury and Osteoarthritis Score (KOOS) and the Western Ontario and McMaster Universities Arthritis Index (WOMAC). The standardized mean difference (SMD) was used to incorporate these different scales into the same network.
By using the Subjective International Knee Documentation Committee (IKDC) score, postoperative subjective feelings were assessed. The recovery of postoperative activity was assessed with the Tenger score. The weighted mean difference (WMD) with 95% confidence intervals (CIs) was calculated for the IKDC and Tenger scores.
The safety endpoints were joint laxity and treatment failure. The degree of laxity was the relaxation difference comparing the operated knee with the non-operated knee measured by the KT-1000 or KT-2000 scale. The SMD with a 95%CI was calculated for the laxity scores. Failure was defined as all patients who had a re-tear or recurrent laxity, regardless of whether or not they underwent revision surgery. The risk ratio (RR) and 95%CI were used for the measurement of the relative failure rate.
STATISTICAL ANALYSIS:
Frequentist method network meta-analysis was conducted in Stata/MP (version 14.0, Stata Corp, College Station, TX, USA) with a random-effects model. The proportional variance-covariance matrix data were pooled by multivariate meta-regression with the random effect; restricted maximum-likelihood was applied in the evaluation of model fit [24].
By using global inconsistency tests and node-split tests, the inconsistencies were evaluated, and the consistency model was used under the condition of no existing significant inconsistency, or else the sensitivity analysis would be applied for the inconsistency source identification. Funnel plots and Egger’s tests were used to assess potential publication bias for each endpoint, and by using the trim and filling method, endpoints with underlying asymmetric funnel plots were estimated for whether significant publication bias existed or not [25]. We also ranked the relative efficacy and safety of different surgical methods through the surface under the cumulative ranking (SUCRA) values [26], and cluster-ranking plots for the optimal choice.
A direct pairwise meta-analysis was conducted to compare the relative efficacy of PR (with or without augmentation) with autograft using RevMan (Review Manager, Version 5.3, Copenhagen, The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). The heterogeneity across studies was tested by the Q and I2 statistics. The fixed-effects model was preferred, but if there was significant heterogeneity (
Although CHSs and non-RCTs can provide important data, study designs introduce unmanageable confounding factors and potential bias. Because of this, a subgroup analysis that included only RCTs was performed to reconfirm the results obtained by the main network meta-analysis. A network plot was used to graphically summarize the evidence incorporated into this network meta-analysis, in which the lines between treatment nodes indicated the direct comparisons made within the evidence and the size of nodes indicated the number of population involving in each treatment.
When the 95%CI did not cover 1 for RR or 0 for SMD and WMD, it was considered significant for differences between treatments.
Results
LITERATURE SELECTION:
Thirty-six studies [27–62] were identified through systematic screening (Figure 1). Six different surgical methods were identified and analyzed: autograft (Autograft), allograft with irradiation (irAllograft), allograft without irradiation (nirAllograft), hybrid graft (Hybrid), PR with augmentation (waRepair), and PR without augmentation (nwaRepair). The irAllograft group was chosen as the standard control group because in the pre-analysis it had the worst performance for efficacy and safety.
STUDY CHARACTERISTICS:
The network plot for main and subgroup results is presented in Figure 2. The main network included 24 RCTs, 5 non-RCTs, and 7 CHs, and a total of 3231 patients. A gap of evidence was found between the Hybrid and nwaRepair groups in the main and subgroup networks. A total of 1587, 267, 650, 362, 201, 164 patients were included in the Autograft, irAllograft, nirAllograft, Hybrid, waRepair, and nwaRepair groups, respectively, for the main network, and 1106, 267, 183, 179, and 59 patients were included in the Autograft, irAllograft, nirAllograft, Hybrid, waRepair, and nwaRepair groups for the subgroup network. The average age was 28.12±5.04 (years, mean±SD), and the proportion of male patients was 64% (range 30–87%) (Table 1).
The quality and bias-risk assessments of all studies are presented in Tables 2 and 3. Two main sources of bias were found. Considering the specificity of the surgical intervention in this study, blinding participants and surgeons was almost impossible; meanwhile, it was also difficult to conceal the allocations. It caused a relatively high and inevitable risk of performance bias. The funnel plots and Egger’s tests did not indicate publication bias in any network (Figure 3). Cluster-rank plots are presented in Figure 4. The league plots, which showed the relative effects between different groups, are presented in Tables 4–8.
SUBJECTIVE EVALUATION IMPROVEMENT:
There were 28 trials with 2403 patients included in the final analysis. No inconsistency was detected and the consistency model was used.
The SUCRA results showed that the nwaRepair group had the highest postoperative subjective evaluation improvement (SUCRA=70.9%), followed by nirAllograft (SUCRA=65.2%) and waRepair (SUCRA=61.8%), while the lowest was irAllograft (SUCRA=1.0%). Paradoxically, all groups except nwaRepair (WMD 4.77, 95% CI [−0.23 to 9.78]), were significantly superior to irAllograft. The interpretation of the results should be done cautiously.
FUNCTIONAL IMPROVEMENT:
A total of 32 trials with 2976 patients were included in this network. No significant inconsistency was detected and the consistency model was used.
The nwaRepair group had the highest probability of having the best postoperative functional improvement (SMD 1.14, 95%CI [0.17 to 2.12] SUCRA=97.2%), followed by Autograft (SMD 0.39, 95%CI [−0.09 to 0.87], SUCRA=62.9%) and waRepair (SMD 0.34, 95%CI [−0.42 to 1.10], SUCRA=52.3%), with nirAllograft being the lowest (SUCRA=16.0%). Based on the SMD, only nwaRepair was significantly better than nirAllograft.
ACTIVITY RECOVERY:
A total of 25 trials with 2330 patients were included in this network. No significant in consistency was detected, and the consistency model was used. All groups were significantly better than the nirAllograft group for postoperative activity status. Based on the SUCRA ranking, the best groups for activity recovery were waRepair (WMD 0.84, 95%CI [0.46 to 1.23], SUCRA=94.5%), nwaRepair (WMD 0.61, 95%CI [0.00 to 1.22], SUCRA=62.5%), and Autograft (WMD 0.54, 95%CI [0.30 to 0.78], SUCRA=58.5%).
SAFETY OUTCOMES:
A total of 26 trials (2241 patients) reporting the degree of postoperative knee laxity and 28 trials (2727 patients) reporting the failure rate were assessed in these 2 networks, respectively. No significant inconsistencies were detected, and the consistency model was used for both networks.
All groups had significantly less joint laxity than the irAllograft group. The Autograft group had the lowest degree of laxity (SMD −1.41, 95%CI [−1.74 to −1.08], SUCRA=84.0%), followed by the nwaRepair group (SMD −1.36, 95%CI [−1.88 to −0.83], SUCRA=72.1%) and waRepair group (SMD −1.27, 95%CI [−1.80 to −0.74], SUCRA=60.2%). There was no significant difference among the Autograft, nwaRepair, repair, nirAllograft, and Hybrid groups.
The Autograft group also had the lowest rate of failure (RR 0.30, 95%CI [0.13 to 0.73], SUCRA=89.5%), followed by nirAllograft (RR 0.36, 95%CI [0.12 to 1.07], SUCRA=76.0%) and Hybrid graft (RR 0.51, 95%CI [0.17 to 1.55], SUCRA=54.7%). No significant difference was shown between nwaRepair and irAllograft (RR 1.03, 95%CI [0.26 to 4.07], SUCRA=19.1%). It is worth noting that nwaRepair had significantly higher failure rates than Autograft (RR 3.40, 95%CI [1.18 to 9.82]). Detailed SUCRA values of the main network analyses are presented in Table 9, and the forest plots are presented in Figures 5 and 6.
SUBGROUP ANALYSIS OF RCTS:
All 24 RCTs (2541 patients) were included in this subgroup analysis. No inconsistencies were reported, and the consistency model was used for all outcomes. The only difference from the full analysis was in activity recovery. In the RCTs subgroup analysis, no significant difference was shown between nwaRepair and irAllograft (WMD 0.57, 95%CI [−0.05 to 1.19]) in activity recovery (Table 10). Forest plots for results of subgroup analysis are shown in Figures 7 and 8.
DIRECT PAIRWISE META-ANALYSIS:
Direct pairwise comparisons of the postoperative efficacy and safety of PR and ACLR showed significant heterogeneity in all outcomes. Therefore, based on a pre-analysis, the direct comparisons were separated into 2: waRepair vs ACLR, and nwaRepair vs ACLR (Tables 11, 12). Sensitivity analysis was used to minimize heterogeneity.
Direct comparison of waRepair with ACLR showed significant heterogeneity in activity improvement (I2=67.5%) and consequently, a random-effects model was used for this outcome, while a fixed-effects model was used for other outcomes. The only significant difference between waRepair and ACLR was in activity improvement outcome (WMD 0.28 95%CI [0.07 to 0.49]). Considering the heterogeneity, this result should be viewed with caution.
Direct comparison of nwaRepair with ACLR showed significant heterogeneity in subjective evaluation improvement (I2=58.80%) and functional improvement (I2=92.30%), and a random-effects model was used for these 2 outcomes. No significant differences were found between nwaPR and ACLR.
Discussion
This is the first network meta based on high-quality studies to compare the functional recovery and adverse effects of PR with ACLR in the surgical treatment of ACL rupture. The important observations from this analysis are: (1) waRepair and nwaRepair ranked the best for postoperative efficacy in activity recovery and subjective and functional improvement, while ACLR with irAllograft was a poor option for the surgical treatment of ACL rupture, with the weakest efficacy and the worst safety profile; (2) ACLR with allograft without irradiation produced a similar improvement in subjective evaluation improvement when compared with PR, but less functional improvement and activity recovery; (3) PR produced less postoperative knee laxity than irradiated allograft ACLR but had a higher failure rate than ACLR with Autograft, if without an augmentation. This suggests that PR may have other potentially serious complications that could necessitate revision surgery; (4) ACLR with autograft and hybrid graft yielded good results for efficacy and safety, and both were good choices for surgery; and (5) ACLR with autograft was the safest and most stable surgery method according to the results of postoperative knee laxity and revision rate and the cluster-rank analysis.
In a study by Sun et al [46], autograft and non-irradiated allograft ACLR had comparable outcomes for postoperative symptoms, functional improvement, and activity level, and both had a lower incidence of graft failure than irradiated allograft ACLR. Separately, Curran et al [61] studied the effects of irradiated allograft ACLR and showed that the low dose of irradiation could weaken the strength and stiffness of the allograft, result in altered graft function, and affect the clinical outcomes of ACLR. Our findings are consistence with these results. In addition, the network meta-analysis by Yang et al [62] compared the long-term outcomes of different grafts in ACLR and recommended double-bundle hamstring autograft as the best choice for its good prognosis. Another study [63] compared different tendon grafts for ACLR and also revealed that autografts (especially quadricep tendon autografts) rather than artificial ligaments were suitable for primary ACLR because artificial ligaments could increase the risk of knee laxity. Compared with the previous studies, the present study pointed out that PR could be an ideal surgical method in terms of efficacy but is related to a significantly higher revision risk, and autograft ACLR may be the optimal strategy for surgical treatment of ACLR.
