21 June 2020: Clinical Research
Serum Cytokines and FeNO in School-Aged Children with Mycoplasma pneumoniae Pneumonia
Hai-li Jin1ABDEG, Lu Zhan1ABC, Shu-fen Mei1BDF, Zheng-yang Shao1CDFG*DOI: 10.12659/MSM.923449
Med Sci Monit 2020; 26:e923449






Abstract
BACKGROUND: Mycoplasma pneumoniae is a major cause of community-acquired pneumonia (CAP) that is particularly prevalent in school-aged children. This study explored the potential involvement of cytokines in children with Mycoplasma pneumoniae pneumonia (MPP) infection.
MATERIAL AND METHODS: Children aged 3–7 years who were hospitalized due to CAP infection were enrolled and divided into 2 groups: an MPP group (n=33) and a NMPP group (n=38), along with 21 age-matched healthy controls. Clinical characteristics and laboratory data were recorded. Serum levels of IL-18, IL-33, IFN-γ, IL-5, IL-6, IL-8, and IL-13 were assessed using Luminex xMAP technology. Correlation analysis and ROC curves analysis were also performed to further explore the role of these detected cytokines in CAP.
RESULTS: Compared with the healthy controls, the serum expression of IL-18, IL-33, IFN-γ, IL-5, IL-6, IL-8, and IL-13 were significantly higher in the MPP and NMPP groups. Furthermore, serum IL-18 expression was found to be significantly correlated with lgE, FeNO, IL-5, IL-8, and IL-13 concentrations. Significant differences were also observed between the MPP group and NMPP group patients in levels of IL-18, IL-5, and IL-6, and further ROC analysis showed that the area under the curve (AUC) of IL-18 and IL-5 were 0.813 (95% CI: 0.710–0.917; P<0.01) and 0.844 (95% CI: 0.756–0.933; P<0.01), respectively.
CONCLUSIONS: IL-18, IL-33, IFN-γ, IL-5, IL-6, IL-8, and IL-13 serum levels showed significant differences in children with CAP. IL-18 and IL-5 were much higher in the MPP group compared to the NMPP group patients, whereas IL-6 levels were significantly lower in these 2 groups.
Keywords: Cytokines, Luminescent Measurements, Nitric Oxide, Pneumonia, Mycoplasma, Receptors, Interleukin-18, Breath Tests, Case-Control Studies, Child, Child, Preschool, Community-Acquired Infections, Immunoglobulin E, interferon-gamma, Interleukin-13, Interleukin-18, Interleukin-33, Interleukin-5, Interleukin-6, Interleukin-8
Background
Cytokines, including Th1-type (IL-2, IFN-γ, TNF-α, and IL-18) and Th2-type (IL-4, IL-5, IL-6, IL-10, and IL-13), can recruit or activate B cells, T cells, and NK cells to initiate and amplify the inflammatory/immune response, thus providing crucial functions in the host defense against bacterial or viral infections.
In the present study, Luminex technology was used to assess the serum Th1/2 cytokines levels in CAP patients treated in our hospital, including 33 children with MPP and 38 with NMPP, as well as 21 healthy controls. Further tests and analysis were performed to investigate the possible roles and correlations of these cytokines in children with CAP with or without
Material and Methods
SUBJECTS AND STUDY DESIGN:
This study, we recruited patients age 3–7 years with signs or symptoms of CAP on admission. We enrolled 71 pneumoniae-infected children (35 girls and 36 boys) from January 2018 to March 2019 in our hospital. The diagnosis of M. pneumoniae was based on clinical and radiological findings, including fever, cough, abnormal lung auscultation, and a new infiltrate on chest radiograph [12]. MPP infection was confirmed based on serologic tests showing MP IgM positivity and antibody titer ≥1: 160, along with positive results for MPP polymerase chain reaction (PCR) tests of nasopharyngeal secretions (Daan Gene, Guangzhou) [13]. The CAP patients without M. pneumoniae infection were defined as having NMPP infection. We also enrolled 21 age-matched, healthy children without pneumoniae infection as healthy controls.
Exclusion criteria were: 1) did not meet the inclusion criteria, or incomplete clinical characteristics data; 2) congenital heart disease, tuberculosis infection, bronchial foreign body, or bronchiectasis; 3) history of personal or family allergies, including asthma, allergic dermatitis, and rhinitis; 4) history of glucocorticoid, bronchodilator, or leukotriene receptor antagonist administration within 2 weeks of admission; and 5) history of smoking or passive smoking [14].
The study was approved by the Ethics Committee of Zhejiang Integrated Traditional and Western Medicine Hospital, China. We obtained signed informed consent from the family members of all participators.
