07 May 2023: Database Analysis
Global Research Hotspots and Trends of Physical Activity in Knee Osteoarthritis: A Bibliometric Analysis
Zhijie Zhang1ABCDEG, Wenjing Wang2BCDEF, Yuanchun Zhu2CDE, Jiayi Guo1ACDEG*DOI: 10.12659/MSM.938919
Med Sci Monit 2023; 29:e938919






Abstract
BACKGROUND: Knee osteoarthritis (OA) is a chronic joint disease characterized by pain, swelling, and limited knee activity. Numerous studies have reported the efficacy and mechanism of physical activity in patients with knee OA. However, bibliometric analyses of physical activity and knee OA are rare. This study aimed to discuss the hotspots, frontiers, and trends in physical activity and knee OA research using bibliometric methods to provide valuable information for future research.
MATERIAL AND METHODS: Relevant literature was obtained from the Web of Science Core Collection database from 2000 to 2021. English-language articles and reviews were selected. CiteSpace (6.1.R2), a bibliometric analytical tool, was used to analyze the countries, institutions, journals, authors, keywords, and references.
RESULTS: A total of 860 papers were obtained. Publications and citations have increased over the years. The most productive country, institution, author, and journal were USA, the University of Melbourne, Bennell KL, and Osteoarthritis and Cartilage. The author and journal with the most citations were Fransen M and Osteoarthritis and Cartilage. McAlindon TE et al’s paper had the most citations and the strongest burst. Two references for the latest bursts were published by Fransen M et al. and Bartholdy C et al. The top 4 keywords were “hip,” “knee osteoarthritis,” “pain,” and “older adult.” The keywords for the latest burst were “guideline” and “risk.”
CONCLUSIONS: Over the past 2 decades, research on physical activity in knee OA has received increasing attention. This study identified research hotspots and development trends, providing meaningful information for researchers.
Keywords: Bibliometrics, Exercise, Osteoarthritis, Knee, Humans, Aged, Knee Joint, Pain
Background
Knee osteoarthritis (OA) is a chronic joint disease characterized by pain, swelling, and limited knee activity that tends to occur in the elderly [1]. The prevalence of knee OA increases with age [2]. An estimated 654.1 million individuals worldwide over the age of 40 years suffered from knee OA in 2020 [3]. In addition, knee OA is a common musculoskeletal disorder causing disabilities and reduced quality of life. Globally, knee OA ranked 11th in disability and 38th in disability-adjusted life years among 291 diseases [4]. As the population ages and obesity increases, the challenge of knee OA will continue to worsen. The prevalence of knee OA in the United States has doubled since the mid-20th century [5]. However, knee OA is incurable, and the pathogenesis is unknown. Finding an effective cure to prevent and treat knee OA is necessary and urgent.
Physical activity achieved excellent clinical and economic outcomes in the management of knee OA [6]. The expert consensus states that physical activity is critical for maintaining good health. Increasing physical activity and introducing exercise training programs in inactive older adults can improve multiple physiological systems and their functional capacity [7]. Recently, numerous studies have reported the efficacy and mechanisms of physical activity [8]. The latest guidelines for knee OA recommend that exercises (aerobic, strengthening, and mind-body exercises) are available and harmless, regardless of whether individuals have other comorbidities [9,10]. Meanwhile, previous research has compared the benefits of different types and intensities of knee OA to explore the optimal exercise strategy [11]. Low-intensity aerobic training improves the clinical symptoms of severe knee osteoarthritis, while high-intensity may aggravate the articular cartilage [12].
Knee OA is a severe public health problem with a high prevalence and disability. Recently, physical activity has become a core component of knee OA management. As an effective, economical, and safe way of prevention and treatment, physical activity has attracted more and more attention from researchers and clinicians since the 21st century. Previous studies have performed bibliometric analyses of studies on other interventions in knee OA, such as unicompartmental knee arthroplasty (UKA) and acupuncture therapy [13,14]. However, bibliometric analyses of studies on physical activity in individuals with knee OA are lacking.
Bibliometric analysis refers to the quantitative and comprehensive analysis of literature information (such as authors, countries, institutions, journals, keywords, and references) using mathematics and statistics to determine research hotspots, frontiers, and trends in a particular field [15]. Recently, bibliometric methods have been applied in many areas, such as low back pain, stroke, and cognitive impairment [16–18]. A bibliometric analysis of physical activity in knee OA can show research hotspots and frontiers in the field. This study also can provide directions for further scientific research and a theoretical basis for non-surgical management in clinical practice. It is valuable to analyze research on physical activity and knee OA using bibliometric methods. This study aimed to identify the hotspots and trends in physical activity and knee OA research by bibliometric analysis from 2000 to 2021 and provide valuable information for future research.
Material and Methods
DATA ACQUISITION:
The relevant literature was collected on July 4, 2022. The Science Citation Index Expanded (SCI-EXPANDED) in the Web of Science Core Collection (WoSCC) was selected, which contains the most literature on physical activity and knee OA research. Previous bibliometrics studies have also used this database [19,20]. The search strategies were as follows: PY=(2000–2021) AND DT=(Article OR Review) AND LA=(English) AND TI=(“physical activit*” OR exercise* OR training OR sport* OR kinesitherapy OR fitness OR jog* OR swim* OR run* OR walk* OR pilates* OR yoga OR cycling OR “tai chi” OR qigong) AND TI=(“knee osteoarthritis” OR “knee OA” OR “osteoarthritis of knee” OR “osteoarthritis of the knee”). The search term covered almost all synonyms for “knee osteoarthritis” and “physical activity” [13,21]. Limiting literature to articles and reviews published in English can make it more representative. Title retrieval makes the literature obtained more relevant to the research topic.
ANALYSIS TOOLS:
The CiteSpace 6.1.R2, a Java-based software program, was developed to analyze papers published from 2000 to 2021 using bibliometric methods [22]. The parameters were set as follows: time span=2000–2021, year per slice=1, selection criteria=top50, and pruning=none.
CiteSpace VI converted the format of the imported literature data and then calculated and analyzed publications of authors, countries, institutions, and journals, citations of references, co-occurrences of keywords, and the cooperation between them, and network maps were created. There are 3 main maps: cooperation, co-occurrence, and co-citation maps. Publications, citations, and co-occurrences are represented by nodes. The cooperation is represented by links. The network maps consist of nodes and links. Larger nodes represent more publications and higher citations and co-occurrences. More and thicker links represent closer cooperation between nodes. CiteSpace VI can also analyze the year of contribution and present them in different colors in the figures. The node and link colors represent the differences in the year. The lighter and yellow the nodes and links are, the closer to 2021. The colors farther from the center of the nodes were closer to the recent year. Nodes with high centrality have purple circles around them, indicating that a node is a crucial point in this field [22,23]. In addition, CiteSpace VI can identify citation bursts of keywords and references to explore frontier topics in the field [24]. Microsoft Excel 2010 was used to show the development trends in publications and paper citations over time.
Results
ANALYSIS OF PUBLICATION OUTPUTS AND TRENDS:
In total, 860 papers published between 2000 and 2021 were retrieved, including 766 articles and 94 reviews. The annual output was 39 papers. Figure 1A shows that the number of publications had a general growth trend (from 10 in 2000 to 100 in 2021). The period from 2017 to 2018 saw the fastest growth in the number of publications (67 to 81). There was a brief decline during 3 periods: 2000–2001 (from 10 to 6), 2008–2009 (from 32 to 24), and 2013–2014 (from 47 to 43). The years with the lowest number of publications were 2001 and 2002, when only 6 papers were published annually. The number of publications had increased to 100 by 2021.