In this analysis, the PR technique showed similar and even better clinical outcomes than autograft and hybrid graft ACLR. This most likely resulted from the lack of harvesting of the graft tissue and avoiding donor site complications, leading to better activity recovery and subjective and functional improvements. However, it should be noted that while PR was shown to produce less knee laxity, it was found to lead to a relatively high graft failure rate compared with that of autograft and non-irradiated allograft. One explanation for this is that after PR surgery the scar formed for healing of the ruptured ACL leads to a contracture of ACL or/and limited knee movement (Hoogeslag et al [19]).
There were still several limitations in this study. First, some factors can affect outcomes but cannot be adjusted or removed by statistical methods, such as the skill of the surgeons and the quality of the postoperative rehabilitation. Second, an RCT is more sensitive to complications, with a high incidence and a short period, while observational studies can more effectively assess the complications with a low incidence and a long period. Given the important role of observational studies, such as cohort studies, in exploring the long-term efficacy and safety of ACL rupture surgery and although CHSs and non-RCTs potentially have confounding factors that can bias the results, we still included them in the analysis and used a subgroup analysis to examine the impact of observational studies on the results. The subgroup analysis on the RCTs showed only 1 difference from the main network analysis, suggesting that any biases from CHSs and non-RCTs were unlikely to be a factor in this analysis. Third, studies with no events in both treatment arms were inevitably included in the failure rate network. Omitting studies with rare events was recommended by the Cochrane Handbook, but this is still controversial as it can alter the biased evaluations and the accuracy of the combined estimation. Therefore, we included such trials and used a 0.5 zero-cell correction. However, the results of the failure rates should be interpreted with caution. Fourth, while funnel plots and Egger’s tests showed no significant publication bias or small study effects, only a limited number of trials were included, and therefore more high-quality trials are warranted.
Conclusions
For surgical treatment of ACLR, irradiated allograft ACLR had the worst efficacy and safety and is not recommended. PR may be an ideal treatment method in terms of efficacy but it is related to a significantly higher revision risk if done without augmentation. Autograft ACLR may be the optimal method currently available for most patients requiring surgical treatment of ACL rupture.
Figures
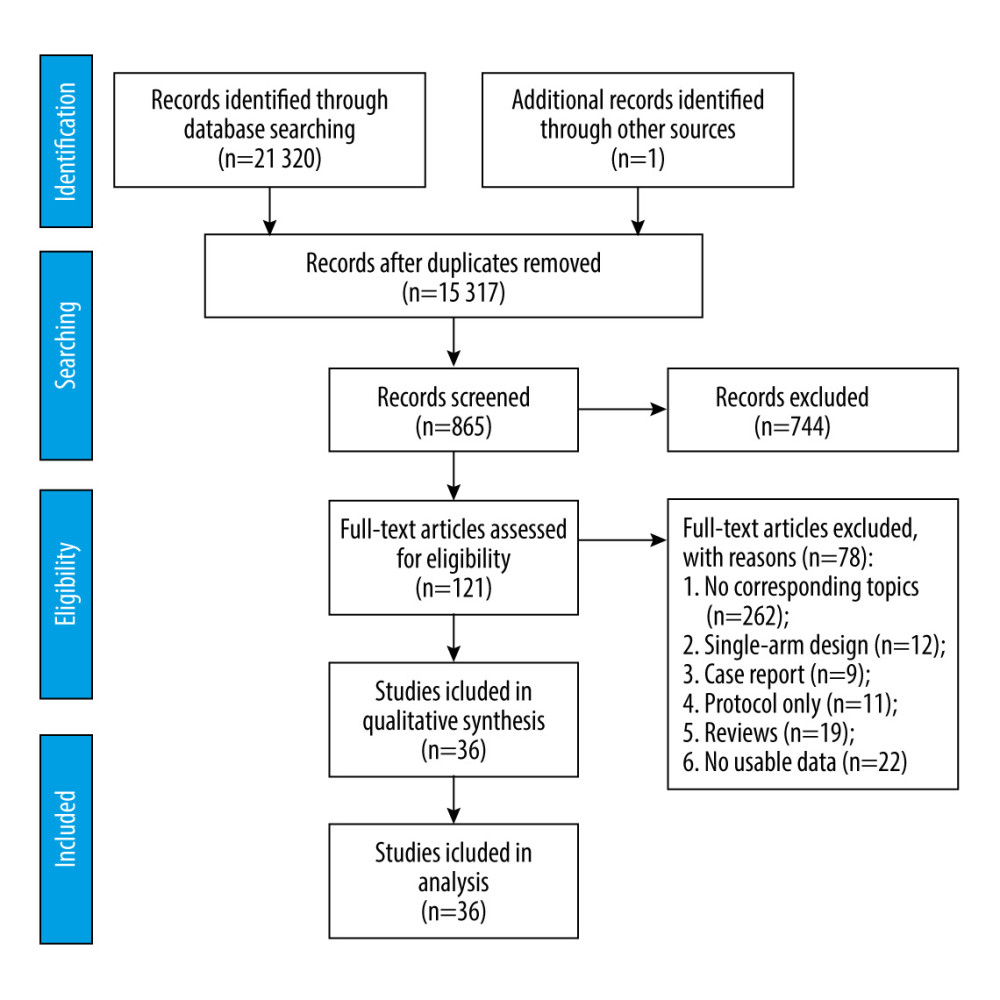 Figure 1. PRISMA Flow Diagram.
Figure 1. PRISMA Flow Diagram. 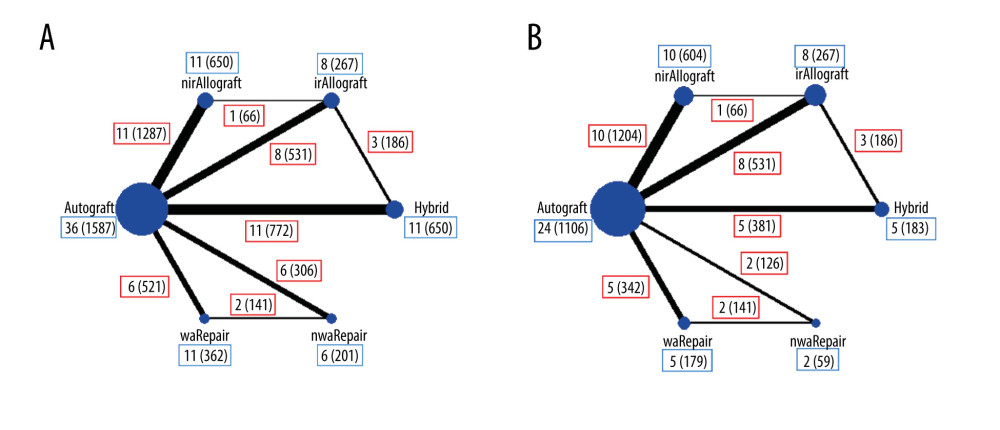 Figure 2. Structure of network formed by interventions. The lines between treatment nodes indicate the direct comparisons made with evidences, the size of nodes indicate the number of participants involved in each treatment. Numbers (n/n) with a blue frame near the line indicate ‘number of trials/number of participants’ of the related treatment group, numbers (n/n) with a red frame near the line indicate ‘number of trials/number of participants’ of the related comparisons. (A) Main network meta-analysis. (B) Subgroup analysis. (Made with Stata/MP, version 14.0, manufacturer Stata Corp.).
Figure 2. Structure of network formed by interventions. The lines between treatment nodes indicate the direct comparisons made with evidences, the size of nodes indicate the number of participants involved in each treatment. Numbers (n/n) with a blue frame near the line indicate ‘number of trials/number of participants’ of the related treatment group, numbers (n/n) with a red frame near the line indicate ‘number of trials/number of participants’ of the related comparisons. (A) Main network meta-analysis. (B) Subgroup analysis. (Made with Stata/MP, version 14.0, manufacturer Stata Corp.). 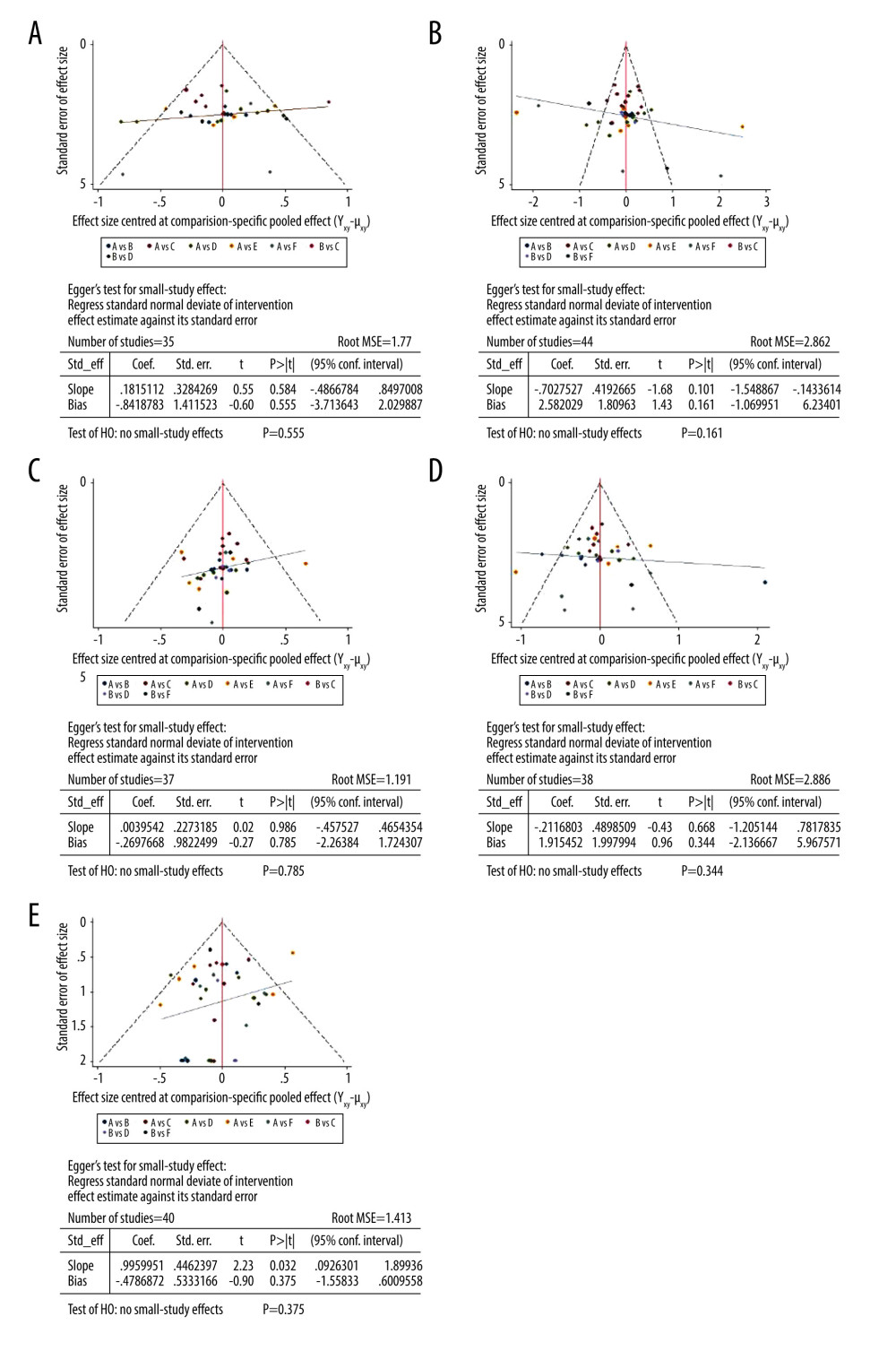 Figure 3. Publication bias and Egger’s test for main networks. (A) Subjective improvement. (B) Functional improvement. (C) Activity recovery. (D) Postoperative laxity. (E) Failure rate.
