21 June 2023: Clinical Research
Plantar Pressure Distribution and Posture Balance During Walking in Individuals with Unilateral Chronic Ankle Instability: An Observational Study
Dong-ping Wan1CDEF, Huan-li Bao1BEF, Jian-peng Wang1BD, Jie Wei2C, Jian-bing Ma1E, Shu-xin Yao1AEG*, Chao Xu1ADEFGDOI: 10.12659/MSM.940252
Med Sci Monit 2023; 29:e940252






Abstract
BACKGROUND: Patients with chronic ankle instability (CAI) can present with abnormal gait. The purpose of this study was to evaluate plantar pressure distributions and posture balance during walking in unilateral CAI patients.
MATERIAL AND METHODS: We recruited 24 unilateral CAI patients and 24 healthy individuals; plantar pressure analysis was conducted using the Footscan® 3D pressure system. The following parameters were assessed and recorded: peak force/weight (PF/W), time to peak force (TPF), time to boundary (TTB), and COP velocity. The differences between the affected and unaffected side of the CAI group and control group were determined. Pearson correlation analysis and univariate analysis was used to investigate the correlation between plantar pressure parameters and related factors.
RESULTS: The comparison of PF/W showed that the plantar pressure of both sides in the CAI group were laterally distributed. The comparison of TPF, TTB, and COP velocity in different groups showed that the posture balance on the affected side of CAI patient was more impaired than the unaffected side and the control group. Male patients with CAI tend to have better posture balance than females, and a low CAIT score is correlated with poor posture balance.
CONCLUSIONS: The plantar pressure on both sides in unilateral CAI patients was laterally distributed and their balance function was impaired. It is necessary for CAI patients to receive functional training of both sides during rehabilitation, and plantar pressure analysis is promising for diagnosis and evaluation of CAI.
Keywords: Ankle Injuries, gait analysis, Musculoskeletal Physiological Phenomena, Physical Functional Performance, postural balance, Female, Humans, Male, Ankle, Ankle Joint, Chronic Disease, Walking, Joint Instability
Background
Lateral ankle sprain (LAS) is an extremely common musculoskeletal injury and more than 23 000 LAS have been estimated to occur per day [1]. Unfortunately, many patients who sustain a LAS have not received appropriate treatment. About 55% to 72% of them have residual symptoms, including pain, weakness, crepitus, instability, swelling, and stiffness, and are considered to have a subsequent pathology known as chronic ankle instability (CAI) [2]. This condition is manifested as the disorder of random control of joint movement, which leads to long-term symptoms including pain, sense of instability, and frequent sprains of the ankle joint [3]. However, through physical and radiological examination, there is no obvious damage to static stable structures such as ligaments around the joint, nor the range of motion [3,4].
The mechanics at the foot and ankle are largely responsible for the development of CAI, the position of the foot at ground contact has also been suggested to play a role in sprain frequency [4]. Previous studies have identified increased adduction-supination of the foot in those with CAI during walking [5], and their balance function is also impaired due to deficits in proprioception and neuromuscular function [6]. Plantar pressure analysis can provide detailed information about the foot loading patterns during the whole gait cycle [7], and the variability of the center of pressure (COP) has been used extensively for stability assessments during walking [8], which shows great promise in the diagnosis and treatment of CAI. Previous investigations have evaluated differences in plantar pressure distribution between CAI patients and uninjured controls [6,9,10], but the unaffected sides of subjects with unilateral CAI have not been included in comparisons. It is yet to be determined if the unaffected side of unilateral CAI patient utilizes different plantar pressure distribution at the foot and ankle than in uninjured controls.
The purpose of this study was to identify differences in plantar pressure distributions and COP patterns during a walking gait between the unaffected side and the affected side of unilateral CAI patients, and we recruited uninjured individuals as a normal control group. It was hypothesized that the affected side of patients with unilateral CAI would demonstrate a laterally distributed plantar pressure during walking and a poor posture balance when compared to the unaffected side and to normal controls. Furthermore, the mechanism of these differences should be investigated to provide theoretical support and a mechanical index for the diagnosis of patients with unilateral CAI.
Material and Methods
STUDY DESIGN:
This study was designed as an observational study in a laboratory environment to compare variables of plantar pressure for CAI and healthy subjects during treadmill walking. All study subjects provided informed consent, and the study protocol was approved by our institutional review board. A priori power analysis (α=0.05, β=0.20) was conducted using GPower 3.0© software to determine the sample size, and a sample size of 19 in each group was estimated based on an unpublished pilot study as well as a review of previous research [6,9,10].
SUBJECTS:
Between April 2019 and March 2022, patients who were diagnosed with unilateral CAI by our institution according to the method described in a previously published study [11] were included in the present study. The inclusion criteria were as follows: (a) age 18 to 50 years old; (b) History of at least 1 unilateral LAS that occurred no less than 1 years prior to the recruitment; (c) Self-reported instability on ankle joint or sense of lose control in the previous 6 months; (d) Cumberland ankle instability tool (CAIT) [12] scores <24; (e) No history of lower-limb surgery or fracture; (f) No complaints of dysfunctions on the other ankle; and (g) No positive result was found by clinical examination. The exclusion criteria were as follows: (a) Diseases affecting the lower extremities, such as hip or knee osteoarthritis; (b) Diseases limiting activities of daily living, such as cardiopulmonary insufficiency; (c) History of LAS within 1 months before the recruitment; and (d) Other conditions that could affect gait and balance control, such as vestibular dysfunction.
