13 November 2021: Clinical Research
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina: A Cross-Sectional Study
Inga Marijanović ABDEF 1, Marija Kraljević ABDEF 1*, Teo Buhovac ABDEF 1, Emir Sokolović CD 2
DOI: 10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788






Abstract
BACKGROUND: The pandemic of Coronavirus infectious disease 2019 (COVID-19) poses a major public health challenge, and an effective vaccine is the potential mechanism to resolve this specific situation. The present study aimed to evaluate acceptance of COVID-19 vaccination among patients attending the Oncology Clinic of University Clinical Hospital Mostar.
MATERIAL AND METHODS: This cross-sectional observational study enrolled 364 patients with cancer from the Oncology Clinic of University Clinical Hospital Mostar during February 2021. Data were collected using a questionnaire that captured general information about the participants and their attitudes toward COVID-19 vaccination.
RESULTS: Of the participants, 41.8% answered “Yes” when asked if they would take the vaccine once it becomes available, 37.6% answered “Not sure”, and 20.6% answered “No”. For patients in favor of vaccination, the main reasons reported were fear of getting sick (77.6%), the desire to contribute to herd immunity (57.8%), and trusting the recommendations of health professionals (57.2%). The main reasons for the patients’ vaccination refusal/indecision were doubts about the results from clinical trials of COVID-19 vaccines (49.1%), concerns about adverse effects (24.5%), and confusion about the various vaccine options (19.8%). The majority of participants (82.4%) stated that recommendation by their oncologist could influence their decision about vaccination. Of the participants who indicated unwillingness (refusal or indecision) to be vaccinated against COVID-19, 65.3% stated that recommendation by their oncologist could influence their decision about vaccination.
CONCLUSIONS: The findings from the present study showed most patients had refused or were indecisive regarding immunization with COVID-19 vaccine. Increasing physician awareness of this situation may result in higher rates of vaccination.
Keywords: COVID-19, Neoplasms, Patients, Vaccination, Bosnia and Herzegovina, COVID-19, COVID-19 Vaccines, Cross-Sectional Studies, Humans, Patient Acceptance of Health Care, SARS-CoV-2, Universities
Background
The pandemic caused by Coronavirus infectious disease 2019 (COVID-19) continues to affect all aspects of our lives [1].
From the beginning of the pandemic in Bosnia and Herzegovina (BiH) in March 2020 to April 19, 2021, according to the Institute for Public Health Federation of BiH, there were 17 125 confirmed cases of COVID-19 in Mostar [2]. The City of Mostar is the administrative center of Herzegovina-Neretva Canton of the Federation of BiH, with a total population of 105 797 according to the results of the most recent 2013 population census in BiH [3]. There is no cancer registry in BiH and we do not have epidemiological data about the number of cancer patients infected by severe acute respiratory syndrome-related Coronavirus-2 (SARS-CoV-2). According to estimates from the International Agency for Research on Cancer (IARC), 14 673 new cancer cases and 9 209 related deaths occurred in 2020 in BiH [4].
The Oncology Clinic of University Clinical Hospital Mostar is the only specialized oncology institution in the southwestern part of BiH that covers the needs for all forms of oncology treatment and care for more than half a million people.
Vaccination is getting more attention as a strategy to combat the COVID-19 pandemic [5] and it seems to be the best solution for a long-term response to this pandemic. However, a vaccine must be accepted and used by the vast majority of the population to be successful [6].
Patients with cancer have been shown to have higher infection rates of SARS-CoV-2 than the general population, and cancer patients with COVID-19 had worse conditions and clinical outcomes [7,8]. The results from another study showed that patients with COVID-19 and cancer had similar outcomes compared to matched patients without diagnosis of cancer [9].
The American Society of Clinical Oncology (ASCO) and the Infectious Diseases Society of America (IDSA) hosted a webinar titled “COVID-19 Vaccine & Patients with Cancer” on December 17, 2020 to address the effectiveness of COVID-19 vaccination and provide expert opinion on its use in cancer patients. Although it should be mentioned that patients receiving treatments have been excluded from enrollment in vaccine trials to date, there is little to no information on the vaccines’ safety and effectiveness in cancer patients, and the panel of experts concluded that the vaccines have been shown to be safe and effective for the general population, and there was no indication that they would not be safe for most cancer patients [10].
Despite the lack of evidence for vaccination in cancer patients, there is sufficient evidence to support anti-infective vaccination in general (excluding live-attenuated vaccines and replication-competent vector vaccines) even in cancer patients receiving immunosuppressive therapy [11–13]. The World Health Organization (WHO) considers the elderly and healthcare professionals as main priorities for vaccination against COVID-19 (phases 1b and 1a, respectively), followed by cancer patients (phase 2) [14,15], and in the United States of America (USA), professionals are considered priorities (1a), followed by cancer patients and the elderly (≥age 65 years) (1b) [16].
