28 November 2023: Clinical Research
A Study of 45 Patients with Chronic Neck Pain to Compare the Effects on Pain and Disability of 4 Weeks of Physical Therapy with the Active Release Technique and Strain-Counterstrain Manipulation with Massage Alone, Before and After Treatment
Deone KangDOI: 10.12659/MSM.942027
Med Sci Monit 2023; 29:e942027






Abstract
BACKGROUND: Active release technique (ART) and strain-counterstrain (SCS) have been reported to be beneficial for patients with trigger point pain. Therefore, this study of 45 patients with chronic neck pain aimed to compare the effects of 4 weeks of physical therapy with the ART and SCS manipulation with massage alone, evaluated before and after treatment, using the visual analog scale (VAS) for pain, the neck disability index (NDI), and the pressure pain threshold (PPT).
MATERIAL AND METHODS: The participants were 45 adults with neck pain lasting >12 weeks, divided into the ART group (n=15), SCS group (n=15), and control group (n=15). All groups received clinical massage (CM) for 15 min twice a week for 4 weeks. The control group received only CM, the ART group received CM and ART for 15 min twice a week for 4 weeks, and the SCS group received CM and SCS for 15 min twice a week for 4 weeks. VAS, NDI, and PPT were measured before and after the interventions.
RESULTS: In all groups, there were significant changes in VAS, NDI, and PPT after the interventions (P<0.05), and there was a significant difference among groups in the difference before and after intervention (P<0.05). VAS and NDI showed the greatest difference among before and after intervention in the ART group (VAS pre-post 3.38±0.76, NDI pre-post 5.69±2.78). PPT showed the greatest difference among before and after intervention in the SCS group (PPT pre-post 1.75±0.62).
CONCLUSIONS: The ART technique and the SCS technique effectively reduced neck pain and neck disorders in adults with chronic neck pain.
Keywords: Myofascial Release Therapy, Neck Pain, Superficial Back Muscles, trigger points
Background
Neck pain is a common phenomenon that occurs at least once in a lifetime of approximately 70% of the total population. It can be triggered by habitual poor posture or the use of a computer for prolonged periods of time or excessive use of the shoulders and cervical spine [1,2]. In most neck pain cases, the pathoanatomical root of the pain cannot be identified, as neck pain is often a nonspecific condition [3].
There are many potential factors involved in nonspecific neck pain. Recently, scientific evidence has indicated the importance of myofascial trigger points (MTrPs) in its pathogenesis. Although the precise mechanism underlying MTrPs has not yet been elucidated, according to hypotheses formulated in recent studies, involuntary muscle shortening due to muscle tissue injury or overuse [4, 5] and the accumulation of microtrauma due to repetitive overuse, muscle imbalance, and dysfunction of postural alignment contribute to the development of MTrPs [6]. MTrPs present with a characteristic referred type of pain and can restrict functional movement by limiting the range of motion of the affected tissue [7,8]. In addition, MTrPs appear frequently in patients with mechanical neck pain and are associated with muscle shortening and a lowered pressure pain threshold (PPT) [9,10]. Upper trapezius MTrPs that cause neck pain develop due to dysfunction of the soft tissue, which is generally affected by the control of humeroscapular and scapulothoracic movements [11].
Myofascial pain is pain in the body’s muscle and connective tissue known as the fascia, which can be localized or widespread and characterized by multiple trigger points [12]. Myofascial pain may also be associated with range of motion limitations. Although the cause of myofascial pain is not fully understood, muscle overuse or trauma, stress, and postural mechanics can all cause myofascial pain. Treatment of myofascial pain generally includes physical therapy, trigger point injections, drug therapy, and botulism toxin injections [13]. Osteopathic manipulative therapy has also been shown to be effective [14].
The active release technique (ART) is a treatment method used for soft tissue injuries of muscles and myofascia that cause mechanical dysfunction, which can lead to pain and muscle weakness [15]. In this method, soft tissues, including tendons, nerves, and muscle fibers, are treated by releasing tension [16–18]. In addition, ART can be used to identify cumulative damage and to restore function and relieve pain by alleviating adhesions of the injured tissue, adhesions of the acidic tissue, which cause pain, cramping, and soreness, as well as adhesions of the soft tissue [19,20].