The clinical characteristics data of the enrolled participants were recorded at the time of admission. Peripheral blood was collected from each participant after an 8-h fast on the day of admission. Blood samples were centrifuged at 3000 g for 10 min at 4°C and the obtained serum samples were stored at −80°C for further tests.
CLINICAL LABORATORY TESTS:
The serological tests with an enzyme-linked immunosorbent assay (ELISA) kit (Savyon, Israel) showed increased levels of the specific antibody IgM. Total serum IgE was measured using the Coat-A Count Total IgE IRMA kit with ELISA assay (Diagnostic Products Co., USA).
FeNO levels were measured by an online technique using a NIOX Flex kit (Aerocrine, Solna, Sweden) in accordance with international guidelines. The child inhaled and immediately exhaled at an exhalation rate of 50±5 ml/s maintaining the expiratory pressure at least 4 s, as previously described [15].
White blood cells (WBC) and neutrophils (NEU) were counted using an automated hematology analyzer (Coulter Counter STKS, Beckman Coulter, USA) with blood samples stored in tubes containing EDTA.
SERUM CYTOKINES ANALYSIS:
The concentrations of the serum cytokines IL-18, IL-33, IFN-γ, IL-4, IL-5, IL-6, IL-8, IL-13, and IgE were determined using Luminex-based Milliplex xMAP technology with the Human Cytokine/Chemokine Magnetic Bead Panel Kit (EMD Millipore Corp., Billerica, MA, USA), following to the manufacturers’ instructions.
STATISTICAL ANALYSIS:
Normally distributed data are expressed as mean±standard deviation (SD). One-way ANOVA or Mann-Whitney test was used for comparison of continuous variables, if appropriate, and the chi-square test was used for comparison of categorical variables. Pearson’s correlation analysis was used to explore the relationships between cytokine concentrations and laboratory data. Receiver operating characteristic (ROC) curve analysis was performed to evaluate candidate indicators with regards to the assessment of patients with MPP. Statistical significance was considered as
Results
CLINICAL CHARACTERISTICS:
A total of 92 participants were enrolled into 3 groups in this study, and the clinical characteristics of these groups are summarized in Table 1. There were 33 patients in the MPP group, 38 patients in the NMPP group, and 21 healthy children in the healthy control group. There were no significant differences in age, sex, or BMI among the 3 groups. In the healthy control group, the male: female ratio was 12: 9, and mean age was 4.88±1.40 years, and mean BMI was 15.62±2.12 kg/m2. In the MPP group, the male: female ratio was 15: 18, mean age was 5.04±1.58 years, and mean BMI was 15.46±2.20 kg/m2. In the NMPP group, the male: female ratio was 21: 17, mean age was 4.79±1.44 years, and mean BMI was 15.83±1.97 kg/m2. We also assessed presence of common clinical respiratory and extra-pulmonary symptoms. Compared with the healthy control group, children in the MPP group and NMPP group were more likely to have fever and cough, with no significantly differences between the 2 groups, and the incidences of sputum, wheezing, and chest pain were also higher. Extra-pulmonary manifestations, including skin manifestations and anemia, were also observed. Concerning the clinical course, we found that the duration was 7.88±3.50 days in the MP group and 8.13±3.62 days in the NMP group.
CLINICAL LABORATORY DATA OF THE STUDY PARTICIPANTS:
Laboratory data of the 3 groups are shown in Table 2. The levels of IgE, FeNO, and WBC and the percentages of NEU in children with MPP and NMPP infection were significantly higher than in healthy children (P<0.05). There were no significant differences in levels of FeNO, and WBC and the percentage of NEU between MPP and NMPP groups, but the level of the lgE in the MP group was significantly higher than in the NMP group (P<0.05).
COMPARISON OF THE SERUM CYTOKINES AMONG GROUPS:
To investigate the roles of the inflammatory cytokines in pneumoniae, the levels of IL-18, IL-33, IFN-γ, IL-4, IL-5, IL-6, IL-8, and IL-13 in serum samples from 21 healthy controls and the 71 patients were measured with Luminex technology (Figure 1). The results showed that the expression of these cytokines was mostly higher in CAP patients compared with those in healthy controls. Serum levels of IL-18, IL-33, IL-5, IL-6, IL-8, and IL-13 in the MPP patient group were significantly higher than those in the healthy control group (P<0.01). Serum levels of IL-18, IL-33, IFN-γ, IL-5, IL-6, and IL-13 in the NMPP group were significantly higher than those in the healthy control group (P<0.01). Significantly differences were also observed between the MPP group and NMPP group in levels of IL-18, IL-5, and IL-6 (P<0.01, P<0.01, and P<0.05, respectively).
