01 July 2020: Clinical Research
A Retrospective Case-Control Study of the Determinants of Iron Deficiency Anemia in Infants in an Urban Community in Shanghai, China Between 2010–2015
Jian Wang1ADEF*, Yuan Liu2DEF, Qi Zhao3CD, Tianwei Liu4B, Zhigang Zhou4BDOI: 10.12659/MSM.921463
Med Sci Monit 2020; 26:e921463






Abstract
BACKGROUND: Iron deficiency anemia (IDA) is a global public health problem. This study aimed to analyze the social determinants of IDA in infants living in Shanghai, China, between 2010–2015.
MATERIAL AND METHODS: Data were analyzed retrospectively from the Shanghai Children’s Health Check Record system in the Tangqiao Community Health Service Center for infants aged <24 months between January 1, 2010, and December 31, 2015. A study group was identified with IDA, and an age-matched and gender-matched healthy control group was identified.
RESULTS: The five-year prevalence rate of IDA was 11.49% (150/1305). Infants with IDA had significantly lower birth weights (3228.720±456.200 gm vs. 3376.870±393.719 gm; P<0.01), a higher percentage of premature births (10.67% vs. 1.33%; P<0.001), a longer exclusive breastfeeding period (10.63±4.844 months vs. 7.08±5.039 months; P<0.001), a higher rate of exclusive breastfeeding within four months after birth (P<0.001), a later start for complementary feeding (7.32±1.633 months vs. 6.93±1.794 months; P<0.05), and a higher rate of starting complementary feeding after 6 months of age (P<0.05). There were no significant differences between the two groups for maternal child-bearing age, mode of delivery, infant birth height, and birth rank.
CONCLUSIONS: The introduction of an iron-fortified formula for exclusively breastfed infants at 4 months of age, starting complementary feeding promptly before 6 months of age, and improving perinatal care for pregnant women to avoid premature birth and reduce low birth weight may be effective measures to prevent IDA.
Keywords: Anemia, Iron-Deficiency, Infant Nutrition Disorders, social determinants of health, Asians, Breast Feeding, Case-Control Studies, Infant, Infant Nutritional Physiological Phenomena, Infant, Low Birth Weight, Infant, Newborn, Iron, Prevalence, Risk Factors, Urban Population
Background
Worldwide, iron deficiency anemia (IDA) is a significant public health problem and causes greater harm to infants than children and adults [1]. In 2013, the Report on Nutrition Development of Chinese Children Aged 0 to 6 years stated that the overall prevalence rate of anemia in China among children under 5 years of age was 12.6% and that infants aged 6–24 months had the highest prevalence of anemia [1]. In 2015, a cross-sectional study of infants aged 6–36 months in Beijing, Shanghai, Nanjing, Shenzhen, and Chengdu showed that the prevalence of anemia in infants was17.2% [2]. One of the main objectives regarding children’s health in the National Program of Action for Child Development in China, 2011–2020, is to reduce the prevalence of anemia to 12% or less in children less than 5 years of age [3].
Recent studies have shown that iron deficiency may harm children’s growth and development, as well as motor skills and immune function [4–6]. Severe iron deficiency in infants may adversely affect their cognitive and learning abilities and behavioral development, which may not be reversed by treatment with iron supplements [7–9]. Therefore, reducing the determinants of IDA is important to prevent health impairment in infants, and priority should be given to reduce the prevalence rate of anemia among infants aged 6–24 months to reach the target of reducing the prevalence rate of anemia in infants less than one year of age. The community health center is the main site for the implementation of systematic childcare management, which means that it is important to investigate the determinants of IDA in infants and to explore community-based preventive measures.
The Tangqiao Community Health Service Center, is located in Pudong New Area, Shanghai, one of the most economically developed cities in China. Therefore, this study aimed to analyze the social determinants of IDA in infants living in Shanghai, China, between 2010–2015. This study was conducted to identify factors to support community-based primary and secondary public health intervention measures to reduce IDA in infants.