Strain-counterstrain (SCS) is a manual therapy technique that uses soft tissue mobilization and is commonly employed in clinical practice to resolve musculoskeletal dysfunction and alleviate pain. In addition, SCS is used as a therapeutic technique for automatically resetting muscle spindles, facilitating control of the length of shortened muscles [21,22]. Recent studies have reported that, based on changes in the PPT and visual analog scale (VAS) score, the SCS technique is effective in reducing hyperalgesia [23–25].
Clinical massage (CM) is a gliding tissue massage technique that focuses on the deeper layers of the fascia and skeletal muscle [26]. CM applied at MTrPs increases the pain-pressure threshold locally and reduces referred pain fields, suggestive of a physiologic change at the MTrP as well as a pain-reducing effect. Trigger point release (formerly referred to as ischemic compression) is a massage technique that consists of moderate compression, typically applied with the fingers, to the MTrP. It is considered an effective and safe method that can manually deactivate MTrP using a direct approach [27].
The increasing use of smartphones and computers is associated with a growing incidence of neck pain, which is recognized as an important clinical problem [28]. Nevertheless, few studies have compared the effects of passive and active therapeutic approaches for treating MTrPs as the causes of nonspecific neck pain [29].
Therefore, this study of 45 patients with chronic neck pain aimed to compare the effects of 4 weeks of physical therapy with ART and SCS manipulation with massage alone, evaluated before and after treatment, using the visual analog scale (VAS) for pain, the neck disability index (NDI), and the pressure pain threshold (PPT).
Material and Methods
ETHICS STATEMENT:
The study design was approved by the Sahmyook University Institutional Review Board (approval no. 2-1040781-AB-N01-2018010HR), In accordance with the Declaration of Helsinki, all subjects were informed about the purpose and procedure of the study and gave their informed consent to participate in the study.
PARTICIPANTS:
The participants were patients who visited the S Clinic in Seoul with concern about neck pain, met the inclusion criteria, and provided consent to participate in the study. With a clinically important effect defines as a 5-point difference among the 2 treatments as, we required a sample of size 15 per group at 5% alpha level and 80% power. Participants were divided into the control group, ART group, and SCS group. The inclusion criteria were: Patients with neck pain for at least 2 months, patients with MTrP that causes tenderness and motor dysfunction, occurs in the upper trapezius muscle, and the hypersensitivity point of the skeletal muscle related to the nodule that can be touched with the hypersensitivity of the tense band in the upper trapezius muscle occur [30]. The exclusion criteria were: diagnosis of fibromyalgia, whiplash injury of the neck, history of cervical spine surgery, pain etiology related to trauma due to a traffic accident, myofascial treatment in the preceding month, abnormal neurological findings, or a suspected herniated disc.
PROCEDURES:
Before the experiment, the patients in each group were subjected to baseline measurements of the VAS score, which is a visual representation of pain severity, the NDI score, which measures the extent of neck disability, and PPT. During the 4-week study period, all 3 groups underwent 8 treatment sessions, each for 15 min, twice per week. The control group only received CM, while the ART group received ART and CM, and the SCS group received SCS and CM. To assess the therapeutic outcomes after 4 weeks, the VAS and NDI scores and PPT were measured in all groups. All measurements were recorded by 2 physical therapists, and 1 physical therapist was assigned to analyze the data.
CLINICAL MASSAGE (CM): CM was administered to all groups to induce muscle relaxation and provide the upper trapezius with nutrients and oxygen required for proper muscle functioning [31]. With the patient lying in a supine position, the upper trapezius MTrPs were massaged using the stripping technique in a longitudinal direction along the muscle fibers and the picking-up-with-palpation technique, in which the thumb and index finger are used to hold the muscle.
ACTIVE RELEASE TECHNIQUE (ART): ART is a non-invasive manual therapy technique that treats soft tissues, including muscles, nerves, and fascia. This technique is a way to treat highly adhesive injuries caused by long-term poor posture [32]. With the patient sitting, the examiner applied force vertically to the MTrP of the upper trapezius muscle. While the therapist was applying pressure (Figure 1A), the patient was instructed to maximally stretch the upper trapezius through contralateral flexion, flexion, and ipsilateral rotation of the neck (Figure 1B). This process was applied for 15 min twice a week for 4 weeks.