As some of the detected serum cytokines levels were significantly different between the MPP and NMPP groups, ROC curves analysis was performed. As shown in Table 3 and Figure 2, the ROC curves results showed that the area under the curve (AUC) of IL-18 and IL-5 were 0.813 (95%CI: 0.710–0.917; P<0.01) and 0.844 (95%CI: 0.756–0.933; P<0.01), respectively. When the cut-off value for IL-18 was set at 250.59 pg/mL, the sensitivity and specificity were 69.7% and 86.8%, respectively; and when the cut-off values for the IL-5 was set at 42.19 pg/mL, the sensitivity and specificity were 84.8% and 68.4%, respectively.
CORRELATION ANALYSIS OF IL-18, IL-33, AND OTHER FACTORS:
The correlations between IL-18, IL-33, and IFN-γ, IL-5, IL-6, IL-8, IL-13, and FeNO are shown in Figure 3. The results indicated that the correlations between the levels of IL-18 and IL-5, IL-6, IL-8, IL-13, FeNO (r=0.552, P<0.001; r=0.234, P<0.05; r=0.461, P<0.001; r=0.457, P<0.001; r=0.206, P<0.05, respectively), as well as the correlations between the levels of IL-33 and IL-4, IL-6, IL-8, FeNO (r=−0.258, P<0.05; r=0.218, P<0.05; r=0.284, P<0.05; r=0.226, P<0.05, respectively) were statistically significant.
Discussion
MPP is a frequent cause of community-acquired respiratory infections in school-aged children. Regarding the pathogenesis of MPP, many studies have revealed that cytokines secreted from various types of cells during
Researchers have found that the cell cytokines-mediated inflammation and immune response of the host play an important role in mycoplasmal pathogenicity, especially Th1-type and Th2-type cytokines [16]. IL-18 is considered to be a Th1 pro-inflammatory cytokine and acts as a co-factor for both Th1/Th2 cells activation and lgE production. Repeated administration of IL-18 can stimulate T cells and macrophages to secrete IFN-γ, IL-5, and IL-6, which in turn induces neutrophilia and eosinophilia in mice [17]. IL-18 also has an important role in allergic disease and pulmonary disease [18,19]. We found that serum levels of IL-18 were significantly higher in MPP and NMPP patients compared with the healthy controls (
IL-5 is secreted by Th2 cells and is critically linked to atopic diseases such as allergies and asthma. A study showed that IL-5-deficient mice failed to develop pulmonary eosinophilia and airway hyperresponsiveness after allergen challenge, indicated an important role of IL-5 in the respiratory tract [23]. In children with wheezing, serum levels of IL-5 were significantly higher in subjects with acute
IL-6 is an important pro-inflammatory cytokine and is a useful biomarker for prediction of mortality in hospitalized patients with CAP [26]. In our study, IL-6 levels were significantly higher in MPP patients compared with the healthy controls, and significant differences were also found between MMP and NMMP patients (
The presence of allergic diseases or respiratory infections specifically increase IgE levels. Our study also found that IgE levels were significantly higher in CAP patients compared with the controls. Wang et al. also reported that the serum levels of IgE in
FeNO is a marker of respiratory disease and is used in clinical practice to evaluate the inflammatory status of patients with various respiratory disorders, especially asthma. The increased FeNO levels are caused by pro-inflammatory cytokines inducing NOS2. Higher FeNO levels were reported to be associated with ever physician-diagnosed pneumonia in a cross-sectional study among 507 children aged 5 years [32]. Lee et al. showed that FeNO levels were significantly higher in patients with acute eosinophilic pneumonia than in those without acute eosinophilic pneumonia, and the elevated FeNO levels were reduced after treatment [33]. In the present study, higher levels of FeNO were also observed in CAP patients, and correlation analysis showed that the concentrations of FeNO were significantly correlated with IL-18 and IL-33 levels, suggesting that FeNO levels in CAP are closely associated with production of pro-inflammatory cytokines and respiratory tract inflammation.
Conclusions
We found that the serum levels of IL-18, IL-5 (increased), and IL-6 (decreased) were significantly different between MPP and NMPP patients. These findings might help to better understand the immunological aspects of MPP pathogenesis and related complications. However, larger clinical and immunological investigations are needed to clarify the precise role of specific cytokines in MPP infection.