Figure 3. Publication bias and Egger’s test for main networks. (A) Subjective improvement. (B) Functional improvement. (C) Activity recovery. (D) Postoperative laxity. (E) Failure rate. 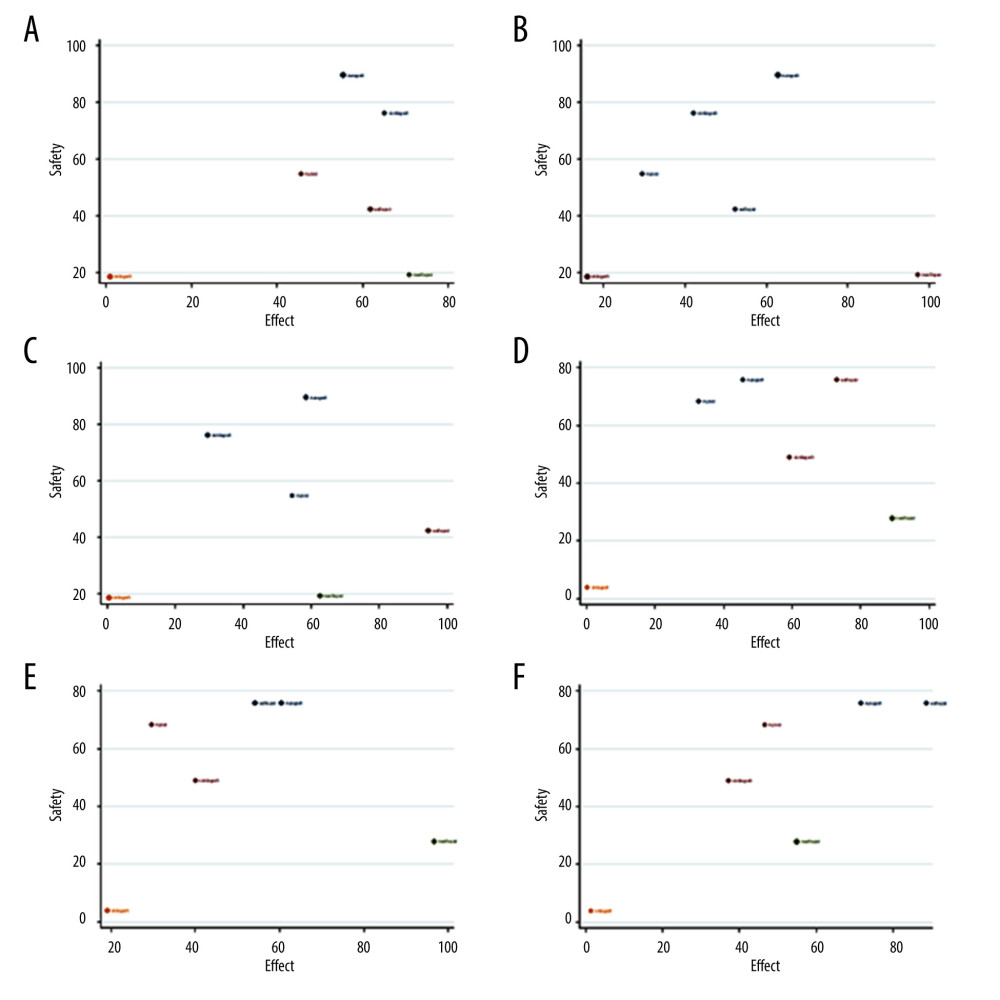 Figure 4. Cluster-rank plots. (A) The cluster-rank plot of subjective improvement and failure rate from main network analyses. (B) The cluster-rank plot of functional improvement and failure rate from main network analyses. (C) The cluster-rank plot of activity recovery and failure rate from main network analyses. (D) The cluster-rank plot of subjective improvement and failure rate from subgroup analyses. (E) The cluster-rank plot of functional improvement and failure rate from subgroup analyses. (F) The cluster-rank plot of activity recovery and failure rate from subgroup analyses. (The cluster-rank value is the product of the abscissa and ordinate of each treatment.)
Figure 4. Cluster-rank plots. (A) The cluster-rank plot of subjective improvement and failure rate from main network analyses. (B) The cluster-rank plot of functional improvement and failure rate from main network analyses. (C) The cluster-rank plot of activity recovery and failure rate from main network analyses. (D) The cluster-rank plot of subjective improvement and failure rate from subgroup analyses. (E) The cluster-rank plot of functional improvement and failure rate from subgroup analyses. (F) The cluster-rank plot of activity recovery and failure rate from subgroup analyses. (The cluster-rank value is the product of the abscissa and ordinate of each treatment.) 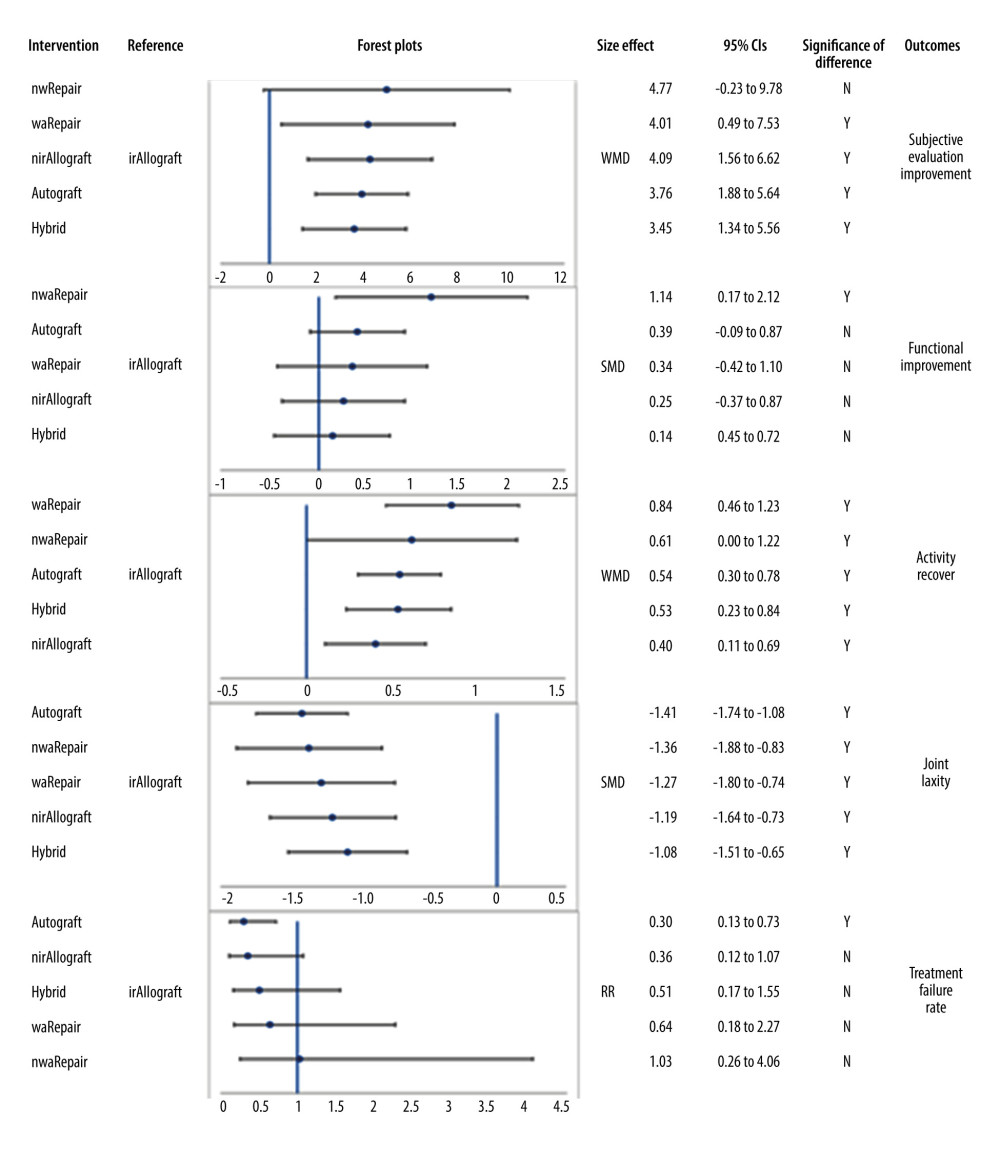 Figure 5. Forest plots of network comparisons of main network meta-analysis (made with Microsoft Excel, version 2019MSO).
Figure 5. Forest plots of network comparisons of main network meta-analysis (made with Microsoft Excel, version 2019MSO). 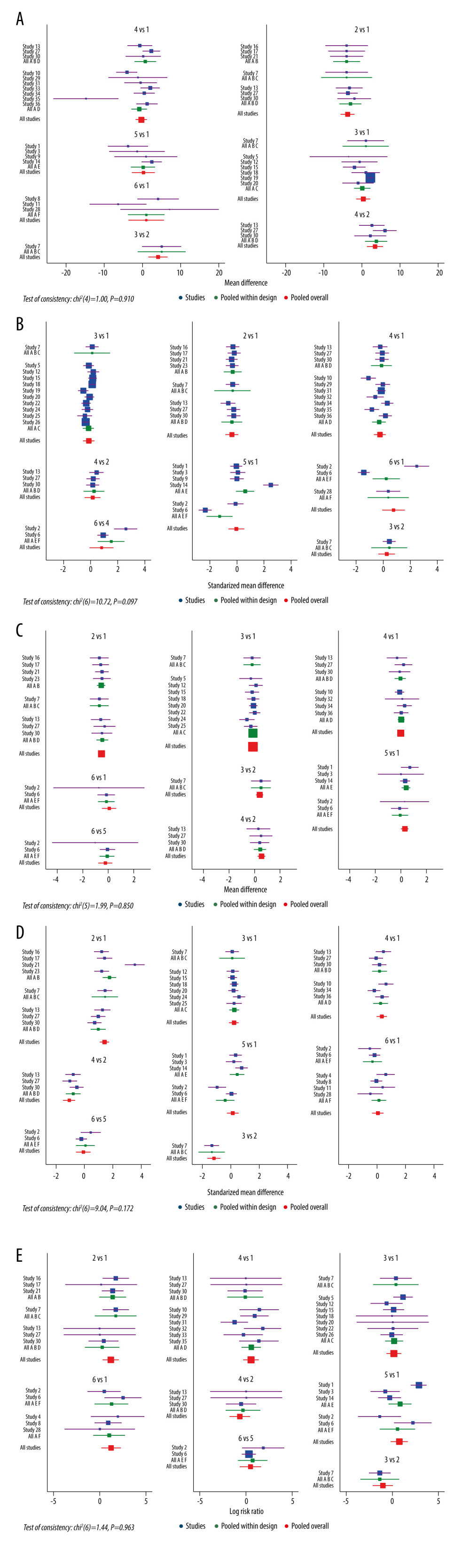 Figure 6. Forest plots incorporated direct comparisons and indirect comparisons of main network meta-analysis. (A) Subjective improvement. (B) Functional improvement. (C) Activity recovery. (D) Postoperative laxity. (E) Failure rate. (A or 1: Autograft; B or 2: Allograft with irradiation; C or 3: Allograft without irradiation; D or 4: Hybrid graft; E or 5: Repair with augmentation; F or 6: Repair without augmentation).