STRAIN-COUNTERSTRAIN (SCS): Strain-counterstrain is a treatment method that is effective for pain relief, functional recovery [33], and muscle strength recovery in patients with musculoskeletal disorders [34]. With the patient lying in a supine position, the examiner applied pressure to the upper trapezius MTrPs, manually used flexion, lateral rotation, and abduction of the patient’s ipsilateral arm to maximally relieve tension on the MTrPs, and then maintained the pressure for 90 s (Figure 2). This process was repeated until approximately 70% of the pain was reduced.
VISUAL ANALOG SCALE (VAS): The visual analog scale (VAS) was used to measure the degree of pain. VAS is an assessment tool that allows patients to self-report their current pain level on a scale from 0 (no pain) to 10 (unbearably severe pain). VAS is a simple measurement method that is most commonly used in clinical practice to measure the intensity of pain. It is a highly reliable evaluation tool, with inter-tester reliability of 0.97 [35].
NECK DISABILITY INDEX (NDI): The NDI questionnaire was used to determine the degree of neck disability due to pain. NDI’s Cronbach’s alpha, which indicates the reliability of the tool, was 0.82. The NDI evaluates 10 activities: pain intensity, personal care (eg, dressing), reading, lifting, headaches, work, concentration, driving, sleeping, and leisure activities. Each item is scored from 0 to 5, for a total of 6. There are several possible responses. It is scored as 0 for no pain or functional impairment, and 5 for unbearable pain or complete functional impairment. Therefore, the total score ranges from 0 to 50. Scores were categorized as follows: 0–4 points, no disability; 5–14 points, mild disability; 15–24 points, moderate disability; 25–34 points, severe disability; and ≥35 points, total disability. A higher score means more severe disability [36].
PRESSURE PAIN THRESHOLD (PPT): Pressure pain threshold was used to determine the pain threshold. Using the method described by Fernandez et al for upper trapezius MTrPs in “Pain Diagnosis and Rehabilitation”, PPT was measured, and it was measured in the affected trapezius [8]. This test was performed according to the guidelines explained by Fischer [37]. During the measurement, the subject was in the supine position. The pressure pain threshold measuring device was placed perpendicular to the trigger point of the trapezius muscle, and pressure was applied at a rate of approximately 1 kg/cm2/s until the pressure was recognized as pain. The pressure displayed on the instrument panel was measured by reporting to the experimenter.
STATISTICAL ANALYSIS:
A Shapiro-Wilk test was used to examine the normality of each item, and paired-sample
Results
CHANGE OF PAIN BEFORE AND AFTER THE INTERVENTION:
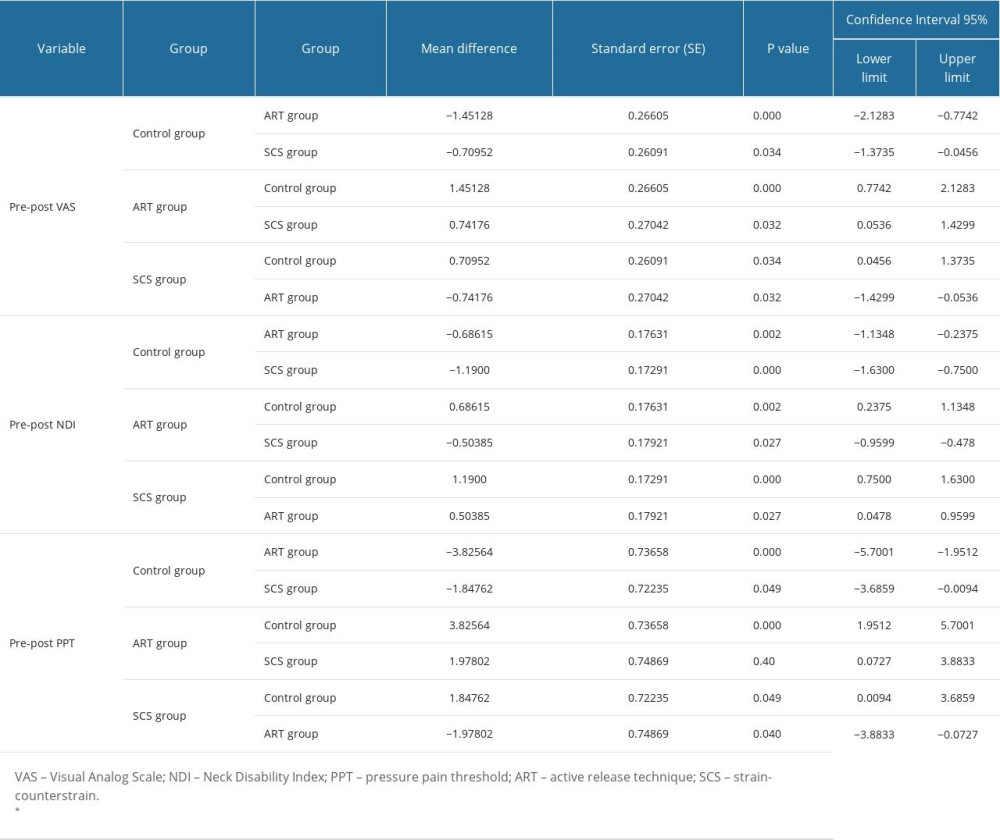
There was a significant difference in VAS scores before and after intervention in all 3 groups (P<0.05) (Table 1). The control group significantly decreased from 4.86±1.47 before the intervention to 2.93±1.16 after the intervention, the ART group significantly decreased from 5.53±1.39 before the intervention to 2.15±0.68 after the intervention, and the SCS group significantly decreased from 4.21±1.05 before the intervention to 2.57±0.64 after the intervention. The VAS score pre-post values of the control group were 1.93±0.59 for the control group, 3.38±0.76 for the ART group, and 2.64±0.74 for the SCS group. The ART group showed the largest decrease, and the pre-post values showed a significant difference among groups (P<0.05) (Table 2).
CHANGE IN NECK DISABILITY INDEX BEFORE AND AFTER THE INTERVENTION:
The NDI of the 3 groups showed significant differences before and after intervention (P<0.05) (Table 1). The control group significantly decreased from 11.06±3.05 before the intervention to 9.20±2.80 after the intervention, the ART group significantly decreased from 13.00±5.19 before the intervention to 7.30±2.81 after the intervention, and the SCS group significantly decreased from 11.57±4.78 before the intervention to 7.85±3.27 after the intervention. The NDI pre-post values were 1.86±0.91 for the control group, 5.69±2.78 for the ART group, and 3.71±1.81 for the SCS group. The ART group showed the largest decrease, and the pre-post values showed a significant difference among groups (P<0.05) (Table 2).
CHANGE IN PRESSURE PAIN THRESHOLD BEFORE AND AFTER THE INTERVENTION:
The PPT of the 3 groups showed significant differences before and after intervention (P<0.05). The control group significantly decreased from 2.94±0.84 before the intervention to 3.50±0.84 after the intervention, the ART group significantly decreased from 2.35±0.69 before the intervention to 3.60±0.48 after the intervention, and the SCS group significantly decreased from 2.27±0.87 before the intervention to 4.02±0.68 after the intervention. The PPT pre-post values for the control group were 0.56±0.21 for the control group, 1.24±0.47 for the ART group, and 1.75±0.62 for the SCS group. The SCS group showed the largest increase, and the pre-post values showed a significant difference among groups (P<0.05) (Table 1).
Discussion
This study evaluated and compared the effects of ART and SCS on neck pain, pain threshold, and neck dysfunction. In this study, ART and SCS improved VAS, NDI, and PPT, and the differences among groups were significant. As a result of comparison among groups, VAS and NDI showed the greatest decrease in the ART group, and the improvement in PPT was greatest in the SCS group.