Material and Methods
ETHICAL APPROVAL:
Data from this case-control study were analyzed retrospectively from the Shanghai Children’s Health Check Record system in the Tangqiao Community Health Service Centre for infants aged <24 months between January 1, 2010, and December 31, 2015. A study group was identified with iron deficiency anemia (IDA), and an age-matched and gender-matched healthy control group was identified. This study was approved by the Ethics Committee of Zhongshan Hospital affiliated to Fudan University. Patient data were anonymized, and each participant was given a unique code during data analysis. The government-financed physical check-up was offered free of charge, and participation was voluntary. Information technology professionals from the district information center secured and exported the data used for analysis, as specified in the study design.
DATA COLLECTION:
The factors that were analyzed were basic demographic information, including family members and their education, parental occupation, and infant information including date of birth, birth weight, whether the birth was premature, and the infant’s birth order. The records of the physical examinations for eight points in time were recorded at 1, 2, 4, 6, 9, 12, 18, and 24 months of age, including height, weight, head circumference, chest circumference, fontanel closure, dental growth, language and movement abilities, and other growth parameters. Data on feeding patterns and complementary feeding details were recorded. The results of laboratory tests were recorded, including routine blood testing of healthy infants at 6, 12, 18, and 24 months of age. Infants that were classified into high-risk or low weight categories received an additional routine blood examination at 4 months of age. For infants diagnosed with anemia, routine examinations were conducted every month until the hemoglobin levels were restored to within the normal range.
After the study design was approved, the anonymized data were exported from the Shanghai Children’s Health Check Record database without any identifying details. All infants that were newly diagnosed with IDA whose ages ranged from 0–24 months between January 1, 2010, and December 31, 2015, were classified as the case group. The same number of healthy infants was selected as the control group of the same gender and age. The infants included three groups: <6 months old; 6–12 months old; and 12–24 months old. The following variables were obtained from the database: date of birth; birth weight; birth height; premature birth or not; firstborn or not; maternal age at delivery; mode of delivery; feeding pattern; exclusive breastfeeding; complementary feeding period; and a complete blood count (CBC) of the infants.
THE DIAGNOSIS OF IDA AND RESPONSE TO IRON THERAPY:
The IDA diagnosis was made according to the recommendations of the Pediatrics Subbranch of the Chinese Medical Association [10]. The diagnostic criteria for infant IDA included a hemoglobin level <110 g/l, a mean corpuscular volume (MCV) <80 fl, a mean corpuscular volume (MCV) <27 pg, and a mean corpuscular hemoglobin concentration (MCHC) <310 g/l. The response to iron therapy was defined as an increase in hemoglobin to >20 g/l after undergoing iron therapy for four weeks. Infants with microcytic hypochromic anemia were identified as having IDA after reviewing the medical history and relevant laboratory results and excluding other types of anemia. The World Health Organisation (WHO) has recommended that the hemoglobin level is used as a screening indicator for IDA [10], and IDA may be clinically diagnosed if iron supplementation is effective.
CALCULATION OF THE STUDY SAMPLE SIZE:
Based on the case-control study design, assuming that the percentage of children with anemia starting complementary feeding earlier than 6 months of age was 40% (p1), while the percentage of children without anemia starting complementary feeding earlier than 6 months of age was 60% (p2), the case-control ratio was 1: 1, and the statistical efficiency was 0.9, the required study sample size was estimated as:
The number of cases in the study group was identified as 130 and the number of cases in the control group was also identified as 130. The total number of all infants with newly diagnosed IDA from the database between January 1, 2010 and December 31, 2015 was 150, which was identified as an adequate study sample size for statistical analysis.
STATISTICAL ANALYSIS:
Data were expressed as the mean, the frequency, and the percentage to describe the characteristics of the groups studied. A paired t-test and the chi-squared (χ2) test were used to determine the differences in the continuous and categorical variables between the IDA and non-IDA groups, respectively. Multivariate logistic regression analysis was used to determine the factors associated with IDA. Statistical analysis was performed using SPSS version 19.0 software (IBM, Chicago, IL, USA). A P-value <0.05 was considered to be statistically significant.