Figures
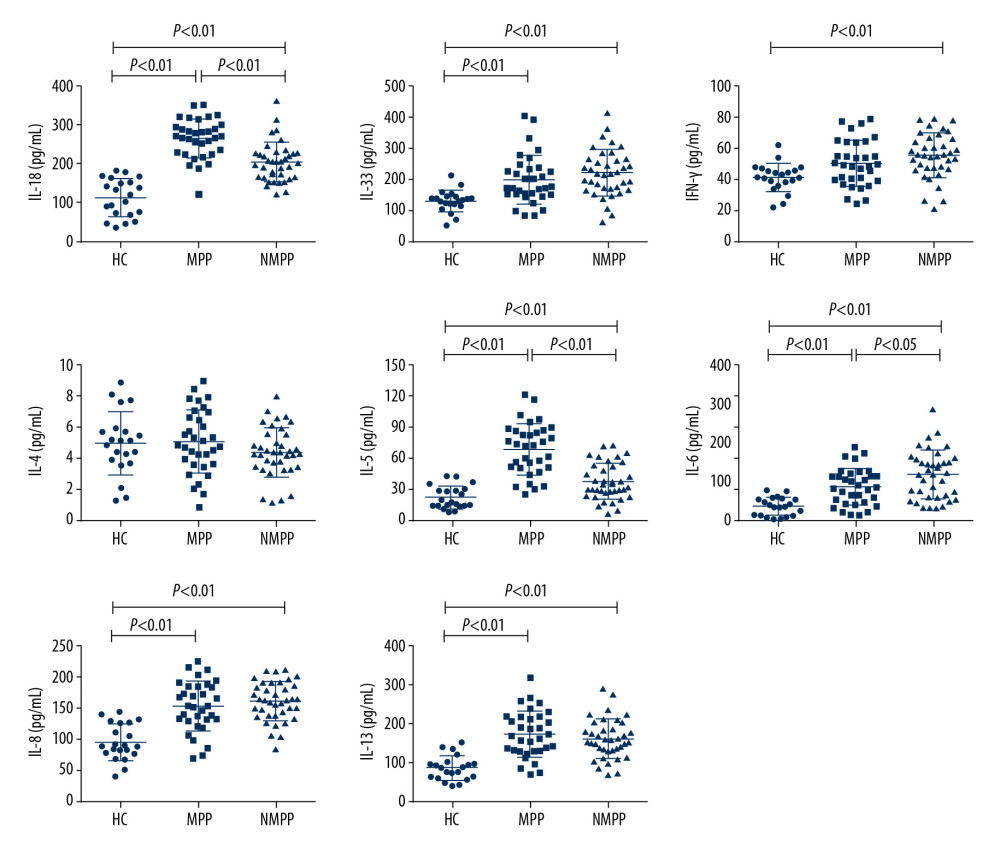 Figure 1. Serum concentrations of IL-18, IL-33, IFN-r, IL-4, IL-5, IL-6, IL-8, and IL-13 in subjects were determined by Luminex assay. HC – healthy control; MPP – Mycoplasma pneumoniae pneumonia; NMPP – non-Mycoplasma pneumoniae pneumonia. Differences among distributed variables were analyzed using the t test or Mann-Whitney U test, as appropriate. Data are presented as the mean±SD (n=21 for HC, n=33 for MPP, patients, n=38 for NMPP patients). P<0.05 was considered as indicating a statistically significant difference.
Figure 1. Serum concentrations of IL-18, IL-33, IFN-r, IL-4, IL-5, IL-6, IL-8, and IL-13 in subjects were determined by Luminex assay. HC – healthy control; MPP – Mycoplasma pneumoniae pneumonia; NMPP – non-Mycoplasma pneumoniae pneumonia. Differences among distributed variables were analyzed using the t test or Mann-Whitney U