As seen in Figure 1B, 860 papers were cited 26 281 times in total from 2000 to 2021. The number of citations also showed a general growth trend (from 3 in 2000 to 3412 in 2021). There was a mild decrease during 2013–2014 (from 1339 to 1312). The model predicted that the number of publications (R=0.9802) and citations (R=0.9866) in this field will gradually increase after 2021.
ANALYSIS OF COUNTRIES AND INSTITUTIONS:
In total, 50 countries and 454 institutions have published 860 papers on physical activity and knee OA research from 2000 to 2021. Table 1 lists the top 10 countries and institutions in terms of their publications.
The most productive country was the USA (254), followed by Australia (114), Canada (104), and China (87), together accounting for 65% of the total published papers (Figure 2A). The country with the highest centrality was the USA (0.39), followed by Australia (0.31), Belgium (0.18), and England (0.14).
Figure 2B shows the cooperation of the institutions; the top 10 institutions were all universities. The University of Melbourne (0.17), University of Sydney (0.08), and University of Southern Denmark (0.07) ranked in the top 3 for centrality. The institutions producing the most publications were the University of Melbourne (60 publications), Boston University (33 publications), and the University of Sydney (30 publications).
ANALYSIS OF JOURNALS AND CO-CITED JOURNALS:
In total, 238 journals published 860 papers on physical activity and knee OA. The top 10 journals produced 302 papers, accounting for approximately 35.12% of the papers (Table 2). The journals with the most publications were Osteoarthritis and Cartilage (55 publications), BMC Musculoskeletal Disorders (49 publications), and Arthritis Care & Research (46 publications). Among the top 10 journals, Osteoarthritis and Cartilage (impact factor [IF] 2021=7.507), Journal of Rheumatology (IF 2021=5.346), and Arthritis Care & Research (IF 2021=5.178) ranked among the top 3 for the IF. The IF ranged from 2.034 to 7.507 among the top 10 journals, with an average of approximately 4.200. The major journals were from England and the USA. The other 4 journals were from the Netherlands, Ireland, Canada, and Germany.
The details of the co-cited journals are presented in Table 3 and Figure 3. In total, 653 co-cited journals were included in the 860 papers published between 2000 and 2021. Osteoarthritis and Cartilage (669 counts), Annals of Rheumatic Diseases (656 counts), and Arthritis and Rheumatism (630 counts) had the most co-citations. The American Journal of Clinical Nutrition ranked first in terms of centrality (0.07).
ANALYSIS OF AUTHORS AND CO-CITED AUTHORS:
A total of 860 papers were published by 621 authors. Figure 4A shows the cooperation map of the authors. The collaboration between the authors was relatively weak and should be strengthened. In terms of publications, Bennell KL and Hinman RS ranked in the top 2, with 52 and 34 articles, respectively. Bennell KL and Hinman RS were from the University of Melbourne, Australia. There were no significant differences in the number of publications among the other authors in the top 10 ranks, ranging from 11 to 16 articles (Table 4). Among the top 10 authors, Bennell KL also had the highest centrality (0.13).
There were 748 co-cited authors in 860 papers. Figure 4B shows a network map of co-cited authors. Fransen M ranked first with 309 co-citations, followed by Bellamy N with 281, Altman R with 246, and Kellgren JH with 245 (Table 4). They were from the Universities of Sydney in Australia, Western Ontario in Canada, Miami in the United States, and Manchester in England. The top 10 co-cited authors had more than 140 co-citations and were reputable researchers in the field of physical activity and knee OA.
ANALYSIS OF REFERENCES:
In total, 939 references were cited in 860 papers. Table 5 shows the points of the top 10 co-cited references. The first paper (103 counts) was published in Osteoarthritis and Cartilage by McAlindon TE et al in 2014, which provided a guideline on knee OA by the OA Research Society International (OARSI). Moreover, it provides proper management strategies for individuals with knee OA, including exercise, education, and weight loss [25]. The second (62 counts) and third (56 counts) papers published by Fransen M et al in 2015 suggested that land-based therapeutic exercises improved the clinical outcomes of knee OA for at least 2–6 months after discontinuation of treatment [26,27].
The references ranked in the top 20 for citation burst strength are listed in Table 6. Each grid represents a year. Red indicated that references were most frequently cited during this period, blue indicated infrequent citations, and light blue indicated no citations. The latest reference by Bartholdy C et al in 2017, in addition to the 2 published by Fransen M et al in 2015 [26,27], was published in Seminars in Arthritis & Rheumatism [28]. McAlindon TE et al published the reference with the strongest citation bursts (30.54) in 2014 [25].
ANALYSIS OF KEYWORDS:
The most frequently used keyword was “hip” (307 times), followed by “knee osteoarthritis” (254 times), “pain” (244 times), “older adult” (220 times), “management” (206 times), “arthritis” (148 times), “physical activity” (144 times), “exercise” (130 times), “disability” (96 times), and “recommendation” (96 times) (Table 7). The co-occurrence network map of the keywords in the 860 papers is shown in Figure 5. There was a strong co-occurrence relationship among the keywords.
Table 8 lists the top 14 keywords with the strongest citation bursts in physical activity and knee OA research from 2000 to 2021. Among these papers, “osteoarthritis” was the strongest citation burst keyword with 9.59. The latest burst keywords were “guideline” (2018–2021) and “risk” (2019–2021).
Discussion
GENERAL INFORMATION FOR PHYSICAL ACTIVITY AND KNEE OA RESEARCH:
We conducted a bibliometric analysis of physical activity and knee OA research by reviewing the papers published between 2000 and 2021. The number of publications and citations in this field has increased significantly since 2000. The extensive attention on physical activity in knee OA may be related to the increasing prevalence of knee OA and popularity of exercise therapy. Seven developed countries were among the top 10 countries that published 658 papers, accounting for 76.5% of the total. The top 10 institutions and journals were all from developed countries. These results show that research on physical activity and knee OA in developing countries was relatively insufficient and requires more attention.
The United States occupied the primary position, had many publications, and established close cooperation with other countries. The most productive and influential institution was the University of Melbourne. The top 10 institutions were all universities, indicating that universities were the backbone of the research field. Osteoarthritis and Cartilage was the most productive and reputable journal on physical activity and knee OA research. Among the top 10 journals, only 3 had an IF >5, accounting for 13.37% of the 860 papers. It was challenging to publish papers in this research area in journals with high impact factors. Bennell KL and Hinman RS were the most productive authors, and often cooperated in providing recommendations for preventing and treating knee OA [29,30].
RESEARCH HOTSPOTS OF PHYSICAL ACTIVITY IN KNEE OA:
The research hotspots were analyzed based on 3 aspects: co-occurrence keywords, co-cited authors, and references. The top 4 keywords that co-occurred frequently were “hip,” “knee osteoarthritis,” “pain,” and “older adult.”
HIP: Hip OA is second in prevalence to knee OA. Studies on knee and hip OA have often been simultaneously reported [4,10,31]. The hip, knee, and ankle are the primary joints that make up lower limb movements, and hip participation is essential for physical activity [32]. Significant hip weakness has been reported in individuals with knee OA [33]. However, there is a lack of prospective studies that determine whether hip strength increases susceptibility to knee OA. Studies have suggested that strengthening the hip muscles benefited the clinical symptoms in individuals with knee OA, but it did not significantly improve the biomechanical measures [34]. In the future, hip muscle strength should be considered when evaluating or developing treatments.
KNEE OSTEOARTHRITIS: Knee OA is a slowly progressing disease. Radiography reveals joint space narrowing and hyperosteogeny [1]. The symptoms of knee OA are not evident early, and some patients experience knee swelling and pain. As the disease progresses, symptoms worsen, and activities are significantly limited. Knee OA has high prevalence and morbidity rates, but there is no known cure [3]. Numerous guidelines have stated that exercise can improve clinical outcomes in individuals with knee OA [9,10,35–38].