Vaccination against COVID-19 has now started in several countries around the world [17], and vaccination in BiH is planned to start soon, but at this moment there is no available data on exactly when [18]. It is known that vaccines in general help to reduce morbidity and mortality, and patients receiving cancer treatment, as a vulnerable population, should be considered for age- and indication-appropriate vaccinations as a certain vaccine-preventable diseases are more common in cancer patients and are linked to worse health outcomes. Many risk factors, including immunological suppression, old age, comorbidities, and malnutrition, contribute to this. Despite these facts, anti-vaccination beliefs and activities have always persisted in response to vaccines and vaccination as a technique of infectious disease prevention. Negative views regarding vaccination, as well as fears of adverse effects, are among the reasons for vaccination refusal [19–21]. Given the large proportion of cancer patients, vaccination is important to gain collective immunity and also to provide protection to patients because cancer treatment delays for any reason, including COVID-19, may lead to worse outcomes of oncology treatment.
According to our literature review, few studies have been conducted to assess the cancer population’s attitudes toward COVID-19 vaccination [22,23] and there is lack of evidence in this area. To the best of our knowledge, no previous published research has evaluated the intent of patients with cancer from BiH to be vaccinated against COVID-19 when a vaccine becomes available.
The aim of this study was to understand the attitudes among cancer patients toward vaccination with a potential COVID-19 vaccine. This was a survey of willingness of oncology patients to receive the COVID-19 vaccine.
Material and Methods
STUDY DESIGN:
We conducted a cross-sectional, observational survey. Ethics approval was obtained from the Hospital Ethics Committee at University Clinical Hospital Mostar (number 857/21). This study was performed following institutional guidelines and all procedures followed were in accordance with the Helsinki Declaration of 1975 in its most recent version. Participation in the study was voluntary. All participants gave their written informed consent.
SETTING:
The present study included oncology patients at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina. Data were collected during February 2021. All cancer patients visiting the Oncology Clinic in that period were invited to participate in this study. After completing a scheduled appointment, patients were asked to respond to a questionnaire by a physician. Patients were clearly informed about the background and objectives of the study. Questions related to medical history (cancer type, therapeutic status, therapeutic strategy, presence of comorbidities and allergies) and how to use the questionnaire were explained to patients who agreed to participate in the study. After obtaining their written informed consent, physicians asked patients to complete the self-administered questionnaire in a separate and quiet room. Participants returned their filled-out questionnaires to locked drop-boxes.
PARTICIPANTS:
Cancer patients 18 years of age and older at any stage of cancer treatment, including before, during, and after treatment and patients on surveillance, were eligible to participate. Patients were volunteers who agreed to fill out the survey. Refusals were not documented.
All patients visiting the Oncology Clinic in the period of recruitment were invited to participate in this study and asked to complete a questionnaire. The Oncology Clinic of University Clinical Hospital Mostar is consulted by approximately 10 000 patients annually. During the study recruitment period, in February 2021, during which preventive measures were in force that limited the number of patient visits, a total of 600 patients were available for testing, 364 of whom agreed to participate in the study.
VARIABLES:
Variables analyzed for all patients included sociodemographic data (age, gender, residence area, educational level, employment status, marital status), medical history variables (presence of allergies, cancer type, therapy status, therapeutic strategy, presence of comorbidities), and variables related to questions about the participants’ experience with COVID-19, including attitudes toward potential COVID-19 vaccination (including questions about participants’ willingness to be vaccinated against COVID-19 and their reasons), and information about previous vaccination against seasonal flu.
DATA SOURCES/MEASUREMENTS:
To create the survey, we performed a literature review to identify current COVID-19 vaccination data and guidelines and recent studies of vaccination against other diseases among cancer patients [22–27]. Surveys were peer-reviewed by the authors of the article and pretested with a sample group of 20 patients to assess the clearness of the questionnaire (to improve choice of words and readability of expression of the study variables). On the basis of their suggestions, the questionnaire was revised to the final form.
The final version of the questionnaire took between 5 and 10 minutes to complete. The questionnaire was distributed in Croatian, one of 3 official languages in BiH. A copy of the administered questionnaire in Croatian and translated into English can be found in Supplementary Material.
The questionnaire comprised baseline participants’ information (age, gender, area of living, educational level, employment status, marital status, presence of allergies, cancer type, therapeutic status, therapeutic strategy, comorbidities); information about the participants’ experience with COVID-19; attitudes toward potential COVID-19 vaccination, including questions about participants’ willingness to be vaccinated against COVID-19 and their reasons (multiple-choice questions); and information about previous vaccination against seasonal flu.
Participants were asked to indicate if they had COVID-19 by answering “yes” or “no”.
Participants were asked whether they would accept receiving COVID-19 vaccines once the vaccine becomes approved and available in BiH, with 3 response options: “yes”, “no”, or “not sure”. Patients who answered “yes” or “no”/”not sure” were asked to indicate their reasons (multiple-choice questions). For analysis, responses to the attitudes section were combined. For example, the responses “no” and “not sure” were combined into a single category.