test, as appropriate. Data are presented as the mean±SD (n=21 for HC, n=33 for MPP, patients, n=38 for NMPP patients). P<0.05 was considered as indicating a statistically significant difference. 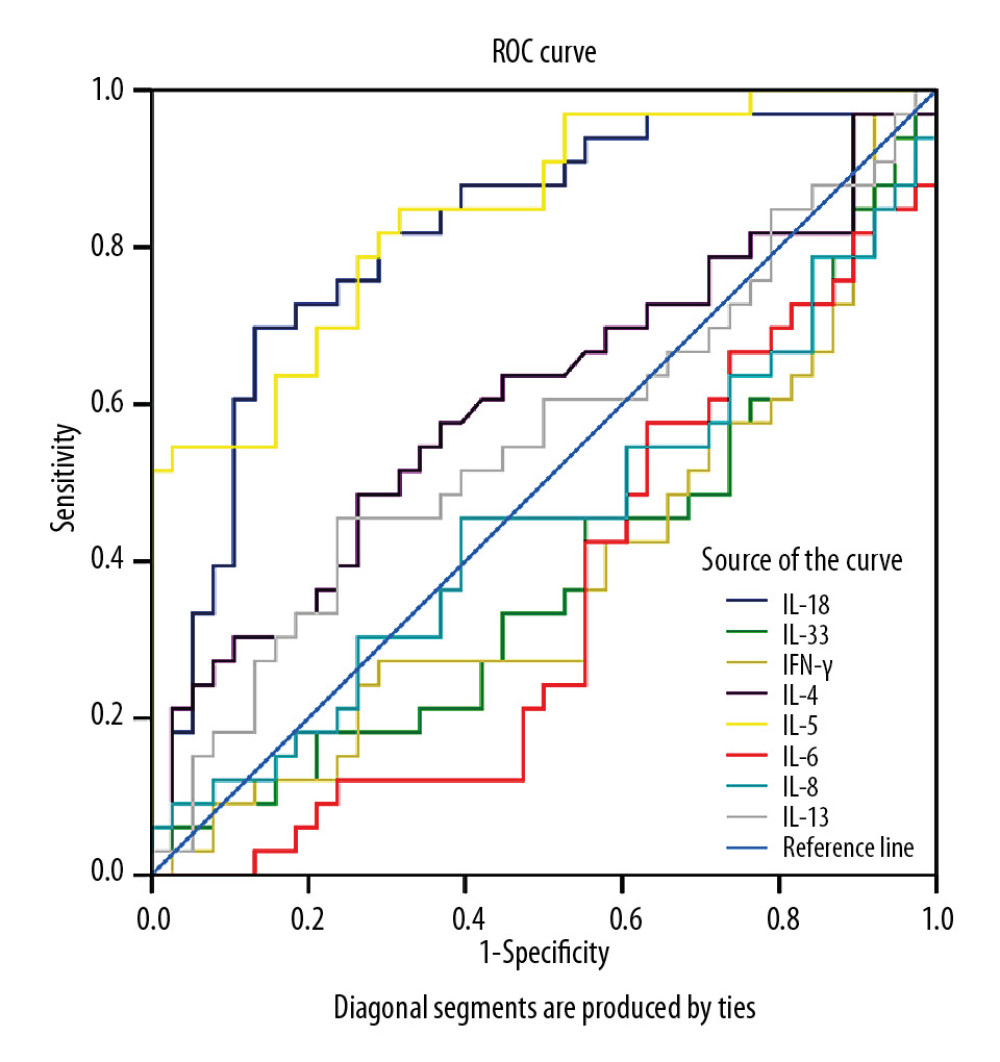 Figure 2. ROC curves of the cytokines differentiating MPP among CAP cases. ROC – receiver operating characteristic; MPP – Mycoplasma pneumoniae pneumonia; CAP – community-acquired pneumonia.
Figure 2. ROC curves of the cytokines differentiating MPP among CAP cases. ROC – receiver operating characteristic; MPP – Mycoplasma pneumoniae pneumonia; CAP – community-acquired pneumonia. 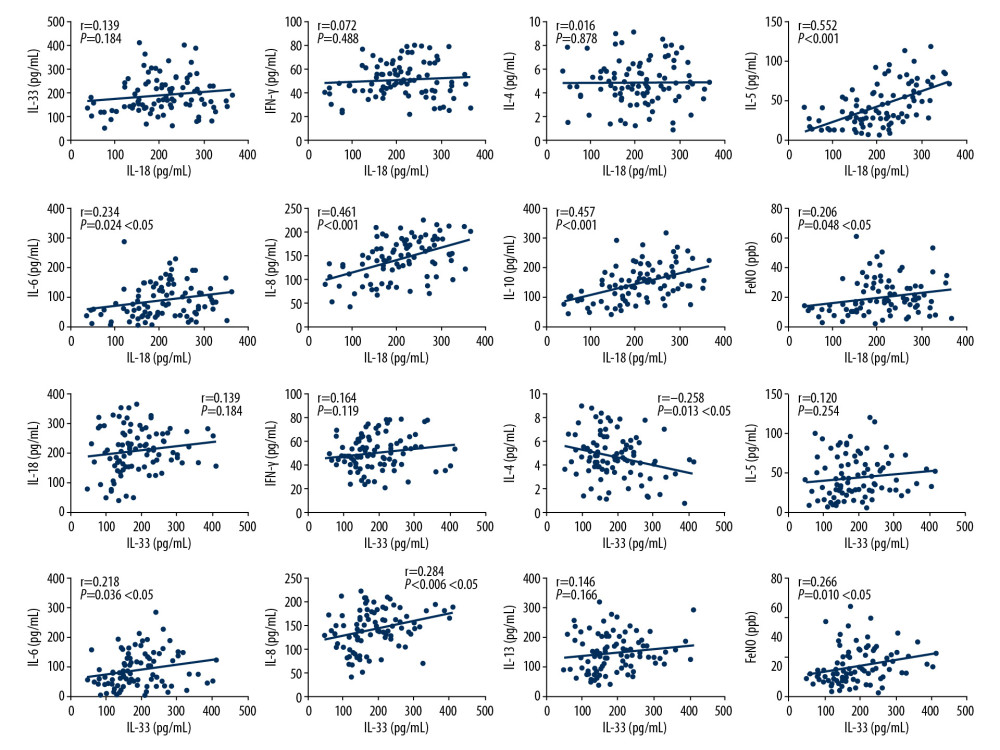 Figure 3. Correlations between IL-18, IL-33, and other serum cytokines. Correlations were tested using the Person’s test, and P<0.05 was considered as indicating a statistically significant difference. Feno – fractional exhaled nitric oxide.