PAIN: Recurrent knee pain within the previous month is a diagnostic criterion for knee OA. The medial knee is the most common site of pain. Diffuse pain is commonly felt, associated with higher pain and catastrophizing scores, and lower knee function and pain self-efficacy scores [39]. Individuals with knee OA reportedly have a reduced pain threshold, which may be related to symptom severity [40]. Psychological factors can influence pain in knee OA, and a lower tendency of pain catastrophizing predicts less pain [41]. Additionally, knee adduction and flexion moments were related to pain intensity. The redistribution of mechanical load may be a way to reduce the pain associated with mechanical stimulation [42].
OLDER ADULT: With aging, knee function deteriorates, wear accelerates, and bone hyperplasia and knee OA may occur [43]. Age is a primary risk factor, with the prevalence of knee OA increasing with age [2]. With an aging population, the public health system will face significant challenges.
Among the co-cited authors, Fransen M et al provided recommendations for exercise in knee OA [26,27]. Bellamy N et al performed a validation study of the WOMAC scale to assess relevant clinical outcomes in hip or knee OA [44]. Altman R et al proposed criteria for the diagnosis of idiopathic knee OA. Specificity and sensitivity have also been reported [45]. Kellgren JH et al proposed a radiological assessment of OA and suggested that X-rays should be read by the same observer or preferably by 2 observers in consultation [46].
According to the top 10 co-cited references, 8 guidelines were used for treating knee OA. They suggested that exercise significantly improves the clinical outcomes of knee OA [10,25–27,31,47–49]. The fourth article compared the differences in the improvement of knee OA according to different exercise types and intensities, program length, and number of sessions per week. The meta-analysis results indicated that the optimal motion scheme for knee OA should focus on improving aerobic capacity, quadriceps strength, or lower limb movement ability. The program worked best when performed 3 times per week [50]. The ninth most co-cited reference reported the global incidence and prevalence of hip and knee OA according to age and sex in 2010 [4].
RESEARCH TRENDS OF PHYSICAL ACTIVITY IN KNEE OA:
Keyword bursts reflect the research frontiers of a field in a certain period. We identified the latest frontier topics on physical activity and knee OA research by analyzing the latest keyword bursts.
GUIDELINE: The latest non-surgical guidelines from the OARSI recommend that structured land-based exercises (strengthening, cardiovascular, balance, and neuromuscular exercises) and mind-body exercises (tai chi and yoga) are vital in treating knee OA, but these guidelines do not suggest any particular exercise. In addition, aquatic exercises are expensive and less acceptable, leading to a conditional recommendation [10]. The European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) guidelines suggest that combining pharmacological and non-pharmacological methods was the key to managing knee OA. However, they did not follow different exercise patterns when making recommendations [9,51]. The European League Against Rheumatism (EULAR) guidelines recommend that physical activity (cardiorespiratory fitness, muscle strength, flexibility, and neuromotor performance) is crucial for the management of knee OA [35,52]. The Ottawa panel clinical practice guidelines recommend that mind-body, aerobic, or strengthening exercises alone or in combination can effectively improve clinical outcomes in individuals with knee OA [36–38].
RISK: Knee OA usually takes decades to develop and has many relevant risk factors, such as obesity, joint injury, and female sex [53]. Knee extensor weakness also increases the risk of knee OA [54]. Advanced interventions in high-risk individuals can significantly reduce their prevalence. Maintaining physical activity in midlife reportedly has a small impact on knee biomechanics, leading to a more stable loading environment for the knee, and, subsequently, a long-term reduction in the risk of knee OA [55]. Physical activity can also reduce cardiovascular and metabolic risks in individuals with knee OA [56]. Moreover, individuals with knee OA are at a high risk of falling. Many studies have shown that balance training can significantly reduce the risk of falls [57].
References that include the latest citation bursts are also an indicator of the research frontier. The latest burst reference by Fransen M et al provided a comprehensive analysis of the exercise benefits in knee OA [26,27]. These suggested that land-based therapeutic exercise improved the clinical outcomes of knee OA for at least 2–6 months after discontinuation of treatment. Bartholdy C et al compared muscle strengthening with other exercises for knee OA [28]; muscle strengthening was found to be more effective in improving knee extensor strength but did not provide superior clinical outcomes. An increase of less than 30% in knee extensor strength is unlikely to improve clinical outcomes in pain and disability.
STRENGTHS AND LIMITATIONS:
This study is the first to explore hotspots and trends in physical activity and knee OA research from 2000 to 2021. We conducted a scientific and comprehensive analysis of the keywords, references, journals, institutions, authors, and countries. However, this study has some limitations. First, some high-impact or high-quality papers may have been omitted. Only articles or reviews were included in this study. Literature was obtained only from the WoSCC database. Only manuscripts written in English were included. Although we have tried to cover all the search terms when formulating the search formula, it is still possible to exclude a few synonyms, which led to omission of some studies. In addition, there could be some inaccuracies in the authors and co-cited authors because only the abbreviated author’s name was extracted from the WoSCC database.
Conclusions
This study performed a bibliometric analysis and found hotspots and trends in physical activity and knee OA research between 2000 and 2021. Further research on physical activity and knee OA will receive more attention in the future. The most influential journals, authors, institutions, and countries were Osteoarthritis and Cartilage, Bennell KL, the University of Melbourne, and USA, respectively. “Hip,” “knee osteoarthritis,” “pain,” and “older adult” were the hot keywords. “Guideline” and “risk” were the latest frontier keywords. In conclusion, this study describes the status and developmental trends in physical activity and knee OA research, providing valuable information for future studies.
Figures
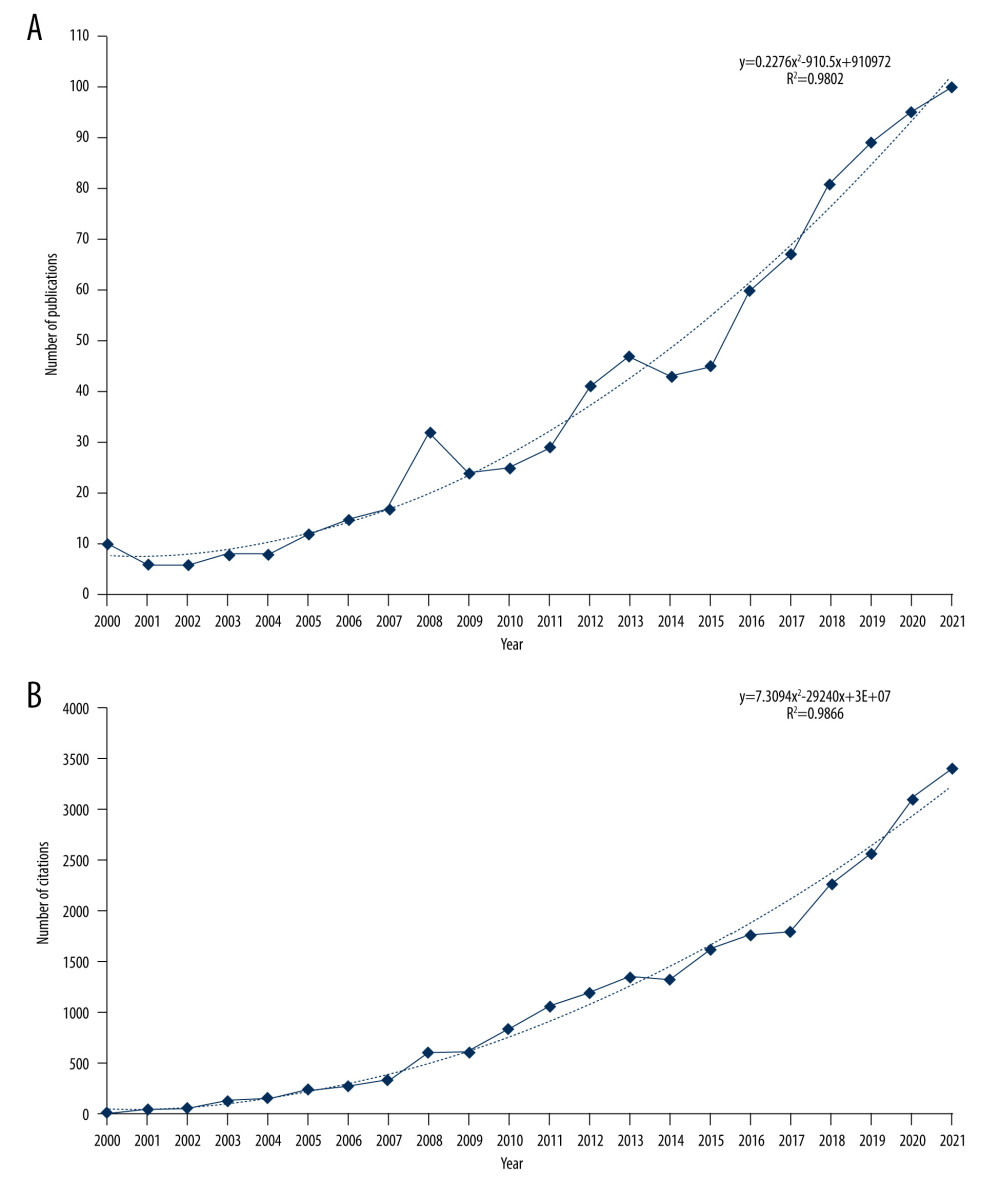 Figure 1. The number of annual (A) publications and (B) citations on physical activity and knee osteoarthritis (OA) research from 2000 to 2021. (Office Excel 2010, Microsoft).
