24 July 2023: Clinical Research
Enhancing Nighttime Surgical Instrument Cleaning Efficiency: An ECRS-Based Approach
Ting Hu12ABE, Liangying Yi12E, Yuxin Tang3C*, Yanhua Chen12E, Ruixue Hu42CDOI: 10.12659/MSM.940346
Med Sci Monit 2023; 29:e940346






Abstract
BACKGROUND: Efficient and timely cleaning of surgical instruments is paramount for optimal patient care. Challenges often arise during the collection and processing of instruments utilized in nighttime surgical procedures, impeding effective cleaning. To address these inefficiencies, we employed the Eliminate-Combine-Rearrange-Simplify (ECRS) strategy to improve the quality and efficiency of nighttime surgical instrument cleaning processes.
MATERIAL AND METHODS: We optimized the nighttime surgical instrument cleaning process using the ECRS methodology. For the study, 27,308 surgical instruments cleaned between May and June 2021 were categorized as the control group, while 28,471 instruments cleaned between October and November 2021 constituted the observation group. We compared the number of quality defects in instrument cleaning, procedure times, and quantities of cleaning agents used before and after the implementation of ECRS.
RESULTS: With the ECRS application, the cleaning process was streamlined from 14 steps to 13. The quality defect rate, cleaning time per instrument batch, and average quantity of cleaning agent used per instrument were initially 2.11%, 115 minutes, and 0.278 mL/piece, respectively. Post-ECRS implementation, these measures were significantly reduced to 0.26%, 91 minutes, and 0.193 mL/piece, correspondingly.
CONCLUSIONS: The ECRS strategy presents a practical solution to optimize the cleaning process for surgical instruments used during nighttime procedures. This approach not only improves the quality and efficiency of cleaning but also contributes to cost reduction. This underscores the potential of ECRS in enhancing healthcare operation management.
Keywords: Procedures and Techniques Utilization, quality improvement, Surgical Instruments, Humans, Plastic Surgery Procedures
Background
Used surgical instruments are contaminated with patients’ body fluids, including secretions, excretions, human tissue, and other non-water-soluble contaminants. Such residues often contain hazardous concentrations of microorganisms. Improper cleaning of used surgical instruments permits the coalescing of residues that then form a biofilm. This biofilm obstructs both the penetration of sterilants and the contact of high-temperature sterilizing gases with microorganisms, thus posing an infection risk to other patients during reuse [1,2]. Cleaning quality defects can result in corrosion, damaging the instrument surface.
In the Central Sterile Supply Department (CSSD) in this case study, the cleaning personnel generally work day shifts, whereas the operating room requires 24-h staffing. This means that the surgical instruments can be collected and processed by CSSD staff only from 8: 00 a.m. until 6: 00 p.m. Therefore, the surgical instruments used by the operating room staff during nighttime hours cannot be collected or processed by CSSD staff in a timely manner. Some instruments may be stored in the operating room for approximately 10 h until the CSSD staff begin their shifts. The day staff’s usage of the CSSD can have a negative influence on the cleaning quality of the instruments used by the operating room staff during nighttime hours.
If the surgical instruments used in nighttime diagnosis and treatment cannot be collected by CSSD staff in a timely manner for processing, then the blood stains, mucus, and proteins remaining on the surfaces of these instruments could dry and form protective films, increasing the difficulty of cleaning and impairing disinfection and sterilization. This can shorten the service life of the instruments and contribute to iatrogenic infections [3,4]. According to a study by Wei et al [5], the pass rate of instrument cleaning was 99.21% when the instruments were cleaned immediately after use, but decreased to 90.75% when they were cleaned 1 h after use. The results of Luo et al [6] and Zhao [7] showed that the longer the time instruments are put aside, the more difficult they become to clean, resulting in increased cleaning costs and decreased service life of these instruments. Therefore, more attention should be paid to the quality of cleaning of surgical instruments that are used and later stored in the used instrument department during nighttime hours. Measures should be taken to improve the quality of cleaning of surgical instruments used and disposed of during nighttime hours, thereby ensuring the quality of subsequent sterilization.