Participants were also asked to respond to whether they had enough information about the vaccine and its safety with responses “yes” or “no”. On the question “How much would recommendation of your oncologist influence your decision to get vaccinated against COVID-19?”, respondents were asked to respond “There is no influence on my decision” or “It is the key factor for my decision” or “It would be one of the factors for my decision.” Additionally, participants were asked to report whether they had previously received a seasonal flu vaccine and whether their general practitioner (GP) recommend it to them.
BIAS:
Participants were assured of the anonymity and confidentiality of their responses, which helped to minimize the possible bias caused by self-reported data. To minimize potential desirability bias, patients completed questionnaire in a separate and quiet room, without the presence of medical staff.
STUDY SIZE:
The study was designed as a cross-sectional survey, so we sought to include all available patients at our institution. Since we did not evaluate the effects of any particular intervention, we did not conduct a sample size calculation. All patients visiting the Oncology Clinic during recruitment in February 2021 were invited to participate in this study, and total of 364 patients agreed to take part in the study. At that time, epidemiological measures were still in place and the number of patient visits was limited (many normally face-to-face follow-up appointments were changed to appointments by email, phone, or fax). It was not yet known when the official vaccination in our region would begin.
QUANTITATIVE VARIABLES:
The variable age was divided into 4 categories: <40 years old, 40–54 years old, 55–64 years old, and >64 years old.
STATISTICAL METHODS:
IBM SPSS Statistics v. 23.0 was used for statistical analysis. We defined descriptive measures, including absolute value and percentages. Multivariate analysis (logistic regression) was used to study the association between study population characteristics and survey outcomes. The chi-square test of independence was used to evaluate relationship between being infected with COVID-19 and willingness to vaccinate against COVID-19.
Direct logistic regression was performed to evaluate the effect of multiple factors on the probability that participants would answer positively to the question about their willingness to get a COVID-19 vaccine. The model consists of 8 independent variables (comorbidities – no vs yes; sex – female vs male; information about COVID-19 vaccines – insufficient vs sufficient; influenza vaccination – no vs yes; recommendation of GP to vaccinate – no vs yes; allergies – no vs yes; age; residence area – rural area vs urban area).
Results
BASELINE CHARACTERISTICS OF THE PARTICIPANTS:
The study sample included 364 patients from the Oncology Clinic of University Clinical Hospital Mostar, the majority of whom were women (61.5%). Of the participants, 3.0%, 23.4%, 34.6%, and 39.0% were aged <40, 40 to 54, 55 to 64, and >64 years, respectively. The mean age was 61.6±11.2 years. Most of the participants were married (81.9%) and had a secondary level of education (56.6%). Most of the participants (76.4%) were not employed. The majority of patients (56%) lived in urban areas. Most of the participants were patients with a diagnosis of breast cancer (35.2%) or gastrointestinal cancer (28.8%). A total of 309 (84.9%) oncology patients did not have allergies. Of the participants, 80.2% were actively receiving anticancer therapy; 31.3% were treated with adjuvant or neoadjuvant therapy, 44.0% with therapy in metastatic setting, 4.9% with primary cancer treatment, and 19.8% of participants were in follow-up or had not been treated in the last 3 months. More than half (58.8%) had other chronic diseases. Baseline characteristics of the participants are shown in Table 1.
INFORMATION ABOUT THE PARTICIPANTS’ EXPERIENCE WITH COVID-19 AND ATTITUDES TOWARD POTENTIAL COVID-19 VACCINATION:
Of the participants, 18.9% were already infected with SARS-CoV-2. The chi-square test of independence did not reveal a significant relationship between being infected with SARS-CoV-2 and willingness to be vaccinated against COVID-19 (
Of the participants, 41.8% answered “Yes” when asked if they would take the vaccine once it becomes available, 37.6% answered “Not sure”, and 20.6% answered “No”.
For patients in favor of vaccination, the main reason they reported was fear of getting sick (77.6%). Other reasons reported by patients in favor of vaccination are shown in Figure 1A. The main reason for the patients’ vaccination refusal/indecision was doubt about the results of clinical trials of COVID-19 vaccines (49.1%). Other reasons for the patients’ vaccination refusal/indecision are shown in Figure 1B. None of the patients who refused or were in doubt about vaccination stated it was it because of religious belief. Most participants (82.4%) stated that recommendation by their oncologist could influence their decision about vaccination.
KNOWLEDGE AND PERCEPTIONS ABOUT COVID-19 VACCINE BASED ON WILLINGNESS TO VACCINATE:
Figure 2 shows that the most patients who indicated willingness to be vaccinated against COVID-19 (65.10%) stated they had sufficient information about vaccines, 23.00% thought that vaccines were safe for oncological patients, 85.60% stated that recommendation of their oncologist could influence their decision about vaccination, 21.70% of them had been vaccinated against seasonal flu, and 27% stated that their GP recommended vaccination. Of the patients who indicated unwillingness (refusal or indecision) to be vaccinated against COVID-19, 34.70% stated they had sufficient information about vaccines, 25.30% thought vaccines were safe for oncological patients, 65.30% stated that recommendation of their oncologist could influence their decision about vaccination, only 4% of them had been vaccinated against seasonal flu, and 12% stated that their GP recommended vaccination.
