15 September 2020: Clinical Research
A Novel Multiple-Cue Observational Clinical Scale for Functional Evaluation of Gait After Stroke – The Stroke Mobility Score (SMS)
Dominik Raab1ABCDEFG*, Brigitta Diószeghy-Léránt2ABF, Meret Wünnemann2B, Christina Zumfelde2B, Elena Cramer3BE, Alina Rühlemann4B, Johanna Wagener45B, Silke Gegenbauer6BE, Francisco Geu Flores1G, Marcus Jäger45BEG, Dörte Zietz3BEG, Harald Hefter7ABCDEFG, Andres Kecskemethy1ACDEFG, Mario Siebler2ABCDEFGDOI: 10.12659/MSM.923147
Med Sci Monit 2020; 26:e923147






Abstract
BACKGROUND: For future development of machine learning tools for gait impairment assessment after stroke, simple observational whole-body clinical scales are required. Current observational scales regard either only leg movement or discrete overall parameters, neglecting dysfunctions in the trunk and arms. The purpose of this study was to introduce a new multiple-cue observational scale, called the stroke mobility score (SMS).
MATERIAL AND METHODS: In a group of 131 patients, we developed a 1-page manual involving 6 subscores by Delphi method using the video-based SMS: trunk posture, leg movement of the most affected side, arm movement of the most affected side, walking speed, gait fluency and stability/risk of falling. Six medical raters then validated the SMS on a sample of 60 additional stroke patients. Conventional scales (NIHSS, Timed-Up-And-Go-Test, 10-Meter-Walk-Test, Berg Balance Scale, FIM-Item L, Barthel Index) were also applied.
RESULTS: (1) High consistency and excellent inter-rater reliability of the SMS were verified (Cronbach’s alpha >0.9). (2) The SMS subscores are non-redundant and reveal much more nuanced whole-body dysfunction details than conventional scores, although evident correlations as e.g. between 10-Meter-Walk-Test and subscore “gait speed” are verified. (3) The analysis of cross-correlations between SMS subscores unveils new functional interrelationships for stroke profiling.
CONCLUSIONS: The SMS proves to be an easy-to-use, tele-applicable, robust, consistent, reliable, and nuanced functional scale of gait impairments after stroke. Due to its sensitivity to whole-body motion criteria, it is ideally suited for machine learning algorithms and for development of new therapy strategies based on instrumented gait analysis.
Keywords: Gait Disorders, Neurologic, Stroke, Symptom Assessment, Aged, 80 and over, Disability Evaluation, gait analysis, Video Recording, young adult
Background
Stroke is a leading cause of severe long-term disabilities in industrialized countries [1]. In the USA, about 7.2 million adults are currently living with post-stroke disabilities, while an additional 3.4 million adults yearly are estimated to have a stroke until 2030 [2]. A common impairment after stroke is limited walking ability [3,4]. Since walking is essential for performing many activities of daily living and good quality of life, gait recovery is a primary goal for stroke survivors [5]. Due to high interindividual variance in stroke severity as well as neurologic regeneration capacity, the rehabilitation of walking ability requires a personalized therapy that coordinates the application of physical therapy, robot-assisted therapy, specific medication and orthotic devices [6–8]. In this context, machine learning is being more and more integrated in the future of medical diagnostics and therapeutics [9,10]. However, the data base has to be carefully developed and controlled by human experts in order to furnish reliable machine learning techniques for reproducing or even improving current medical decisions [11]. In order to accomplish effective adjustments of the therapy program during treatment and application for machine learning, a refined assessment of patients’ individual gait dysfunction is necessary.
For stroke rehabilitation, a broad spectrum of established medical scores is available, but their usefulness for functional evaluation of gait after stroke remains limited. On the one hand, neurological scales such as the National Institutes of Health Stroke Scale [6] or the Modified Ashworth Scale [12] are useful for the assessment and documentation of neurologic deficits and motor function after stroke. But since they are based on a medical examination of the patient – in part in lying position – they lack parameters for patients’ dynamic movement performance, which are essential for the evaluation of gait ability.
On the other hand, observational assessments of activities of daily living like the Barthel Index [13], the Functional Independence Measure [6], and the Functional Ambulation Categories [14] or patient questionnaires such as ABILOCO (“ABILOCO: A Rasch-Built 13-Item Questionnaire to Assess Locomotion Ability in Stroke Patients”) [15], ACTIVLIM-Stroke (“A Cross-cultural Rasch-Built Scale of Activity Limitations in Patients With Stroke”) [16], and the Modified Rankin Scale [12] provide an indicator of activity as well as participation after stroke. However, these scores only assess overall gait performance. This also applies to conventional functional tests for mobility, balance, and motor function such as the 10-Meter-Walk-Test [17], the Timed-Up-And-Go-Test [12], and the Berg Balance Scale [18].