Figure 1. The number of annual (A) publications and (B) citations on physical activity and knee osteoarthritis (OA) research from 2000 to 2021. (Office Excel 2010, Microsoft). 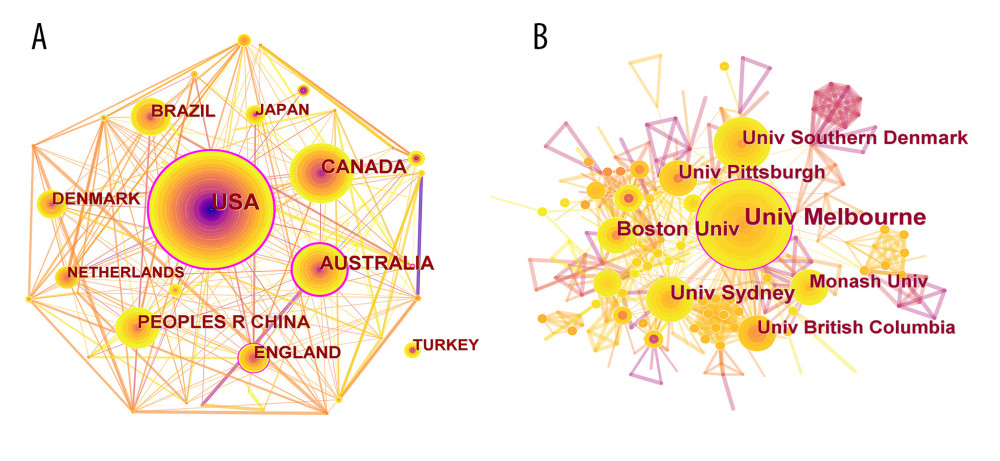 Figure 2. Cooperation map of (A) countries and (B) institutions with publications on physical activity and knee OA research from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA).
Figure 2. Cooperation map of (A) countries and (B) institutions with publications on physical activity and knee OA research from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA). 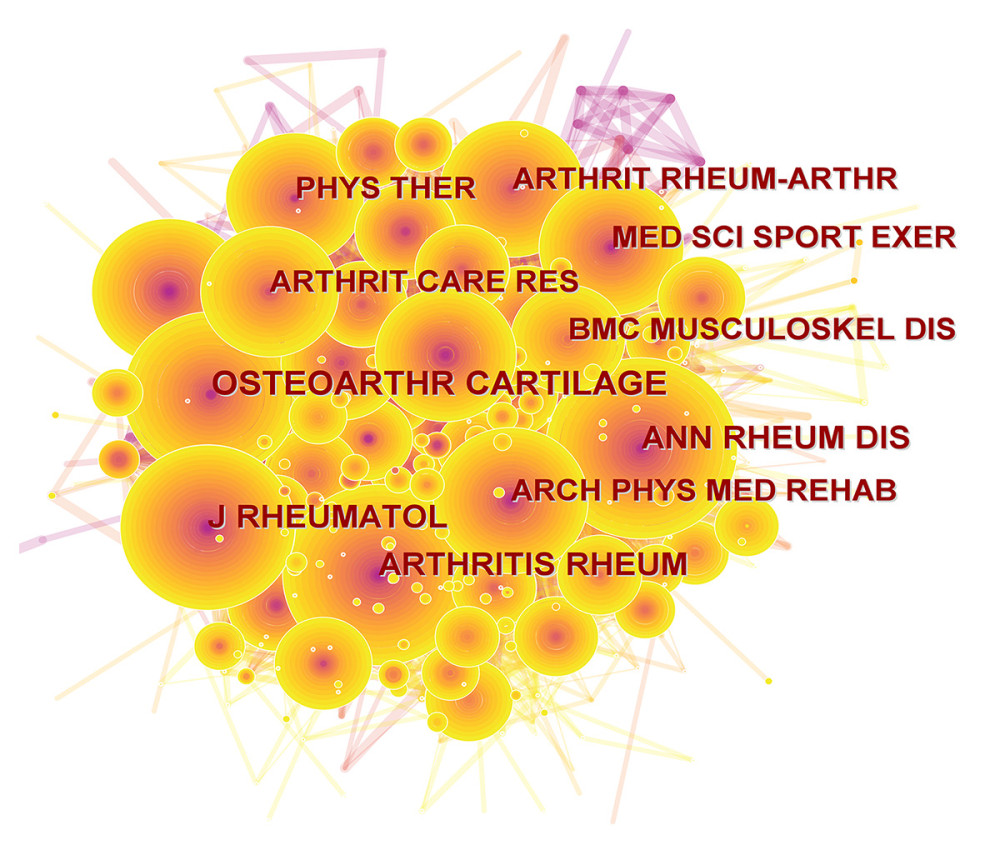 Figure 3. Map of cited journals on physical activity and knee OA research from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA).
Figure 3. Map of cited journals on physical activity and knee OA research from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA). 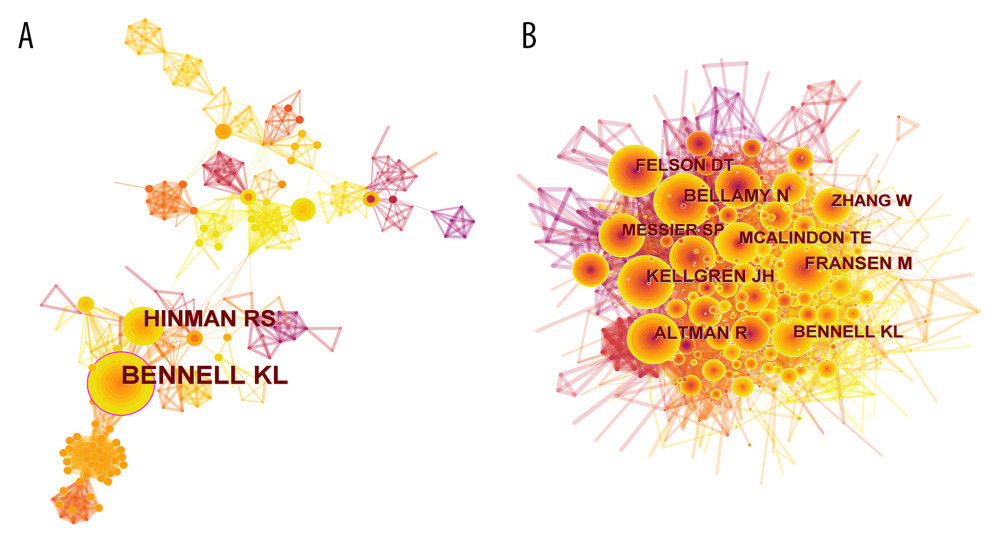 Figure 4. Cooperation map of (A) authors and (B) co-cited authors on physical activity and knee OA research from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA).