Figure 3. Correlations between IL-18, IL-33, and other serum cytokines. Correlations were tested using the Person’s test, and P<0.05 was considered as indicating a statistically significant difference. Feno – fractional exhaled nitric oxide. References
1. Atkinson TP, Balish MF, Waites KB: FEMS Microbiol Rev, 2008; 32(6); 956-73
2. Principi N, Esposito S: Lancet Infect Dis, 2001; 1(5); 334-44
3. Poddighe D: Curr Opin Rheumatol, 2018; 30(4); 380-87
4. Wagner K, Imkamp F, Pires VP, Keller PM: Clin Microbiol Infect, 2019; 25(3); 383.e5-e7
5. Zar HJ, Bacterial and viral pneumonia: New insights from the Drakenstein Child Health Study: Paediatr Respir Rev, 2017; 24; 8-10
6. Liu L, Oza S, Hogan D, Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: An updated systematic analysis: Lancet, 2015; 385(9966); 430-40
7. Principi N, Esposito S, Management of severe community-acquired pneumonia of children in developing and developed countries: Thorax, 2011; 66(9); 815-22
8. Chu HW, Honour JM, Rawlinson CA: Infect Immun, 2003; 71(3); 1520-26
9. Shimizu T, Kida Y, Kuwano K: Infect Immun, 2008; 76(1); 270-77
10. Ding S, Wang X, Chen W: PLoS One, 2016; 11(1); e0146397
11. Gasiuniene E, Janulaityte I, Zemeckiene Z, Elevated levels of interleukin-33 are associated with allergic and eosinophilic asthma: Scand J Immunol, 2019; 89(5); e12724
12. Zhang Y, Mei S, Zhou Y: Sci Rep, 2016; 6; 37037
13. Zhang Y, Zhou Y, Li S: PLoS One, 2016; 11(5); e0156465
14. Fan Q, Gu T, Li P: Heart Lung Circ, 2016; 25(12); 1226-31
15. Schoos AM, Christiansen CF, Stokholm J, FeNO and exercise testing in children at risk of asthma: J Allergy Clin Immunol Pract, 2018; 6(3); 855-62.e2
16. Yang J, Hooper WC, Phillips DJ, Talkington DF: Cytokine Growth Factor Rev, 2004; 15(2–3); 157-68
17. Ogura T, Ueda H, Hosohara K, Interleukin-18 stimulates hematopoietic cytokine and growth factor formation and augments circulating granulocytes in mice: Blood, 2001; 98(7); 2101-7
18. Kandikattu HK, Upparahalli Venkateshaiah S, Mishra A, Synergy of Interleukin (IL)-5 and IL-18 in eosinophil mediated pathogenesis of allergic diseases: Cytokine Growth Factor Rev, 2019; 47; 83-98
19. Dima E, Koltsida O, Katsaounou P, Implication of Interleukin (IL)-18 in the pathogenesis of chronic obstructive pulmonary disease (COPD): Cytokine, 2015; 74(2); 313-17
20. Ding S, Wang X, Chen W: PLoS One, 2016; 11(1); e0146397
21. Tanaka H, Narita M, Teramoto S: Chest, 2002; 121(5); 1493-97