Other common observational gait assessment techniques such as the Edinburgh Visual Gait Score [19] and the Rivermead Visual Gait Assessment [20] assess gait movement in detail and thus provide a general picture of gait impairment. However, since they do not include any stroke-specific context, their practical benefit in stroke rehabilitation is limited. Recent review papers [17,21,22] show that the only currently existing scale for gait disorders after stroke is the Wisconsin Gait Scale (WGS) [23]. The WGS is based on a subdivision of the gait cycle of the affected leg in 4 phases and the rating of 14 items describing the leg motion during these phases. However, this approach is complex and focuses solely on leg motion, while the rest of the body is neglected. This contrasts with recent studies that show the movements of the arms and trunk are important aspects of gait pattern after stroke [24,25].
In summary, despite a wide range of scales currently available in neurology and gait analysis, there is still a need for a simple nuanced functional assessment of gait after stroke including arm movement and trunk posture based on standard video recordings. The objective of this study was to introduce a new multiple-cue observational scale, called the stroke mobility score (SMS), to fulfil these requirements.
Material and Methods
POPULATION:
Inclusion criteria for the study population were: (1) proven recent stroke (ischemia or haemorrhage) as verified in a computer tomography (CT) or magnetic resonance imaging (MRI) of the head; (2) medical history of only 1 stroke; (3) time since stroke ≤3 months (time period within 3 months after stroke onset was defined as subacute stroke time, as we wanted to exclude chronic stroke patients in the validation phase of this study to avoid secondary complications due to hip, knee, or spinal pain effected by the walking disability); (4) ability to walk 30 meters without help from an assistant or use of a walking frame; (5) age ≥18 years; and (6) written informed consent. Exclusion criteria were: (1) any surgery within the last year; (2) any neurological or orthopedic symptoms of the stroke interfering with walking during clinical examination; (3) known peripheral artery disease with a restriction of gait or other reasons for limiting walking prior to the stroke; and (4) participation in another study.
The authors obtained Institutional Review Board approval for instrumental gait analysis and clinical examination of stroke patients from the Ethics Committee of the University Duisburg-Essen (application number 18.7988).
MEDICAL EXAMINATION:
All patients received a standard neurological examination and were assessed with the following scores: 10-Meter-Walk-Test [17], Timed-Up-And-Go-Test [12], Modified Rankin Scale [12], National Institutes of Health Stroke Scale [6], Berg Balance Scale [18], Barthel Index [13], and FIM-Item L [6]. Results were documented in a case record file (CRF) and reviewed by an independent study nurse.
VIDEO RECORDINGS:
The SMS is based on standardized whole-body video recordings of gait while walking at a self-selected pace in underwear. The recordings were conducted using 2 video cameras (Basler 602fc, 100 Hz) aligned along and perpendicular to a straight 10-meter indoor walkway, capturing front, back, and left/right side views. Patients were instructed to stand at the beginning of the walkway and to start walking when prompted. At the end of the walkway, the patients had to stop, turn 180 degrees and stand in an upright position, lifting the arms to horizontally as possible. Afterwards, the arms were lowered again, and the patient walked back. The videos were saved on a standalone PC and stored for offline analysis. All recordings were carried out by the same technician.
SCORE DEVELOPMENT:
The Stroke Mobility Score was developed based on the Delphi method by an interdisciplinary team of neurologists, orthopedic surgeons, physiotherapists, study nurses, orthotics specialists, and biomechanical engineers over a period of 5 years within 2 multidisciplinary research projects: “ReHabX-Stroke: Personalized therapy planning of gait disorders based on the example of stroke” (2012–2015) [26] and “RehaBoard: A computer assistance system for the interdisciplinary treatment planning of gait impairments after stroke” (ongoing project 2017–2020) [27]. In a first run (development run), video recordings of the gait of 131 patients were discussed, and essential whole-body movement properties relevant to diagnosis and therapy planning were identified. This led to the following 6 principal functional criteria: (1) trunk posture, (2) leg movement of the most affected side, (3) arm movement of the most affected side, (4) gait speed, (5) gait fluency, and (6) stability of walking on flat ground/risk of falling. For each criterion, a set of 4 simple brief scoring descriptions from 0 (no pathological finding) to 3 (significant pathological findings) was developed and iterated until convergence of the assessment was achieved. The total score is thus the sum of the 6 SMS subscores, giving a number between 0 (no findings) and 18 (most critical). This scale is based solely on observation of videos with only 4 answer options per item, taking about 2–3 minutes for completion. In a second run (validation run), 6 independent medical raters (2 neurologists, 2 physiotherapists, an orthopedic surgeon, and a sports scientist) scored anonymized videos of 60 additional, randomly selected patients according to the SMS manual and an initial calibration step involving supervised scoring of 3 patients not included in the group. None of the raters participated in the score development and thus were novice to the rating system.