A group of age-matched normal individuals was recruited as the control group, who had no previous history of injury, surgery, or musculoskeletal diseases. All subjects were physically fit enough to participate in a dynamic plantar pressure analysis based on results of the Physical Activity Readiness Questionnaire.
INSTRUMENTATION:
Plantar pressure was measured using the Footscan® 3D pressure system (RSscan International®, Belgium) at a sampling frequency of 125 Hz, including a data processing box and a force plate, which has 40 960 resistive sensors distributed in a 256×64 matrix. The minimum measurement area was 0.25 cm2, and the pressure sensitivity ranged from 0 to 200 N/cm2. The 2.00×0.40×0.02 m force plate was located between 2 1.00×0.40×0.02 m carpets, providing a “4-m treadmill”.
PLANTAR PRESSURE ANALYSIS:
Before the formal tests, all participants were instructed to perform acclimatization training 3~5 times, walking along the treadmill barefoot at a comfortable pace without any assistance while looking forward. Based on results of these trials, each participant recorded a suitable starting point to ensure that 3 steps were taken prior to contacting the force plate [13]. The formal tests were conducted according to the above standards after 10 minutes, and the dynamic plantar pressure data was recorded. For each test, only 1 complete footprint for each side was manually selected for analysis.
DATA COLLECTION:
All participants’ general information such as age, sex, weight, height, body mass index (BMI), foot length, and foot width was recorded. All participants were also requested to complete the CAIT questionnaire.
The Scientific Footscan® software could automatically divide the foot into 10 zones: hallux (T1), toes 2–5 (T2–5), first to fifth metatarsals (M1–M5), midfoot (MF), medial heel (MH), and lateral heel (LH). Because T2–5 and MF zone are not the main load-bearing areas, only the clinically most relevant parameters of the remaining 8 zones were collected for further analysis, including peak force/weight (PF/W, N/kg), and time to peak force reported as a percentage of the stance time (TPF,%)
During the data collection, the COP was automatically generated by the aforementioned software for every 80 ms, and the position relative to the boundary of the footprint and the instantaneous velocity of each COP was recorded. According to the position and velocity of each COP, the time to boundary (TTB, s) could be calculated to assess postural stability [14]. Finally, the minimum value of TTB in anterior-posterior and medial-lateral directions was collected for further analysis.
For the CAI group, we assessed plantar pressure parameters of both sides, while for the control group, we used the average of 2 sides for further analysis [15].
STATISTICAL ANALYSIS:
Statistical analysis was conducted using SPSS version 24.0 software (SPSS, Inc., IL, USA). The data were explored for outliers and distribution by Shapiro-Wilk test. All normally distributed data were presented as mean±standard deviation.
Results
THE DEMOGRAPHIC INFORMATION OF SUBJECTS:
From April 2019 to March 2022, 32 CAI patients satisfying the inclusion criteria were recruited into the present study. Among those patients, 5 could not walk without aid, another 3 patients’ data collection was incomplete. Finally, 24 CAI patients participated and completed the plantar pressure analysis successfully. Among the CAI group, there are 15 males and 9 females, the average age was 31.31±4.17 years, the average CAIT score on the affected side was 14.38±3.75, and on the unaffected side it was 27.91±2.13. Another 24 age-matched healthy individuals were recruited as the control group, including 17 males and 7 females, 29.43±5.35 years old, with an average CAIT score of 27.69±3.31. There were no significant differences between the 2 groups in age, sex, height, weight, foot length and width, or BMI (P>0.05). We found significant differences in CAIT scores between the unaffected side and affected side in unilateral CAI patients (P<0.001), as well as the affected side in unilateral CAI patients and the healthy group (P<0.001) (Table 1).
COMPARISON OF THE PARAMETERS OF THE AFFECTED AND UNAFFECTED SIDE OF CAI PATIENTS:
There was no significant difference of PF/W between the affected side and unaffected side (P>0.05) (Figure 1). For TPF, significant differences and large effect size were found in M3 and M4 zones (M3, P=0.44, effect size=0.86 and M4, P<0.001, effect size=0.91) (Figure 2), indicating that the time of the affected foot entering the middle stage of the supporting phase was prolonged, which may be the compensatory mechanism of ankle instability. In the meantime, the minimum medial-lateral TTB of the affected side was significantly lower than that of the unaffected side (P=0.032, effect size=0.61), indicating that the affected side was more likely to lose posture stability. No significant difference was found in COP velocity of the affected side and unaffected side. Detailed data are shown in Table 2.