LOGISTIC REGRESSION:
Logistic regression modeling showed statistically significant results for all predictors (χ2 8, N=364, P<0.001), which shows that our model distinguished participants who wanted to be vaccinated from those who did not. The model in total explains between 22.4% (Cox & Snell R Square) and 30.1% (Nagelkerke R Square) of variance of willingness to get a COVID-19 vaccine status and accurately classifies 72.3% of cases. As shown in Table 2, 3 of the independent variables gave a unique statistically significant contribution to the model (gender, information about COVID-19 vaccines, and recommendation of GP to vaccinate). The strongest predictor of willingness to be vaccinated is sufficient information about COVID-19 vaccines, with odds ratio (OR) of 3.97 (95% CI 2.43–6.49). Participants who answered that they had sufficient information about COVID-19 vaccines were almost 4 times more likely to answer that they want to be vaccinated. Since being a female was marked as a reference category, the OR of 3.1 (95% CI 1.88–5.14) for gender covariate means that men are almost 3 times more likely to answer that they want to be vaccinated.
HISTORY OF INFLUENZA VACCINATION:
The majority had not received an influenza vaccine in previous years (86.3%). A total of 300 participants (82.4%) stated that their GP did not recommend vaccination against influenza.
Discussion
This study presents results addressing the attitudes and beliefs of cancer patients toward COVID-19 vaccination. It is unclear how active treatment affects a patient’s ability to mount protective immunity against COVID-19 after vaccination, and studies stratifying patients by type of treatment and the type of vaccine are a top priority for the international oncology community [22,23].
Given the importance of this topic, and for physicians and other health professionals to promote vaccination, it is necessary to better understand patients’ attitudes regarding vaccines.
Our study shows that the majority of cancer patients expressed unwillingness (refusal/indecision) to be vaccinated against COVID-19, which does not agree with other surveys, in which the majority of participants showed willingness to be vaccinated against COVID-19 [22,23,28].
Given the obtained results, which differ from those of other studies, it was also important to investigate patients’ opinions about their willingness to be vaccinated against COVID-19 and earlier vaccination behaviors, in order to identify and understand the reasons for vaccination hesitance, which could help us address this problem.
One reason that could explain above results is the smaller number of patients previously vaccinated against influenza virus in our study (13.7%), in contrast to the cancer patients in the French study (52.2%) because previous influenza vaccination is considered a predictor for vaccination acceptance [22].
The lower percentage of patients vaccinated against influenza, as shown by the results of our study and in accordance with results from previous studies [25–27], can be explained by the lack of recommendations from attending physicians (the majority of participants in our study stated that their GP did not recommend vaccination against influenza). Results from previous studies, including those among cancer patients and also in the general population, have confirmed the role of primary physicians in increasing influenza vaccination awareness and acceptance [25–27,29].
The results from the present study showed that the most patients stated that recommendation of their oncologist could influence their decision about vaccination. It is important to emphasize that among the participants who indicated unwillingness (refusal or indecision) to be vaccinated against COVID-19, most stated that recommendation of their oncologist could influence their decision about vaccination. Similar findings have also been confirmed in other surveys, including those related to influenza vaccination [22,25–27], emphasizing the importance of primary physicians and mostly clinical oncologists in promoting vaccine acceptance among cancer patients.
Accordingly, increasing oncologists’ awareness of this problem, as well as counseling and educating patients about it, could result in a higher rate of vaccine acceptance, especially in countries where there is a lack of public vaccination campaigns. This is important because results from the present study also showed that the strongest predictor of willingness to vaccinate was sufficient information about COVID-19 vaccines, which can be provided during medical consultations.
However, it should be emphasized that the provision of oncology services during the pandemic has contributed to mental health challenges among health care workers, and preventive measures should be taken to address these problems, which negatively impact the delivery of appropriate care for patients with cancer [30,31].
Another reason that may influence patients’ decision about vaccination against COVID-19 is their therapeutic status. Accordingly, a study of Romanian adults with cancer only included patients under treatment, as they might be afraid of possible cancer treatment delays because of possible COVID-19 infection. The present study also included patients who were in follow-up [28].
Our study also revealed the main reasons for the refusal/indecision of the patients to vaccination, which included doubts about the results of clinical trials of COVID-19 vaccines, concerns about adverse effects, and confusion about different vaccine options.
Previous studies of COVID-19 vaccine acceptance, including those among cancer patients and also the general population, revealed similar attitudes [6,22,32,33].
