23 August 2020: Clinical Research
Normal Pancreas Graft Appearance in Magnetic Resonance Diffusion Tensor Imaging (DTI)
Agnieszka Surowiecka1CDE, Michał Frączek2D, Bartosz Mruk2F, Marta Matejak-Górska1B, Jerzy Walecki2A, Marek Durlik1A, Katarzyna Sklinda2ABCDEFG*DOI: 10.12659/MSM.920262
Med Sci Monit 2020; 26:e920262






Abstract
BACKGROUND: The main purpose of diagnostic imaging after pancreas transplantation is to exclude potential complications. As long as standard anatomical imaging such as sonography, contrast-enhanced computed tomography, and magnetic resonance imaging (MRI) are sufficient to display macroscopic vasculature, early changes within the graft caused by insufficient microperfusion will not be displayed for evaluation.
MATERIAL AND METHODS: Patients with pancreas allograft function in good condition were included in the study. No specific preparation was demanded before the MRI examination. The results of MRI were correlated with Igls criteria. It was a preliminary study to examine diffusion tensor imaging (DTI) value and safety in pancreas transplantation.
RESULTS: Our results indicated that higher fractional anisotropy (FA) values of the graft’s head were associated with delayed graft function and insulin intake. We also compared grafts’ images in early and late periods and found differences in T1 signal intensity values. DTI is a reliable noninvasive tool, requiring no contrast agent, to assess graft microstructure in correlation with its function, with FA values showing the most consistent results. By Igls criteria, no graft failure, 76% had optimal function, 10% had good function, and 14% had marginal function.
CONCLUSIONS: Our results suggest that DTI can be safely used in patients after pancreas transplantation and is advantageous in detecting early as well as late postoperative complications such as intra-abdominal fluid collection, malperfusion, and ischemia of the graft. Our findings correspond with clinical condition and Igls criteria. DTI is free of ionizing agents and is safe for kidney grafts.
Keywords: Diffusion Magnetic Resonance Imaging, diffusion tensor imaging, Magnetic Resonance Imaging, Pancreas Transplantation, Allografts, Anisotropy, C-peptide, Contrast Media, Delayed Graft Function, Glycated Hemoglobin A, Hypoglycemia, Insulin, Insulin-Secreting Cells, Ischemia, Postoperative Complications, Prospective Studies, Transplantation, Homologous
Background
Pancreas transplantation is a one of the curative options for selected diabetic patients with confirmed organ complications or rigid course resistant to conservative treatment [1]. Simultaneous pancreas and kidney transplantation (SPK), in comparison with kidney transplantation from a deceased donor or kidney transplantation from a living donor, gives best long-term survival and quality of life for diabetic patients with end-stage renal disease [2]. The pancreas can also be transplanted alone (PTA) or after kidney transplantation (PAK) from deceased as well as living donors [3]. Candidates for pancreas transplantation are those diagnosed with brittle diabetes resistant to all available pharmacological agents, with symptoms of severe metabolic acidosis, recurrent episodes of serious silent nocturnal hypoglycemia, and rapid development of microangiopathies [4]. The first pancreas transplant was performed by Kelly et al. in 1966 [5]. Since then the results of transplantation have improved, and now the estimated 5-year graft survival is 73% [1].
Pancreas transplantation provides diabetic patients with the endocrine component of the pancreas. The pancreatic islets of Langerhans are spherical, with a mean diameter of 50 to 500 μm, and are organized in clusters. The smallest clusters are usually vascularized with one artery, whereas bigger ones have 2 to 5 arterioles. Usually these are end arteries. Intralobular arteries create a network surrounding the parenchyma, forming fenestrated capillary plexuses inside the lobules. The vascularization is delivered to the islet first, and then to the acini, forming an “insuloacinar” portal system. [6,7]. Lobules are innervated by sympathetic, parasympathetic, and sensory nerves [8]. Pancreatic parenchyma is very sensitive to ischemia and hypoperfusion. Parenchymal microcirculation is impaired by ischemia time, reperfusion syndrome, and mechanical injury during allograft harvesting and transplantation [9]. Disturbances in microcirculation can lead to inflammation, edema, and necrosis [6]. The complications after pancreas transplantation can be divided into surgical and nonsurgical. Early vascular complications, including vascular full thrombosis, in most cases lead to graft loss. Other complications, such as graft pancreatitis or rejection, are difficult to diagnose [10]. Still, the trigger of graft pancreatitis remains unclear and potentially disturbances in microcirculation can be one of the main causes. Usually, the diagnosis is made on the basis of clinical, laboratory, and radiological findings; in the case of rejection suspicion, also on fine-needle biopsy.