Results
GENERAL INFORMATION:
There were 1,305 infants who received regular follow-up at the Child Care Clinic of Tangqiao Community Health Service Center between January 1, 2010, and December 31, 2015. There were 150 infants diagnosed with iron deficiency anemia (IDA) (82 male infants and 68 female infants). The overall five-year prevalence rate of IDA between 2010–2015 was 11.49% (12.75% for male infants and 10.27% for female infants). There was no significant difference in the prevalence of IDA between male and female infants (P>0.05) (Figure 1). When classified by the age at the time of diagnosis of IDA, 11 infants (7.33%) were <6 months old, 111 infants were 6–12 months old (74%), and 28 infants (18.67%) were 12–24 months old. The 6–12 month age group had the highest prevalence of IDA (P<0.01) (Figure 2).
SOCIAL DETERMINANTS OF IDA:
As shown in Table 1, the IDA group had a lower birth weight (3228.720±456.200 gm vs. 3376.870±393.719 gm; P<0.001), a longer exclusive breastfeeding period (10.63±4.844 months vs. 7.08±5.039 months; P<0.001) and a later start for complementary feeding (7.32±1.633 months vs. 6.93±1.794 months; P<0.05) when compared with the control group. There were no significant differences in maternal age at delivery and infant birth height between the two groups (P>0.05) (Table 1).
The percentage of premature births was significantly higher in the IDA group than in the control group (10.67% vs. 1.33%; P<0.001). Also, the prevalence of exclusive breastfeeding within four months after birth was significantly higher in the IDA group than in the control group (P<0.001). The percentage of infants who received exclusive breastfeeding for more than four months after birth was significantly higher in the IDA group than in the control group (P<0.001). Infants in the IDA group were more likely to receive complementary feeding after 6 months of age, which was significantly later than the control group (P<0.05). Differences in maternal age at delivery, mode of delivery, and whether the child was the first birth in the family were not significantly different between the IDA group and the control group (P>0.05) (Table 1). Factors associated with IDA were identified using logistic regression analysis, which showed that normal birth weight (OR=0.999) and mixed feeding (OR=0.239) were protective factors against the development of IDA (Table 2).
Discussion
The findings from the present study showed that premature birth, low birth weight, long exclusive breastfeeding time (>4 months old), and late adoption of complementary food (>6 months old) were risk factors for iron deficiency anemia (IDA) in infants living in Shanghai, China, between 2010–2015. However, high birth weight and mixed feeding were factors that protected infants from IDA. In 2001, data from the World Health Organisation (WHO) showed that the prevalence of IDA in infants living in industrialized and non-industrialized countries were 21.1% and 39.0%, respectively [4]. This study showed that the prevalence of IDA in infants in the Tangqiao Community in the city of Shanghai, China was 11.49%, which was slightly lower than that previously from both local and international sources. One possible reason for this discrepancy is that Pudong New District in Shanghai is an economically developed area. Also, this study only included infants living in the Tangqiao Community and did not include the infants of the transient population, which belong to a lower socio-economic class, which may underestimate the prevalence rate of IDA in this community.
During late pregnancy, the mother’s body continues to transfer nutrients, including iron, to the fetus, representing a high proportion of nutrient transfer during pregnancy. Premature infants do not have enough time to receive and accumulate iron from the mother’s body, lack iron reserves from birth, and are more likely to develop IDA during infancy [11]. A prospective cohort study in the Netherlands showed that late premature infants born after 32 weeks of gestation had a higher risk of IDA than term infants [12]. Recently, in 2019, Li et al. showed that in Beijing, China, premature infants had a high incidence of IDA [13]. This finding was supported by Xu et al. in 2015, who showed that premature birth was a risk factor for medium to severe IDA in infants 6–12 months old [14]. The findings from the present study showed that the percentage of premature infants in the IDA group was significantly higher than in the control group (10.67%
A domestic survey of nutritional conditions in China in 2013 showed that infants aged 5 months to 1 year had the highest prevalence rate of IDA, with the IDA prevalence rate in male infants 38.3% and that in female infants being 34.7% [1]. In 2019, a study in Japan reported by Amano et al. showed that male infants were more likely to develop IDA than female infants [15]. However, in 2019, in Iran, Riahi et al. reported no statistically significant difference in the prevalence of IDA between male and female infants [16]. The findings from the present study showed that male infants were more likely to develop IDA than female infants (12.75%