The present study has several limitations. Because of the cross-sectional design, longitudinal follow-up is lacking. The vaccine was not available at the time this study was conducted, and participants’ vaccination intentions may differ when the vaccines become available. Also, our study did not include patients who responded to the survey by email, phone, or fax. This could also affect the results of our study, as these patients are probably more likely to be in greater fear of COVID-19 and more of these patients may be in favor of vaccination. The public COVID-19 vaccination campaigns have been launched around the world. Lack of such public campaigns in BiH may be one of the reasons why a slightly smaller percentage of patients would accept vaccination against COVID-19.
This was a single-institution study and the results we obtained do not give a complete picture of vaccination acceptance among oncology patients with cancer in BiH.
Conclusions
In summary, our study showed the COVID-19 vaccination refusal/indecision of a majority of patients in active cancer therapy or on surveillance, mainly because of doubts in clinical trials of COVID-19 vaccines, concerns about adverse effects, and confusion about different vaccine options.
It is also important to emphasize that most patients stated that recommendation of their oncologist could influence their decision about vaccination.
Healthcare professionals must raise awareness about the importance of vaccination in preventing infection and gaining herd immunity.
Figures
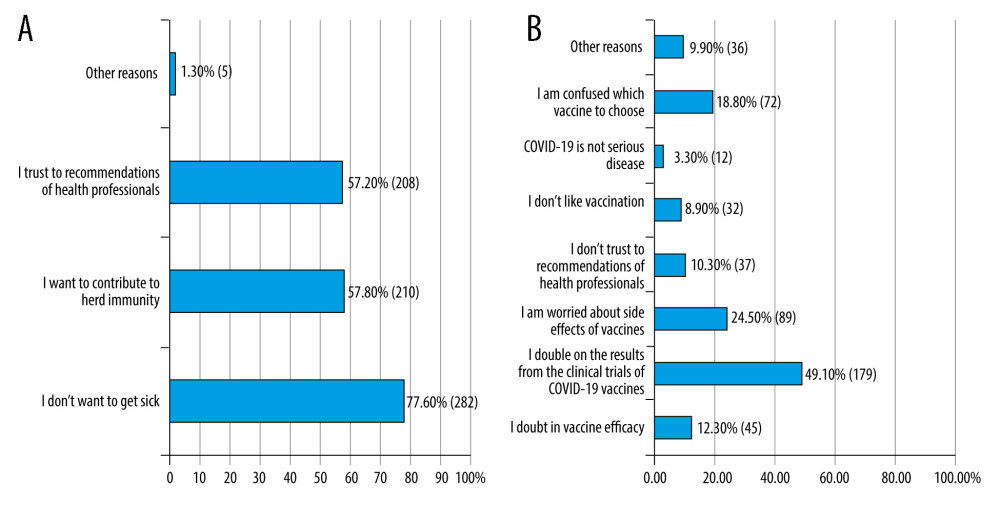 Figure 1. (A) Reasons for willingness to get vaccinated against COVID-19 among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021. (B) Reasons for unwillingness to get vaccinated against COVID-19 among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021 (Microsoft Excel 2013).
Figure 1. (A) Reasons for willingness to get vaccinated against COVID-19 among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021. (B) Reasons for unwillingness to get vaccinated against COVID-19 among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021 (Microsoft Excel 2013). 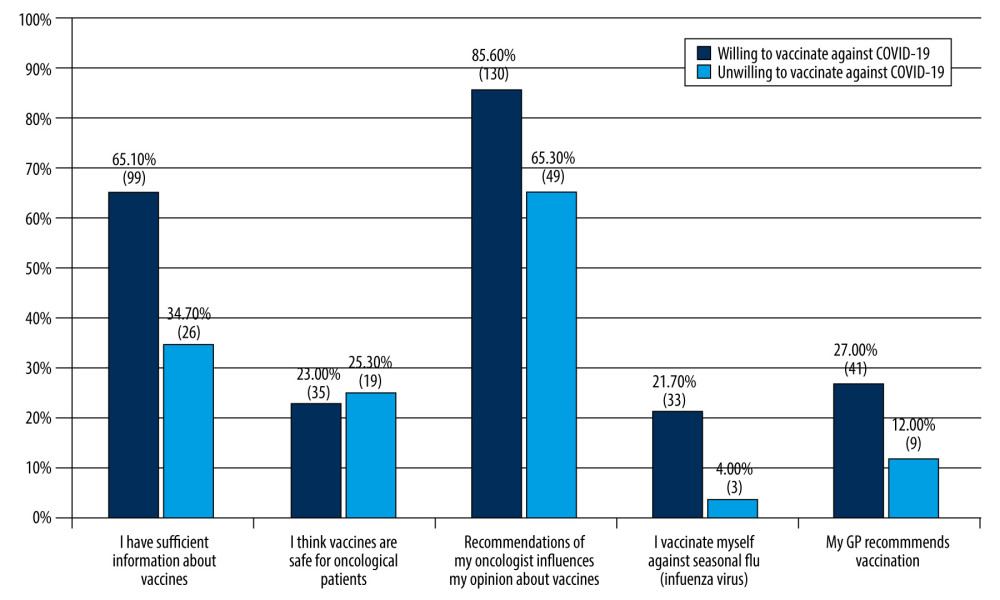 Figure 2. Knowledge and perceptions about COVID-19 vaccine based on willingness to be vaccinated among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021 (Microsoft Excel 2013).