STATISTICAL ANALYSIS:
The statistical analysis of the SMS was based on the sample of the 60 validation-run patients. Descriptive statistics were compiled for age, sex, impaired side, and time period since the occurrence of the stroke. All statistics were calculated using IBM SPSS Statistics version 23. A critical level of p<0.05 was considered significant for all statistics except for Tukey’s test of additivity and Levene’s test, for which a progressive critical level of p<0.25 was used according to Wirtz’s recommendation [28].
The consistency of the ratings of the 6 raters was evaluated by corrected item-total correlation and Cronbach’s alpha coefficient. Since the ratings were not normally distributed (Shapiro-Wilk-Test: pi=0.000–0.024), the relationship between the SMS subscores and established clinical scores was assessed by non-parametric rank correlation applying Spearman’s rho. Inter-rater reliability was analysed using the interclass correlation coefficient (ICC) of type 2,1 (two-way random effects model). Tukey’s test of additivity and Levene’s test for equality of variances were calculated as quality criteria of the ICC. The application of the parametric ICC-analysis can be regarded as valid, since it is robust with respect to the normality assumption as long as 50 or more observations are analysed [29].
Results
CONSISTENCY:
Consistency between raters was analysed using corrected item-total Cronbach’s alpha coefficient between each rater’s scorings and the average of the other raters for each SMS subscore and the SMS total score, respectively, over all patients. Table 3 displays the corresponding results. For all raters and for all SMS items, a correlation >0.7 was achieved. The lowest correlations were found for “trunk posture”, while SMS total score and “stability” subscore showed the highest correlation. Only 2 raters (rater 1 and 4) differed moderately from the others in some subscores.
INTER-RATER RELIABILITY:
SMS inter-rater reliability according to interclass correlation coefficient ICC type 2,1 (two-way random effects model) following Fleiss’ guideline [30] proved to be good-to-excellent. Excellent reliability scores (>0.75) were obtained for “leg movement”, “stability of walking on flat ground/risk of falling” and total score, and good reliability scores (>0.6) were achieved for “trunk posture”, “arm movement”, “gait speed”, and “gait fluency” (Table 4).
INTER-SUBSCORE CROSS-CORRELATION:
SMS subscore cross-correlation was evaluated by computing the rank correlation according to Spearman’s rho values between each pair of items (15 pairs) over all 60 patients for each rater (6 raters). Then, the average was taken for each item pair over the 6 raters. Table 5 shows the obtained average values for all item pairs. It can be observed that no SMS item pair correlates high, but that all SMS item pair correlations range on a level of good to moderate. “Leg movement” and “stability/risk of falling” displayed the highest item-total correlation (Cronbach’s alpha coefficient 0.962 resp. 0.974) and inter-rater reliability (ICC2.1 0.796 resp. 0.842), while “trunk posture” and “arm motion” yielded the lowest (Cronbach’s alpha coefficient 0.919 resp. 0.931/ICC2.1 0.601 resp. 0.688).
CROSS-CORRELATION OF AVERAGE SMS SUBSCORES WITH CONVENTIONAL SCORES:
Table 6 shows the cross-correlation between the averaged SMS subscores and the conventional scores used for gait impairment assessment. For better interpretation, columns and rows are ordered such that higher values are displayed in the upper left and the lower values are displayed in the bottom right. The highest correlation results were between the SMS subscores “gait speed”/“gait fluency” and the conventional Ten-Meter-Walk- and Timed-Up-And-Go-Tests. This is not surprising, as both assess velocity, which is quite easy to determine. What was surprising is that the observational SMS assessment based on a simple video was as good in velocity assessment as the measurement with a clock. Reading this result in inverse direction shows that a simple remote observational scale can replace complex instrumented walking speed analysis settings with almost the same clinical information. The table also shows that specific SMS subscores rating localized functional impairments are not reflected by the conventional scores, as seen for the 3 SMS subscores “trunk posture”, “leg movement”, and “arm movement”, which have only weak to moderate correlation with the conventional scores (the lowest being “arm movement”). The results also display that all existing conventional scales, such as Barthel Index, FIM-Item L and Berg Balance Scale, correlate only weakly to moderately with the functional SMS subscores.
Discussion
OUTLOOK:
Due to its observational nature and the empirical evidence that all test raters scored consistently after a short video training on calibration patients and that the results of the different raters from different disciplines were interchangeable, the SMS score is ideal for later training of machine learning algorithms.
Moreover, the SMS score proves to be a consistent, reliable, tele-assessable, and easy-to-learn clinical observational scale for multiple-cue functional evaluation of gait dysfunctions after stroke, which can be used as a bedside test without access to instrumented gait analysis. Thus, the SMS is also suitable for monitoring of the stroke course.