Ultrasound (US) and contrast-enhanced computed tomography (CECT) are imaging modalities commonly used for the evaluation of a pancreas transplant. Each of them has its unique advantages.
Magnetic resonance imaging (MRI) is gaining acceptance for evaluation of the graft including vascular complications [11] and the whole abdomen. Contrast agents may have a harmful effect on kidney allograft’s function, and some protocols exclude contrast-enhanced sequences when pancreatic graft abnormalities are suspected [12].
Diffusion-weighted imaging (DWI) is a noninvasive MRI technique that does not require contrast administration and provides indirect information about cellular microstructure of an examined organ. It enables quantitative evaluation of restriction of movement of water molecules between cells as average apparent diffusion coefficient (ADC) independent from the direction of the diffusion process in a defined structure. Diffusion tensor imaging (DTI), on the other hand, measures the diffusion coefficients in defined directions. It is superior to DWI as it estimates diffusion anisotropy, providing information regarding microstructure of the examined tissue [13]. In DTI, data about the magnitude of water’s mobility (ADC) and its directionality are denoted by fractional anisotropy (FA). Hence, in this study we intend to compare FA and ADC values of a healthy control group with those of patients who received pancreatic allografts. We also intend to determine the trend in change of values of FA and ADC with disease progression. The Igls criteria are the International Pancreas and Islet Transplant Association (IPITA)/European Pancreas and Islet Transplant Association (EPITA) statement established in 2018 defining the function of the pancreas graft [14]. The factors included in the score are glycated hemoglobin, episodes of hypoglycemia, insulin requirement, and C-peptide (Table 1).
Material and Methods
ETHICAL STATEMENT:
The Internal Review Board of CSK MSWiA approved all protocols and all patients gave written consent to participate in the study. Twenty one pancreas graft patients participated in this prospective study from February to April 2019.
INCLUSION CRITERIA:
All patients underwent pancreas transplantation. DTI was performed only on stable patients without serious clinical complications, in good clinical condition. Only patients with pancreas allograft function were included in the study. The period from pancreas transplantation to MRI was a minimum of 10 days. We divided our cohort into two groups: early (within the first 3 months after transplantation) and late (more than 3 months after transplantation). Additionally, from February to April 2019, ten healthy volunteers were examined as a control group.
CONTROL GROUP:
Before performing this study, we enrolled 10 volunteers who underwent MRI because of nonpancreatic conditions. The FA and ADC values of these autologous pancreases were a guideline. However, pancreas graft has different vascularization from autologous pancreases, and we did not compare these values with pancreatic graft. We decided to consider patients with clinical symptoms of good graft function as “healthy” pancreatic graft and as a reference to a malfunctioning pancreas graft. These values were compared via statistical analysis.
SURGICAL TECHNIQUE AND MANAGEMENT:
The preprocurement pancreas suitability score was used for the selection of the donors. Recipient qualification was performed at our center. Our clinic possesses the permission of the Polish Ministry of Health to conduct pancreas and kidney transplantations (date of current permission 22 December 2017, expires in 2022).
The mesenteric superior artery and splenic artery were reconstructed into a Y-graft with the donor’s iliac artery. We do not elongate the portal vein routinely. After exposition of the right retroperitoneal space, we dissected the distal vena cava and right iliac arteries. We created end-to-side continuous vascular anastomoses. Then we performed enteric drainage to the first segments of the intestine, as it enables an endoscopic approach in case of bleeding or need for a duodenum biopsy.
We examined patients with US daily in the early period (day 0–day 10) after transplantation. Routinely, CECT was performed 3 months after the transplantation. If complications were suspected, additional US and CT examinations were done.
The immunosuppressive therapy scheme at our clinic consists of induction (monoclonal or polyclonal antibodies) and steroids, calcineurin inhibitors, and antiproliferative agents (mycophenolate). We do not use intraoperative heparinization. After transplantation we administer low-molecular-weight heparin in prophylactic doses, dependent-form epidermal growth factor receptor for 3 months, and then continue with oral acetylsalicylic acid.