The iron reserve in the infant’s body can support growth and development for approximately 3–4 months. The infant then requires a supply of iron from food after 4–6 months of age. Therefore, infants aged 6–24 months are at higher risk of developing IDA. A cross-sectional study in Bhaktapur, Nepal in 2016 showed that the prevalence of IDA in infants aged 2–6 months was 49%, whereas the prevalence rate of IDA among infants aged 7–12 months was 72% [17]. In 2015, an investigation of 300 infants with IDA aged between 0–6 years in Beijing showed that infants aged 7–12 months had a high prevalence of IDA [13]. The Nutrition Development Report of Chinese Children Aged 0–6 Year
Although iron from breast milk can be absorbed more easily, the iron content is low. After the first four months, infants exhaust their supply of iron transferred from their mother. Infants grow quickly with a high demand for iron, and may easily develop IDA if they are still fed exclusively with breast milk. Exclusive breastfeeding is a risk factor for moderate to severe IDA among infants aged 6–12 months [14]. The longer the infant is breastfed, the worse the severity of childhood anemia [18]. In 2017, Hirata et al. in Japan showed that the infant feeding method was the most significant risk factor for IDA, followed by exclusive breastfeeding, and partial breastfeeding, with formula feeding having the lowest risk [19]. A cross-sectional study in Thailand reported that if mothers received adequate nutritional supplements, including iron, during pregnancy and lactation, exclusive breastfeeding up to 6 months should be advocated due to its substantial health benefits, particularly for anemia [20]. The American Paediatric Society suggested that term infants might take iron supplements to prevent IDA at 4 months of age [21]. The present study found that a longer period of exclusive breastfeeding (>4 months) was a risk factor for infant IDA, whereas mixed feeding was a protective factor. This finding is consistent with the findings from these previous studies. Therefore, communities should improve the guidance for infant feeding, especially regarding starting complementary feeding promptly to reduce the occurrence of IDA.
The WHO and the China Infants Food Guide suggest that complementary feeding should commence at 6 months of age [22]. One domestic study reported that infants who start receiving complementary feeding after 6 months of age had a high incidence of IDA [6]. A systematic retrospective study in Canada showed that starting complementary feeding after 4 months of age may help to reduce the incidence rate of infant IDA in breastfed infants [23]. This study showed that more infants in the IDA group started complementary feeding after 6 months of age than in the control group, and starting complementary feeding late (>6 months of age) was a risk factor for infant IDA. The findings from the present study support that starting complementary feeding of infants at 4–6 months of age may reduce the incidence of infant IDA.
In 2015, Xu et al. showed that low birth weight was a risk factor for moderate to severe IDA in infants aged 6–12 months [14]. The findings from the present study showed that low birth weight was a risk factor for infant IDA, whereas normal birth weight was a protective factor. Also, this study investigated other possible risk factors for IDA. In the 2012 study by Elalfy et al. in Egypt, of infants aged 6–24 months from a poor social background, the investigators identified that being the second-born or later birth order infant was an independent risk factor for IDA [24]. The findings from the present study showed that there was no significant difference in IDA associated with birth order (P>0.05). A domestic cohort study and a case-control study from Sudan found that cesarean births were associated with infant anemia [25,26]. However, the present study showed that the mode of delivery was not significantly associated with the incidence of IDA (P>0.05).
Previous studies have shown that the prevalence of IDA in developed countries was lower than in non-undeveloped areas. Premature infants with low birth weight, aged between 6–24 months (especially 6–12 months) and the introduction of complementary foods later than 6 months of age, are believed to contribute to IDA. The National Program of Action for Child Development in China, 2011–2020, including the strategy for Shanghai Pudong New District, indicated that during 2020, the medical standards of Pudong New District have reached those of a moderately developed country [3]. This study selected a community in Pudong New District, Shanghai, to assess the prevalence and risk factors for IDA in infants and young children in more developed regions in China. Previous studies on IDA have focused more on underdeveloped regions in China. The present study complemented these previous studies, but this study from the Shanghai Children’s Health Check Record system in the Tangqiao Community Health Service Center for infants aged <24 months included the five-year (2010–2015) prevalence of IDA, which was 11.49% overall, 12.75% for male infants, and 10.27% for female infants.