COMPARISON OF THE PARAMETERS OF CAI AND CONTROL GROUPS:
As shown in Table 2 and Figure 1, compared with normal individuals, the PW/F of T1, M1, M2, and MH zones on the affected side of CAI patients were significantly decreased with large effect sizes (P<0.001), while the PW/F of M5 and LH zones were significantly increased with large effect sizes (P<0.001). In addition, the PW/F of T1 zone on the unaffected side of CAI patients were significantly lower than in normal individuals (P=0.004, effect size=0.74), while the PW/F of the LH zone was higher (P=0.036, effect size=0.68). The results showed that the plantar pressure of both sides of CAI patients tended to distribute more laterally during walking, and both ankle joints showed varus in different degrees. In addition, the decrease of PF/W in the T1 zone of both sides indicated that CAI patients had insufficient power to push off from the ground.
For CAI patients, the TPF of M3 and M4 zones on the affected side (P<0.001), and M4 zone on the unaffected side (P=0.025) were prolonged during walking, all with a large effect size (Figure 2). Both the anterior-posterior and medial-lateral TTB on the affected side of CAI patients were significantly decreased compared to the control group (P<0.001, effect size >0.80), while only medial-lateral TTB on the unaffected side was significantly decreased (P=0.012, effect size=0.63). As for the anterior-posterior and medial-lateral COP velocity, both sides were significantly increased compared to the control group (P<0.001, effect size >0.80). The difference of the above parameters indicates that the balance control of both sides in CAI patients is relatively poor, which may be the reason for repeated LASs.
CORRELATION AND UNIVARIATE ANALYSIS BETWEEN PLANTAR PRESSURE PARAMETERS AND RELATED FACTORS:
Table 3 shows results of univariate analysis or correlation analysis based on the patient’s basic information and the different plantar pressure parameters according to the data type (sex and injured side are classified variables, CAIT score and BMI are continuous variables). The results show that the medial-lateral TTB of males was significantly longer than in females (P=0.01), while the medial-lateral COP velocity of males was significantly lower than in females (P=0.01), suggesting that male patients with CAI have better posture balance than females in the medial-lateral direction. The TPF of the M4 zone (r=−0.57, P<0.001), COP velocity (anterior-posterior, r=−0.55, P=0.01), and medial-lateral (r=−0.68, P=0.005) were negatively correlated with CAIT scores, and TTB was significantly positively correlated with CAIT score (anterior-posterior, r=0.79, P<0.001 and medial-lateral r=0.63, P<0.001), suggesting that patients with low CAIT scores may have poor balance control ability.
Discussion
CAI is a common complication after ankle sprain [1,3]. However, the current clinical diagnosis of CAI is mainly based on the subjective description of the patient [16], which could be biased by the patient’s individual differences, leading to inaccurate assessment. Although numerous questionnaires have been developed [12,16], they are still subjective evaluation tools. Plantar pressure analysis plays an important role in objectively evaluating ankle function when walking [7,8], and few studies have shown detailed characteristics of plantar pressure distributions in CAI patients, limiting its application in CAI diagnosis and evaluation. The present study systematically analyzed the characteristics of plantar pressure distribution in patients with CAI during walking by comparing the affected side, the unaffected side, and a healthy control.
For CAI patients, the TPF of M3 and M4 zones on the affected side was higher than that of the unaffected side, which was also observed when compared to healthy controls. For the unaffected side, the TPF of M4 zone was significantly increased compared to normal individuals. This indicates that the process of weight transfer to the midfoot is prolonged, and the support phase is longer on the affected side, which is also shown by the COP trajectory in Figure 3. Because the anatomy of the talus is wide in front and narrow in back, the stability of the ankle joint in extension is higher than that in flexion [17]. The time of ankle flexion in CAI patients is prolonged, which increases walking instability. As for the PF/W of each zone, there was no significant difference between the affected side and unaffected side in CAI patients, but compared to the control group, the PF/W of T1, M1, M2, and MH zones on the affected side and PF/W of T1 on the unaffected side were decreased, while the PF/W of M5 and LH zone on the affected side and PF/W on LH zones on unaffected side were increased. Consistent with previous studies [6], during the support phase of CAI patients, the PF/W of the anterolateral foot of the affected side was higher than in normal individuals, indicating that the plantar pressure was distributed more laterally, which further aggravated the possibility of repeated sprain. In addition, the plantar pressure distribution on unaffected side was abnormal, indicating a gait adjustment to maintain balance. During human walking, the feet are alternately load-bearing, so abnormalities in one foot will affect the overall postural balance [18]. When the other foot contacts the ground, this overall imbalance needs to be adjusted, which will inevitably affect plantar pressure distribution. Previous studies have also confirmed that patients with unilateral clubfoot also have abnormal plantar pressure distribution on the unaffected side [15], but the specific mechanism is unclear.
TTB can reflect an individual’s posture stability; smaller values indicate poorer balance function [14]. CAI patients tend to place their COP close to the stable boundary; therefore, TTB is shorter, indicating the possibility of potential instability. The current study found that the medial-lateral TTB of the affected side of CAI patients was shorter than that of the unaffected side. Moreover, compared with the control group, there were significant differences in TTB and COP velocity on both the affected side and unaffected side. TTB and COP velocity are also useful in objectively evaluating the effects of interventions. Previous study has found that after 4 weeks of comprehensive balance training, the anterior-posterior TTB of CAI patients increased significantly, and posture balance significantly improved [19]. McKeon et al [20] reported that after joint mobilization, plantar fascia massage, and gastrocnemius muscle stretching, the anterior-posterior and medial-lateral COP velocity of CAI patients were significantly decreased. Further research is needed to assess the clinical value of these parameters in CAI diagnosis.