Figure 2. Knowledge and perceptions about COVID-19 vaccine based on willingness to be vaccinated among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021 (Microsoft Excel 2013). Tables
Table 1. Baseline characteristics of participants. Survey of patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021.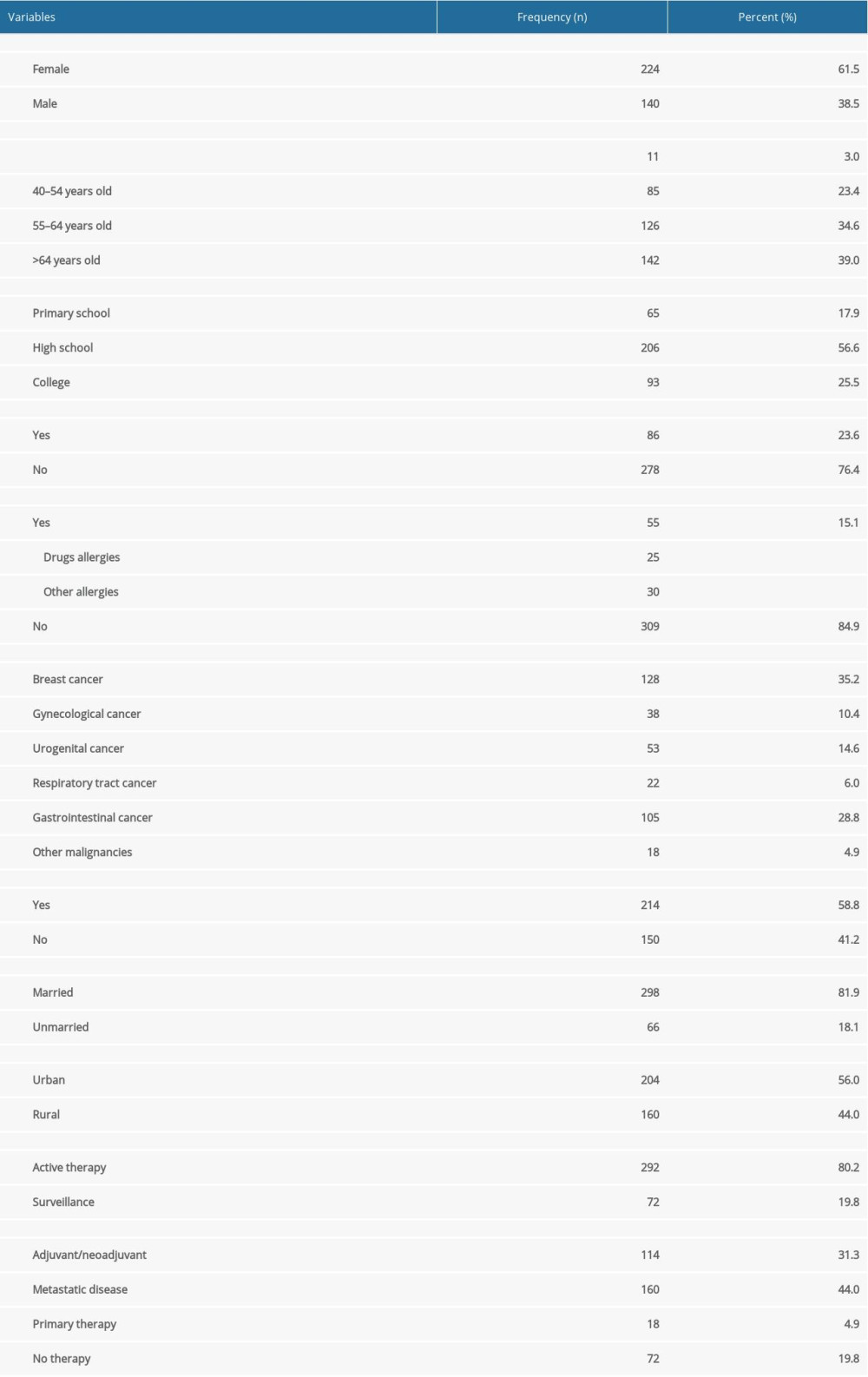 Table 2. Probability prediction of answer that participant is willing to get the COVID-19 vaccine. Survey among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021.