A limitation of this study is that the sample patient database was not balanced between male and female patients. This is due to the situation that a database of patients in normal treatment was used that contained more males than females, and that the random selection from the complete database used in this setting yielded the given male/female distribution. Future studies might use broader test groups. However, it is believed that these will not influence the main findings of this paper, as the observational score is independent of gender differences, in contrast to instrumented gait analysis, in which physiologic differences in geometry and muscle and mass distribution must be considered.
Conclusions
A novel observational clinical scale for multiple-cue functional evaluation of gait after stroke – the Stroke Mobility Score (SMS) – is presented. The score is easy to learn and to apply and is based solely on video recordings of patients’ gaits on a 10-meter walkway, allowing for fast evaluation in just 2–3 minutes, and can also be used in tele-assessment. The SMS can measure aspects of walking that are not part of existing scores, enabling, despite its simplicity, a nuanced functional assessment of gait after stroke, including arm and leg movement as well as trunk posture. Statistical evaluations show that the SMS subscores and its total score have excellent consistency and good-to-excellent inter-rater reliability after a short period of self-study. The analysis of SMS subscore cross-correlations unveils new functional interrelationships for stroke gait profiling. Due to its sensitivity to whole-body motion criteria, it is ideally suited for machine learning algorithms and for development of new therapies based on instrumented gait analysis. Therefore, the SMS meets all relevant requirements for a useful clinical tool for assessment of gait dysfunctionality after stroke and for training of machine learning algorithms. The SMS manual and 6 anonymized patient calibration videos can be downloaded as supplementry materials.
Supplementary Material
T{01, 03, 08, 10, 12, 17}.mp4 and Ratings of SMS training videos.pdf
Material for self-study of SMS: Six videos of impaired gaits and corresponding SMS ratings
SMS scoresheet.pdf
SMS scoresheet as a blank form (DIN A4)
Tables
Table 1. SMS manual.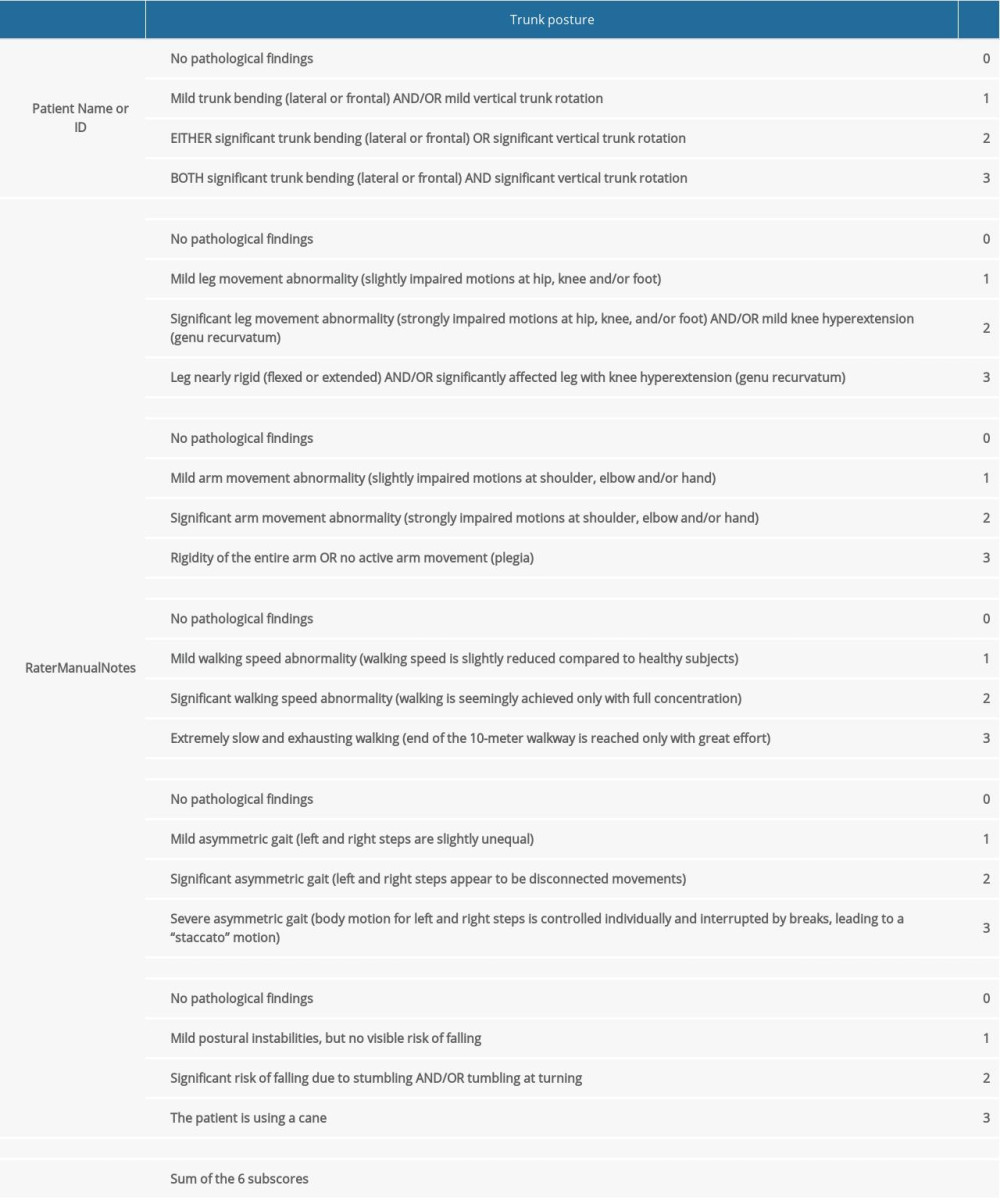 Table 2. Demographical data of rated patients during score development and score validation.