The Eliminate-Combine-Rearrange-Simplify (ECRS) method is a process re-engineering method and tool. It uses process charts to explore the hidden systemic problems in the work process and adopts 4 core principles (eliminate wasteful steps, combine duplicate process steps, rearrange the sequence of steps, and simplify steps) to achieve high efficiency [8,9]. Application of the ECRS method in hospital management can save working time, and thus offers economic benefits [10,11]. The cleaning of surgical instruments used and disposed of during nighttime hours is always a focus of the cleaning work in the CSSD. However, relevant studies are rare not only in China but also in other countries and regions. In this case study, we conducted an ECRS-based optimization of the cleaning procedures for surgical instruments being used and then disposed of in the used surgical instruments department during nighttime hours, with the intent of determining an optimal working procedure.
Material and Methods
ETHICS APPROVAL:
This study was conducted in accordance with the Declaration of Helsinki. All research methods were carried out in accordance with the relevant guidelines and regulations. This study was approved by the medical ethics committee of the authors’ institution (2023 Medical Scientific Research for Ethical Approval No. 005). Verbal informed consent to participate in this study was obtained from all participants. The medical ethics committee of the authors’ institution approved the procedure of verbal informed consent of this study.
STUDY SETTING:
A total of 27 308 surgical instruments subjected to these procedures in our hospital during May and June 2021 were classified as the control group; 28 471 surgical instruments subjected to these procedures in our hospital during October and November 2021 were classified as the observation group. Data concerning the numbers of the surgical instruments were derived from our hospital’s health information system, and data concerning the number of quality defects associated with cleaning of these surgical instruments were obtained via an inspection form. Our hospital has 45 operating rooms, and there are around 3800 surgical procedures in our hospital per month. Approximately 520 000 surgical instruments are processed by our CSSD each month. Of them, about 14 000 instruments were used by operating rooms during nighttime hours. Our CSSD is 650 m away from the operating rooms.
CLEANING QUALITY EVALUATION CRITERIA:
The quality of surgical instrument cleaning was assessed by the appointed inspector by means of visual or magnifying glass-based inspection. The inspector had received appropriate training in cleaning procedures and quality standards prior to the inspection. The inspection results were recorded in the inspection form designed by the researchers. A “pass” rating was conferred only when no contaminants (eg, blood stains, dirt, water spots) or rusts were detected on the surfaces of the instruments, their articulations, or grooves.
INCLUSION AND EXCLUSION CRITERIA:
Surgical instruments satisfying the following criteria were included in this study: (1) those used for diagnosis and treatment during nighttime hours and temporarily stored in the operating room; and (2) those for which the period after use and before CSSD cleaning was ≥1 h. Surgical instruments used in daytime and those used during the night but collected within 1 h were excluded from this study.
CLEANING MATERIALS CONSUMPTION:
Details of the cleaning materials used on the surgical instruments were recorded by the cleaning personnel on the surgical instrument cleaning consumable form. These data were collected to investigate whether the brands and model numbers of the cleaning agents and the cleaning tools were the same, both before and after ECRS-based optimization. The cleaning personnel involved in this study had received the necessary training on proper use of cleaning agents and tools.
CLEANING TIME:
Surgical instrument cleaning was performed by specific personnel who had received the training on cleaning procedures prior to doing so. The cleaning time was recorded for each surgical instrument.
CLEANING TEAM:
The team responsible for cleaning surgical instruments used and disposed of during nighttime hours consisted of a head nurse, a quality control nurse, researchers, clinical nurses, and CSSD cleaning personnel.
ECRS IMPLEMENTATION AT CSSD:
Process analysis was adopted to record the entire surgical instrument collection and cleaning process, in accordance with the cleaning flowchart. The process consisted of 5 steps: operation, inspection, transport, wait, and storage. The time and moving distance required for each step were recorded. Process analysis consisted of 2 parts: process steps and routing. The whole cleaning procedure was represented by the process analysis, and the routing showed the work flow route of the entire working space. The process flowchart of the cleaning procedures for the surgical instruments prior to ECRS implementation is presented in Figure 1.