MRI PROTOCOLS:
Before the MRI examination no specific preparation was demanded. The MRI protocols were acquired on a 3 Tesla (3T) MRI Philips scanner (Philips Ingenia; Philips Healthcare, the Netherlands). Transmitting body coil and a receiving multichannel body matrix and spine matrix coils (Philips Ingenia) were applied. A bellows belt (Philips Ingenia) was placed on the chest for respiratory triggering, and a dielectric pad (Philips Ingenia) used to avoid effects due to radiofrequency interference was placed on the abdomen [13].
The DTI protocol was acquired with a fat-suppressed, respiratory-triggered spin-echo sequence using 15 diffusion gradient directions at
All examinations included a T2-weighted axial fast two-dimensional protocol, without and with fat suppression, using a respiratory-triggered spin-echo sequence with TE/TR of 59/3000 ms, generalized autocalibrating partially parallel acquisition with parallel imaging factor 2, and the same slice thickness as in the DTI protocol. The nominal acquisition time was 2.52 min.
STATISTICAL ANALYSIS:
Statistical analysis was performed with Statistica 12 software (StatSoft, Poland). Continuous and categorical variables were compared between the study group and the control group using Student’s
CLINICAL EVALUATION:
We used the Igls criteria to define the function of the pancreatic graft. DTI results were correlated with the Igls criteria.
LIMITATIONS:
The limitation of the study results from a small number of patients, even though we are the biggest pancreatic center in Poland, with 227 pancreases transplanted. Pancreas transplantation is a rare and expert procedure. Each year we transplant approximately 20 pancreases: SPK, PTA, or PAK.
Results
The FA values in a healthy pancreas are 0.26 for the parenchyma. Hypovascular lesion and malperfusion are detected in DTI as lower FA values, whereas solid tumors are characterized by higher FA.
There were 21 patients enrolled in the study. The mean age of the whole group was 41 years. The mean time of DTI examination was 775 days after transplantation (minimum 7, maximum 5200; standard deviation [SD] 1352). Eighty percent of MRIs were performed after SPKs, 2 in PTAs, and 1 on retransplantation and PAK. Delayed graft function (DGF) was diagnosed in the early group; there was a history of DGF in the late group. There were no significant differences found between the clinical features of the groups.
By the Igls criteria, no graft failure, 76% had an optimal function, 10% were good, and 14% had marginal function. The FA of the pancreatic head and the FA head ratios were higher in the marginal group in comparison with the optimal group (
The early group (less than 30 days posttransplantation) consisted of 83% males. The mean age was 41 years. The mean C-peptide level was 8 (3.4–10.7; SD 2.8) and C-reactive protein 60 (2–160; SD 48). There were 2 cases of DGF and pancreatitis. According to Igls criteria in these two cases a good graft function was detected.
The DTI head and tail ratios were higher in the early group (
Among patients with DGF the FA of the pancreatic head and FA head ratio were higher. (head: DGF median FA value 0.53, non-DGF 0.265,
A healthy pancreas was diagnosed when there was no history of pancreatitis, DGF, or insulin intake. The T1 of the iliopsoas was higher in the healthy group (
Discussion
Diagnostic imaging is essential for the postoperative evaluation of the transplanted pancreas allograft and decision making in further management. US is readily available, portable, lacks ionizing radiation, does not demand intravenous contrast medium administration, and may provide a complete diagnosis; therefore it is the first imaging technique used [12]. However, the graft may not be visualized well because of postoperative changes or bowel gas. CECT of the pancreas allograft is an imaging modality that clearly demonstrates postsurgical anatomy of the graft, the vasculature, abdominal contents, and most of the surgical complications. Its main disadvantages are ionizing radiation and intravenous contrast medium administration, which is potentially harmful for transplanted kidneys. DTI is a modality that provides information about the microstructure of the tissues through the quantification of free diffusion of water molecules between cells. Clinical conditions such as malperfusion, inflammation, and fibrosis should influence DTI values as the lead to changes in the microenvironment of the pancreas. Indices commonly derived from DTI include mean diffusivity independent of direction, FA or relative anisotropy, axial diffusivity, and radial diffusivity. In our study, FA values were assessed using circular regions of interest drawn in the head, trunk, and tail of the transplanted pancreas. According to our knowledge, no methodology was proposed earlier to access the transplanted pancreas with DTI. There has been, however, a study on transplanted kidney allografts in which kidneys with rejection or acute tubular necrosis had lower FA values [13]. In early kidney grafts, normal grafts of the medullar ADC and FA were higher, whereas cortical measurements were lower than in a graft with deteriorated function [14]. In our study there were no significant differences between the head, body, and tail of a pancreas allograft, but the FA of the head was higher in the DGF group.