Previous studies have investigated the changes in pain using the treatment techniques mentioned above. Specifically, Tak et al (2013) administered ART to the gluteus medius of 24 chronic low back pain patients for 20 min per session, 2 sessions per week, for 3 weeks, and reported a significant decrease in VAS scores [12]. A previous study reported a decrease in VAS and recovery of ROM when ART was applied to the iliotibial band to treat external coxa saltans [15]. A study by Lee S-J, applying ART to patients with supraspinatus rupture 3 to 5 times a week for about 4 weeks, showed an increase in shoulder ROM and a decrease in VAS [17]. A study by Nagrale that applied SCS to patients with nonspecific neck pain found that VAS and NDI were significantly improved [22]. Another study reported significant effects in VAS, PPT, and ROM after applying ART and JM to the muscles involved in neck movements in 24 neck pain patients for 20 min per session, twice per week, for 3 weeks [38].
Previous studies have reported that ART application results in pain reduction and ROM recovery by removing adhesions in damaged tissues, and SCS application has been reported to benefit tissue length and tension through automatic resetting of muscle spindles. In addition, it has been reported that treatment involving active movement not only promotes muscle relaxation through sympathetic nerve stimulation through muscle and joint-based mechanisms, but also has a physiological effect in reducing pain [39]. This indicates that ART and SCS promote relaxation of muscle fiber segments and are therefore suitable treatment options for MTrP and pain relief. The results of this study are consistent with the results of a previous study that found that ART and SCS reduced pain and restored neck function through reduction of intratissue adhesions and tissue tension.
When we analyzed NDI scores, we observed statistically significant post-treatment changes in all 3 experimental groups (
Previous studies investigating NDI score improvement and functional recovery in patients with neck pain using these treatment methods, SCS and the muscle energy technique in combination with the ischemic compression technique to the upper trapezius MTrPs in patients with nonspecific neck pain reported significant decreases in pain and NDI scores [22]. In another study, patients with neck pain were divided into male and female patient groups, and when the effects of ART were compared, both groups showed a significant decrease in NDI scores [40]. Based on these studies, it is postulated that the greater reduction in NDI score with ART and SCS than with CM that was seen in our study was due to improved functional movements of daily living.
When we measured the PPT, a significant increase was noted after the treatment in both test groups and the control group (
Among previous studies using these treatment methods to investigate their effect on PPT, 1 study analyzed immediate effects after applying ART to patients with an adductor injury and reported a significant increase in PPT [41]. Another study reported immediate reduction in PPT and functional recovery in patients with back pain by applying SCS to digitally tender points involved in back pain [19,20]. Meseguer et al reported that the sensitivity to tenderness of tender points was immediately reduced as a result of applying existing SCS and SCS with added vertical strokes to the upper trapezius in patients with neck pain [21]. In a studied examining the effects of applying SCS to the upper trapezius MTrPs reported a 33% increase in PPT [42]. Regarding the pain relief observed in the aforementioned studies, SCS has been shown to inhibit excessive secretion of acetylcholine, thereby preventing continuous contracture of muscle fibers [6]. Similar to previous study findings, we found that SCS and ART were effective in improving PPT in our study, and the combination of SCS and CM further enhanced the effects on PPT.
Several limitations should be considered in interpreting the results of this study. First, because the number of participants was relatively small and they were recruited from a single hospital, it is difficult to generalize the results to all individuals with neck pain. Second, it is not possible to draw conclusions about long-term treatment effects due to the short study period of 4 weeks. Therefore, to evaluate the independent intervention effects of ART and SCS only in patients with neck pain, a follow-up study with a larger sample size and longer duration is needed. Third, in this study, pain and neck dysfunction were reduced through ART and SCS, but the independent treatment effect of ART and SCS could not be determined. Thus, to completely resolve the pain reduction and functional recovery of neck pain, a complex rehabilitation protocol related to neck pain is necessary.
Conclusions
The purpose of this study was to investigate and compare the effects of ART, SCS, and CM on pain and disability in adults with chronic neck pain. As a result of the study, the effects of ART and SCS were confirmed for the improvement of VAS, NDI, and PPT in patients with neck pain.