22. Hoshino T, Kawase Y, Okamoto M: J Immunol, 2001; 166(12); 7014-18
23. Hoek KL, Cassell GH, Duffy LB, Atkinson TP: J Allergy Clin Immunol, 2002; 109; 470-76
24. Esposito S, Droghetti R, Bosis S: Pediatr Pulmonol, 2002; 34(2); 122-27
25. Chung HL, Kim SG, Shin IH: Pediatr Allergy Immunol, 2006; 17(4); 285-90
26. Andrijevic I, Matijasevic J, Andrijevic L, Interleukin-6 and procalcitonin as biomarkers in mortality prediction of hospitalized patients with community acquired pneumonia: Ann Thorac Med, 2014; 9; 162-67
27. Michelow IC, Katz K, McCracken GH, Hardy RD, Systemic cytokine profile in children with community-acquired pneumonia: Pediatr Pulmonol, 2007; 42(7); 640-45
28. Xu XF, Li XJ, Liu JL: Cytokine, 2016; 86; 73-78
29. Wang L, Chen Q, Shi C, Changes of serum TNF-α, IL-5 and IgE levels in the patients of mycoplasma pneumonia infection with or without bronchial asthma: Int J Clin Exp Med, 2015; 8(3); 3901-6
30. Wang Z, Sun J, Liu Y: J Clin Lab Anal, 2019; 33(5); e22887
31. Poddighe D, Comi EV, Brambilla I: Iran J Allergy Asthma Immunol, 2018; 17(5); 490-96
32. Zhang X, Fan Q, Bai X, Levels of fractional exhaled nitric oxide in children in relation to air pollution in Chinese day care centres: Int J Tuberc Lung Dis, 2018; 22(7); 813-19
33. Lee JE, Rhee CK, Lim JH, Fraction of exhaled nitric oxide in patients with acute eosinophilic pneumonia: Chest, 2012; 141(5); 1267-72
Figures
Figure 1. Serum concentrations of IL-18, IL-33, IFN-r, IL-4, IL-5, IL-6, IL-8, and IL-13 in subjects were determined by Luminex assay. HC – healthy control; MPP – Mycoplasma pneumoniae pneumonia; NMPP – non-Mycoplasma pneumoniae pneumonia. Differences among distributed variables were analyzed using the t test or Mann-Whitney U test, as appropriate. Data are presented as the mean±SD (n=21 for HC, n=33 for MPP, patients, n=38 for NMPP patients). P<0.05 was considered as indicating a statistically significant difference.Figure 2. ROC curves of the cytokines differentiating MPP among CAP cases. ROC – receiver operating characteristic; MPP – Mycoplasma pneumoniae pneumonia; CAP – community-acquired pneumonia.Figure 3. Correlations between IL-18, IL-33, and other serum cytokines. Correlations were tested using the Person’s test, and P<0.05 was considered as indicating a statistically significant difference. Feno – fractional exhaled nitric oxide. Tables
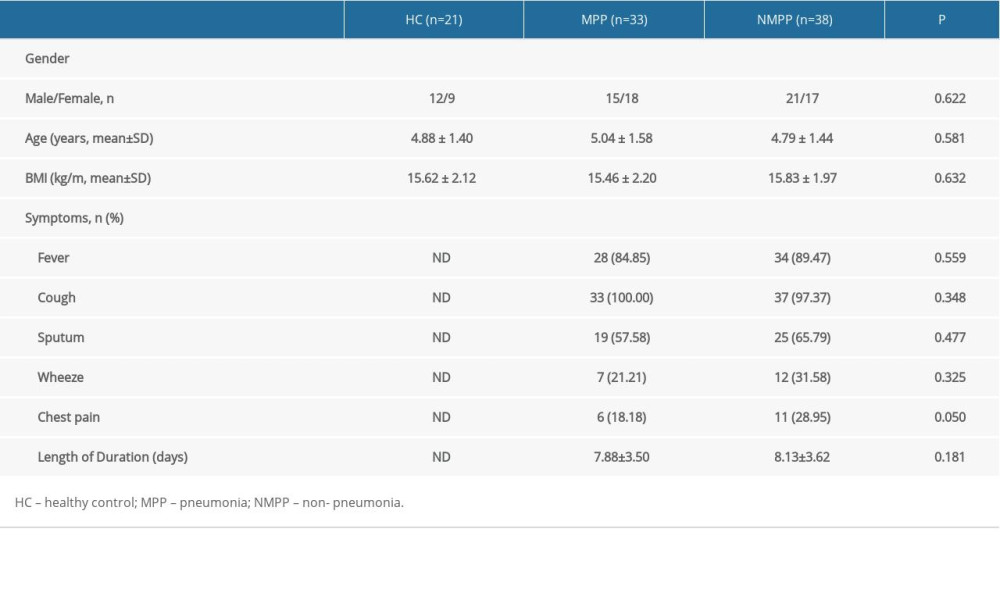 Table 1. Clinical characteristics of the study subjects.