MRI performed on a 3T scanner is comparable with CT in terms of spatial resolution but does not demand ionizing radiation and iodine-based contrast agents. Even though MRI is useful in defining pancreatic vasculature and parenchyma, it is less valuable in evaluating fluid collections and intestinal obstructions [11]. In pathologic conditions causing rise in cell numbers such as edema, inflammation, necrosis, and neoplasm, the image changes. In contrast to the other imaging modalities, DWI enables not only qualitative but also quantitative evaluation of the examined structure. DTI is even more detailed in giving an opportunity to understand the pathophysiological processes of the disease by providing knowledge of the structure and, indirectly, function of the examined organ. So far the potential of DTI to reveal the complex microstructure and physiology of the transplanted pancreas and detect pathological changes has not been investigated.
Relative hyperintensity of T1-weighted and T2-weighted images is typical for the normal pancreas graft because of protein- and water-based exocrine secretions produced by the gland. Coronal and axial images are useful in displaying pancreatic and peripancreatic graft edema, as occurs in pancreatitis, and in characterizing peritransplant fluid collections (hematoma). In our study T1 values of the pancreatic head and body were higher in later observations, which is secondary to concentration of proteins.
Patients are referred for MRI less frequently than for CT because of time consumption and issues regarding patients’ general state. MRI evaluation of pancreas grafts is at least as valuable as CECT in evaluation of prostatic parenchyma, vasculature, and surrounding tissue but it is inferior to CT in the evaluation of bowel complications.
In our study, FA values in patients with DGF were significantly higher than in normal controls (
In our series, we found that patients with DGF had higher SI in the head of pancreas. The reason for this is probably increased concentration of proteins excreted into the extracellular space, causing increase of SI. Again, the described pathology is limited to the graft’s head, which is supplied by the mesenteric artery, even though there was a correlation among T1 SI values of the graft’s head, body, and tail.
MRI has specific technical limitations such as patient motion artifacts and metallic clip artifacts, which can obscure the pancreatic and peripancreatic vasculature. Image resolution may be limited by patients’ motion, including jejunal peristalsis, the large fields of view used in the imaging of the pelvis and abdomen, and the long readouts in diffusion imaging that are susceptible to off-resonance and eddy current artifacts.
DGF is a poorly characterized condition. The interpretation of this observation demands further analysis and comparison with pathomorphological studies; however, changes in FA values remain in keeping with regions of vascular supply. Therefore it is probable that it reflects microedema of acini followed by diminished excretory function. Increased value of FA may indicate the rise of organization within the pancreatic head structure in keeping with neovascularization or early fibrosis.
Conclusions
Interpretation of an image of a transplanted pancreas requires a knowledge of surgical anatomy and possible early and late complications. Our results suggest that DTI can be safely used in patients after pancreas transplantation and is advantageous in detecting early, as well as late, postoperative complications such as intra-abdominal fluid collections, malperfusion, and ischemia of the graft. Our findings correspond with clinical condition and Igls criteria. DTI is free of ionizing agents and is safe for the kidney graft. FA values are credible indicators of early changes in graft parenchyma and in later grafts’ functional deterioration. Even with a small number of patients, we showed that DTI is a promising tool in pancreatic graft clinical evaluation. We believe that a greater number of patients should be enrolled in future studies.
Figures
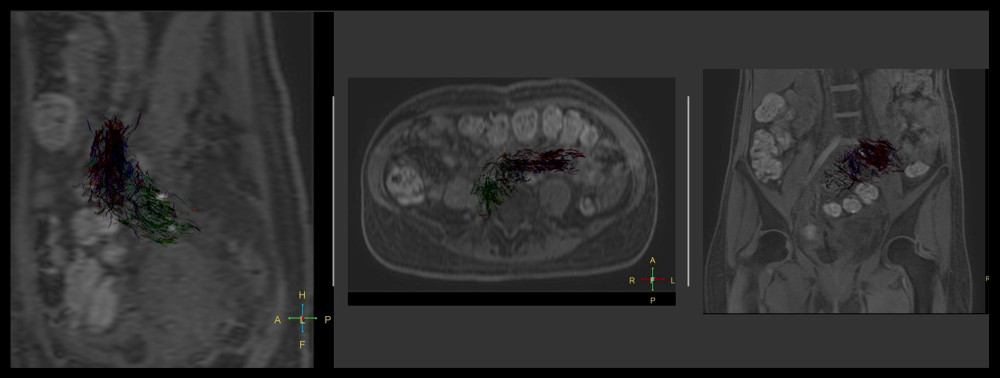 Figure 1. Diffusion tensor imaging (DTI) reconstruction of transplanted pancreas superimposed on DTI b0; sagittal, axial, and coronal images.