Figures
 Figure 1. Active Release Technique (ART) Procedure. (A) Active Release Technique (ART): Pressure applied to upper trapezius myofascial trigger points (MTrPs). (B) ART: While maintaining pressure, the patient’s neck is subjected to lateral flexion, flexion, and ipsilateral rotation.
Figure 1. Active Release Technique (ART) Procedure. (A) Active Release Technique (ART): Pressure applied to upper trapezius myofascial trigger points (MTrPs). (B) ART: While maintaining pressure, the patient’s neck is subjected to lateral flexion, flexion, and ipsilateral rotation.  Figure 2. Strain-counterstrain technique procedure. After compressing the trigger point of the upper trapezius muscle while maintaining pressure, the experimenter finds the point of lowest tension through flexion, abduction, and external rotation of the subject’s shoulder and maintains the posture.
Figure 2. Strain-counterstrain technique procedure. After compressing the trigger point of the upper trapezius muscle while maintaining pressure, the experimenter finds the point of lowest tension through flexion, abduction, and external rotation of the subject’s shoulder and maintains the posture. 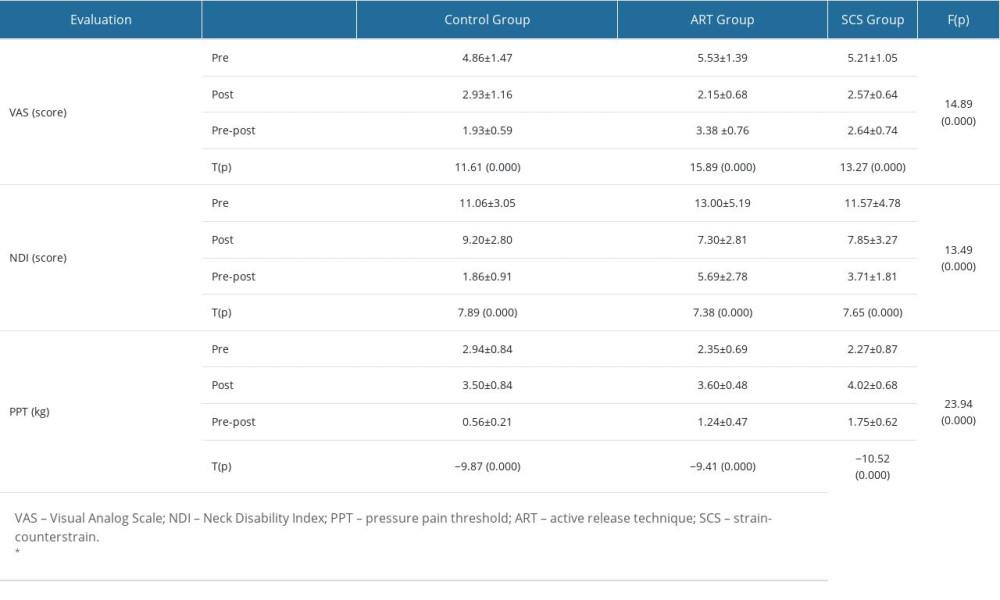
References
1. Chung SH, Her JG, Ko T, Effects of exercise on deep cervical flexors in patients with chronic neck pain: J Phys Ther Sci, 2012; 24(7); 629-32
2. Mangone M, Paoloni M, Procopio S, Sagittal spinal alignment in patients with ankylosing spondylitis by rasterstereographic back shape analysis: An observational retrospective study: Eur J Phys Rehabil Med, 2020; 56(2); 191-96
3. Borghouts JA, Koes BW, Bouter LM, The clinical course and prognostic factors of non-specific neck pain: A systematic review: Pain, 1998; 77(1); 1-13
4. Mense S, Simons DG, Russell IJ: Muscle pain: Understanding its nature, diagnosis, and treatment, 2001, Lippincott Williams & Wilkins
5. Travell JG, Simons DG: Myofascial pain and dysfunction, 1999, Baltimore, Williams and Wilkins
6. Huguenin LK, Myofascial trigger points: The current evidence: Phys Ther sport, 2004; 5(1); 2-12
7. Harden RN, Bruehl SP, Gass S, Signs and symptoms of the myofascial pain syndrome: A national survey of pain management providers: Clin J Pain, 2000; 16(1); 64-72
8. Fernandez-de-Las-Penas C, Alonso-Blanco C, Miangolarra J, Myofascial trigger points in subjects presenting with mechanical neck pain: A blinded, controlled study: Man Ther, 2007; 12(1); 29-33
9. Fischer AA, Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold: Pain, 1987; 30(1); 115-26
10. Jonsson E, Nachemson A: Neck and back pain: the scientific evidence of causes, diagnosis, and treatment, 2000, Lippincott Williams & Wilkins
11. Seo J, Song C, Shin D, A single-center study comparing the effects of thoracic spine manipulation vs mobility exercises in 26 office workers with chronic neck pain: A randomized controlled clinical study: Med Sci Monit, 2022; 28; e937316
12. Giamberardino MA, Affaitati G, Fabrizio A, Costantini R, Myofascial pain syndromes and their evaluation: Best Pract Res Clin Rheumatol, 2011; 25(2); 185-98
13. Esenyel M, Caglar N, Aldemir T, Treatment of myofascial pain: Am J Phys Med Rehabil, 2000; 79(1); 48-52