The present study found that the medial-lateral COP velocity was related to sex, indicating that the posture stability of female CAI patients was worse than in males. Nigg et al [21] reported that female CAI patients had a larger anterior-posterior COP deviation, which may indicate that the stability posture stability of females with CAI is weaker than in males due to differences in muscle strength. The Cumberland ankle instability tool (CAIT) was designed by Hiller et al [12] to diagnose and grade ankle stability, which was demonstrated to have good reliability and validity. In contrast to other questionnaires, such as foot and ankle ability measure (FAAM) [22] scores, the CAIT requires the subjects to score the left and right ankles separately, rather than comparing the left and right ankle functions, so it more accurately evaluates patients with unilateral CAI. However, the CAIT is still a subjective evaluation tool. The correlation analysis of this study shows that plantar pressure parameters are highly correlated with the CAIT score, which confirms that plantar pressure analysis can be used for the objective evaluation and diagnosis of CAI.
There are still same limitations in the present study. First, we only analyzed the plantar pressure distribution of CAI patients during walking, and other conditions such as running, jumping, and stepping up or down need further investigation. Secondly, all patients included in this study were CAI after LAS, but patients with arthrochalasis can also present as CAI [23], and whether there is any difference needs to be clarified. Last but not the least, although LAS account for more than 90% of ankle sprains [1], it is still necessary to conduct research on the plantar pressure distribution of patients with inversion ankle sprain.
Conclusions
The present study analyzed the plantar pressure distributions of CAI patients, and observed a significant correlation between the CAIT scores and plantar pressure parameters. It is suggested that plantar pressure analysis can be used for the objective evaluation of CAI patients. The present study also made comparisons with healthy individuals to describe the characteristics of plantar pressure distribution of CAI patients during walking. The results showed that the posture stability of CAI patient was significantly worse than that of normal individuals, and the plantar pressure was more laterally distributed. Our results show that patients with CAI need to pay attention to functional training of the affected side as well as the unaffected side during rehabilitation, and that plantar pressure analysis is promising in auxiliary diagnosis and rehabilitation evaluation of CAI.
Figures
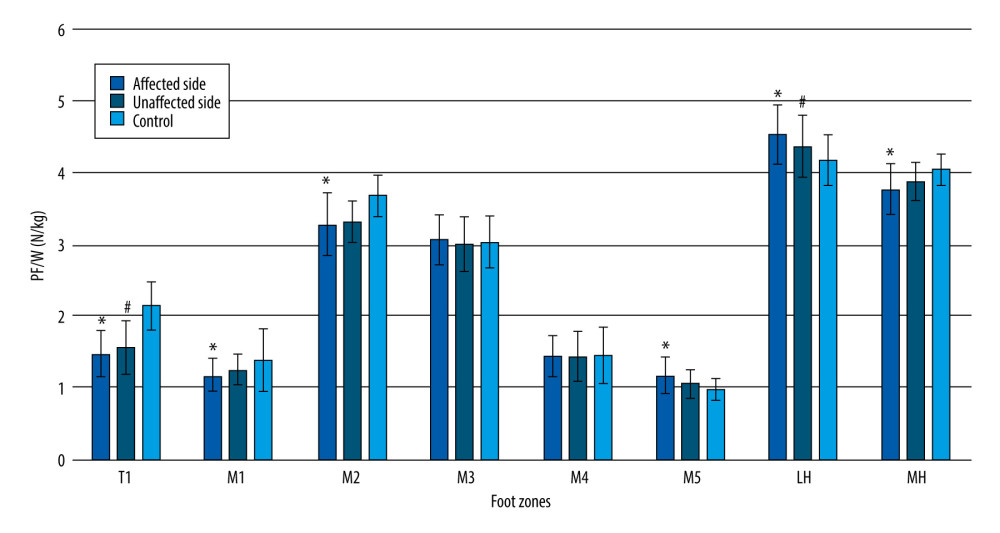 Figure 1. Comparison of PF/W on the affected side and unaffected side in CAI group and the control group* Indicates significant difference between affected side in the CAI group and control group; # indicates significant difference between unaffected side in CAI group and control group. Microsoft® Excel® (Microsoft Corporation, USA) was used for creation of the figure.