Table 2. Demographical data of rated patients during score development and score validation.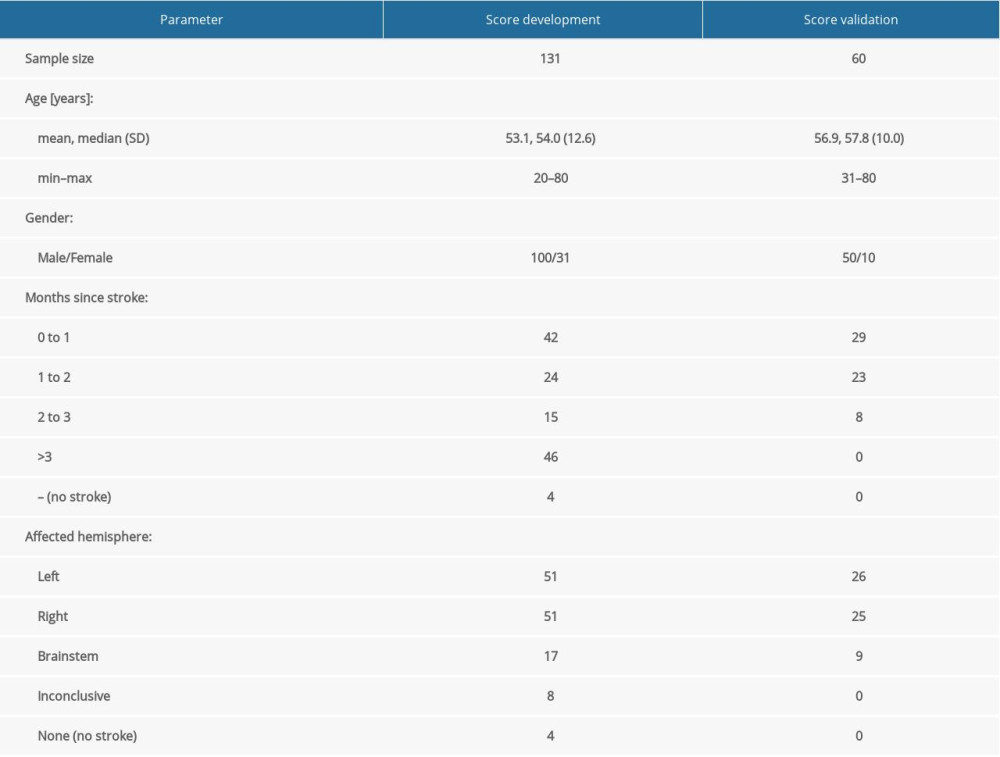 Table 3. Corrected item-total correlation and Cronbach’s alpha for SMS subscores and total score for 6 sample medical raters.