This study had several limitations. A retrospective case-control study was conducted to rapidly determine the risk factors for IDA for infants in Shanghai, China, between 2010–2015, and to investigate the relationship between multiple risk factors and the development of IDA in infants. This study analyzed cross-sectional data and did not establish a causal relationship between the identified risk factors and IDA. Also, the study only included resident infants living in the Tangqiao community in Shanghai, and did not include the infants of the migrant population, which belong to a low socio-economic class and may have underestimated the prevalence rate of IDA in this community. Therefore, this study included a selection bias for the study population. Also, as one community was chosen with a high level of economic development and a relatively stable population in Shanghai was included for data analysis, the study might have underestimated the prevalence of anemia in the population. Also, this study included only one community and caution should be taken when extrapolating these results to the entire city of Shanghai, China, or other communities.
Conclusions
This study aimed to analyze the social determinants of iron deficiency anemia (IDA) in infants living in Shanghai, China, between 2010–2015. The study was conducted to identify factors to support community-based primary and secondary public health intervention measures to reduce IDA in infants. The introduction of an iron-fortified formula for exclusively breastfed infants at 4 months of age, starting complementary feeding promptly before 6 months of age, and improving perinatal care for pregnant women to avoid premature birth and reduce low birth weight may be effective measures to prevent IDA.
Figures
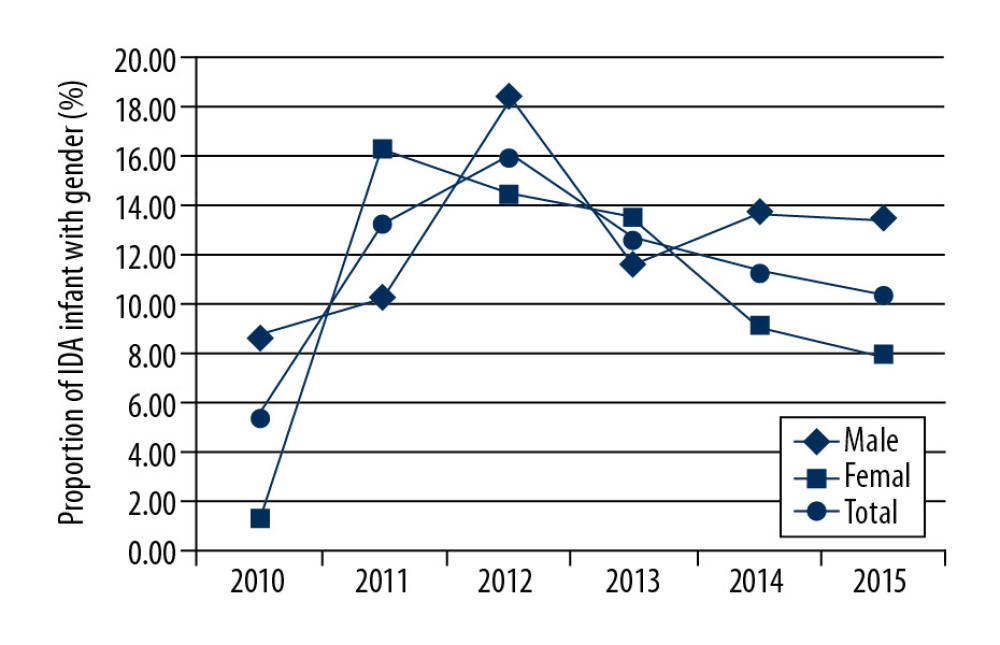 Figure 1. The prevalence of iron deficiency anemia (IDA) in male and female infants in an urban community in Shanghai, China between 2010–2015. The prevalence of IDA in male and female infants was not significantly different (P>0.05).