The 5W1H [12] questioning technique was used to encourage us to think critically about surgical instrument cleaning: What (W) are the main causes of improper cleaning of the studied instruments? Why (W) do these causes exist? Which (W) steps are in need of improvement? When (W) should they be improved? Who (W) is the key person responsible for optimizing the cleaning process? And, How (H) to optimize? The ECRS team members discussed and answered these questions and agreed that the difficulty in instrument cleaning was due to the day shift, which leaves CSSD staff unable to process the instruments in time. This increased the difficulty of cleaning after the contaminants on the surface of the instruments dried up. The ECRS team members also considered whether manual cleaning could be canceled and machine cleaning could be carried out directly. For cleaning, the pre-processing and cleaning procedures could be improved, with them best to optimize before and during the cleaning procedures. The key persons to optimize the work procedures are operating room nurses and the CSSD nurses responsible for cleaning.
Two further questions were raised: (1) Is manual cleaning compulsory for instrument cleaning, or could machine-based cleaning substitute manual cleaning? (2) Given that both multi-enzyme and alkali cleaning agents are used in machine-based cleaning, can either be used as a standalone agent in machine-based cleaning? Following a discussion based on these questions, the ECRS-based optimization was conducted.
“ELIMINATE”:
This refers to the elimination of unnecessary steps in the cleaning process and workflow. To this end, application of a multi-enzyme cleaning agent has greater efficacy in the removal of softened contaminants. Surgical instruments being used and disposed of during nighttime hours, which hitherto were being soaked in alkaline cleaning agent in order to soften the contaminants, could instead be cleaned directly in a cleaning machine using the multi-enzyme cleaning agent.
“COMBINE”:
This refers to the combination of steps, each of which cannot be eliminated. Following combination, the sequence of the steps should be rearranged, and the work content and steps should be simplified to optimize the work flow and save resources.
“REARRANGE”: The surgical instruments used in the operating room during nighttime hours should be pre-processed by operating room nurses. The operating room nurses used gauze to remove the visible blood stains on the surface of the instruments and moistened the instruments using a moisturizing agent. Then, the instruments were placed in the temporary storage site within the operating room. The CSSD cleaning personnel used the high-pressure steam gun (temperature: 160°C; pressure: 8 MPa) to flush the instruments. The sprayed high-temperature steam and the friction generated by it allowed the dirt fall off naturally [13], generating a positive cleaning effect. The time spent performing manual scrubbing was much longer than that of flushing using the high-pressure steam gun; therefore, it is advisable to substitute the flushing for scrubbing
“SIMPLIFY”: It is known that an alkaline cleaning agent can reduce the adhesion of contaminants on the surfaces of instruments via the multiple effects of saponification, emulsification, and wetting, thereby making it a good softener [14]. Soaking in alkaline cleaning agent for 15 min results in significant decomposition of such organic contaminants, and the alkaline cleaning agent is still an active agent even if it is used repeatedly (within 24 h). A more efficient cleaning process is to soak the used surgical instruments in the alkaline cleaning agent and keep them moistened via sealing prior to disinfection and cleaning. This is a process that consumes less moisturizing solution [15]. Pre-soaking can reduce (up to 96%) prion-infected tissue contamination [16], and keeping instruments moist can potentially improve subsequent purification of reusable surgical instruments [17], while reducing processing time and costs. Therefore, the 2 steps (manual flushing and scrubbing of surgical instruments by cleaning personnel) of the cleaning process could be simplified.
Overall, implementation of these improved steps led to a reduction in the instrument cleaning time from 115 min to 91 min (Figure 2).
Results
The number of quality defects in cleaning before and after ECRS implementation are presented in Table 1.
The average quantities of cleaning agent used in each instrument before and after ECRS implementation were 0.278 mL/piece and 0.193 mL/piece, respectively. Mechanical cleaning using an alkaline cleaning agent was eliminated by ECRS analysis, thus saving cleaning agent. The cleaning agent for the instruments used in the operating room during nighttime hours was stored separately. The monthly average quantities of cleaning agent used for each instrument equaled the total consumption amount of cleaning agent for the instruments used in the operating room during nighttime hours divided by the total number of the instruments used in operating room during nighttime hours in that month (Table 2).