Table 1. Clinical characteristics of the study subjects.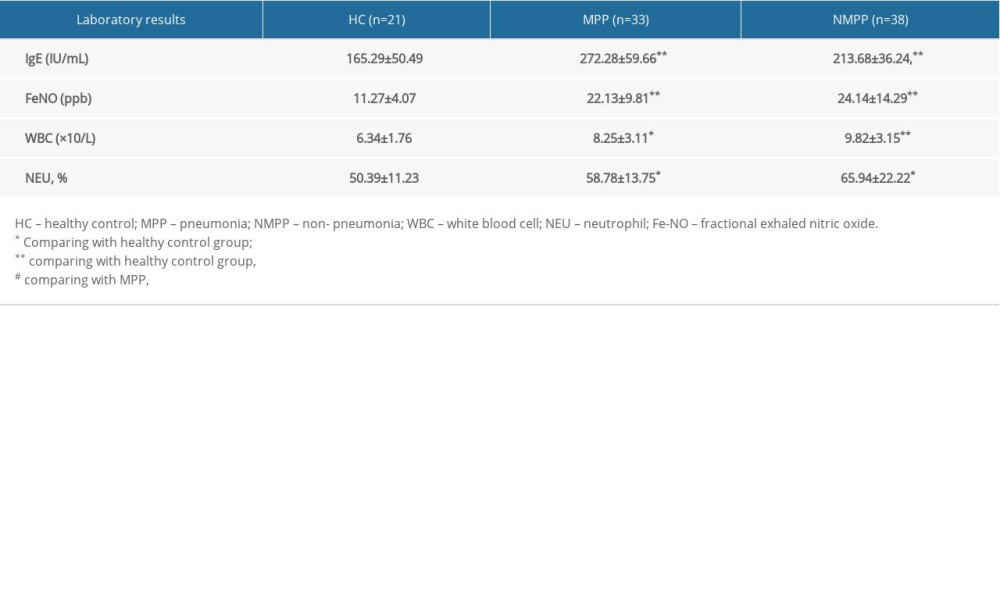 Table 2. Laboratory data of the children with or without Mycoplasma pneumoniae infection. (Data are presented as the mean±SD).
Table 2. Laboratory data of the children with or without Mycoplasma pneumoniae infection. (Data are presented as the mean±SD).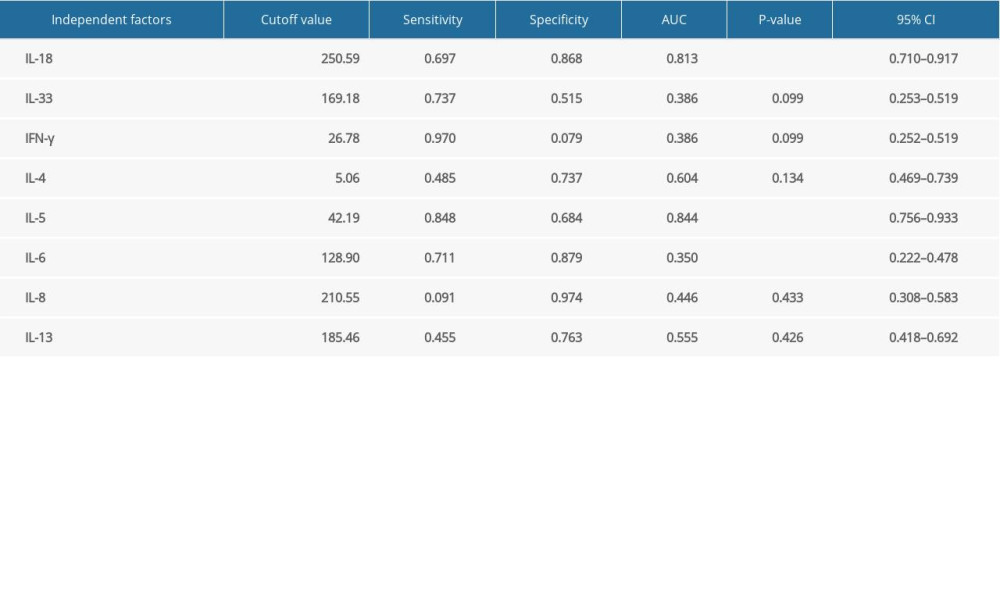 Table 3. ROC curve analysis of differences in cytokines in MPP and NMPP.Table 1. Clinical characteristics of the study subjects.Table 2. Laboratory data of the children with or without Mycoplasma pneumoniae infection. (Data are presented as the mean±SD).Table 3. ROC curve analysis of differences in cytokines in MPP and NMPP.
Table 3. ROC curve analysis of differences in cytokines in MPP and NMPP.Table 1. Clinical characteristics of the study subjects.Table 2. Laboratory data of the children with or without Mycoplasma pneumoniae infection. (Data are presented as the mean±SD).Table 3. ROC curve analysis of differences in cytokines in MPP and NMPP. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387