Figure 1. The prevalence of iron deficiency anemia (IDA) in male and female infants in an urban community in Shanghai, China between 2010–2015. The prevalence of IDA in male and female infants was not significantly different (P>0.05). 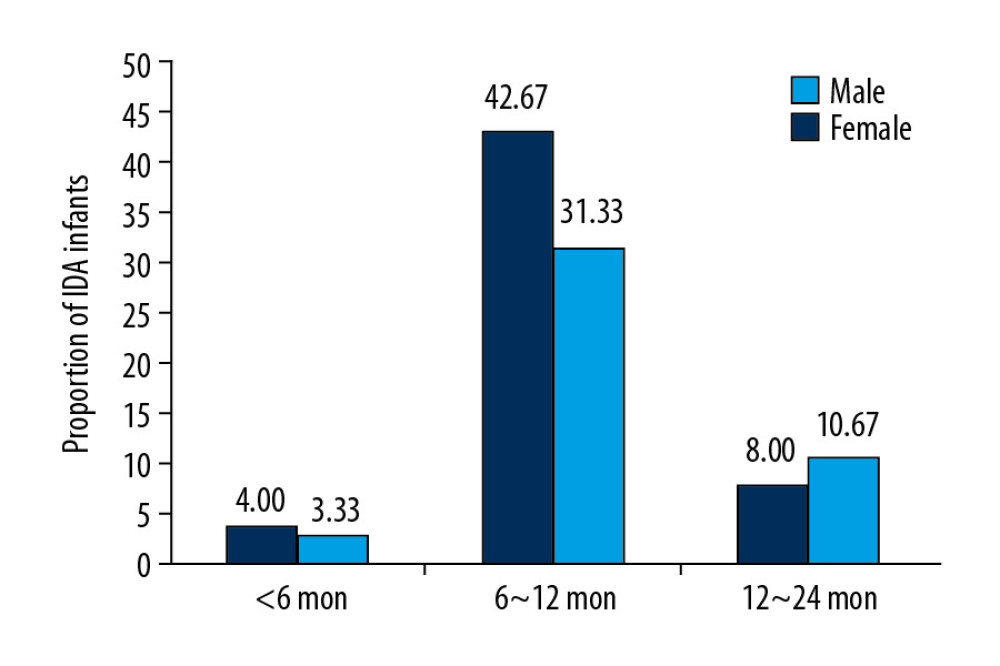 Figure 2. 0Distribution of the age at the time of diagnosis of iron deficiency anemia (IDA) in infants in an urban community in Shanghai, China between 2010–2015. Age at the time of diagnosis of IDA included 11 (7.33%) infants <6 months old, 111 (74%) infants between 6–12 months old, and 28 (18.67%) infants between 12–24 months old. The 6–12 month age group had the highest prevalence of IDA (P<0.01).
Figure 2. 0Distribution of the age at the time of diagnosis of iron deficiency anemia (IDA) in infants in an urban community in Shanghai, China between 2010–2015. Age at the time of diagnosis of IDA included 11 (7.33%) infants <6 months old, 111 (74%) infants between 6–12 months old, and 28 (18.67%) infants between 12–24 months old. The 6–12 month age group had the highest prevalence of IDA (P<0.01). Tables
Table 1. The clinical and demographic characteristics of the infants with iron deficiency anemia (IDA) and the matched control group in an urban community in Shanghai, China between 2010–2015.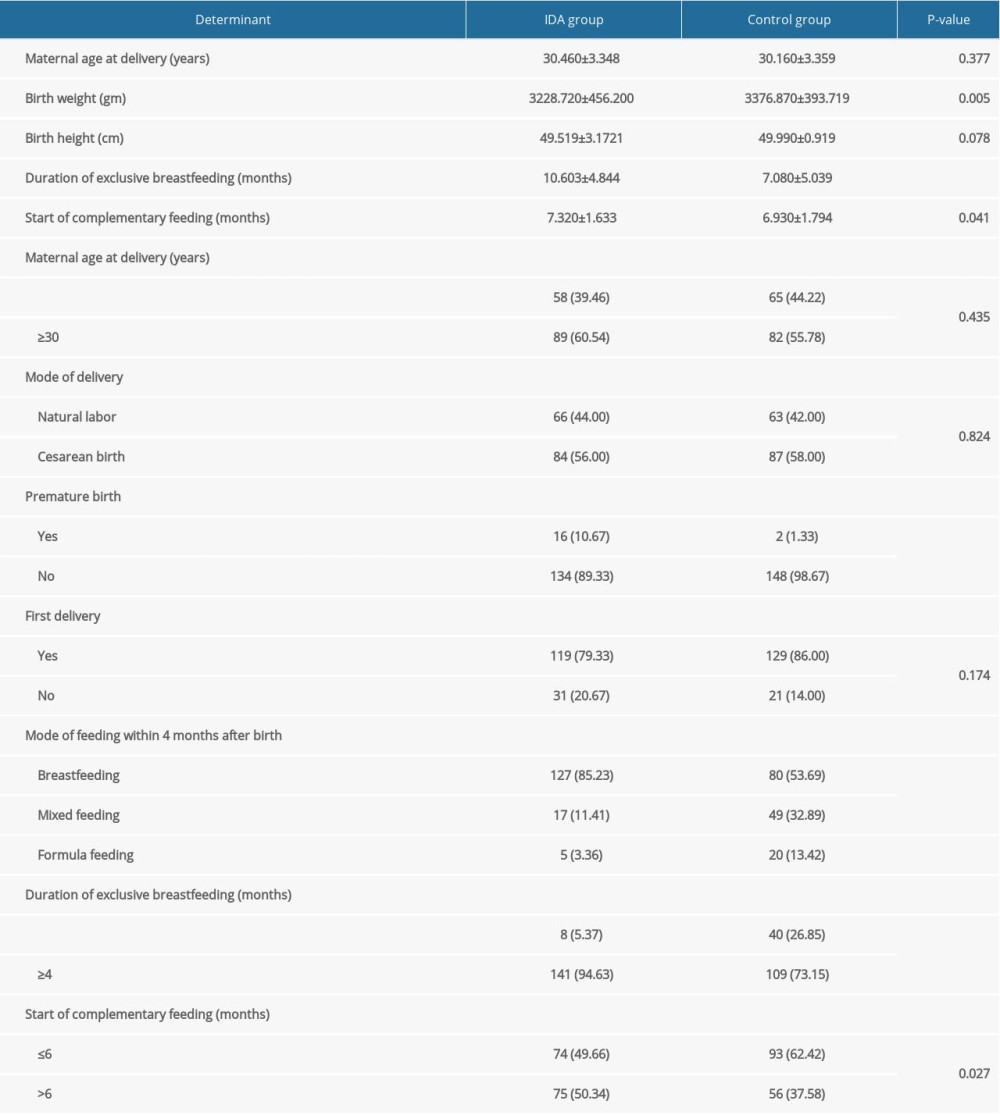 Table 2. Logistic regression analysis of the determinants of iron deficiency anemia (IDA) in infants in an urban community in Shanghai, China between 2010–2015.
Table 2. Logistic regression analysis of the determinants of iron deficiency anemia (IDA) in infants in an urban community in Shanghai, China between 2010–2015.
References
1. Ministry of Health (MOH), National report on nutritional status of children aged 0 to 6 years: Acta Nutrimenta Sinica, 2013; 1; 1-4
2. Jia N, Zhang S, Li T, Dietary survey of anaemic infants and young children in urban areas of China: A cross-sectional study: Asia Pac J Clin Nutr, 2015; 24; 659-64
3. Zhao F: China National Program for Child Development (2011–2020) Feb 13, 2015 http://www.womenofchina.cn/womenofchina/html1/source/1502/997-1.htm
4. WHO/UNICEF/UNU: Iron deficiency anaemia assessment, prevention, and control: A guide for programme managers, 2001, Geneva, World Health Organization https://www.who.int/nutrition/publications/en/ida_assessment_prevention_control.pdf
5. Grantham-McGregor S, Ani C, A review of studies on the effect of iron deficiency on cognitive development in children: J Nutr, 2001; 131; 649S-68S