Table 3. Corrected item-total correlation and Cronbach’s alpha for SMS subscores and total score for 6 sample medical raters.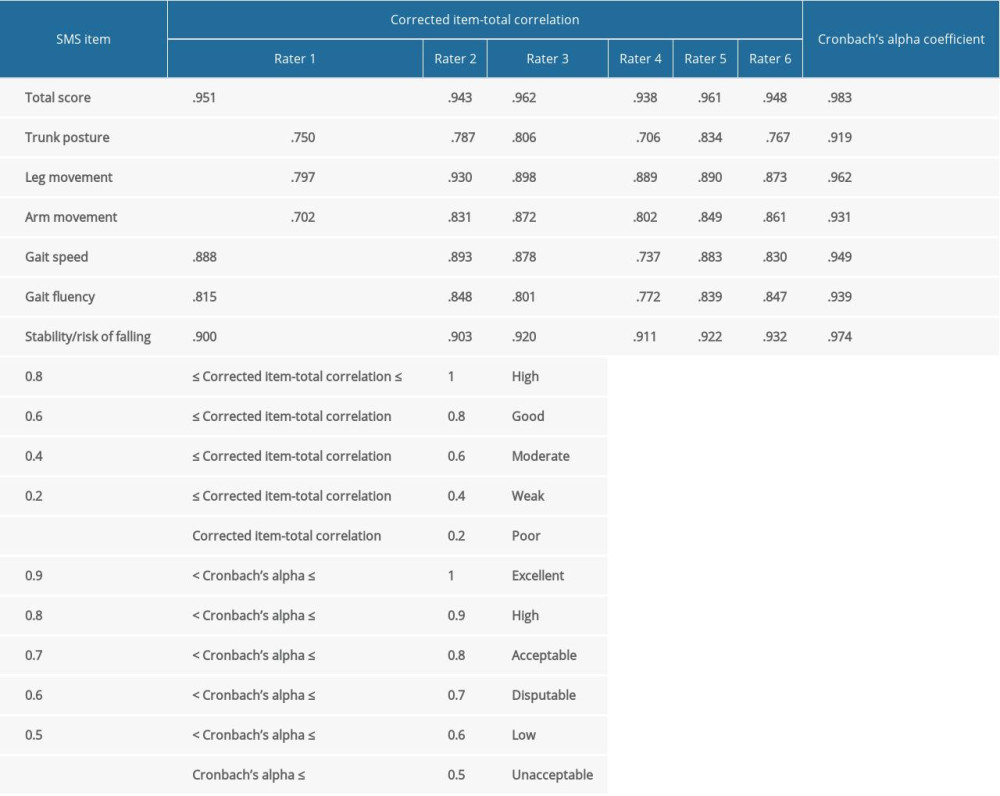 Table 4. Inter-rater reliability ICC2.1 of SMS subscores and SMS total score for 6 sample medical raters.
Table 4. Inter-rater reliability ICC2.1 of SMS subscores and SMS total score for 6 sample medical raters.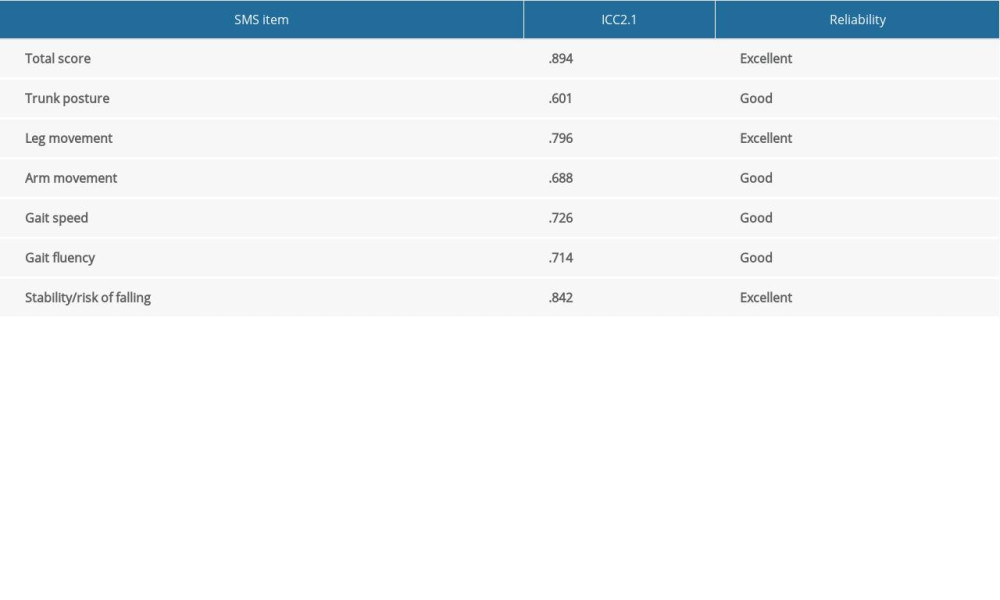 Table 5. Mean Spearman’s cross-correlations between SMS subscores over 6 sample medical raters.
Table 5. Mean Spearman’s cross-correlations between SMS subscores over 6 sample medical raters.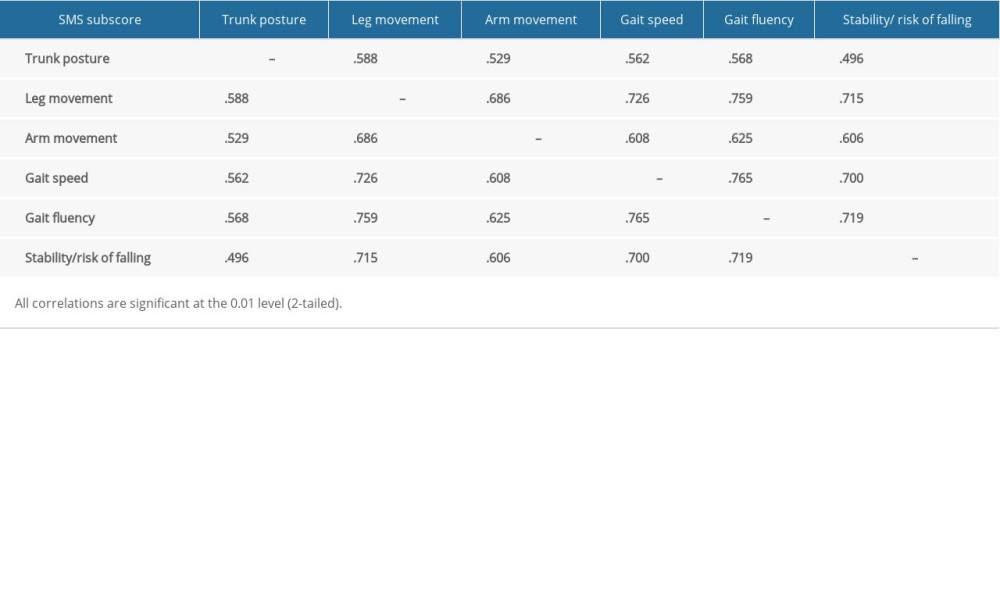 Table 6. Spearman’s cross-correlation between the average SMS subscores and average SMS total score and established scores in stroke rehabilitation.