Cleaning time decreased from 115 min to 91 min. Through ECRS analysis, the operating room nurses pre-processed and moisturized the instruments in a timely manner, which greatly reduced the quantity of dirt on the surgical instruments. Meanwhile, keeping the instruments moist reduced the difficulty of cleaning, thereby simplifying the washing and scrubbing procedures and shortening the cleaning time of instruments.
Discussion
The results of our study show that the ECRS method successfully optimized the CSSD cleaning process for surgical instruments being used and disposed of during nighttime hours. The 4 principles – eliminate, combine, rearrange, and simplify – can help CSSD personnel realize better efficiency and find better working processes. Liu et al [18] used the 5W1H questioning technique and ECRS principles to determine an avenue for eliminating bottlenecking and defective processes, thereby ensuring a more balanced assembly line alongside better timekeeping during each procedure. Qi et al [19] used the ECRS method and process analysis methodologies to optimize the hospital’s work mode by reducing unnecessary steps in the diagnosis and treatment process, thus greatly improving work efficiency within the hospital. The results of Chien et al [20] obtained before and after process re-engineering in 3 hospitals in Taiwan showed that process re-engineering can significantly improve hospitals’ work efficiency.
In this study, we analyzed the cleaning procedures of the surgical instruments used in our hospital at night in terms of 5 components (operation, transport, inspection, wait, and storage) by means of process analysis and field survey. During application of ECRS, 1 step was eliminated, 1 step was rearranged, and 2 steps were simplified. Finally, the cleaning processes were reduced from 14 steps to 13 steps.
We demonstrated that ECRS-based optimization led to a significant improvement in the CSSD’s instrument processing efficiency. The CSSD cleaning personnel can now sanitize the nightly used surgical instruments using cleaning machines, without resorting to manual cleaning. The time required for the whole cleaning process was reduced from 115 min to 91 min, and the quality defect rate in cleaning was reduced from 2.11% to 0.26%. Thus, the ECRS method led to significant improvements in cleaning efficiency and cleaning quality. In recognition, the hospital has incorporated the enhanced cleaning process into its standardized operating procedure, which in turn can serve as a valuable reference for the processing of nightly used surgical instruments in other hospitals.
ECRS-based optimization can also lead to a reduction in the injury incidents among the cleaning personnel, as caused by manually cleaning sharp instruments. Sharp instrument-inflicted injuries are the most common occupational exposure in the CSSD. The results of Zhu et al [21] and Fan et al [22] showed that CSSD personnel face a considerable risk of sharp instrument-inflicted injury during manual work. Application of ECRS has yielded an optimized process less reliant on manual scrubbing, effectively reducing the risk of sharp instrument-inflicted injuries.
The average amounts of used cleaning agent and the cleaning time for each batch of instruments prior to ECRS-based optimization were 0.278 mL/piece and 115 min, respectively. Following ECRS-based optimization, these were reduced to 0.193 mL/piece and 91 min, respectively, reducing the CSSD’s expenditures on manpower and materials.
By using the ECRS analysis, the step of mechanical cleaning using an alkaline cleaning agent was eliminated; thus, the amount of alkaline cleaning agent was reduced. The “Central Sterile Supply Department (CSSD) – Part II: Standard for operating procedure of cleaning, disinfection and sterilization” [4] issued by the National Health and Family Planning Commission of China, requires that the instrument users remove obvious dirt from the surface of the instruments, utensils, and articles in a timely manner after use, and moisturize them as required. Through providing operating room nurses the training on pre-processing and moisturizing methods and their influence on sterilization quality and prolonging the service life of surgical instruments, the operating room nurses’ performance of pre-processing and moisturizing improved. Timely pre-processing and instrument moistening by the operating room nurse can reduce blood stains and other contaminants on the surface of the instruments. For example, spraying moisturizing agent can keep the instruments moist, so that the contaminants could not dry up. Then, the instruments will not need to be washed and scrubbed after being delivered to CSSD, thus saving time.
The studied surgical instruments might have been cleaned more effectively if they had been washed with flowing water and sprayed with alkaline cleaning agents for moistening prior to processing in the cleaning machines. In this study, manual cleaning was eliminated, and a high-pressure steam gun (temperature of 160°C; pressure: 8 MPa) was used to flush the instruments. As mentioned, the sprayed high-temperature steam and the friction generated by it caused the dirt to fall off naturally, generating a good cleaning effect and reducing the rate of quality defects in instrument cleaning.