Figure 6. Forest plots incorporated direct comparisons and indirect comparisons of main network meta-analysis. (A) Subjective improvement. (B) Functional improvement. (C) Activity recovery. (D) Postoperative laxity. (E) Failure rate. (A or 1: Autograft; B or 2: Allograft with irradiation; C or 3: Allograft without irradiation; D or 4: Hybrid graft; E or 5: Repair with augmentation; F or 6: Repair without augmentation). 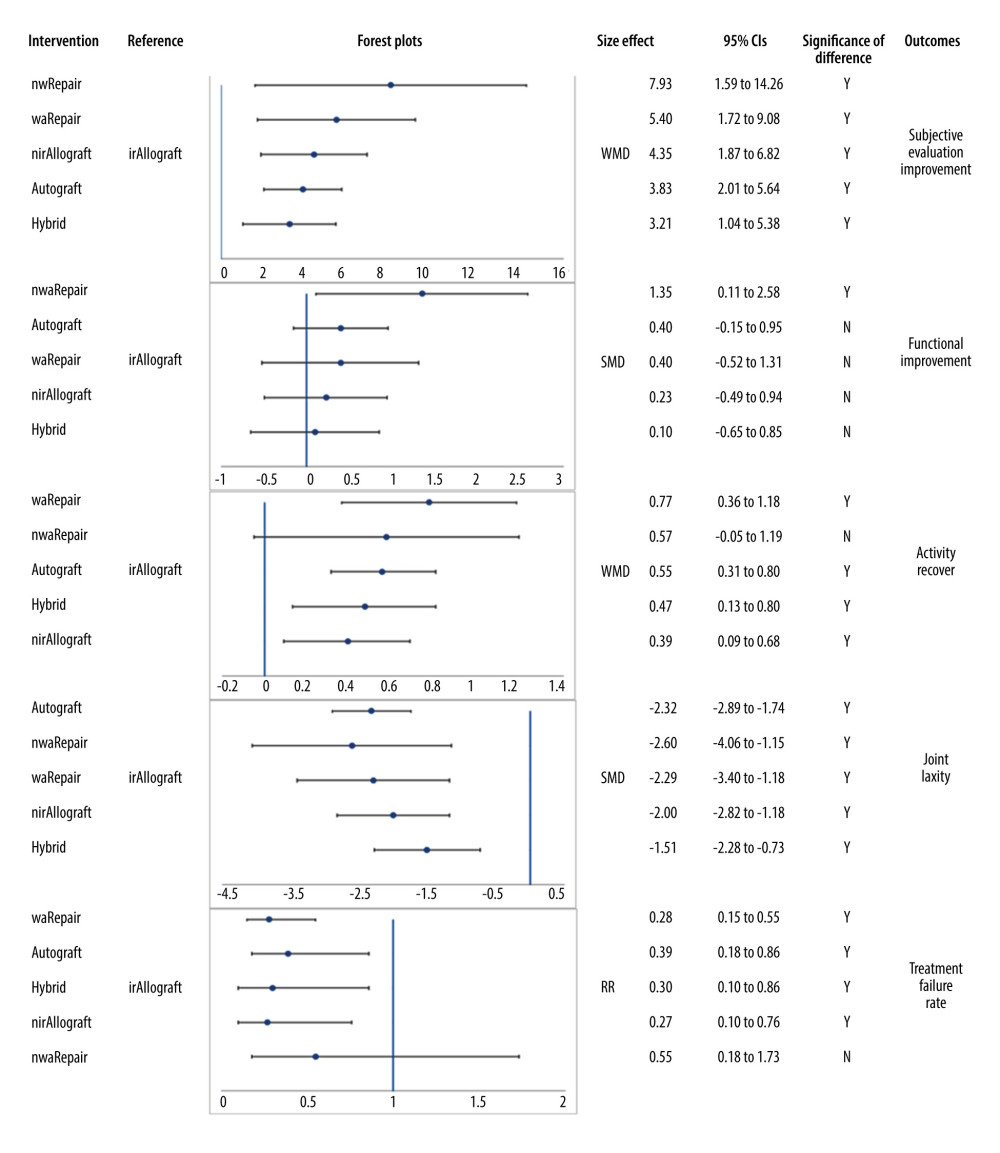 Figure 7. Forest plots of network comparisons of subgroup network meta-analysis (made with Microsoft Excel, version 2019MSO).
Figure 7. Forest plots of network comparisons of subgroup network meta-analysis (made with Microsoft Excel, version 2019MSO). 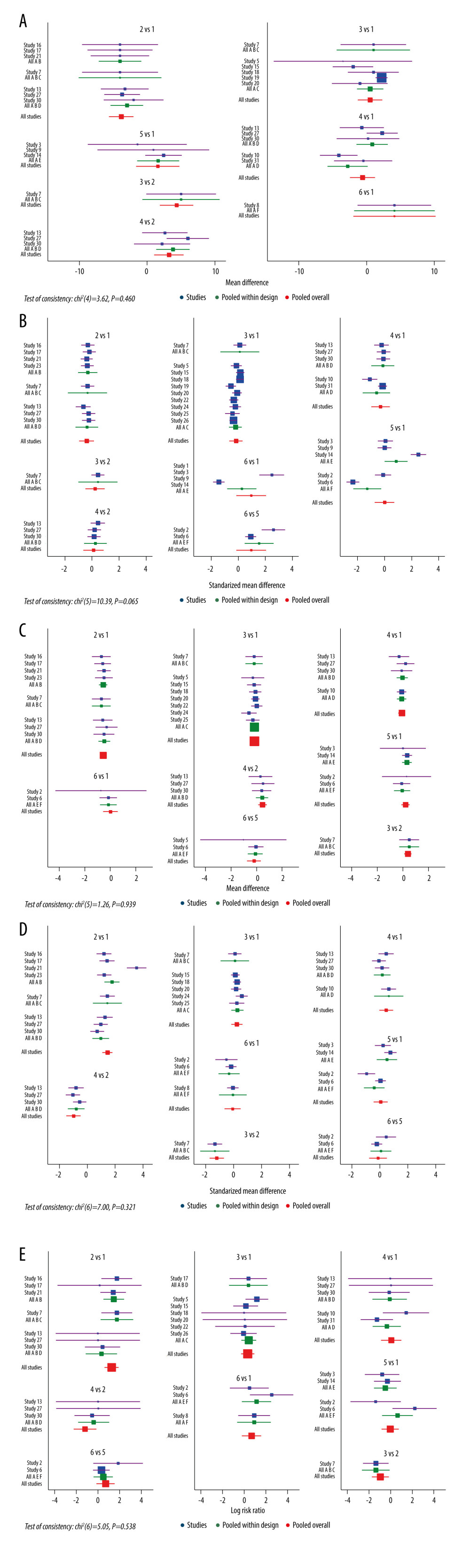 Figure 8. Forest plots incorporated direct comparisons and indirect comparisons of subgroup analysis. (A) Subjective improvement. (B) Functional improvement. (C) Activity recovery. (D) Postoperative laxity. (E) Failure rate. (A or 1: Autograft; B or 2: Allograft with irradiation; C or 3: Allograft without irradiation; D or 4: Hybrid graft; E or 5: Repair with augmentation; F or 6: Repair without augmentation.).
Figure 8. Forest plots incorporated direct comparisons and indirect comparisons of subgroup analysis. (A) Subjective improvement. (B) Functional improvement. (C) Activity recovery. (D) Postoperative laxity. (E) Failure rate. (A or 1: Autograft; B or 2: Allograft with irradiation; C or 3: Allograft without irradiation; D or 4: Hybrid graft; E or 5: Repair with augmentation; F or 6: Repair without augmentation.). Tables
Table 1. Baseline characteristics of included studies.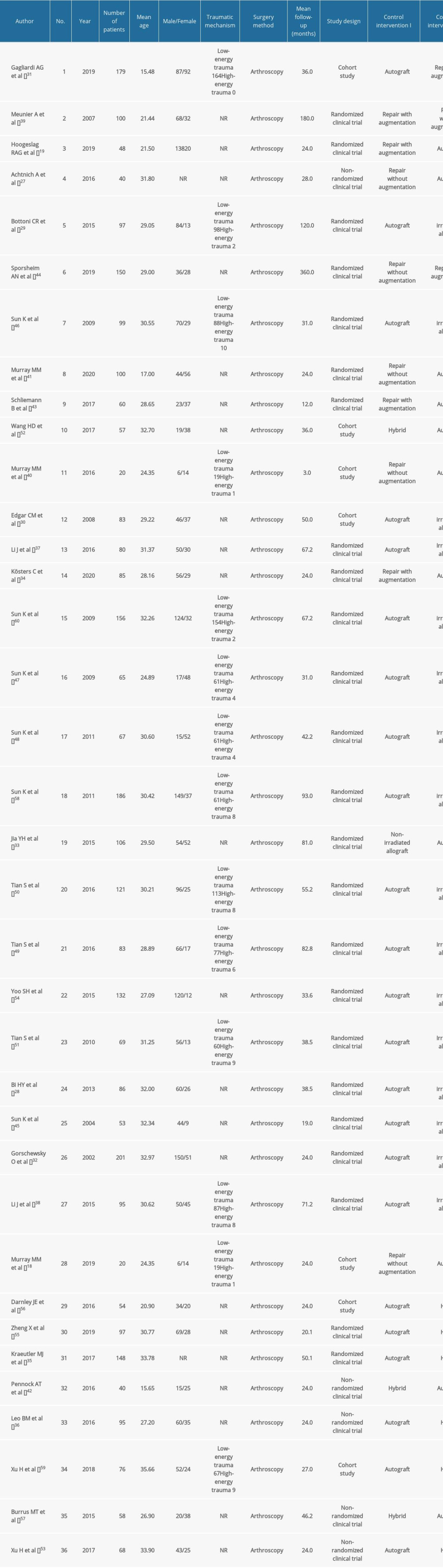 Table 2. Methodological quality and risk of bias evaluation of randomized controlled studies.