14. Kashyap R, Iqbal A, Alghadir AH, Controlled intervention to compare the efficacies of manual pressure release and the muscle energy technique for treating mechanical neck pain due to upper trapezius trigger points: J Pain Res, 2018; 11; 3151-60
15. Tak S, Lee Y, Choi W, Lee G, The effects of active release technique on the gluteus medius for pain relief in persons with chronic low back pain: Phys Ther Rehabil Sci, 2013; 2(1); 27-30
16. Drover JM, Forand DR, Herzog W, Influence of active release technique on quadriceps inhibition and strength: A pilot study: J Manipulative Physiol Ther, 2004; 27(6); 408-13
17. George JW, Tepe R, Busold D, The effects of active release technique on carpal tunnel patients: A pilot study: J Chiropr Med, 2006; 5(4); 119-22
18. Spina AA: J Can Chiropr Assoc, 2007; 51(1); 23
19. Brian A, Kamali A, Michael Leahy P, Release your pain: resolving repetitive strain injuries with active release techniques: Pub Group West, 2005; 15-29
20. Lee S-J, Park J-H, Nam S-H, Kang J-H, Two clinical cases of active release technique with Koeran Medicine treatment for supraspinatus tendon partial tear: The Journal of Korea CHUNA Manual Medicine for Spine and Nerves, 2014; 9(1); 89-101
21. Jones L, Kusunose R, Goering E: Jones Strain-Counterstrain, 1995, Idaho, Jones Strain-Counterstrain. Inc
22. Lewis C, Flynn TW, The use of strain-counterstrain in the treatment of patients with low back pain: J Man Manip Ther, 2001; 9(2); 92-98
23. Lewis C, Khan A, Souvlis T, Sterling M, A randomised controlled study examining the short-term effects of strain-counterstrain treatment on quantitative sensory measures at digitally tender points in the low back: Man Ther, 2010; 15(6); 536-41
24. Meseguer AA, Fernández-de-las-Peñas C, Navarro-Poza JL, Immediate effects of the strain/counterstrain technique in local pain evoked by tender points in the upper trapezius muscle: Clinical Chiropractic, 2006; 9(3); 112-18
25. Nagrale AV, Glynn P, Joshi A, Ramteke G, The efficacy of an integrated neuromuscular inhibition technique on upper trapezius trigger points in subjects with non-specific neck pain: A randomized controlled trial: J Man Manip Ther, 2010; 18(1); 37-43
26. Koren Y, Kalichman L, Deep tissue massage: What are we talking about?: J Bodyw Mov Ther, 2018; 22(2); 247-51
27. Simons DG, Travell J, Simons LS: Myofascial pain and dysfunction: The trigger point manual: volume 1, 1999
28. Masiero S, Litwocenko S, Agostini F, Rehabilitation in an Italian thermal setting: A new therapeutic strategy for patients with musculoskeletal disability – the results of an Italian survey: Int J Biometeorol, 2020; 64(6); 951-54
29. Sarig-Bahat H, Evidence for exercise therapy in mechanical neck disorders: Man Ther, 2003; 8(1); 10-20
30. Simons DG, Travell JG, Simons LS: Travell & Simons’ myofascial pain and dysfunction: Upper half of body, 1999, Lippincott Williams & Wilkins
31. Tappan MB, Power, privilege, and critique in the study of moral development: Hum Dev, 2000; 43(3); 165-69
32. Abelson B, Abelson KT: Release your pain: Resolving repetitive strain injuries with active release techniques, 2004, Calgary, Rowan Tree Books