Table 6. Spearman’s cross-correlation between the average SMS subscores and average SMS total score and established scores in stroke rehabilitation.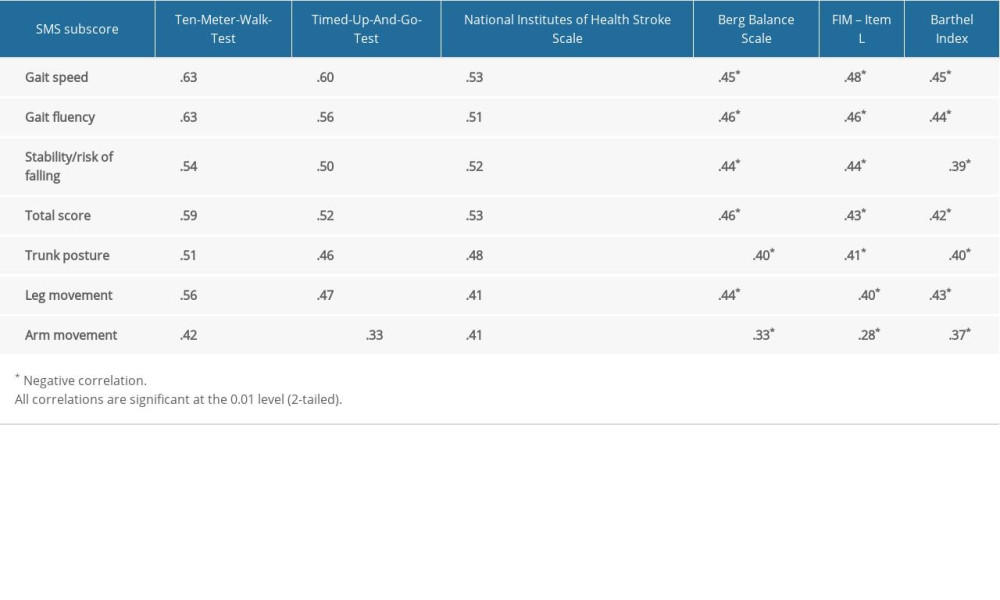
References
1. Belda-Lois J-M, Horno SM-d, Bermejo-Bosch I, Rehabilitation of gait after stroke: A review towards a top-down approach: J Neurong Rehabil, 2011; 8; 66
2. Benjamin EJ, Blaha MJ, Chiuve SE, Heart disease and stroke statistics – 2017 update: A report from the American Heart Association: Circulation, 2017; 135; e146-603
3. Kollen B, van de Port I, Lindeman E, Predicting improvement in gait after stroke: A longitudinal prospective study: Stroke, 2005; 36; 2676-80
4. Lamontagne A, Stephenson JL, Fung J, Physiological evaluation of gait disturbances post stroke: Clin Neurophysiol, 2007; 118; 717-29
5. Preston E, Ada L, Dean CM, What is the probability of patients who are nonambulatory after stroke regaining independent walking? A systematic review: Int J Stroke, 2011; 6; 531-40
6. Duncan PW, Zorowitz R, Bates B, Management of adult stroke rehabilitation care: Stroke, 2005; 36; e100-43
7. Hesse S, Schmidt H, Werner C, Bardeleben A, Upper and lower extremity robotic devices for rehabilitation and for studying motor control: Curr Opin Neurol, 2003; 16; 705-10
8. Husemann B, Müller F, Krewer C, Effects of locomotion training with assistance of a robot-driven gait orthosis in hemiparetic patients after stroke: a randomized controlled pilot study: Stroke, 2007; 38; 349-54
9. Jang H-J, Cho K-O, Applications of deep learning for the analysis of medical data: Arch Pharm Res, 2019; 42; 492-504
10. Kononenko I, Machine learning for medical diagnosis: History, state of the art and perspective: Artif Intell Med, 2001; 23; 89-109
11. Ozcift A, Gulten A, Classifier ensemble construction with rotation forest to improve medical diagnosis performance of machine learning algorithms: Comput Methods Programs Biomed, 2011; 104; 443-51
12. Herndon RM: Handbook of neurologic rating scales, 2006, New York, Demos Medical Publ
13. Mahoney FI, Barthel DW, Functional evaluation: The Barthel Index: Md State Med J, 1965; 14; 61-65
14. Holden MK, Gill KM, Magliozzi MR, Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness: Phys Ther, 1984; 64; 35-40
15. Caty GD, Arnould C, Stoquart GG, ABILOCO: A Rasch-Built 13-Item Questionnaire to assess locomotion ability in stroke patients: Arch Phys Med Rehabil, 2008; 89; 284-90
16. Batcho CS, Tennant A, Thonnard J-L, ACTIVLIM-stroke: A crosscultural Rasch-Built Scale of activity limitations in patients with stroke: Stroke, 2012; 43; 815-23
17. Tyson S, Connell L, The psychometric properties and clinical utility of measures of walking and mobility in neurological conditions: A systematic review: Clin Rehabil, 2009; 23; 1018-33
18. Berg K, Measuring balance in the elderly: Preliminary development of an instrument: Physiotherapy Canada, 1989; 41; 304-11
19. Read HS, Hazlewood ME, Hillman SJ, Edinburgh visual gait score for use in cerebral palsy: J Pediatr Orthop, 2003; 23; 296-301