Figure 1. Comparison of PF/W on the affected side and unaffected side in CAI group and the control group* Indicates significant difference between affected side in the CAI group and control group; # indicates significant difference between unaffected side in CAI group and control group. Microsoft® Excel® (Microsoft Corporation, USA) was used for creation of the figure. 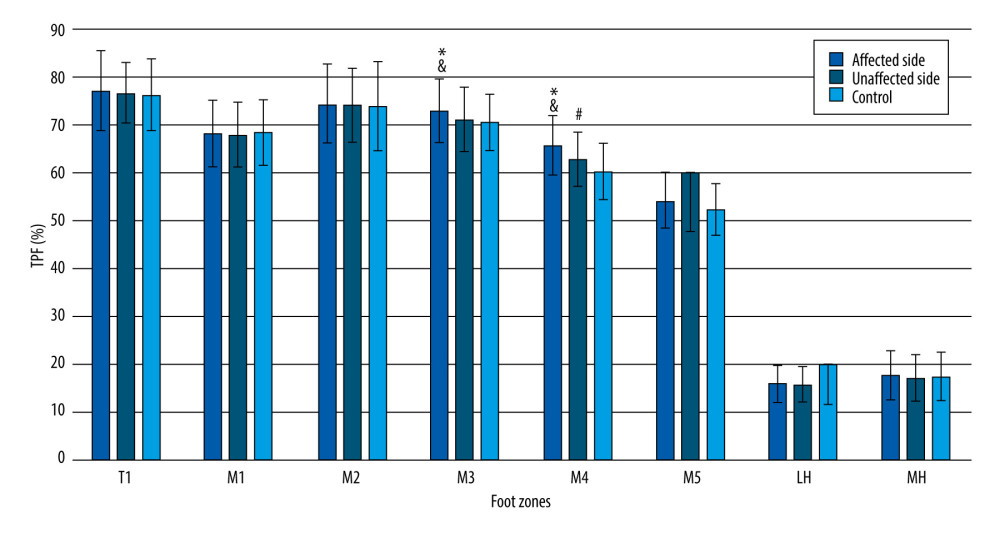 Figure 2. Comparison of TPF on the affected side and unaffected side in the CAI group and the control group. & Indicates significant difference between affected side and unaffected side in CAI group; * indicates significant difference between affected side in CAI group and control group; # indicates significant difference between unaffected side in the CAI group and control group. Microsoft® Excel® (Microsoft Corporation, USA) was used for creation of the figure.
Figure 2. Comparison of TPF on the affected side and unaffected side in the CAI group and the control group. & Indicates significant difference between affected side and unaffected side in CAI group; * indicates significant difference between affected side in CAI group and control group; # indicates significant difference between unaffected side in the CAI group and control group. Microsoft® Excel® (Microsoft Corporation, USA) was used for creation of the figure. 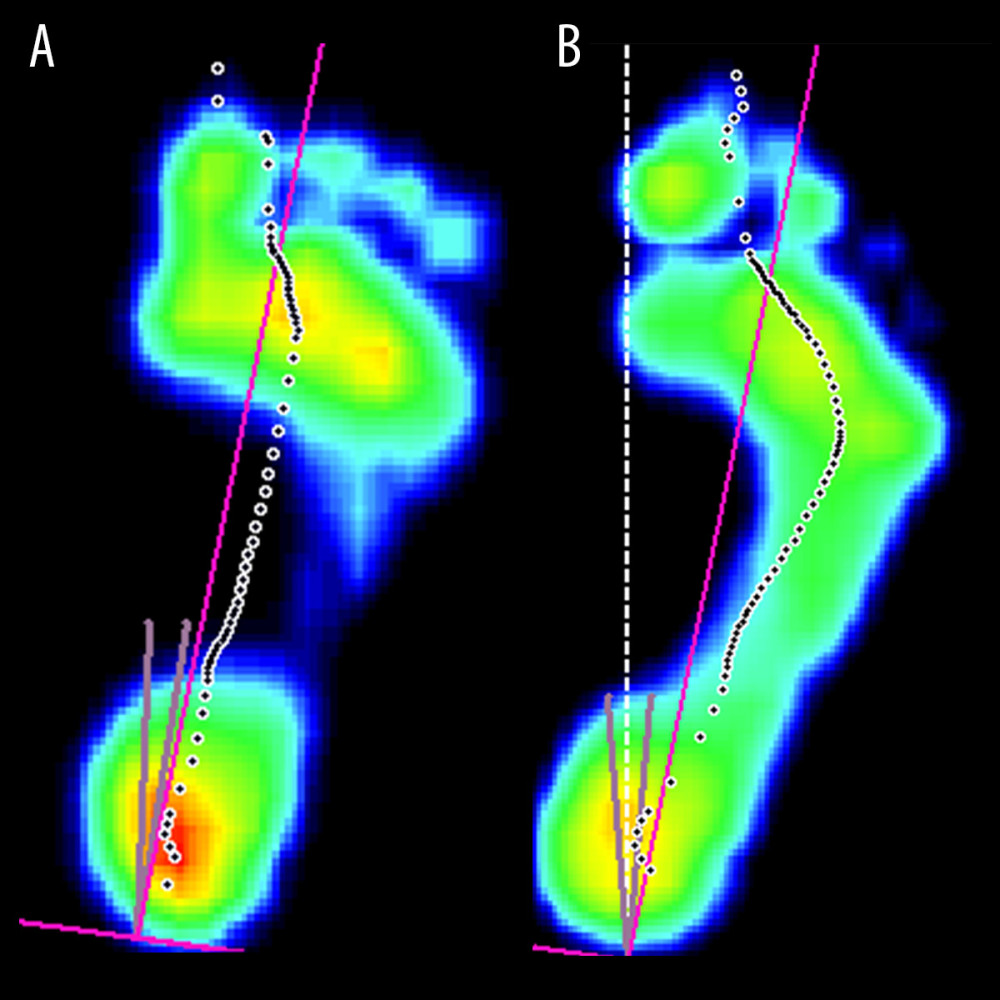 Figure 3. Schematic diagram of plantar pressure distribution between normal (A) and CAI patients (B) during walking(A) Normal individual; (B) CAI patient. The purple line stands for longitudinal axis of the foot, passing through the midpoint of heel and the midpoint of the 2nd and 3rd metatarsal heads. The dashed line composed of black dots represents the COP trajectory. The figure shows that the COP trajectory of CAI patients is shifted to the lateral side of the foot compared to normal individuals. Scientific Footscan® software (RSscan International®, Belgium) was used for creation of the figure.