33. Dardzinski BJ, Smith SL, Towfighi J, Increased plasma beta-hydroxybutyrate, preserved cerebral energy metabolism, and amelioration of brain damage during neonatal hypoxia ischemia with dexamethasone pretreatment: Pediatr Res, 2000; 48(2); 248-55
34. Wong CK, Schauer C, Reliability, validity and effectiveness of strain counterstrain techniques: J Man Manip Ther, 2004; 12(2); 107-12
35. Bijur PE, Silver W, Gallagher EJ, Reliability of the visual analog scale for measurement of acute pain: Acad Emerg Med, 2001; 8(12); 1153-57
36. Vernon H, Mior S, The Neck Disability Index: A study of reliability and validity: J Manipulative Physiol Ther, 1991; 14(7); 409-15
37. Fischer AA, Introduction: Pressure algometry in quantification of diagnosis and treatment outcome: J Musculoskelet Pain, 1998; 6(1); 1-3
38. Kim JH, Lee HS, Park SW, Effects of the active release technique on pain and range of motion of patients with chronic neck pain: J Phys Ther Sci, 2015; 27(8); 2461-64
39. Kumar GY, Sneha P, Sivajyothi N, Effectiveness of muscle energy technique, ischaemic compression and strain counterstrain on upper trapezius trigger points: A comparative study: International journal of physical education, sports and Health, 2015; 1(3); 22-26
40. Rafaqat A, Usman M, Shahzad MF, Sattar MI, Effects of active release technique in males as compared to females with postural and psychological cervical muscle spasm: A Quasi experimental study: Italian Journal of Sports Rehabilitation and Posturology, 2018; 4; 870-87
41. Robb A, Pajaczkowski J, Immediate effect on pain thresholds using active release technique on adductor strains: pilot study: J Bodyw Mov Ther, 2011; 15(1); 57-62
42. Jung J-H, Lee N-G, You S-H, Immediate effects of strain-counterstrain technique on pressure pain threshold and muscle activity in male adults with upper trapezius latent trigger point: Physical Therapy Korea, 2011; 18(2); 76-83
Figures
Figure 1. Active Release Technique (ART) Procedure. (A) Active Release Technique (ART): Pressure applied to upper trapezius myofascial trigger points (MTrPs). (B) ART: While maintaining pressure, the patient’s neck is subjected to lateral flexion, flexion, and ipsilateral rotation.Figure 2. Strain-counterstrain technique procedure. After compressing the trigger point of the upper trapezius muscle while maintaining pressure, the experimenter finds the point of lowest tension through flexion, abduction, and external rotation of the subject’s shoulder and maintains the posture. In Press
11 Mar 2024 : Clinical Research
Comparison of Effects of Sugammadex and Neostigmine on Postoperative Neuromuscular Blockade Recovery in Pat...Med Sci Monit In Press; DOI: 10.12659/MSM.942773
12 Mar 2024 : Clinical Research
Comparing Neuromuscular Blockade Measurement Between Upper Arm (TOF Cuff®) and Eyelid (TOF Scan®) Using Miv...Med Sci Monit In Press; DOI: 10.12659/MSM.943630
11 Mar 2024 : Clinical Research
Enhancement of Frozen-Thawed Human Sperm Quality with Zinc as a Cryoprotective AdditiveMed Sci Monit In Press; DOI: 10.12659/MSM.942946
12 Mar 2024 : Database Analysis
Risk Factors of Age-Related Macular Degeneration in a Population-Based Study: Results from SHIP-TREND-1 (St...Med Sci Monit In Press; DOI: 10.12659/MSM.943140
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952