Table 2. Methodological quality and risk of bias evaluation of randomized controlled studies.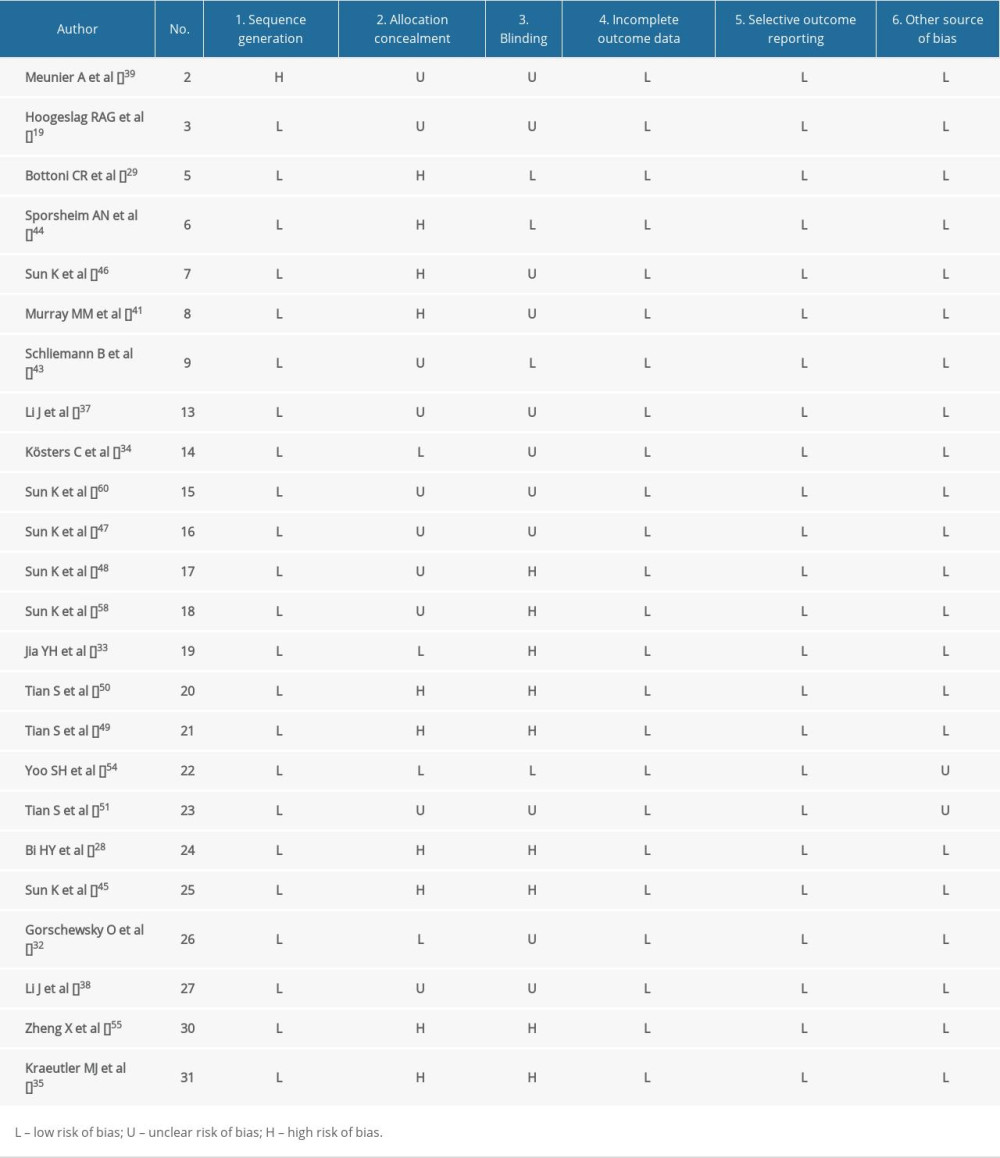 Table 3. Methodological quality and risk of bias evaluation of non-randomized control and cohort design studies.
Table 3. Methodological quality and risk of bias evaluation of non-randomized control and cohort design studies.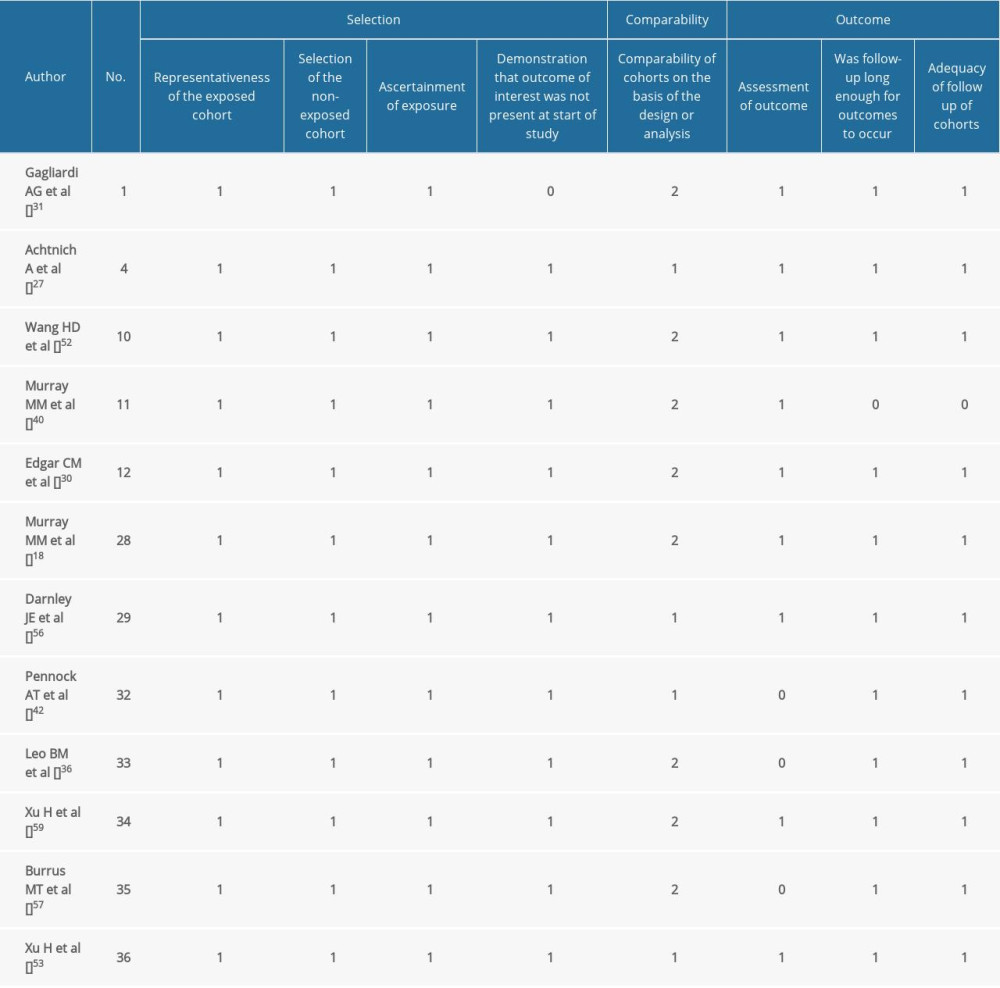 Table 4. The league plots of subjective improvement. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, WMD with 95% CI).
Table 4. The league plots of subjective improvement. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, WMD with 95% CI).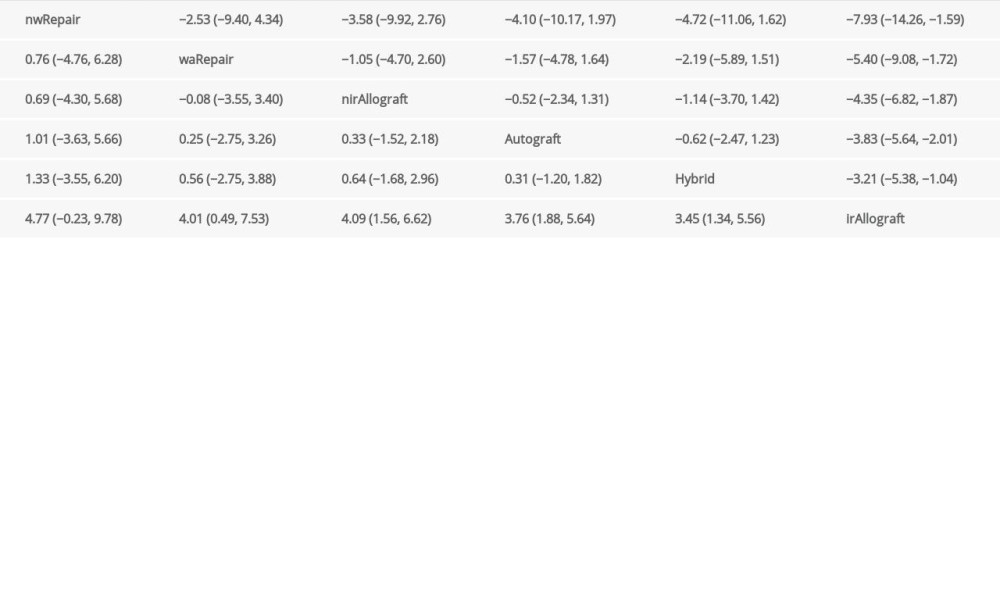 Table 5. The league plots of functional improvement. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, SMD with 95% CI).
Table 5. The league plots of functional improvement. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, SMD with 95% CI).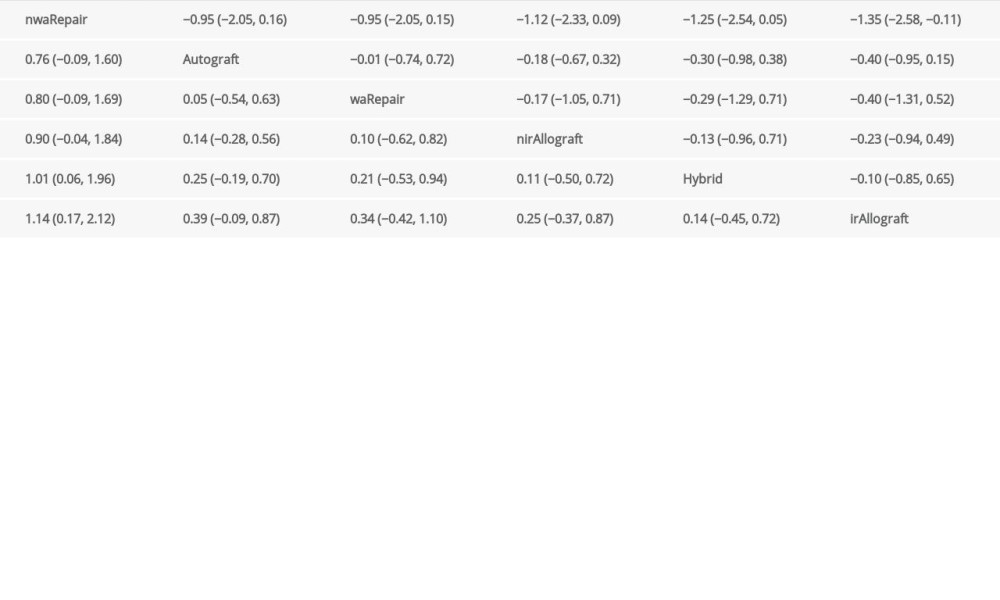 Table 6. The league plots of activity recovery. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, WMD with 95% CI).
