29 June 2020: Clinical Research
Clinical Efficacy of Combined Hysteroscopic and Laparoscopic Surgery and Reversible Ligation of the Uterine Artery for Excision and Repair of Uterine Scar in Patients with Type II and III Cesarean Scar Pregnancy
Lina Huang1ABEF, Lingjun Zhao1BCD, Huiwei Shi1ABC*DOI: 10.12659/MSM.924076
Med Sci Monit 2020; 26:e924076






Abstract
BACKGROUND: With the changes in China’s family planning policy, the incidence of cesarean scar pregnancy (CSP) significantly increased in recent years. The present study aimed to investigate the clinical efficacy of combined hysteroscopic and laparoscopic surgery and reversible ligation of the uterine artery for cesarean scar excision and repair in patients with type II and III CSP.
MATERIAL AND METHODS: This was a retrospective study of 173 patients with type II and III CSP. They were assigned to the hysteroscopy and laparoscopy group (group A), hysteroscopy group (group B), and curettage group (group C) according to the surgery they underwent. The surgical indicators (intraoperative bleeding volume and hospital stay), postoperative recovery (time of serum β-hCG returning to the normal, postoperative residual lesion, the thickness of the uterine scar, and recovery time of menstruation), and the postoperative complications were compared among the 3 groups.
RESULTS: In patients with type II and III CSP, significant differences (P<0.05) were observed between group A vs. groups B and C in terms of the time of serum β-HCG returning to normal, postoperative residual lesions, the thickness of the uterine scar, and recovery time of menstruation, while there were no significant differences in intraoperative bleeding volume and postoperative hospital stay (P>0.05).
CONCLUSIONS: For patients with type II and III CSP, hysteroscopy and laparoscopy surgery and reversible ligation of the uterine artery achieved better clinical outcomes than hysteroscopy or curettage with respect to postoperative recovery. This could be suitable for patients with CSP and desire for fertility.
Keywords: Hysteroscopy, Laparoscopy, Postoperative Complications, uterine artery embolization, Blood Loss, Surgical, Cesarean Section, Cicatrix, Dilatation and Curettage, Length of Stay, Ligation, Pregnancy, Pregnancy, Ectopic, Reconstructive Surgical Procedures, Surgery, Computer-Assisted, Ultrasonography, uterine artery
Background
A cesarean scar pregnancy (CSP) is a type of ectopic pregnancy in which the fertilized egg implants itself in the uterine incision scar left by a previous cesarean section, and this is a time-limited definition limited to early pregnancy only (≤12 weeks) [1]. The incidence of CSP is 1: 1800 to 1: 2216 and accounts for 6.1% of all ectopic pregnancies or in 0.15% of women with a history of cesarean section [2,3].
Recently, the family planning policy of China was adjusted, and many women with a history of cesarean section are allowed the possibility of becoming pregnant again, and the incidence of CSP has been increasing. CSP can cause uncontrollable severe bleeding, uterine rupture, and damage to the surrounding organs such as the bladder, seriously threatening the women’s reproductive health and even their lives. Therefore, the definitive diagnosis should be made available as early as possible for reasonable treatments [4,5].
Ultrasound is the preferred diagnostic choice for CSP, but MRI is an effective method when a definitive diagnosis cannot be obtained by ultrasound [6–8]. In 2016, the
Presently, there is no consensus on the management of CSP. Individualized therapeutic strategies are planned based on the location of the gestational sac, the thickness of the uterine scar, and blood supply [4,10,11]. Surgical methods for CSP mainly include curettage, removal of pregnancy tissues, and repair of the uterine scar. In critical situations such as major bleeding, hysterectomy can be performed to save the life of patients [5,12]. Curettage involves ultrasound-guided curettage and hysteroscopic removal of pregnancy tissues. The removal of the pregnancy products and repair of the uterine scar can be performed by laparotomy and laparoscopy (or combined with hysteroscopy), which can be performed transvaginally [13]. To reduce the risk of intraoperative bleeding in patients with type II and III CSP, uterine arterial embolization (UAE) or temporary occlusion of the uterine artery is often used as a pretreatment, followed by curettage or removal of the pregnancy tissues.