Figure 1. Diffusion tensor imaging (DTI) reconstruction of transplanted pancreas superimposed on DTI b0; sagittal, axial, and coronal images. 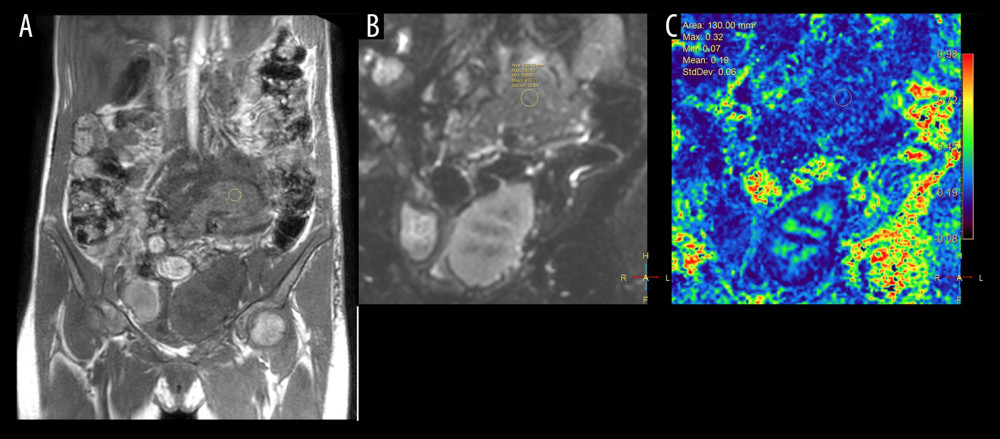 Figure 2. T1W (A), diffusion tensor imaging (DTI) b0 (B), and DTI fractional anisotropy map (C). DTI measures in the head of the transplanted pancreas ranged from 0.07 to 0.32, with a mean value of 0.19.
Figure 2. T1W (A), diffusion tensor imaging (DTI) b0 (B), and DTI fractional anisotropy map (C). DTI measures in the head of the transplanted pancreas ranged from 0.07 to 0.32, with a mean value of 0.19. 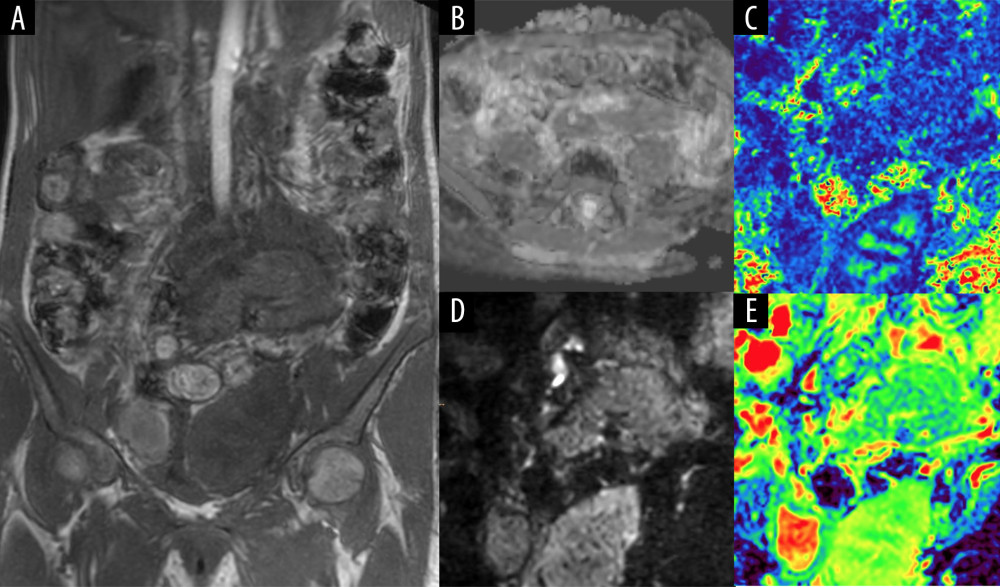 Figure 3. (A) Dixon T1-weighted image, coronal section. (B) Apparent diffusion coefficient map from isotropic diffusion-weighted images, axial section. (C) Fractional anisotropy map from diffusion tensor imaging (DTI), coronal section. (D) Isotropic diffusion image from DTI, b value 800, coronal section. (E) Apparent diffusion coefficient map from DTI, coronal section.