Table 6. The league plots of activity recovery. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, WMD with 95% CI).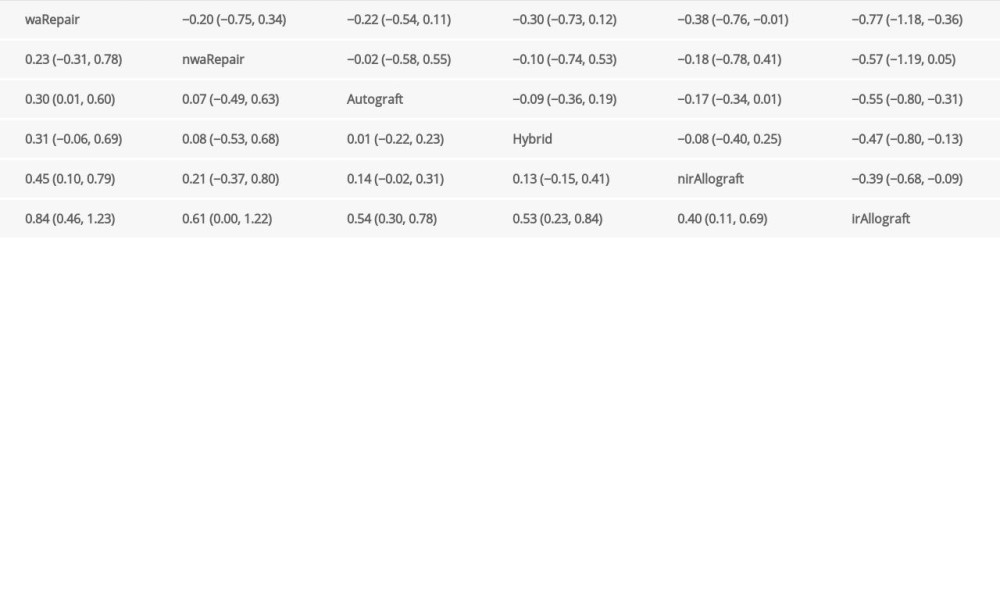 Table 7. The league plots of postoperative laxity. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, SMD with 95% CI).
Table 7. The league plots of postoperative laxity. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, SMD with 95% CI).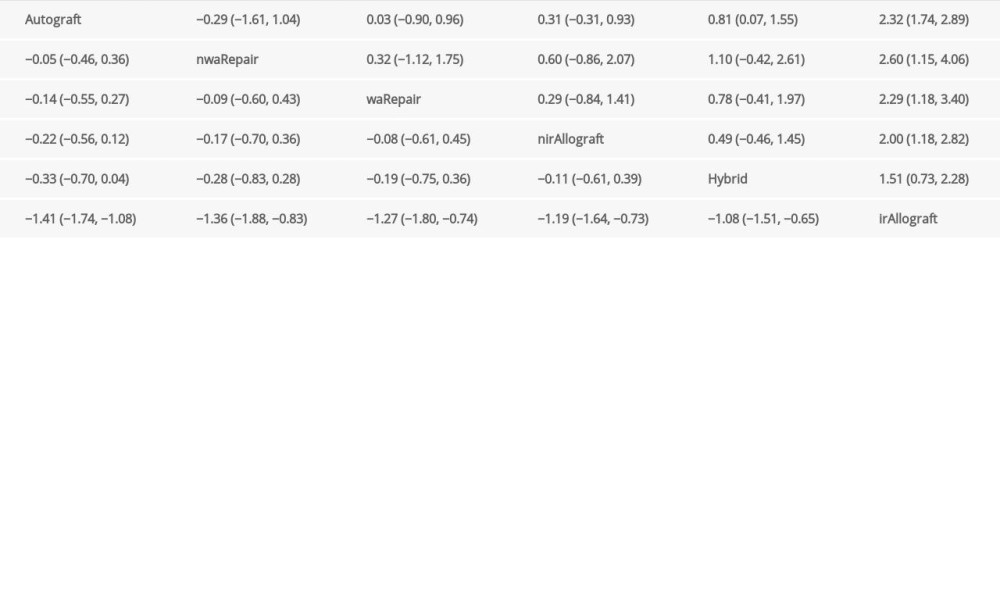 Table 8. The league plots of failure rate. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, RR with 95% CI).
Table 8. The league plots of failure rate. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, RR with 95% CI).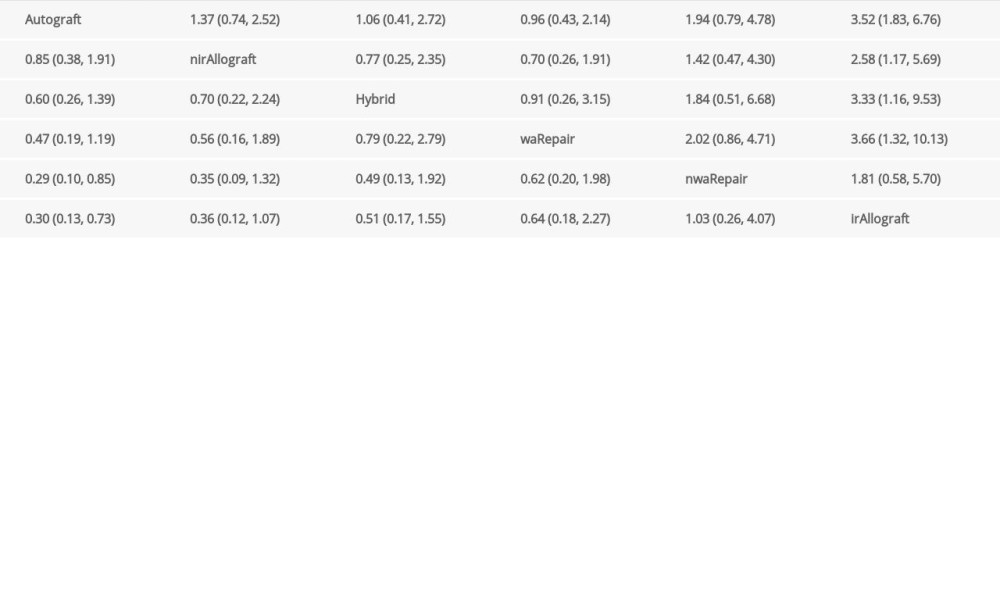 Table 9. Detailed results of main network analysis.
Table 9. Detailed results of main network analysis.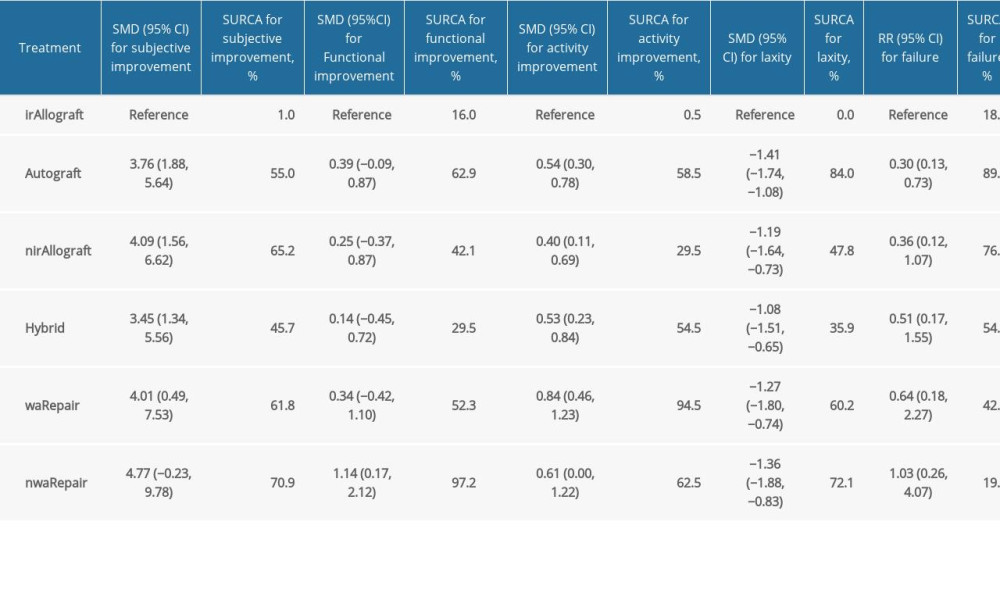 Table 10. Detailed results of subgroup analysis.
Table 10. Detailed results of subgroup analysis.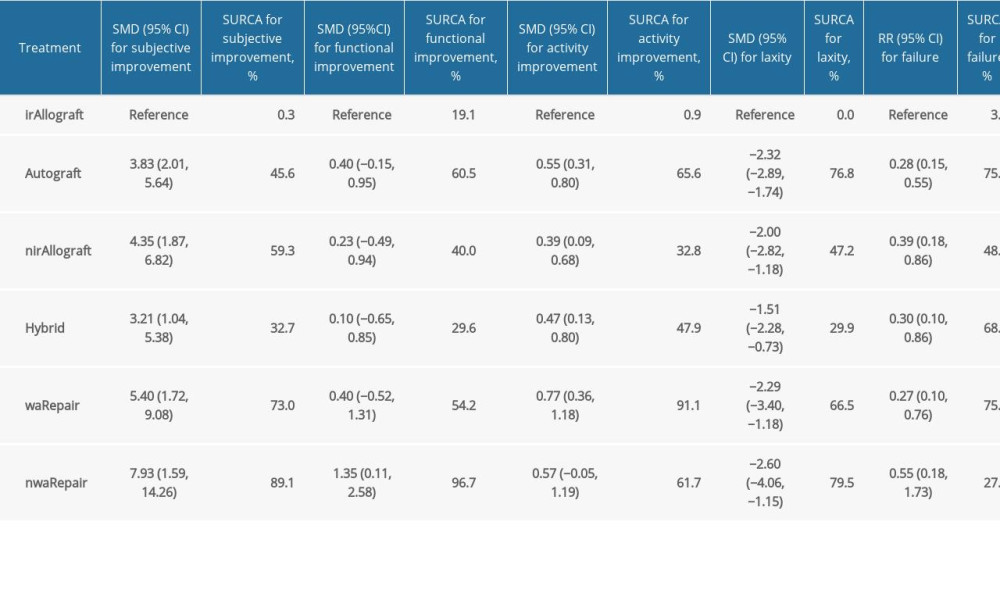 Table 11. The detailed results of direct pair-wise meta-analyses between primary repair (PR) with augmentation and anterior cruciate ligament reconstruction (ACLR).