The newly established CSSD shall consider having direct decontamination channels with the operating room to shorten the distance between operating room and CSSD. If no direct decontamination channels exist between the operating room and CSSD, the frequency of instrument collection by CSSD staff shall be increased so that the used instruments can be processed as soon as possible. The operating room nurses’ responsibilities of pre-processing and moisturizing need clarification. The CSSD can arrange night duty personnel according to the quantity of nighttime surgeries to allow timely processing of the instruments used for nighttime diagnosis and treatment in the operating room, thereby ensuring the cleaning quality of these instruments.
Since the cleaning task is moved from the operating room to the CSSD, ensuring the quality of cleaning while increasing the cleaning efficiency has become a key issue to cleaning within the CSSD. During daytime hours, the instrument pre-processing and moistening should be performed by trained CSSD workers. Only emergency operations are performed in our hospital during nighttime hours. If CSSD staff work night shifts, the labor costs will increase. Therefore, the night shift operating room nurses should pre-process the surgical instruments used in nighttime surgeries. The night shift operating room nurses should use gauze to remove the visible blood stains on the surface of the surgical instruments and moisten the instruments using a moisturizing agent. This procedure can lead to an increase in workload for the night shift operating room nurses. The hospital managers should coordinate workload of operating room nurses and CSSD staff. It is necessary to provide training on surgical instrument moistening to improve the compliance of operating room nurses to pre-process the instruments.
Conclusions
Our study combined ECRS-based optimization and 5W1H methodologies to scrutinize existing cleaning procedures of the surgical instruments being used and disposed of during nighttime hours and develop a standardized work flow to that end, thereby identifying optimal cleaning procedures and improving cleaning quality and work efficiency. However, it should be noted that the data collection period of this study and the observation period following ECRS implementation were short. In future studies, the sample size should be increased and the observation period should be extended in order to more accurately determine the effect of ECRS implementation.
Figures
 Figure 1. Process flowchart of cleaning procedures for surgical instruments prior to implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization (Software: Word; Version: 2019 Manufacturer: Microsoft). CSSD – Central Sterile Supply Department.
Figure 1. Process flowchart of cleaning procedures for surgical instruments prior to implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization (Software: Word; Version: 2019 Manufacturer: Microsoft). CSSD – Central Sterile Supply Department. 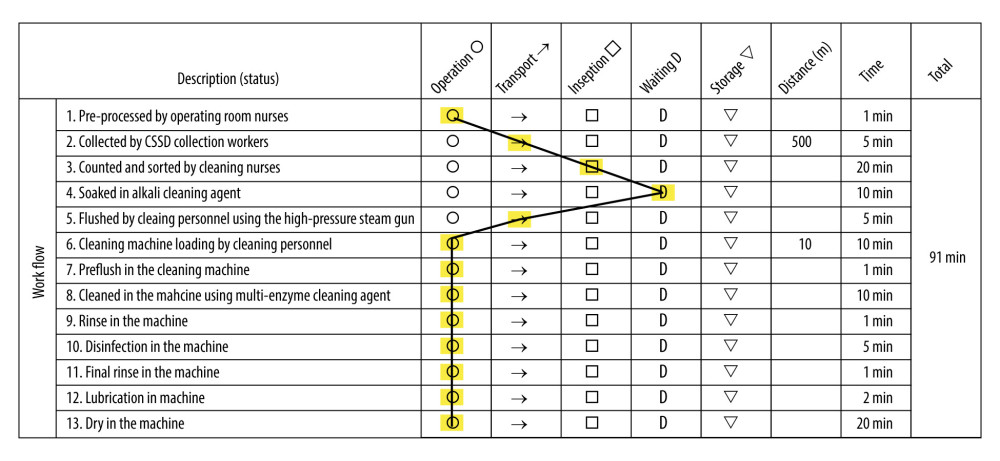 Figure 2. Process flowchart of cleaning procedures of surgical instruments following implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization (Software: Word; Version: 2019 Manufacturer: Microsoft). CSSD – Central Sterile Supply Department.