Figure 3. Schematic diagram of plantar pressure distribution between normal (A) and CAI patients (B) during walking(A) Normal individual; (B) CAI patient. The purple line stands for longitudinal axis of the foot, passing through the midpoint of heel and the midpoint of the 2nd and 3rd metatarsal heads. The dashed line composed of black dots represents the COP trajectory. The figure shows that the COP trajectory of CAI patients is shifted to the lateral side of the foot compared to normal individuals. Scientific Footscan® software (RSscan International®, Belgium) was used for creation of the figure. References
1. Doherty C, Delahunt E, Caulfield B, The incidence and prevalence of ankle sprain injury: A systematic review and meta-analysis of prospective epidemiological studies: Sports Med, 2014; 44(1); 123-40
2. Delahunt E, Remus A, Risk factors for lateral ankle sprains and chronic ankle instability: J Athl Train, 2019; 54(6); 611-16
3. Drakos M, Hansen O, Kukadia S, Ankle instability: Foot Ankle Clin, 2022; 27(2); 371-84
4. Miklovic TM, Donovan L, Protzuk OA, Acute lateral ankle sprain to chronic ankle instability: A pathway of dysfunction: Phys Sportsmed, 2018; 46(1); 116-22
5. Koldenhoven RM, Hart J, Saliba S, Gait kinematics & kinetics at three walking speeds in individuals with chronic ankle instability and ankle sprain copers: Gait Posture, 2019; 74; 169-75
6. Koldenhoven RM, Feger MA, Fraser JJ, Surface electromyography and plantar pressure during walking in young adults with chronic ankle instability: Knee Surg Sports Traumatol Arthrosc, 2016; 24(4); 1060-70
7. Buldt AK, Allan JJ, Landorf KB, The relationship between foot posture and plantar pressure during walking in adults: A systematic review: Gait Posture, 2018; 62; 56-67
8. Mettler A, Chinn L, Saliba SA, Balance training and center-of-pressure location in participants with chronic ankle instability: J Athl Train, 2015; 50(4); 343-49
9. Torp DM, Thomas AC, Donovan L, External feedback during walking improves measures of plantar pressure in individuals with chronic ankle instability: Gait Posture, 2019; 67; 236-41
10. Morrison KE, Hudson DJ, Davis IS, Plantar pressure during running in subjects with chronic ankle instability: Foot Ankle Int, 2010; 31(11); 994-1000
11. Gribble PA, Delahunt E, Bleakley CM, Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium: J Athl Train, 2014; 49(1); 121-27
12. Hiller CE, Refshauge KM, Bundy AC, The Cumberland ankle instability tool: A report of validity and reliability testing: Arch Phys Med Rehabil, 2006; 87(9); 1235-41
13. He YJ, Zheng XL, Wang DF: Med Sci Monit, 2023; 29; e938485