Table 11. The detailed results of direct pair-wise meta-analyses between primary repair (PR) with augmentation and anterior cruciate ligament reconstruction (ACLR).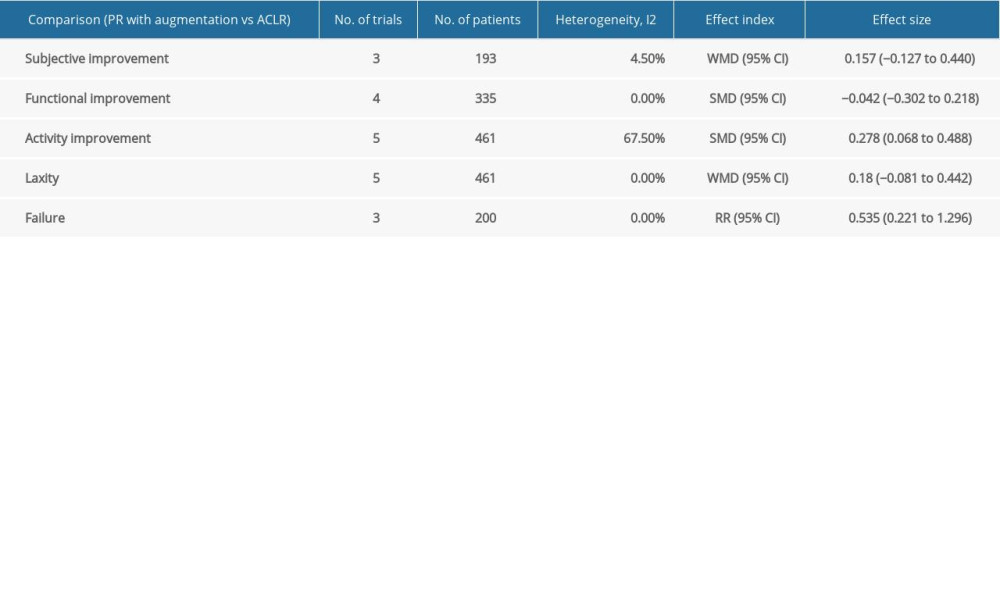 Table 12. The detailed results of direct pair-wise meta-analyses between primary repair (PR) without augmentation and anterior cruciate ligament reconstruction (ACLR).
Table 12. The detailed results of direct pair-wise meta-analyses between primary repair (PR) without augmentation and anterior cruciate ligament reconstruction (ACLR).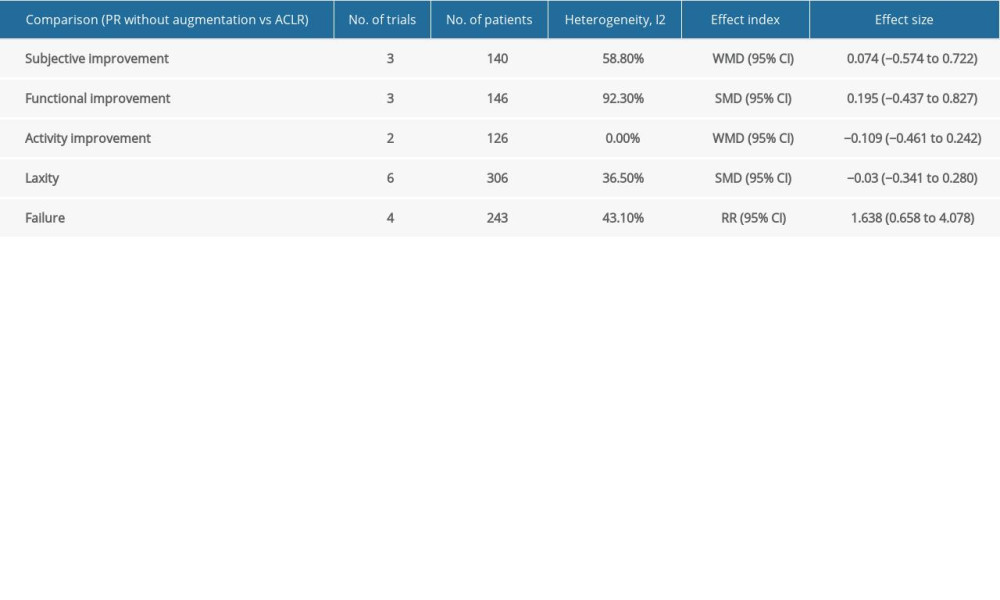
References
1. Musahl V, Karlsson J, Anterior cruciate ligament tear: N Engl J Med, 2019; 380(24); 2341-48
2. Diermeier TA, Rothrauff BB, Engebretsen L, Treatment after ACL injury: Panther Symposium ACL Treatment Consensus Group: Br J Sports Med, 2021; 55(1); 14-22
3. Boden BP, Dean GS, Feagin JA, Mechanisms of anterior cruciate ligament injury: Orthopedics, 2000; 23(6); 573-78
4. Feagin JA, Curl WW, Isolated tear of the anterior cruciate ligament: 5-year follow-up study: Am J Sports Med, 1976; 4(3); 95-100
5. Marshall JL, Warren RF, Wickiewicz TL, Primary surgical treatment of anterior cruciate ligament lesions: Am J Sports Med, 1982; 10; 103-7
6. Engebretsen L, Benum P, Sundalsvoll S, Primary suture of the anterior cruciate ligament. A 6-year follow-up of 74 cases: Acta Orthop Scand, 1989; 60(5); 561-64
7. van der List JP, Vermeijden HD, Sierevelt IN, Arthroscopic primary repair of proximal anterior cruciate ligament tears seems safe but higher level of evidence is needed: A systematic review and meta-analysis of recent literature [published correction appears in Knee Surg Sports Traumatol Arthrosc. 2019 Nov 6] [published correction appears in Knee Surg Sports Traumatol Arthrosc. 2022;30(3):1123–25]: Knee Surg Sports Traumatol Arthrosc, 2020; 28(6); 1946-57
8. van der List JP, DiFelice GS, Range of motion and complications following primary repair versus reconstruction of the anterior cruciate ligament: Knee, 2017; 24(4); 798-807
9. Mackay GM, Blyth MJ, Anthony I, A review of ligament augmentation with the InternalBrace™: the surgical principle is described for the lateral ankle ligament and ACL repair in particular, and a comprehensive review of other surgical applications and techniques is presented: Surg Technol Int, 2015; 26; 239-55
10. Duchman KR, Lynch TS, Spindler KP, Graft selection in anterior cruciate ligament surgery: Who gets what and why?: Clin Sports Med, 2017; 36(1); 25-33
11. Alvarez-Pinzon AM, Barksdale L, Krill MK, Hybrid graft anterior cruciate ligament reconstruction: A predictable graft for knee stabilization: Orthopedics, 2015; 38(6); e473-76
12. Grassi A, Carulli C, Innocenti M, New trends in anterior cruciate ligament reconstruction: a systematic review of national surveys of the last 5 years: Joints, 2018; 6(3); 177-87
13. Engelman GH, Carry PM, Hitt KG, Comparison of allograft versus autograft anterior cruciate ligament reconstruction graft survival in an active adolescent cohort: Am J Sports Med, 2014; 42(10); 2311-18
14. Freedman KB, Editorial commentary: Graft choice for anterior cruciate ligament reconstruction: Will there ever be a correct answer? Probably not: Arthroscopy, 2020; 36(6); 1647-48
15. Wang HD, Gao SJ, Zhang YZ, Hamstring autograft versus hybrid graft for anterior cruciate ligament reconstruction: A systematic review: Am J Sports Med, 2020; 48(4); 1014-22
16. Li N, Xue X, Tu H, Anterior cruciate ligament reconstruction with hybrid graft versus autograft: A systematic review and meta-analysis: J Healthc Eng, 2021; 2021; 7562649
17. Sun J, Wei XC, Li L, Autografts vs synthetics for cruciate ligament reconstruction: A systematic review and meta-analysis: Orthop Surg, 2020; 12(2); 378-87
18. Murray MM, Fleming BC, Badger GJ, Bridge-enhanced anterior cruciate ligament repair is not inferior to autograft anterior cruciate ligament reconstruction at 2 years: Results of a prospective randomized clinical trial: Am J Sports Med, 2020; 48(6); 1305-15
19. Hoogeslag RAG, Brouwer RW, Boer BC, Acute anterior cruciate ligament rupture: Repair or reconstruction? Two-year results of a randomized controlled clinical trial: Am J Sports Med, 2019; 47(3); 567-77
20. Burton DA, Schaefer EJ, Shu HT, Primary anterior cruciate ligament repair using suture tape augmentation: A case series of 29 patients with minimum 2-year follow-up: Arthroscopy, 2021; 37(4); 1235-41
21. Hutton B, Salanti G, Caldwell DM, The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations: Ann Intern Med, 2015; 162(11); 777-84
22. Higgins JP, Green S: Cochrane handbook for systematic reviews of interventions, 2008, Wiley-Blackwell
23. Wells G, Shea B, O’Connell D, The Newcastle-Ottawa Scale (NOS) for assessing the quality of case-control studies in meta-analyses: Eur J Epidemiol, 2011; 25; 603-5
24. White IR, Barrett JK, Jackson D, Consistency and inconsistency in network meta-analysis: Model estimation using multivariate meta-regression: Res Synth Methods, 2012; 3(2); 111-25
25. Duval S, Tweedie R, Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis: Biometrics, 2000; 56(2); 455-63
26. Rücker G, Schwarzer G, Ranking treatments in frequentist network meta-analysis works without resampling methods: BMC Med Res Methodol, 2015; 15; 58
27. Achtnich A, Herbst E, Forkel P, Acute proximal anterior cruciate ligament tears: Outcomes after arthroscopic suture anchor repair versus anatomic single-bundle reconstruction: Arthroscopy, 2016; 32(12); 2562-69
28. Bi HY, Sun XJ, Mu HJProspective comparative study of arthroscopic anterior cruciate ligament construction with autograft and allograft: Zhonghua Wai Ke Za Zhi, 2013; 51(1); 44-48 [in Chinese]
29. Bottoni CR, Smith EL, Shaha J, Autograft versus allograft anterior cruciate ligament reconstruction: A prospective, randomized clinical study with a minimum 10-year follow-up: Am J Sports Med, 2015; 43(10); 2501-9
30. Edgar CM, Zimmer S, Kakar S, Prospective comparison of auto and allograft hamstring tendon constructs for ACL reconstruction: Clin Orthop Relat Res, 2008; 466(9); 2238-46
31. Gagliardi AG, Carry PM, Parikh HB, ACL repair with suture ligament augmentation is associated with a high failure rate among adolescent patients: Am J Sports Med, 2019; 47(3); 560-66
32. Gorschewsky O, Browa A, Vogel UClinico-histologic comparison of allogenic and autologous bone-tendon-bone using one-third of the patellar tendon in reconstruction of the anterior cruciate ligament: Unfallchirurg, 2002; 105(8); 703-14 [in German]
33. Jia YH, Sun PF, Comparison of clinical outcome of autograft and allograft reconstruction for anterior cruciate ligament tears: Chin Med J (Engl), 2015; 128(23); 3163-66
34. Kösters C, Glasbrenner J, Spickermann L, Repair with dynamic intraligamentary stabilization versus primary reconstruction of acute anterior cruciate ligament tears: 2-year results from a prospective randomized study: Am J Sports Med, 2020; 48(5); 1108-16
35. Kraeutler MJ, Kim SH, Brown CC, Clinical outcomes following primary anterior cruciate ligament reconstruction with hamstring autograft versus planned hybrid graft: J Knee Surg, 2018; 31(9); 827-33
36. Leo BM, Krill M, Barksdale L, Failure rate and clinical outcomes of anterior cruciate ligament reconstruction using autograft hamstring versus a hybrid graft: Arthroscopy, 2016; 32(11); 2357-63
37. Li J, Kong F, Gao X, Prospective randomized comparison of knee stability and proprioception for posterior cruciate ligament reconstruction with autograft, hybrid graft, and γ-irradiated allograft: Arthroscopy, 2016; 32(12); 2548-55
38. Li J, Wang J, Li Y, A prospective randomized study of anterior cruciate ligament reconstruction with autograft, γ-irradiated allograft, and hybrid graft: Arthroscopy, 2015; 31(7); 1296-302
39. Meunier A, Odensten M, Good L, Long-term results after primary repair or non-surgical treatment of anterior cruciate ligament rupture: A randomized study with a 15-year follow-up: Scand J Med Sci Sports, 2007; 17(3); 230-37
40. Murray MM, Flutie BM, Kalish LA, The bridge-enhanced anterior cruciate ligament repair (BEAR) procedure: An early feasibility cohort study: Orthop J Sports Med, 2016; 4(11); 2325967116672176
41. Murray MM, Kalish LA, Fleming BC, Bridge-enhanced anterior cruciate ligament repair: Two-year results of a first-in-human study: Orthop J Sports Med, 2019; 7(3); 2325967118824356
42. Pennock AT, Ho B, Parvanta K, Does allograft augmentation of small-diameter hamstring autograft ACL grafts reduce the incidence of graft retear?: Am J Sports Med, 2017; 45(2); 334-38
43. Schliemann B, Glasbrenner J, Rosenbaum D, Changes in gait pattern and early functional results after ACL repair are comparable to those of ACL reconstruction: Knee Surg Sports Traumatol Arthrosc, 2018; 26(2); 374-80
44. Sporsheim AN, Gifstad T, Lundemo TO, Autologous BPTB ACL reconstruction results in lower failure rates than ACL repair with and without synthetic augmentation at 30 years of follow-up: A prospective randomized study: J Bone Joint Surg Am, 2019; 101(23); 2074-81
45. Sun K, Tang JW, Xu QA prospective study of the anterior cruciate ligament reconstruction: allograft versus autograft: Chin J Surg, 2004; 42(16); 989-92 [in Chinese]
46. Sun KS, Tian S, Zhang J, Anterior cruciate ligament reconstruction with BPTB autograft, irradiated versus non-irradiated allograft: A prospective randomized clinical study: Knee Surg Sports Traumatol Arthrosc, 2009; 17(5); 464-74