Figure 4. Cooperation map of (A) authors and (B) co-cited authors on physical activity and knee OA research from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA). 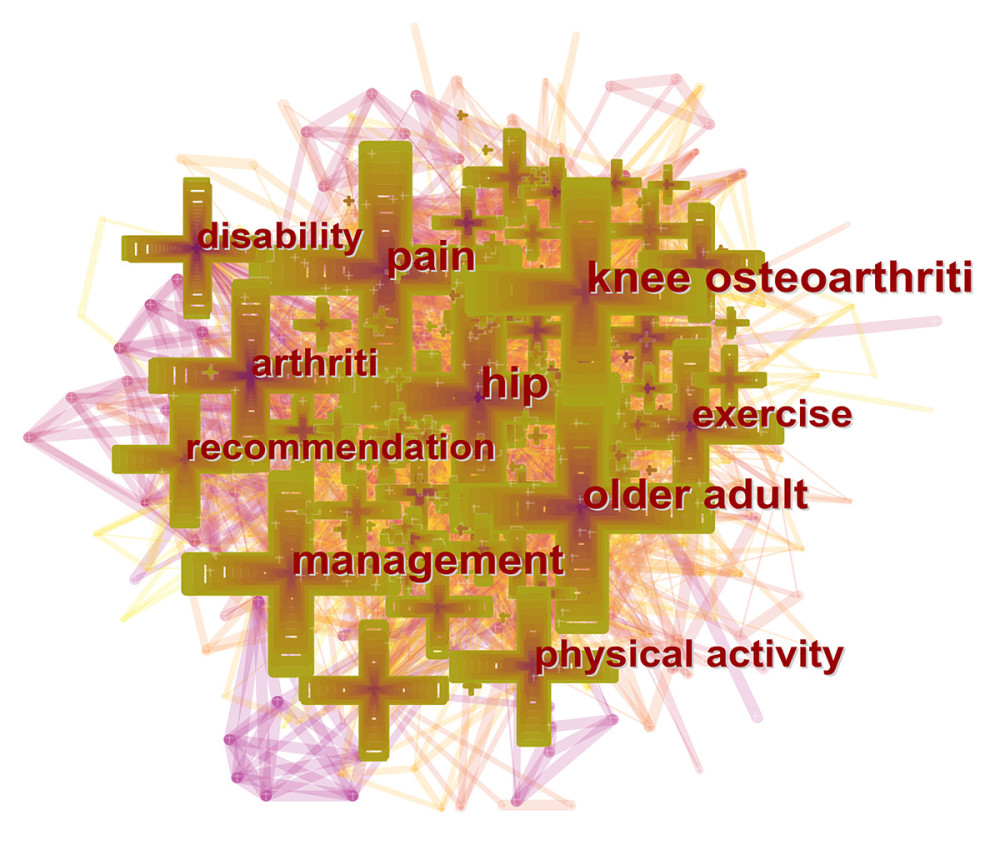 Figure 5. Map of the co-occurrence keywords with publications from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA).
Figure 5. Map of the co-occurrence keywords with publications from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA). Tables
Table 1. Top 10 countries and institutions in terms of publications from 2000 to 2021.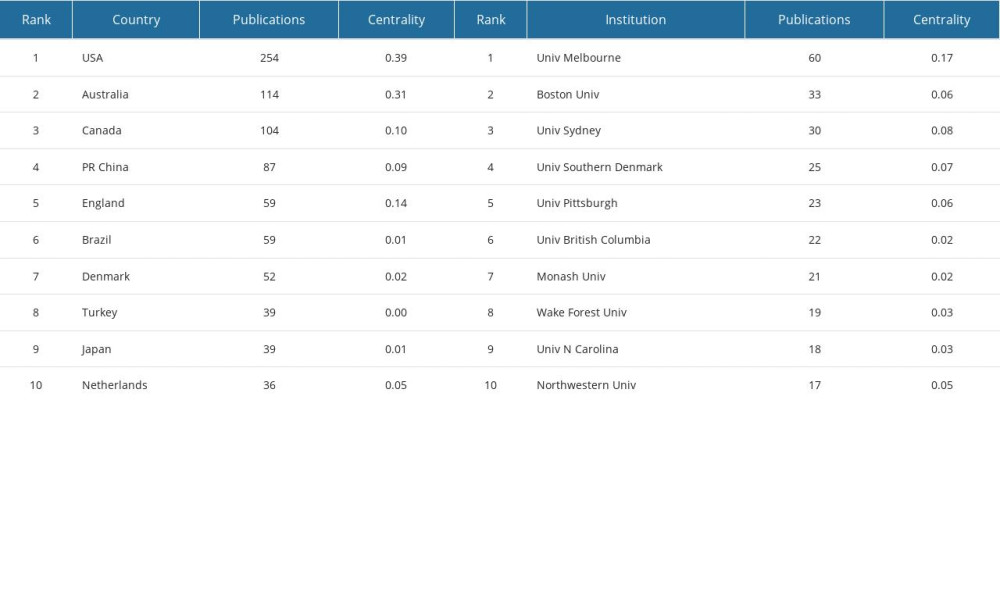 Table 2. Top 10 journals in terms of publications from 2000 to 2021.
Table 2. Top 10 journals in terms of publications from 2000 to 2021.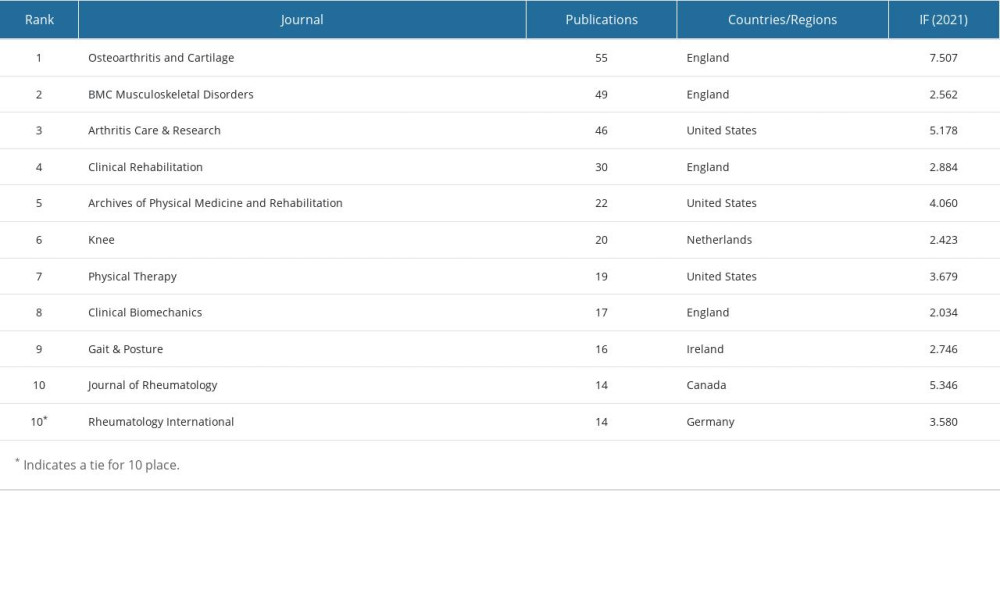 Table 3. Top 10 co-cited journals in terms of co-citations and centrality from 2000 to 2021.