Table 2. Probability prediction of answer that participant is willing to get the COVID-19 vaccine. Survey among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021.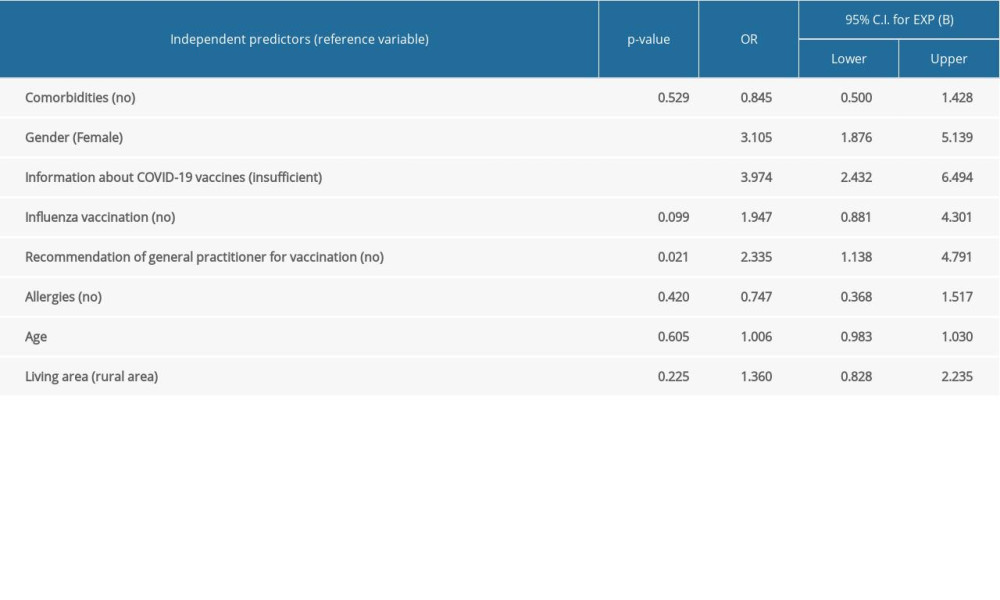
References
1. Dubey S, Biswas P, Ghosh R, Psychosocial impact of COVID-19: Diabetes Metab Syndr, 2020; 14(5); 779-88
2. Institute for public health of the Federation of Bosnia and Herzegovina (FBiH): COVID-19: Analytical and graphical presentation of FBiH data, 2021 https://covid-19.ba/
3. Agency for Statistics of Bosnia and Herzegovina (BiH): Census 2013 in Bosnia and Herzegovina, 2013 www.popis.gov.ba/popis2013/mapa/?lang=bos
4. International Agency for Research on Cancer, Global Cancer Observatory: Bosnia and Herzegovina – Globocan 2020, 2021 https://gco.iarc.fr/today/data/factsheets/populations/70-bosnia-and-herzegovina-fact-sheets.pdf
5. Qiao S, Tam CC, Li X, Risk exposures, risk perceptions, negative attitudes toward general vaccination, and COVID-19 vaccine acceptance among college students in South Carolina: medRxiv, 2020; 2020; 20239483
6. Pogue K, Jensen JL, Stancil CK, Influences on attitudes regarding potential COVID-19 vaccination in the United States: Vaccines (Basel), 2020; 8(4); 582
7. Yang F, Shi S, Zhu J, Clinical characteristics and outcomes of cancer patients with COVID-19: J Med Virol, 2020; 92(10); 2067-73
8. Salunke AA, Nandy K, Pathak SK, Impact of COVID -19 in cancer patients on severity of disease and fatal outcomes: A systematic review and meta-analysis: Diabetes Metab Syndr, 2020; 14(5); 1431-37
9. Brar G, Pinheiro LC, Shusterman M, COVID-19 severity and outcomes in patients with cancer: A matched cohort study: J Clin Oncol, 2020; 38(33); 3914-24
10. ASCO: American Society of Clinical Oncology: COVID-19 Vaccine & Patients with Cancer, 2020 www.asco.org/asco-coronavirus-resources/covid-19-patient-care-information/covid-19-vaccine-patients-cancer
11. Cordonnier C, Einarsdottir S, Cesaro S, Vaccination of haemopoietic stem cell transplant recipients: Guidelines of the 2017 European Conference on Infections in Leukaemia (ECIL 7): Lancet Infect Dis, 2019; 19; e200-12
12. Mikulska M, Cesaro S, de Lavallade H, Vaccination of patients with haematological malignancies who did not have transplantations: Guidelines from the 2017 European Conference on Infections in Leukaemia (ECIL 7): Lancet Infect Dis, 2019; 19; e188-99
13. Rieger CT, Liss B, Mellinghoff S, Anti-infective vaccination strategies in patients with hematologic malignancies or solid tumors-Guideline of the Infectious Diseases Working Party (AGIHO) of the German Society for Hematology and Medical Oncology (DGHO): Ann Oncol, 2018; 29; 1354-65
14. World Health Organization: WHO SAGE values framework for the allocation and prioritization of COVID-19 vaccination, 2020 https://apps.who.int/iris/handle/10665/334299
15. World Health Organization: Evidence to recommendations for COVID-19 vaccines: Evidence framework, 2020 www.who.int/publications/i/item/WHO-2019-nCoV-SAGE-Framework-Evidence-2020-1
16. Dooling KACIP COVID-19 Vaccines Work Group: Phase 1 allocation COVID-19 vaccine: Work Group considerations, 2020 www.cdc.gov/vaccines/acip/meetings/downloads/slides-2020-09/COVID-07-Dooling-508.pdf
17. Bloomberg: More than 334 million shots given: Covid-19 vaccine tracker, 2021 www.bloomberg.com/graphics/covid-vaccine-tracker-global-distribution/
18. World Health Organization: COVID-19 vaccine programme monitor, 2021 https://worldhealthorg.shinyapps.io/EURO_COVID-19_vaccine_monitor/
19. Shah MK, Kamboj M, Immunizing cancer patients: Which patients? Which vaccines? When to give?: Oncology (Williston Park), 2018; 32(5); 254-8
20. Zaorsky NG, Churilla TM, Egleston BL, Causes of death among cancer patients: Ann Oncol, 2017; 28(2); 400-7
21. Jacobson RM, St Sauver JL, Finney Rutten LJ, Vaccine hesitancy: Mayo Clin Proc, 2015; 90(11); 1562-8
22. Barrière J, Gal J, Hoch B, Cassuto O, Acceptance of SARS-CoV-2 vaccination among French patients with cancer: A cross-sectional survey: Ann Oncol, 2021; 32(5); 673-74