Figure 2. Process flowchart of cleaning procedures of surgical instruments following implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization (Software: Word; Version: 2019 Manufacturer: Microsoft). CSSD – Central Sterile Supply Department. Tables
Table 1. Quality defects in cleaning before and after implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization. Table 2. Average quantities of cleaning agent used for each instrument before and after implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization.
Table 2. Average quantities of cleaning agent used for each instrument before and after implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization.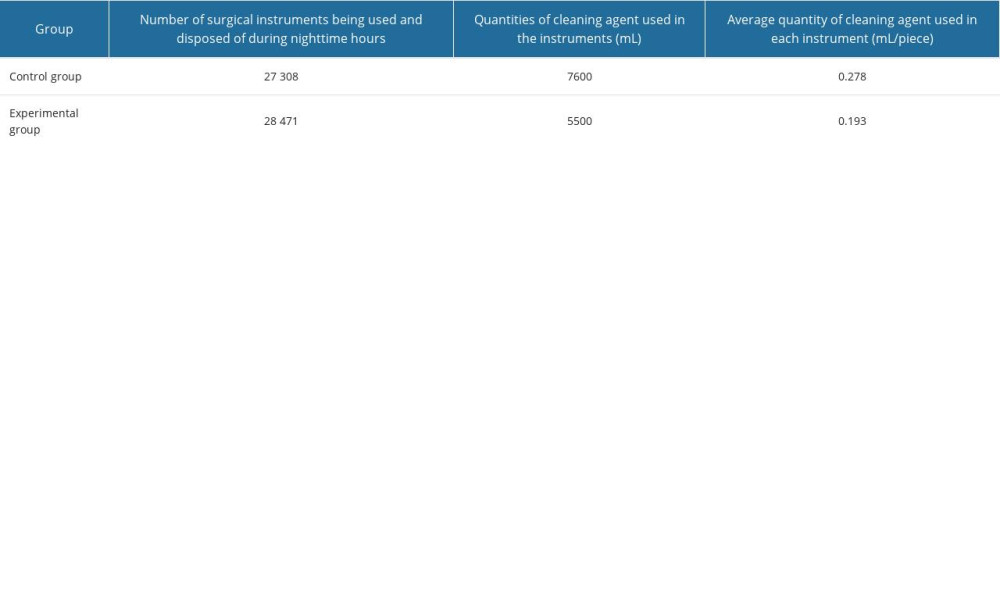
References
1. Luo W, Xu R, Wang W, Study on the influence of pretreatment methods and storage time of contaminated instruments on cleaning effect: Chinese Journal of Disinfection, 2015; 32(12); 1188-90
2. Evangelista SS, Guimaraes NR, Garcia NB: Am J Infect Control, 2020; 48(3); 267-74
3. Liu S, He Y, Yin Z, Guo L, Continuously improve the cleaning quality of reusable medical devices by root cause analysis: Chin J Infect Control, 2015; 14(12); 807-10
4. : Central Sterile Supply Department (CSSD) – Part II : Standard for operating procedure of cleaning, disinfection and sterilization (WS 310.2-2016), 2016, National Health and Family Planning Commission of the People’s Republic of China
5. Wei J, Li B, Shi J, The analysis of cleaning efficacy of medical instruments: China Medical Equipment, 2007(2); 4-6
6. Luo X, Zhu Y, Yan X, Non-thermal cleaning and disinfection effect of surgical instruments in different time after used and evaluation methods: Chin J Nosocomiol, 2014; 24(14); 3625-26
7. Zhao C, Influences of pretreatment methods on the cleaning effect after nonthermal cleaning and disinfecting for surgical instruments: China Medical Devices, 2017; 32(7); 134-36
8. Zhou Y, Thinking innovation and creativity development: Hangzhou: Zhejiang University Press, 2008; 144-46
9. Yu J, Zhou L, Hu L, Optimization of outpatient service process in large hospitals based on ECRS: Chinese Hospital, 2016; 20(11); 79-80
10. Luo L, Jiang K, Reducing the under-reporting rate of adverse transfusion reactions: Application of 5W+1H method combined with ECRS analysis principle: Chin J Blood Transfusion, 2021; 34(8); 870-73
11. Zhang W, Zhang Y, Pan Y, Nie G, Reconstruction of discharge settlement process for medical insurance patients based on ECRS: China Health Economics, 2020; 39(8); 71-74
12. Zhou F, Yang Z, Research on archival data management based on 5W1H method: Archives Science Study, 2019(4); 21-25
13. Yao Y, Yu Z, Peng S, Observation of the effect of moisturizing pretreatment on overnight surgical instrument cleaning: Chinese Journal of Disinfection, 2017; 34(6); 576-77
14. Liu L, Yang X, Zhang S, Research on the improvement of pretreatment method of overnight emergency surgical instruments: Chinese Journal of Hospital Infectology, 2016; 26(1); 227-28
15. Lipscomb IP, Pinchin H, Collin R, Keevil CW, Effect of drying time, ambient temperature and pre-soaks on prion-infected tissue contamination levels on surgical stainless steel: Concerns over prolonged transportation of instruments from theatre to central sterile service departments: J Hosp Infect, 2007; 65(1); 72-77