Table 3. Top 10 co-cited journals in terms of co-citations and centrality from 2000 to 2021.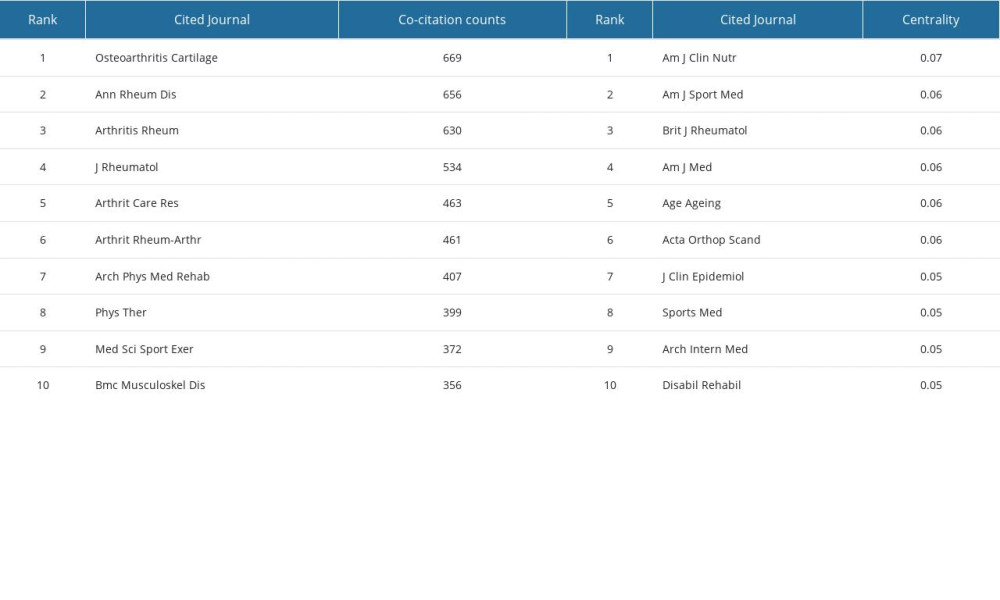 Table 4. Top 10 authors and co-cited authors on physical activity and knee osteoarthritis (OA) research from 2000 to 2021.
Table 4. Top 10 authors and co-cited authors on physical activity and knee osteoarthritis (OA) research from 2000 to 2021.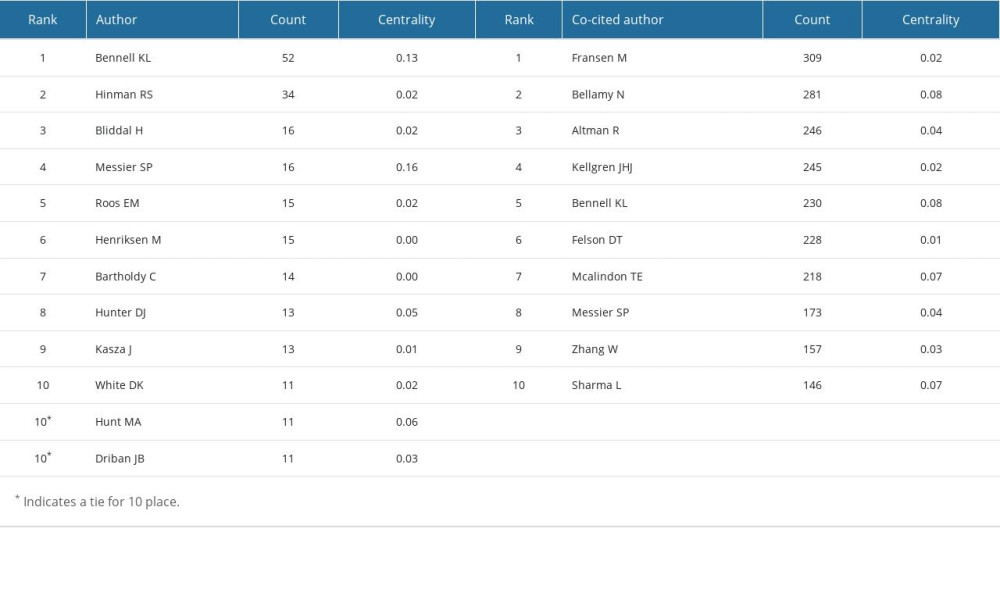 Table 5. Top 10 co-cited references in terms of co-citations from 2000 to 2021.
Table 5. Top 10 co-cited references in terms of co-citations from 2000 to 2021.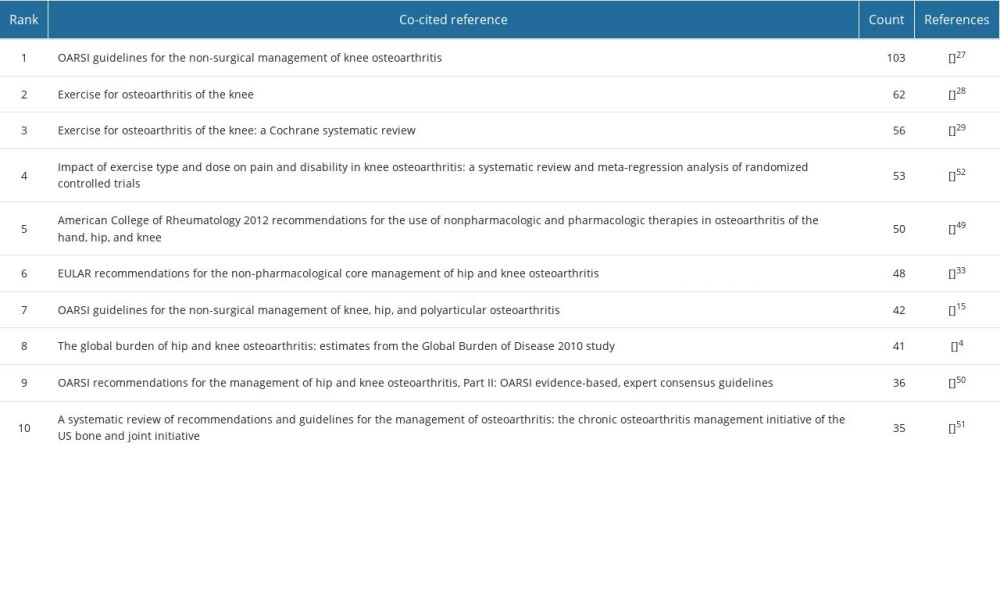 Table 6. Top 20 references with the strongest citation bursts.
Table 6. Top 20 references with the strongest citation bursts. Table 7. Top 10 keywords in terms of frequency and centrality from 2000 to 2021.