Hence, the present study aimed to investigate the clinical efficacy of combined hysteroscopic and laparoscopic surgery and reversible ligation of the uterine artery for cesarean scar excision and repair in patients with type II and III CSP. The patients were grouped according to the surgery they underwent: hysteroscopy and laparoscopy
Material and Methods
GENERAL DATA:
Patients with type II and III CSP who were hospitalized at the Gynecology Department of Ningbo Women and Children’s Hospital between May 2015 and April 2019 were retrospectively analyzed; 173 patients with complete follow-up data were included in this study. All patients were confirmed with type II and III CSP by three-dimensional B-mode ultrasound and/or pelvic enhanced MRI before surgery and met the diagnostic criteria for CSP [1]. Of the 173 patients, there were 109 with type II CSP. They were grouped based on the surgical strategy used: hysteroscopy and laparoscopy (group A1), hysteroscopy (group B1), and curettage (group C1). The surgical strategy for patients in group A1 included laparoscopic reversible ligation of the bilateral uterine arteries, removal of the pregnancy tissues of the uterine scar, repair of the uterine scar, and hysteroscopic exploration. In group B1, UAE and hysteroscopic removal of pregnancy tissues were used. For group C1, UAE and ultrasound-guided curettage were used. There were 64 patients with type III CSP. They were grouped according to the surgery they underwent: hysteroscopy and laparoscopy (group A2), hysteroscopy (group B2), and curettage (group C2). The surgical methods were the same as above. The selection of the surgical strategy was made after a comprehensive discussion between the patient and the surgeon about the surgical options and their pros and cons. The patient would then determine the surgical method they preferred and signed the surgery informed consent before the surgery, as per routine clinical practice. The study was approved by the Ethics Committee of Ningbo Women and Children’s Hospital. The informed consent was waived off due to the retrospective nature of the study. All patient data were kept confidential.
OUTCOME MEASURES AND FOLLOW-UP:
The surgical indicators and postoperative recovery among the 3 groups of patients with type II and III CSP were compared. The surgical indicators included intraoperative bleeding volume, hospital stay, and surgical complications. The intraoperative bleeding volume was calculated by using the volumetric method after the blood was collected by the aspirator. The conditions of postoperative recovery included the time of serum β-HCG returning to the normal, postoperative residual lesion, the thickness of the uterine scar, and the recovery time of menstruation. The serum β-HCG levels were detected every 2 days during hospitalization and, after discharge, at the outpatient clinic once a week until it returned to normal. Ultrasound was performed 1 week after discharge. If there were any residual lesions, reexamination was performed every week until it returned to normal. Ultrasound was performed 3 months after surgery to measure the thickness of the uterine scar.
STATISTICAL ANALYSIS:
SPSS 25.0 software (IBM, USA) was used for data analysis. The continuous data with a normal distribution were presented as means±standard deviations and compared using the independent-samples analysis of variance and the Bonferroni post hoc test. For continuous data that did not conform to the normal distribution were presented as median (P25–P75), and compared using the Kruskal-Wallis test. The categorical data were presented as n (%) and compared using the chi-square test. The significant level (α) was 0.05.
Results
COMPARISON OF THE GENERAL DATA OF THE PATIENTS:
There were no significant differences among the 3 groups in age, time from last menstruation, the average diameter of the gestational sac, and the number of cesarean sections (all P>0.05, Tables 1, 2).
There were no significant differences in age, time from last menstruation, the average diameter of the gestational sac, and number of cesarean sections among groups A1, B1, and C1 (H and chi-square value was 3.056, 1.882, 1.723, and 0.156, respectively, all P>0.05)
COMPARISON OF DIFFERENT SURGICAL INDICATORS OF TYPE II CSP PATIENTS:
The surgery was successfully completed in all patients with type II CSP without any surgical complications. Postoperative ultrasound in group A1 showed no significant residual lesions in the uterine isthmus. Eight patients with residual lesions in group B1 and 11 in group C1 were conservatively treated with success. Among patients with type II CSP, comparison between group A1 vs. groups B1 and C1 showed statistically significant differences (P<0.05) in terms of the postoperative time of serum β-HCG returning to the normal, residual lesion, thickness of the uterine scar, and recovery time of menstruation. There were no significant differences in intraoperative bleeding volume and postoperative hospital stay (P>0.05), as shown in Table 3. Compared with groups B1 and C1, and for group A1, the postoperative time of serum β-HCG returning to normal remained shorter, the residual lesions were reduced, the thickness of the scars was increased, and the recovery time of menstruation was shorter.
COMPARISON OF THE OUTCOME MEASURES WITH DIFFERENT SURGICAL METHODS IN PATIENTS WITH TYPE III CSP:
The surgery in all groups for type III CSP patients was completed successfully. Color Doppler ultrasound in group A2 showed no significant residual lesions in the uterine isthmus. There were 8 patients with residual lesions in group B2, among whom one patient underwent hysteroscopy and laparoscopy combined with the removal of pregnancy tissues of the uterine scar on day 14 after surgery due to the presence of residual lesions in the uterine scar, as revealed by postoperative color Doppler ultrasound and increased bleeding; the remaining 7 patients were successfully treated conservatively. There were 10 patients with residual lesions in group C2, among whom 2 underwent hysteroscopy and laparoscopy combined with the removal of the pregnancy tissues of uterine the scar on days 23 and 35 after surgery, respectively, due to the presence of residual lesions in the uterine scar, as revealed by postoperative color Doppler ultrasound and increased bleeding; the remaining 8 patients were successfully treated conservatively.