6. Allali S, Brousse V, Sacri AS, Anemia in children: Prevalence, causes, diagnostic work-up, and long-term consequences: Expert Rev Hematol, 2017; 10(11); 1023-28
7. Larson LM, Phiri KS, Pasricha SR, Iron and cognitive development: What is the evidence?: Ann Nutr Metab, 2017; 71(Suppl 3); 25-38
8. McCann JC, Ames BN, An overview of evidence for a causal relation between iron deficiency during development and deficits in cognitive or behavioral function: Am J Clin Nutr, 2007; 85; 931-45
9. Cusick SE, Georgieff MK, Rao R, Approaches for reducing the risk of early-life iron deficiency-induced brain dysfunction in children: Nutrients, 2018; 10(2); E227
10. Children’s iron deficiency and iron deficiency anaemia, recommendations for prevention and control: Chin J Pediatr, 2008; 46; 502-4 [in Chinese]
11. Lagemaat M, Amesz EM, Schaafsma A, Iron deficiency and anemia in iron-fortified formula and human milk-fed preterm infants until 6 months post-term: Eur J Nutr, 2014; 53; 1263-71
12. Uijterschout L, Domellof M, Abbink M, Iron deficiency in the first 6 months of age in infants born between 32 and 37 weeks of gestational age: Eur J Clin Nutr, 2015; 69; 598-602
13. Li Q, Liang F, Liang W, Prevalence of anemia and its associated risk factors among 6-months-old infants in Beijing: Front Pediatr, 2019; 12(7); 286
14. Xu K, Zhang CM, Huang LHRisk factors for iron deficiency anemia in infants aged 6 to 12 months and its effects on neuropsychological development: Zhongguo Dang Dai Er Ke Za Zhi, 2015; 17(8); 830-36 [in Chinese]
15. Amano I, Murakami A, Prevalence of infant and maternal anemia during the lactation period in Japan: Pediatr Int, 2019; 61(5); 495-503
16. Riahi SM, Mohammadi M, Fakhri Y, Prevalence and determinant factors of anemia in children aged 6–12 months after starting an iron supplement in the east of Iran: Arch Pediatr, 2019; 26(6); 347-51
17. Chandyo RK, Henjum S, Ulak M, The prevalence of anemia and iron deficiency is more common in breastfed infants than their mothers in Bhaktapur, Nepal: Eur J Clin Nutr, 2016; 70; 456-62
18. Buck S, Rolnick K, Nwaba AA, Longer breastfeeding associated with childhood anemia in rural South-Eastern Nigeria: Int J Pediatr, 2019; 2019 9457981
19. Hirata M, Kusakawa I, Ohde S, Risk factors of infant anemia in the perinatal period: Pediatr Int, 2017; 59(4); 447-51