Table 7. Top 10 keywords in terms of frequency and centrality from 2000 to 2021.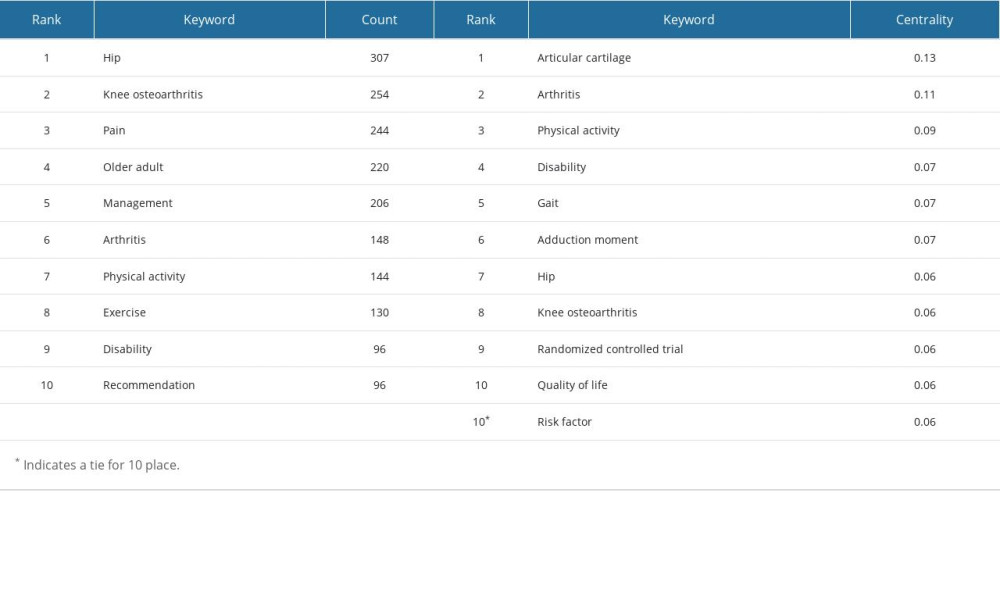 Table 8. Top 14 keywords with the strongest citation bursts.
Table 8. Top 14 keywords with the strongest citation bursts.
References
1. Lespasio MJ, Piuzzi NS, Husni ME, Knee osteoarthritis: A primer: Perm J, 2017; 21; 16-83
2. Prieto-Alhambra D, Judge A, Javaid MK, Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: influences of age, gender and osteoarthritis affecting other joints: Ann Rheum Dis, 2014; 73(9); 1659-64
3. Cui A, Li H, Wang D, Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies: EClinicalMedicine, 2020; 29-30; 100587
4. Cross M, Smith E, Hoy D, The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study: Ann Rheum Dis, 2014; 73(7); 1323-30
5. Wallace IJ, Worthington S, Felson DT: Proc Natl Acad Sci USA, 2017; 114(35); 9332-36
6. Silva GS, Sullivan JK, Katz JN, Long-term clinical and economic outcomes of a short-term physical activity program in knee osteoarthritis patients: Osteoarthritis Cartilage, 2020; 28(6); 735-43
7. Bangsbo J, Blackwell J, Boraxbekk CJ, Copenhagen Consensus statement 2019: Physical activity and ageing: Br J Sports Med, 2019; 53(14); 856-58
8. Zeng CY, Zhang ZR, Tang ZM, Hua FZ, Benefits and mechanisms of exercise training for knee osteoarthritis: Front Physiol, 2021; 12; 794062
9. Bruyere O, Honvo G, Veronese N, An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO): Semin Arthritis Rheum, 2019; 49(3); 337-50
10. Bannuru RR, Osani MC, Vaysbrot EE, OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis: Osteoarthritis Cartilage, 2019; 27(11); 1578-89
11. Regnaux JP, Lefevre-Colau MM, Trinquart L, High-intensity versus low-intensity physical activity or exercise in people with hip or knee osteoarthritis: Cochrane Database Syst Rev, 2015; 2015(10); CD010203
12. Messier SP, Mihalko SL, Beavers DP, Effect of high-intensity strength training on knee pain and knee joint compressive forces among adults with knee osteoarthritis: The START randomized clinical trial: JAMA, 2021; 325(7); 646-57
13. Li R, Sun J, Hu H, Research trends of acupuncture therapy on knee osteoarthritis from 2010 to 2019: A bibliometric analysis: J Pain Res, 2020; 13; 1901-13
14. Liu P, Zhang C, Lu Z, Global research status and trends of UKA for knee osteoarthritis: A bibliometric analysis: Arthroplasty, 2020; 2(1); 20
15. Donthu N, Kumar S, Mukherjee D, How to conduct a bibliometric analysis: An overview and guidelines: J Bus Res, 2021; 133; 285-96
16. Dong Y, Weng L, Hu Y, Exercise for stroke rehabilitation: A bibliometric analysis of global research from 2001 to 2021: Front Aging Neurosci, 2022; 14; 876954
17. Serrano-Pozo A, Aldridge GM, Zhang Q, Four decades of research in Alzheimer’s disease (1975–2014): A bibliometric and scientometric analysis: J Alzheimers Dis, 2017; 59(2); 763-83
18. Liang YD, Li Y, Zhao J, Study of acupuncture for low back pain in recent 20 years: A bibliometric analysis via CiteSpace: J Pain Res, 2017; 10; 951-64
19. Li W, Weng L, Xiang Q, Fan T, Trends in research on traditional Chinese health exercises for improving cognitive function: A bibliometric analysis of the literature from 2001 to 2020: Front Public Health, 2021; 9; 794836
20. You Y, Wang D, Wang Y, A bird’s-eye view of exercise intervention in treating depression among teenagers in the last 20 years: A bibliometric study and visualization analysis: Front Psychiatry, 2021; 12; 661108
21. Zhang Z, Zhu Y, Wang Q, Global trends and research hotspots of exercise for intervening diabetes: A bibliometric analysis: Front Public Health, 2022; 10; 902825
22. Chen C, CiteSpace II: Detecting and visualizing emerging trends and transient patterns in scientific literature: J Am Soc Inf Sci Technol, 2006; 57(3); 359-77
23. Chen C, Dubin R, Kim MC, Emerging trends and new developments in regenerative medicine: A scientometric update (2000–2014): Expert Opin Biol Ther, 2014; 14(9); 1295-317
24. Wu H, Wang Y, Tong L, Global research trends of ferroptosis: A rapidly evolving field with enormous potential: Front Cell Dev Biol, 2021; 9; 646311
25. McAlindon TE, Bannuru RR, Sullivan MC, OARSI guidelines for the non-surgical management of knee osteoarthritis: Osteoarthritis Cartilage, 2014; 22(3); 363-88
26. Fransen M, McConnell S, Harmer AR, Exercise for osteoarthritis of the knee: Cochrane Database Syst Rev, 2015; 2015; CD004376
27. Fransen M, McConnell S, Harmer AR, Exercise for osteoarthritis of the knee: A Cochrane systematic review: Br J Sports Med, 2015; 49(24); 1554-57
28. Bartholdy C, Juhl C, Christensen R, The role of muscle strengthening in exercise therapy for knee osteoarthritis: A systematic review and meta-regression analysis of randomized trials: Semin Arthritis Rheum, 2017; 47(1); 9-21
29. Bennell KL, Hunt MA, Wrigley TV, Muscle and exercise in the prevention and management of knee osteoarthritis: An internal medicine specialist’s guide: Med Clin N Am, 2009; 93(1); 161-77
30. Bennell KL, Wrigley TV, Hunt MA, Update on the role of muscle in the genesis and management of knee osteoarthritis: Rheum Dis Clin North Am, 2013; 39(1); 145-76
31. Fernandes L, Hagen KB, Bijlsma JW, EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis: Ann Rheum Dis, 2013; 72(7); 1125-35
32. Schlenk EA, Fitzgerald GK, Rogers JC, Promoting physical activity in older adults with knee osteoarthritis and hypertension: A randomized controlled trial: J Aging Phys Act, 2021; 29(2); 207-18
33. Deasy M, Leahy E, Semciw AI, Hip strength deficits in people with symptomatic knee osteoarthritis: A systematic review with meta-analysis: J Orthop Sports Phys Ther, 2016; 46(8); 629-39
34. Raghava Neelapala YV, Bhagat M, Shah P, Hip muscle strengthening for knee osteoarthritis: a systematic review of literature: J Geriatr Phys Ther, 2020; 43(2); 89-98
35. Rausch Osthoff AK, Niedermann K, Braun J, 2018 EULAR recommendations for physical activity in people with inflammatory arthritis and osteoarthritis: Ann Rheum Dis, 2018; 77(9); 1251-60
36. Brosseau L, Taki J, Desjardins B, The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis. Part one: Introduction, and mind-body exercise programs: Clin Rehabil, 2017; 31(5); 582-95
37. Brosseau L, Taki J, Desjardins B, The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis. Part three: Aerobic exercise programs: Clin Rehabil, 2017; 31(5); 612-24
38. Brosseau L, Taki J, Desjardins B, The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis. Part two: Strengthening exercise programs: Clin Rehabil, 2017; 31(5); 596-611