16. Secker TJ, Hervé R, Keevil CW, Adsorption of prion and tissue proteins to surgical stainless steel surfaces and the efficacy of decontamination following dry and wet storage conditions: J Hosp Infect, 2011; 78(4); 251-55
17. Gao X, Yang J, Zhang T, Analysis of factors affecting the cleaning quality of reusable surgical instruments under the application of steam cleaning machine and countermeasures for continuous improvement: Qilu Journal of Nursing, 2020; 26(18); 125-28
18. Liu B, Zhang T, Wei M, Production efficiency improvement of a company based on IE method: Value Engineering, 2019; 38(20); 261-63
19. Qi E, Xu G, Li C, Research on improvement of hospital treatment process based on industrial engineering ECRS: Journal of Inner Mongolia Agricultural University (Social Science Edition), 2007; 3; 178-80
20. Chien C, Zhao L, Chu P, Research and application of industrial engineering to hospital management in Taiwan: Industrial Engineering Journal, 2013; 16(1); 1-8
21. Sun J, Qin W, Jia L, Investigation and analysis of sharp injuries among health care workers from 36 hospitals in Shandong Province, China: Biomed Res Int, 2021; 2021; 5698483
22. Fan L, Zhou H, Investigation on risk factors and protection of sharp instrument injuries among personnel in the disinfection and supply center: Industrial Health and Occupational Diseases, 2022; 48(3); 243-45
Figures
Figure 1. Process flowchart of cleaning procedures for surgical instruments prior to implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization (Software: Word; Version: 2019 Manufacturer: Microsoft). CSSD – Central Sterile Supply Department.Figure 2. Process flowchart of cleaning procedures of surgical instruments following implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization (Software: Word; Version: 2019 Manufacturer: Microsoft). CSSD – Central Sterile Supply Department. Tables
Table 1. Quality defects in cleaning before and after implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization.Table 2. Average quantities of cleaning agent used for each instrument before and after implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization.Table 1. Quality defects in cleaning before and after implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization.Table 2. Average quantities of cleaning agent used for each instrument before and after implementation of Eliminate-Combine-Rearrange-Simplify (ECRS)-based optimization. In Press
15 Mar 2024 : Clinical Research
Impact of One-Lung Ventilation on Oxygenation and Ventilation Time in Thoracoscopic Heart Surgery: A Compar...Med Sci Monit In Press; DOI: 10.12659/MSM.943089
14 Mar 2024 : Clinical Research
Differential DHA and EPA Levels in Women with Preterm and Term Births: A Tertiary Hospital Study in IndonesiaMed Sci Monit In Press; DOI: 10.12659/MSM.943895
15 Mar 2024 : Clinical Research
Evaluation of an Optimized Workflow for the Radiofrequency Catheter Ablation of Paroxysmal Atrial FibrillationMed Sci Monit In Press; DOI: 10.12659/MSM.943526
09 Apr 2024 : Clinical Research
Correlation between Thalamocortical Tract and Default Mode Network with Consciousness Levels in Hypoxic-Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.943802
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952