20. Sawasdivorn S, Taeviriyakul S, Are infants exclusively breastfed up to 6 months of age at risk of anemia?: J Med Assoc Thai, 2011; 94(Suppl 3); S178-82
21. Baker RD, Greer FR, Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0–3 years of age): Pediatrics, 2010; 126; 1040-50
22. World Health Organisation (WHO): Global strategy for infant and young child feeding, 2003, Geneva https://www.who.int/nutrition/topics/global_strategy/en/
23. Qasem W, Fenton T, Friel J, Age of introduction of first complementary feeding for infants: A systematic review: BMC Pediatr, 2015; 15; 107
24. Elalfy MS, Hamdy AM, Maksoud SS, Pattern of milk feeding and family size as risk factors for iron deficiency anemia among poor Egyptian infants 6 to 24 months old: Nutr Res, 2012; 32; 93-99
25. Li HT, Trasande L, Zhu LP, Association of cesarean delivery with anemia in infants and children in 2 large longitudinal Chinese birth cohorts: Am J Clin Nutr, 2015; 101; 523-29
26. Adam I, Kheiri S, Sharif ME, Anaemia is associated with an increased risk for caesarean delivery: Int J Gynaecol Obstet, 2019; 147(2); 202-5
Figures
Figure 1. The prevalence of iron deficiency anemia (IDA) in male and female infants in an urban community in Shanghai, China between 2010–2015. The prevalence of IDA in male and female infants was not significantly different (P>0.05).Figure 2. 0Distribution of the age at the time of diagnosis of iron deficiency anemia (IDA) in infants in an urban community in Shanghai, China between 2010–2015. Age at the time of diagnosis of IDA included 11 (7.33%) infants <6 months old, 111 (74%) infants between 6–12 months old, and 28 (18.67%) infants between 12–24 months old. The 6–12 month age group had the highest prevalence of IDA (P<0.01). Tables
Table 1. The clinical and demographic characteristics of the infants with iron deficiency anemia (IDA) and the matched control group in an urban community in Shanghai, China between 2010–2015.Table 2. Logistic regression analysis of the determinants of iron deficiency anemia (IDA) in infants in an urban community in Shanghai, China between 2010–2015.Table 1. The clinical and demographic characteristics of the infants with iron deficiency anemia (IDA) and the matched control group in an urban community in Shanghai, China between 2010–2015.Table 2. Logistic regression analysis of the determinants of iron deficiency anemia (IDA) in infants in an urban community in Shanghai, China between 2010–2015. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387