47. Sun K, Tian SQ, Zhang JH, ACL reconstruction with BPTB autograft and irradiated fresh frozen allograft: J Zhejiang Univ Sci B, 2009; 10(4); 306-16
48. Sun K, Zhang J, Wang Y, Arthroscopic anterior cruciate ligament reconstruction with at least 2.5 years’ follow-up comparing hamstring tendon autograft and irradiated allograft: Arthroscopy, 2011; 27(9); 1195-202
49. Tian S, Wang B, Liu L, Irradiated hamstring tendon allograft versus autograft for anatomic double-bundle anterior cruciate ligament reconstruction: midterm clinical outcomes: Am J Sports Med, 2016; 44(10); 2579-88
50. Tian S, Wang Y, Wang B, Anatomic double-bundle anterior cruciate ligament reconstruction with a hamstring tendon autograft and fresh-frozen allograft: A prospective, randomized, and controlled study: Arthroscopy, 2016; 32(12); 2521-31
51. Tian S, Zhang J, Wang YA prospective study on anterior cruciate ligament reconstruction with patellar tendon autograft versus gamma irradiated allograft.]: Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi, 2010; 24(3); 282-86 [in Chinese]
52. Wang HD, Gao SJ, Zhang YZ, Comparison of clinical outcomes after anterior cruciate ligament reconstruction using a hybrid graft versus a hamstring autograft: Arthroscopy, 2018; 34(5); 1508-16
53. Xu H, Dong J, Xin D, Second-look arthroscopic evaluation and clinical outcomes of anatomic anterior cruciate ligament reconstruction with autograft and hybrid graft: A retrospective study: Med Sci Monit, 2017; 23; 5564-73
54. Yoo S-H, Song EK, Shin Y-R, Comparison of clinical outcomes and second-look arthroscopic findings after ACL reconstruction using a hamstring autograft or a tibialis allograft: Knee Surg Sports Traumatol Arthrosc, 2017; 25; 1290-97
55. Zheng X, Hu Y, Xie P, Clinical outcomes and second-look arthroscopic findings of anterior cruciate ligament reconstruction with autograft, hybrid graft, and allograft: J Orthop Surg Res, 2019; 14(1); 380
56. Darnley JE, Léger-St-Jean B, Pedroza AD, Anterior cruciate ligament reconstruction using a combination of autograft and allograft tendon: A MOON Cohort Study: Orthop J Sports Med, 2016; 4(7); 2325967116662249
57. Burrus MT, Werner BC, Crow AJ, Increased failure rates after anterior cruciate ligament reconstruction with soft-tissue autograft-allograft hybrid grafts: Arthroscopy, 2015; 31(12); 2342-51
58. Sun K, Zhang J, Wang Y, Arthroscopic reconstruction of the anterior cruciate ligament with hamstring tendon autograft and fresh-frozen allograft: A prospective, randomized controlled study: Am J Sports Med, 2011; 39(7); 1430-38
59. Xu H, Lin W, Jin G, Graft choice for anatomic anterior cruciate ligament reconstruction: The comparison between thin autograft and thick hybrid graft. An observational study: Medicine (Baltimore), 2018; 97(30); e11597
60. Sun K, Tian SQ, Zhang JH, Anterior cruciate ligament reconstruction with bone-patellar tendon-bone autograft versus allograft: Arthroscopy, 2009; 25(7); 750-59
61. Curran AR, Adams DJ, Gill JL, The biomechanical effects of low-dose irradiation on bone-patellar tendon-bone allografts: Am J Sports Med, 2004; 32(5); 1131-35
62. Yang W, Huang X, Wang S, The long-term outcomes of different grafts in anterior cruciate ligament reconstruction: A network meta-analysis: J Orthop Translat, 2020; 26; 16-30
63. Yang XG, Wang F, He X, Network meta-analysis of knee outcomes following anterior cruciate ligament reconstruction with various types of tendon grafts: Int Orthop, 2020; 44(2); 365-80
Figures
Figure 1. PRISMA Flow Diagram.Figure 2. Structure of network formed by interventions. The lines between treatment nodes indicate the direct comparisons made with evidences, the size of nodes indicate the number of participants involved in each treatment. Numbers (n/n) with a blue frame near the line indicate ‘number of trials/number of participants’ of the related treatment group, numbers (n/n) with a red frame near the line indicate ‘number of trials/number of participants’ of the related comparisons. (A) Main network meta-analysis. (B) Subgroup analysis. (Made with Stata/MP, version 14.0, manufacturer Stata Corp.).Figure 3. Publication bias and Egger’s test for main networks. (A) Subjective improvement. (B) Functional improvement. (C) Activity recovery. (D) Postoperative laxity. (E) Failure rate.Figure 4. Cluster-rank plots. (A) The cluster-rank plot of subjective improvement and failure rate from main network analyses. (B) The cluster-rank plot of functional improvement and failure rate from main network analyses. (C) The cluster-rank plot of activity recovery and failure rate from main network analyses. (D) The cluster-rank plot of subjective improvement and failure rate from subgroup analyses. (E) The cluster-rank plot of functional improvement and failure rate from subgroup analyses. (F) The cluster-rank plot of activity recovery and failure rate from subgroup analyses. (The cluster-rank value is the product of the abscissa and ordinate of each treatment.)Figure 5. Forest plots of network comparisons of main network meta-analysis (made with Microsoft Excel, version 2019MSO).Figure 6. Forest plots incorporated direct comparisons and indirect comparisons of main network meta-analysis. (A) Subjective improvement. (B) Functional improvement. (C) Activity recovery. (D) Postoperative laxity. (E) Failure rate. (A or 1: Autograft; B or 2: Allograft with irradiation; C or 3: Allograft without irradiation; D or 4: Hybrid graft; E or 5: Repair with augmentation; F or 6: Repair without augmentation).Figure 7. Forest plots of network comparisons of subgroup network meta-analysis (made with Microsoft Excel, version 2019MSO).Figure 8. Forest plots incorporated direct comparisons and indirect comparisons of subgroup analysis. (A) Subjective improvement. (B) Functional improvement. (C) Activity recovery. (D) Postoperative laxity. (E) Failure rate. (A or 1: Autograft; B or 2: Allograft with irradiation; C or 3: Allograft without irradiation; D or 4: Hybrid graft; E or 5: Repair with augmentation; F or 6: Repair without augmentation.). Tables
Table 1. Baseline characteristics of included studies.Table 2. Methodological quality and risk of bias evaluation of randomized controlled studies.Table 3. Methodological quality and risk of bias evaluation of non-randomized control and cohort design studies.Table 4. The league plots of subjective improvement. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, WMD with 95% CI).Table 5. The league plots of functional improvement. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, SMD with 95% CI).Table 6. The league plots of activity recovery. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, WMD with 95% CI).Table 7. The league plots of postoperative laxity. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, SMD with 95% CI).Table 8. The league plots of failure rate. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, RR with 95% CI).Table 9. Detailed results of main network analysis.Table 10. Detailed results of subgroup analysis.Table 11. The detailed results of direct pair-wise meta-analyses between primary repair (PR) with augmentation and anterior cruciate ligament reconstruction (ACLR).Table 12. The detailed results of direct pair-wise meta-analyses between primary repair (PR) without augmentation and anterior cruciate ligament reconstruction (ACLR).Table 1. Baseline characteristics of included studies.Table 2. Methodological quality and risk of bias evaluation of randomized controlled studies.Table 3. Methodological quality and risk of bias evaluation of non-randomized control and cohort design studies.Table 4. The league plots of subjective improvement. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, WMD with 95% CI).Table 5. The league plots of functional improvement. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, SMD with 95% CI).Table 6. The league plots of activity recovery. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, WMD with 95% CI).Table 7. The league plots of postoperative laxity. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, SMD with 95% CI).Table 8. The league plots of failure rate. Main network analysis (red) and subgroup analysis (blue). (From the top left to the bottom right, higher comparator vs lower comparator, RR with 95% CI).Table 9. Detailed results of main network analysis.Table 10. Detailed results of subgroup analysis.Table 11. The detailed results of direct pair-wise meta-analyses between primary repair (PR) with augmentation and anterior cruciate ligament reconstruction (ACLR).Table 12. The detailed results of direct pair-wise meta-analyses between primary repair (PR) without augmentation and anterior cruciate ligament reconstruction (ACLR). In Press
06 Mar 2024 : Clinical Research
Prevalence and Variation of Medical Comorbidities in Oral Surgery Patients: A Retrospective Study at Jazan ...Med Sci Monit In Press; DOI: 10.12659/MSM.943884
08 Mar 2024 : Clinical Research
Evaluation of Foot Structure in Preschool Children Based on Body MassMed Sci Monit In Press; DOI: 10.12659/MSM.943765
15 Apr 2024 : Laboratory Research
The Role of Copper-Induced M2 Macrophage Polarization in Protecting Cartilage Matrix in OsteoarthritisMed Sci Monit In Press; DOI: 10.12659/MSM.943738
07 Mar 2024 : Clinical Research
Knowledge of and Attitudes Toward Clinical Trials: A Questionnaire-Based Study of 179 Male Third- and Fourt...Med Sci Monit In Press; DOI: 10.12659/MSM.943468
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952