39. Nian XY, He Y, Ji YR, Associations between pain patterns and self-reported clinical outcomes in patients with knee osteoarthritis: Pain Med, 2019; 20(4); 818-25
40. Fingleton C, Smart K, Moloney N, Fullen BM, Doody C, Pain sensitization in people with knee osteoarthritis: A systematic review and meta-analysis: Osteoarthritis Cartilage, 2015; 23(7); 1043-56
41. Helminen EE, Sinikallio SH, Valjakka AL, Determinants of pain and functioning in knee osteoarthritis: A one-year prospective study: Clin Rehabil, 2016; 30(9); 890-900
42. Huang C, Chan PK, Chiu KY, Exploring the relationship between pain intensity and knee moments in participants with medial knee osteoarthritis: A cross-sectional study: Bmc Musculoskel Dis, 2021; 22(1); 9
43. Rezus E, Burlui A, Cardoneanu A, From pathogenesis to therapy in knee osteoarthritis: Bench-to-bedside: Int J Mol Sci, 2021; 22(5); 2697
44. Bellamy N, Buchanan WW, Goldsmith CH, Validation-study of WOMAC – a health-status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug-therapy in patients with osteo-arthritis of the hip or knee: J Rheumatol, 1988; 15(12); 1833-40
45. Altman R, Asch E, Bloch D, Development of criteria for the classification and reporting of osteoarthritis – classification of osteoarthritis of the knee: Arthritis Rheum, 1986; 29(8); 1039-49
46. Kellgren JH, Lawrence JS, Radiological assessment of osteo-arthrosis: Ann Rheum Dis, 1957; 16(4); 494-502
47. Hochberg MC, Altman RD, April KT, American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee: Arthritis Care Res (Hoboken), 2012; 64(4); 465-74
48. Zhang W, Moskowitz RW, Nuki G, OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines: Osteoarthritis Cartilage, 2008; 16(2); 137-62
49. Nelson AE, Allen KD, Golightly YM, A systematic review of recommendations and guidelines for the management of osteoarthritis: The Chronic Osteoarthritis Management Initiative of the US Bone and Joint Initiative: Semin Arthritis Rheum, 2014; 43(6); 701-12
50. Juhl C, Christensen R, Roos EM, Zhang W, Lund H, Impact of exercise type and dose on pain and disability in knee osteoarthritis: A systematic review and meta-regression analysis of randomized controlled trials: Arthritis Rheumatol, 2014; 66(3); 622-36
51. Arden NK, Perry TA, Bannuru RR, Non-surgical management of knee osteoarthritis: Comparison of ESCEO and OARSI 2019 guidelines: Nat Rev Rheumatol, 2021; 17(1); 59-66
52. Bull FC, Al-Ansari SS, Biddle S, World Health Organization 2020 guidelines on physical activity and sedentary behaviour: Br J Sports Med, 2020; 54(24); 1451-62
53. Silverwood V, Blagojevic-Bucknall M, Jinks C, Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis: Osteoarthritis Cartilage, 2015; 23(4); 507-15
54. Oiestad BE, Juhl CB, Eitzen I, Thorlund JB, Knee extensor muscle weakness is a risk factor for development of knee osteoarthritis. A systematic review and meta-analysis: Osteoarthritis Cartilage, 2015; 23(2); 171-77
55. Hafer JF, Kent JA, Boyer KA, Physical activity and age-related biomechanical risk factors for knee osteoarthritis: Gait Posture, 2019; 70; 24-29
56. de Almeida AC, Aily JB, Pedroso MG, Reductions of cardiovascular and metabolic risk factors after a 14-week periodized training model in patients with knee osteoarthritis: A randomized controlled trial: Clin Rheumatol, 2021; 40(1); 303-14
57. Lee PA, Liu HC, Chen TY, Recovery of balance control in bilateral medial knee osteoarthritis after total knee arthroplasty during level walking: J Orthop Res, 2022; 40(9); 1993-2003
Figures
Figure 1. The number of annual (A) publications and (B) citations on physical activity and knee osteoarthritis (OA) research from 2000 to 2021. (Office Excel 2010, Microsoft).Figure 2. Cooperation map of (A) countries and (B) institutions with publications on physical activity and knee OA research from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA).Figure 3. Map of cited journals on physical activity and knee OA research from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA).Figure 4. Cooperation map of (A) authors and (B) co-cited authors on physical activity and knee OA research from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA).Figure 5. Map of the co-occurrence keywords with publications from 2000 to 2021. (CiteSpace 6.1.R2, Drexel University, Philadelphia, USA). Tables
Table 1. Top 10 countries and institutions in terms of publications from 2000 to 2021.Table 2. Top 10 journals in terms of publications from 2000 to 2021.Table 3. Top 10 co-cited journals in terms of co-citations and centrality from 2000 to 2021.Table 4. Top 10 authors and co-cited authors on physical activity and knee osteoarthritis (OA) research from 2000 to 2021.Table 5. Top 10 co-cited references in terms of co-citations from 2000 to 2021.Table 6. Top 20 references with the strongest citation bursts.Table 7. Top 10 keywords in terms of frequency and centrality from 2000 to 2021.Table 8. Top 14 keywords with the strongest citation bursts.Table 1. Top 10 countries and institutions in terms of publications from 2000 to 2021.Table 2. Top 10 journals in terms of publications from 2000 to 2021.Table 3. Top 10 co-cited journals in terms of co-citations and centrality from 2000 to 2021.Table 4. Top 10 authors and co-cited authors on physical activity and knee osteoarthritis (OA) research from 2000 to 2021.Table 5. Top 10 co-cited references in terms of co-citations from 2000 to 2021.Table 6. Top 20 references with the strongest citation bursts.Table 7. Top 10 keywords in terms of frequency and centrality from 2000 to 2021.Table 8. Top 14 keywords with the strongest citation bursts. In Press
05 Mar 2024 : Clinical Research
Role of Critical Shoulder Angle in Degenerative Type Rotator Cuff Tears: A Turkish Cohort StudyMed Sci Monit In Press; DOI: 10.12659/MSM.943703
06 Mar 2024 : Clinical Research
Comparison of Outcomes between Single-Level and Double-Level Corpectomy in Thoracolumbar Reconstruction: A ...Med Sci Monit In Press; DOI: 10.12659/MSM.943797
21 Mar 2024 : Meta-Analysis
Economic Evaluation of COVID-19 Screening Tests and Surveillance Strategies in Low-Income, Middle-Income, a...Med Sci Monit In Press; DOI: 10.12659/MSM.943863
10 Apr 2024 : Clinical Research
Predicting Acute Cardiovascular Complications in COVID-19: Insights from a Specialized Cardiac Referral Dep...Med Sci Monit In Press; DOI: 10.12659/MSM.942612
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952