14. DiLiberto FE, Nawoczenski DA, Tome J, Use of time-to-boundary to assess postural instability and predict functional mobility in people with diabetes mellitus and peripheral neuropathy: Gait Posture, 2021; 83; 141-46
15. Xu C, Wei J, Yan YB, Pedobarographic Analysis following Ponseti treatment for unilateral neglected congenital clubfoot: Sci Rep, 2018; 8(1); 6270
16. Chang SH, Morris BL, Saengsin J, Diagnosis and treatment of chronic lateral ankle instability: Review of our biomechanical evidence: J Am Acad Orthop Surg, 2021; 29(1); 3-16
17. Medina McKeon JM, Hoch MC, The ankle-joint complex: A kinesiologic approach to lateral ankle sprains: J Athl Train, 2019; 54(6); 589-602
18. Wen JX, Yang HH, Han SM, Trunk balance, head posture and plantar pressure in adolescent idiopathic scoliosis: Front Pediatr, 2022; 10; 979816
19. Powden CJ, Hoch JM, Jamali BE, A 4-week multimodal intervention for individuals with chronic ankle instability: Examination of disease-oriented and patient-oriented outcomes: J Athl Train, 2019; 54(4); 384-96
20. McKeon PO, Wikstrom EA, The effect of sensory-targeted ankle rehabilitation strategies on single-leg center of pressure elements in those with chronic ankle instability: A randomized clinical trial: J Sci Med Sport, 2019; 22(3); 288-93
21. Nigg BM, GKE , Federolf P, Gender differences in lower extremity gait biomechanics during walking using an unstable shoe: Clin Biomech (Bristol, Avon), 2010; 25(10); 1047-52
22. Saarinen AJ, Uimonen MM, Suominen EN, Structural and construct validity of the Foot and Ankle Ability Measure (FAAM) with an emphasis on pain and functionality after foot surgery: A multicenter study: J Foot Ankle Surg, 2022; 61(4); 872-78
23. Owen JR, Elson RA, Grech P, Generalized hypermobility of joints: Arthrochalasis multiplex congenita: Arch Dis Child, 1973; 48(6); 487-89
Figures
Figure 1. Comparison of PF/W on the affected side and unaffected side in CAI group and the control group* Indicates significant difference between affected side in the CAI group and control group; # indicates significant difference between unaffected side in CAI group and control group. Microsoft® Excel® (Microsoft Corporation, USA) was used for creation of the figure.Figure 2. Comparison of TPF on the affected side and unaffected side in the CAI group and the control group. & Indicates significant difference between affected side and unaffected side in CAI group; * indicates significant difference between affected side in CAI group and control group; # indicates significant difference between unaffected side in the CAI group