23. van der Veldt AAM, Oosting SF, Dingemans AC, COVID-19 vaccination: The VOICE for patients with cancer: Nat Med, 2021; 27(4); 568-69
24. European Society for Medical Oncology: ESMO statements for vaccination against COVID-19 in patients with cancer, 2020 https://www.esmo.org/covid-19-and-cancer/covid-19-vaccination
25. Ariza-Heredia EJ, Azzi J, Shah DP, Influenza vaccination in patients with cancer: Factors associated with vaccination practices for patients and their household members: Infect Control Hosp Epidemiol, 2015; 36(10); 1239-41
26. Akin S, Dizdar O, Ozisik L, Vaccination attitudes among patients with cancer receiving chemotherapy: International Journal of Hematology and Oncology, 2016; 26(3); 167-72
27. Poeppl W, Lagler H, Raderer M, Influenza vaccination perception and coverage among patients with malignant disease: Vaccine, 2015; 33(14); 1682-87
28. Gheorghe AS, Negru ŞM, Niţipir C, Knowledge, attitudes and practices related to the COVID-19 outbreak among Romanian adults with cancer: A cross-sectional national survey: ESMO Open, 2021; 6(1); 100027
29. Domnich A, Cambiaggi M, Vasco A, Attitudes and beliefs on influenza vaccination during the COVID-19 pandemic: Results from a representative Italian survey: Vaccines (Basel), 2020; 8(4); 711
30. Marijanović I, Kraljević M, Buhovac T, Use of the Depression, Anxiety and Stress Scale (DASS-21) questionnaire to assess levels of depression, anxiety, and stress in healthcare and administrative staff in 5 oncology institutions in Bosnia and Herzegovina during the 2020 COVID-19 pandemic: Med Sci Monit, 2021; 27; e930812
31. Banerjee S, Lim KHJ, Murali K, The impact of COVID-19 on oncology professionals: Results of the ESMO Resilience Task Force survey collaboration: ESMO Open, 2021; 6(2); 100058
32. Ghosh R, Dubey S, Roy D, Focal onset non-motor seizure following COVID-19 vaccination: A mere coincidence?: Diabetes Metab Syndr, 2021; 15(3); 1023-24
33. Al-Qerem WA, Jarab AS, COVID-19 vaccination acceptance and its associated factors among a Middle Eastern population: Front Public Health, 2021; 9; 632914
Figures
Figure 1. (A) Reasons for willingness to get vaccinated against COVID-19 among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021. (B) Reasons for unwillingness to get vaccinated against COVID-19 among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021 (Microsoft Excel 2013).Figure 2. Knowledge and perceptions about COVID-19 vaccine based on willingness to be vaccinated among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021 (Microsoft Excel 2013). Tables
Table 1. Baseline characteristics of participants. Survey of patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021.Table 2. Probability prediction of answer that participant is willing to get the COVID-19 vaccine. Survey among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021.Table 1. Baseline characteristics of participants. Survey of patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021.Table 2. Probability prediction of answer that participant is willing to get the COVID-19 vaccine. Survey among patients with cancer at the Oncology Clinic of University Clinical Hospital Mostar, Bosnia and Herzegovina, 2021. In Press
Clinical Research
Comparative Effectiveness of a Nurse-Led Care Model vs Usual Care in Rheumatoid Arthritis: A Longitudinal C...Med Sci Monit In Press; DOI: 10.12659/MSM.953211
Clinical Research
Impact of Treatment Modality on Pain, Sexual Function, and Psychological Well-Being in Patients With Bartho...Med Sci Monit In Press; DOI: 10.12659/MSM.952422
Clinical Research
Association Between Radiographic Knee Osteoarthritis, Pre-Fracture Mobility, and Hip Fracture Patterns in O...Med Sci Monit In Press; DOI: 10.12659/MSM.952678
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,084
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,530
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,116
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,768
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387