20. Lord SE, Halligan PW, Wade DT, Visual gait analysis: The development of a clinical assessment and scale: Clin Rehabil, 1998; 12; 107-19
21. Salter K, Jutai JW, Teasell R, Issues for selection of outcome measures in stroke rehabilitation: ICF Participation: Disabil Rehabil, 2005; 27; 507-28
22. Barak S, Duncan PW, Issues in selecting outcome measures to assess functional recovery after stroke: NeuroRX, 2006; 3; 505-24
23. Rodriquez AA, Black PO, Kile KA, Gait training efficacy using a home-based practice model in chronic hemiplegia: Arch Phys Med Rehabil, 1996; 77; 801-5
24. Hefter H, Rosenthal D, Improvement of upper trunk posture during walking in hemiplegic patients after injections of botulinum toxin into the arm: Clin Biomech, 2017; 43; 15-22
25. Hefter H, Jost WH, Reissig A, Classification of posture in poststroke upper limb spasticity: A potential decision tool for botulinum toxin A treatment?: Int J Rehabil Res, 2012; 35; 227-33
26. Kecskeméthy A, Siebler M, Raab D, ReHabX: Personalisierte Therapiesteuerung bei Gangstörungen am Beispiel des Schlaganfalls: Digitale Transformation von Dienstleistungen im Gesundheitswesen V, 2019; 237-54, Wiesbaden, Springer Fachmedien Wiesbaden [in German]
27. Jäger M, Mayer C, Hefter H, Big Data und maschinelles Lernen bei Prävention und Rehabilitation: Orthopade, 2018; 47; 826-33 [in German]
28. Wirtz M, Caspar F: Beurteilerübereinstimmung und Beurteilerreliabilität: Methoden zur Bestimmung und Verbesserung der Zuverlässigkeit von Einschätzungen mittels Kategoriensystemen und Ratingskalen, 2002, Göttingen, Hogrefe Verl. für Psychologie [in German]
29. Stevens JP: Intermediate statistics: A modern approach [SAS, SPSS], 2007, New York NY ua, Erlbaum
30. Fleiss JLWiley classics library: The design and analysis of clinical experiments, 2010, New York, Wiley
31. Vickers AJ, van Calster B, Steyerberg EW, Net benefit approaches to the evaluation of prediction models, molecular markers, and diagnostic tests: BMJ, 2016; 352; i6
32. Wei WE, de Silva DA, Chang HM, Post-stroke patients with moderate function have the greatest risk of falls: A National Cohort Study: BMC Geriatr, 2019; 19; 373
33. Park S-H, Tools for assessing fall risk in the elderly: A systematic review and meta-analysis: Aging Clin Exp Res, 2018; 30; 1-16
34. Tarlov AR, The medical outcomes study: JAMA, 1989; 262; 925-30
Tables
Table 1. SMS manual.Table 2. Demographical data of rated patients during score development and score validation.Table 3. Corrected item-total correlation and Cronbach’s alpha for SMS subscores and total score for 6 sample medical raters.Table 4. Inter-rater reliability ICC2.1 of SMS subscores and SMS total score for 6 sample medical raters.Table 5. Mean Spearman’s cross-correlations between SMS subscores over 6 sample medical raters.Table 6. Spearman’s cross-correlation between the average SMS subscores and average SMS total score and established scores in stroke rehabilitation. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387