and control group. Microsoft® Excel® (Microsoft Corporation, USA) was used for creation of the figure.Figure 3. Schematic diagram of plantar pressure distribution between normal (A) and CAI patients (B) during walking(A) Normal individual; (B) CAI patient. The purple line stands for longitudinal axis of the foot, passing through the midpoint of heel and the midpoint of the 2nd and 3rd metatarsal heads. The dashed line composed of black dots represents the COP trajectory. The figure shows that the COP trajectory of CAI patients is shifted to the lateral side of the foot compared to normal individuals. Scientific Footscan® software (RSscan International®, Belgium) was used for creation of the figure. Tables
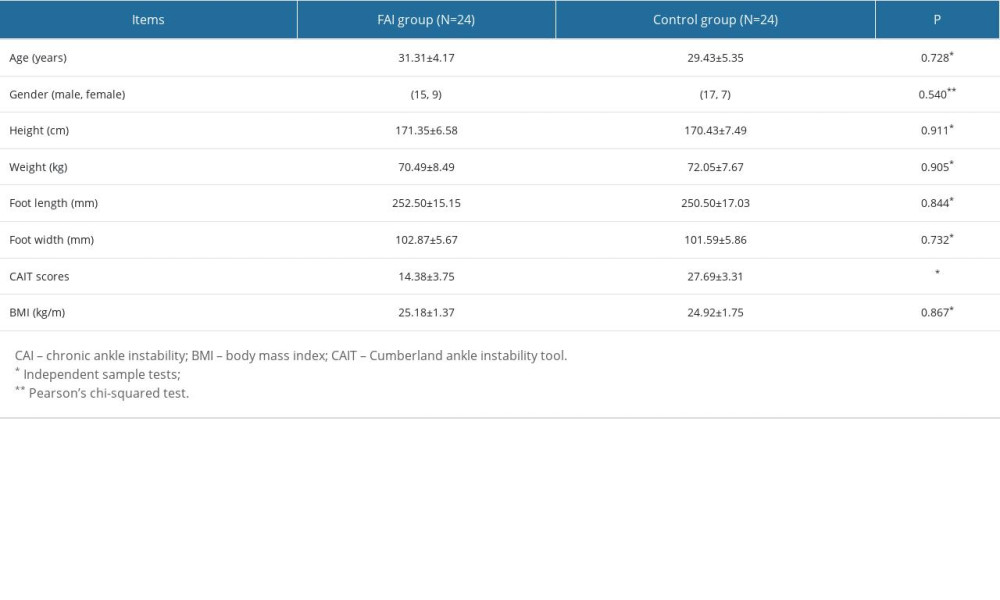 Table 1. Demographic data for the CAI group and control group.
Table 1. Demographic data for the CAI group and control group.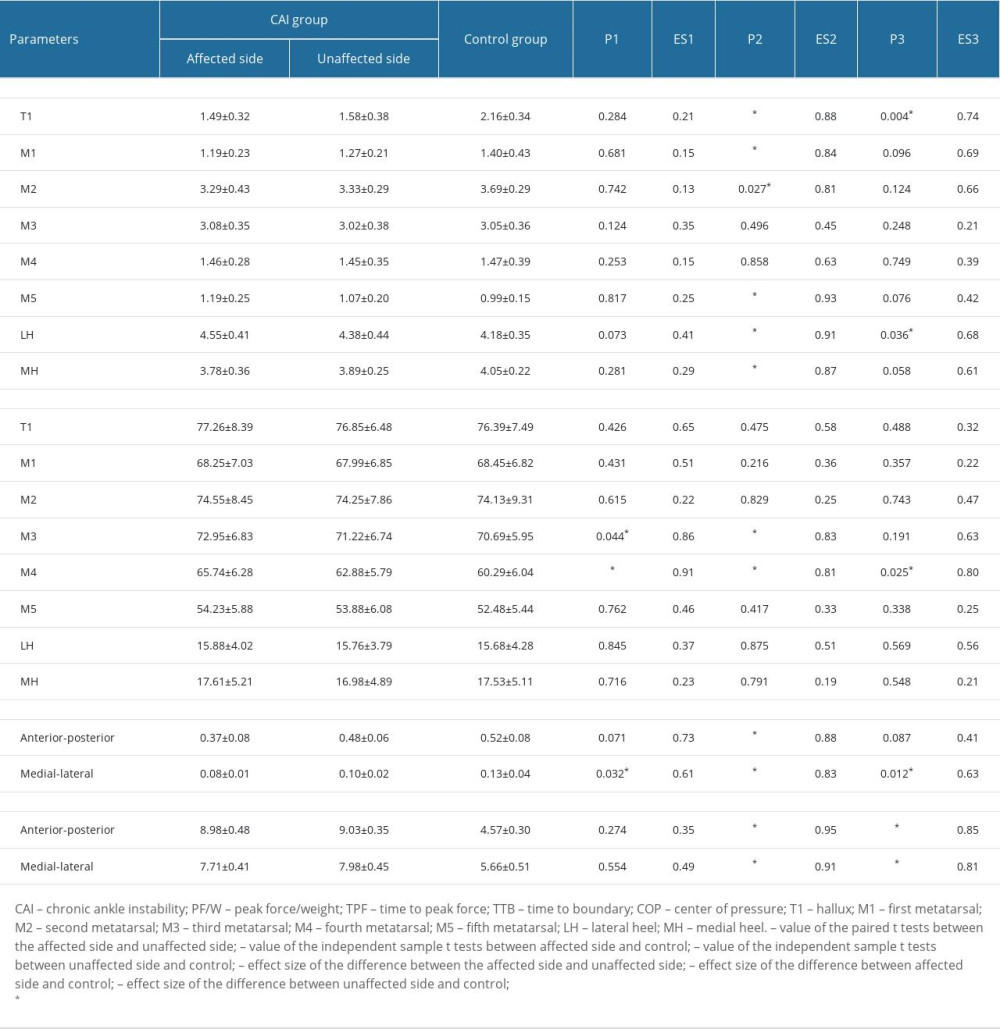 Table 2. Comparison of the plantar pressure parameters of the CAI and control group.
Table 2. Comparison of the plantar pressure parameters of the CAI and control group.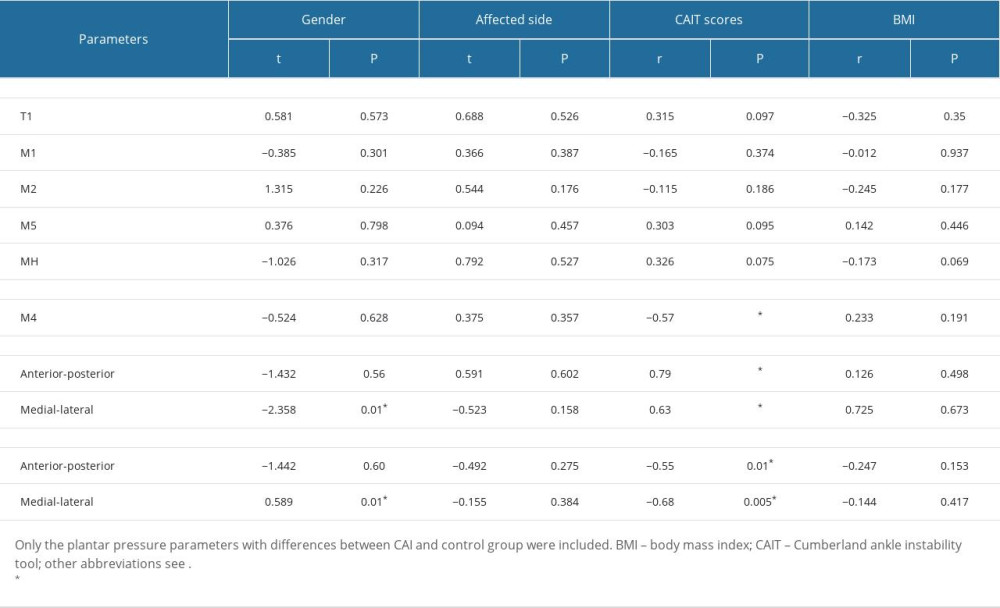 Table 3. Correlation and univariate analysis between plantar pressure parameters and related factors.Table 1. Demographic data for the CAI group and control group.Table 2. Comparison of the plantar pressure parameters of the CAI and control group.Table 3. Correlation and univariate analysis between plantar pressure parameters and related factors.
Table 3. Correlation and univariate analysis between plantar pressure parameters and related factors.Table 1. Demographic data for the CAI group and control group.Table 2. Comparison of the plantar pressure parameters of the CAI and control group.Table 3. Correlation and univariate analysis between plantar pressure parameters and related factors. In Press
08 Mar 2024 : Clinical Research
Evaluation of Foot Structure in Preschool Children Based on Body MassMed Sci Monit In Press; DOI: 10.12659/MSM.943765
15 Apr 2024 : Laboratory Research
The Role of Copper-Induced M2 Macrophage Polarization in Protecting Cartilage Matrix in OsteoarthritisMed Sci Monit In Press; DOI: 10.12659/MSM.943738
07 Mar 2024 : Clinical Research
Knowledge of and Attitudes Toward Clinical Trials: A Questionnaire-Based Study of 179 Male Third- and Fourt...Med Sci Monit In Press; DOI: 10.12659/MSM.943468
08 Mar 2024 : Animal Research
Modification of Experimental Model of Necrotizing Enterocolitis (NEC) in Rat Pups by Single Exposure to Hyp...Med Sci Monit In Press; DOI: 10.12659/MSM.943443
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952