Figure 3. (A) Dixon T1-weighted image, coronal section. (B) Apparent diffusion coefficient map from isotropic diffusion-weighted images, axial section. (C) Fractional anisotropy map from diffusion tensor imaging (DTI), coronal section. (D) Isotropic diffusion image from DTI, b value 800, coronal section. (E) Apparent diffusion coefficient map from DTI, coronal section. Tables
Table 1. Igls criteria [14].![Igls criteria [14].](https://jours.isi-science.com/imageXml.php?i=t1-medscimonit-26-e920262.jpg&idArt=920262&w=1000)
References
1. Gruessner AC, Gruessner RW, Long-term outcome after pancreas transplantation: A registry analysis: Curr Opin Organ Transplant, 2016; 21; 377-85
2. Wai PW, Sollinger HW, Long-term outcomes after simultaneous pancreas-kidney transplant: Curr Opin Organ Transplant, 2011; 16; 128-34
3. Laftavi MR, Gruessner A, Gruessner R, Surgery of pancreas transplantation: Curr Opin Organ Transplant, 2017; 22; 389-97
4. Kałuża B, Durlik M, Grzeszczak W, Qualification of patients with diabetes to pancreas transplantation alone: Diabet Klin, 2013; 2(5); 172-77
5. Farney AC, Rogers J, Stratta RJ, Pancreas graft thrombosis: Causes, prevention, diagnosis, and intervention: Curr Opin Organ Transplant, 2012; 17; 87-92
6. Cuthbertson MB, Christophi C, Disturbances of the microcirculation in acute pancreatitis: Br J Surg, 2006; 93; 518-30
7. Henry BM, Skinningsrud B, Saganiak K, Development of the human pancreas and its vasculature – An integrated review covering anatomical, embryological, histological, and molecular aspects: Ann Anat, 2019; 221; 115-24
8. Ahrén B, Autonomic regulation of islet hormone secretion – implications for health and disease: Diabetologia, 2000; 43; 393-410
9. Maglione M, Ploeg R, Friend P, Donor risk factors, retrieval technique, preservation and ischemia/reperfusion injury in pancreas transplantation: Curr Opin Organ Transplant, 2013; 18(1); 83-88
10. Redfield RR, Kaufman DB, Odorico JS, Diagnosis and treatment of pancreas rejection: Curr Transplant Rep, 2015; 2; 169-75
11. Hagspiel KD, Nandalur K, Pruett TL, Evaluation of vascular complications of pancreas transplantation with high-spatial-resolution contrast-enhanced MR angiography: Radiology, 2007; 242(2); 590-99
12. Vandermeer FQ, Manning MA, Frazier AA, Wong-You-Cheong JJ, Imaging of whole-organ pancreas transplants: Radiographics, 2012; 32(2); 411-35
13. Hagmann P, Jonasson L, Maeder P, Understanding diffusion MR imaging techniques: From scalar diffusion-weighted imaging to diffusion tensor imaging and beyond: Radiographics, 2006; 26(Suppl 1); S205-23
14. Caroli A, Schneider M, Friedli I, Diffusion-weighted magnetic resonance imaging to assess diffuse renal pathology: A systematic review and statement paper: Nephrol Dial Transplant, 2018; 33; ii29-40
Figures
Figure 1. Diffusion tensor imaging (DTI) reconstruction of transplanted pancreas superimposed on DTI b0; sagittal, axial, and coronal images.Figure 2. T1W (A), diffusion tensor imaging (DTI) b0 (B), and DTI fractional anisotropy map (C). DTI measures in the head of the transplanted pancreas ranged from 0.07 to 0.32, with a mean value of 0.19.Figure 3. (A) Dixon T1-weighted image, coronal section. (B) Apparent diffusion coefficient map from isotropic diffusion-weighted images, axial section. (C) Fractional anisotropy map from diffusion tensor imaging (DTI), coronal section. (D) Isotropic diffusion image from DTI, b value 800, coronal section. (E) Apparent diffusion coefficient map from DTI, coronal section. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387