Among patients with type III CSP, comparison between group A2 vs. groups B2 and C2 showed statistically significant differences (P<0.05) in terms of the postoperative time of serum β-HCG returning to the normal, residual lesion, thickness of the uterine scar, and recovery time of menstruation. No significant differences were observed in intraoperative bleeding volume and postoperative hospital stay (P>0.05), as shown in Table 4. Compared with groups B2 and C2, the postoperative time of serum β-HCG returning to normal was shorter, the residual lesions were reduced, the thickness of the scars was increased, and the recovery time of menstruation was shorter in group A2.
Discussion
CSP is a special type of ectopic pregnancy that poses a great reproductive harm to women of childbearing age with a history of cesarean section. Although there is no consensus on the treatment of CSP, the basic therapeutic principles include early diagnosis, timely treatment, and bleeding reduction to preserve the fertility of the patients [10,12,17]. Currently, the pathogenesis of CSP remains unclear, but some studies suggested that CSP is related to uterine scar defects and the formation of microfissures due to the destruction of the endometrial basal layer after cesarean section [18–20]. The muscle layer in the CSP remains weak, and the thickness of the scar is <3 mm. The risk of CSP, massive hemorrhage, dangerous placenta previa, and uterine rupture can be increased during pregnancy, and laparoscopic surgery is a recommended treatment strategy to repair these uterine defects [21–23]. The muscular thickness of the scar in the anterior uterine wall of type II and III CSP is ≤3 mm in both types. In type II CSP, the gestational sac is partially implanted in the muscle layer of the uterine scar, and the local muscle layer is damaged. In type III CSP, the gestational sac is completely implanted into the muscle layer of the uterine scar and protrudes towards the bladder, and the damage it causes to the muscle layer is more serious. According to previous reports, patients with exogenous CSP a uterine scar thickness <3 mm and who undergo hysteroscopic surgery or curettage often suffer from uncontrollable bleeding, uterine perforation, and bladder injury during surgery, and the rate of secondary treatment after surgery is high, and the uterine scars might not be repaired [21,23,24]. The first-intention cure rate of exogenous CSP with hysteroscopic surgery alone is approximately 75% [15,25]. The main causes for treatment failure include increased intraoperative bleeding, conversion to transabdominal or laparoscopic surgery, postoperative residual lesions, a slow decrease in β-HCG levels, and slow absorption of local masses, among others. The present study suggests that for treating patients with type II and III CSP, hysteroscopy combined with laparoscopy were superior over hysteroscopy and curettage with respect to postoperative time of serum β-HCG returning to the normal, residual lesion, thickness of the uterine scar, and recovery time of menstruation.
For types II and III CSP, the muscular layer at the scar of the anterior uterine wall is thin, but the blood supply is rich, and they are at high risk of massive hemorrhage. Thus, pretreatment is often recommended before the curettage or removal of any pregnancy tissues in patients with type II and III CSP. UAE is often used as a pretreatment. The intraoperative local injection of methotrexate directly acts on the gestational sac, destroys the villous tissues, and prevents the development of the embryo. This is conducive to the subsequent curettage, thus lowering the risk of bleeding [14,16,26]. Nevertheless, postembolization syndrome, pelvic infection, damage to the ovarian function, or endometrial atrophy leading to amenorrhea, intrauterine adhesions, and infertility might occur, affecting the reproductive function of patients [27–29]. In addition, rare complications such as ureteral injury, bladder necrosis, lower limb necrosis, pulmonary embolism, and nerve injury have been reported [30]. In this study, the patients in group A (A1 and A2) underwent pretreatment with reversible ligation of the bilateral uterine arteries and showed no significant difference in intraoperative bleeding volume compared with the UAE groups. Therefore, ligation could avoid the UAE-related complications, with little effect on the uterine and ovarian blood supply.
Conclusions
This study strongly suggests that combined hysteroscopic and laparoscopic surgery and reversible ligation of the uterine artery can completely remove the pregnancy tissues, reduce or avoid the use of methotrexate, and repair the weak uterine scars. This is considered suitable for patients with CSP and subsequent fertility desire. Nevertheless, due to the limited sample size and unavailability of long-term follow-up data, further research with large sample size and long-term follow-up is warranted to explore the long-term clinical efficacy and reproductive outcomes of patients with treated type II and III CSP. In addition, hysteroscopic surgery combined with laparoscopic surgery requires high operation skills of surgeons, and increases the costs, limiting its clinical use. As a treatment option for CSP, hysteroscopic surgery combined with laparoscopic surgery and reversible ligation of the uterine artery will benefit patients with CSP by improving surgeons’ skills.
Tables
Table 1. Comparison of general data of patients with type II CSP.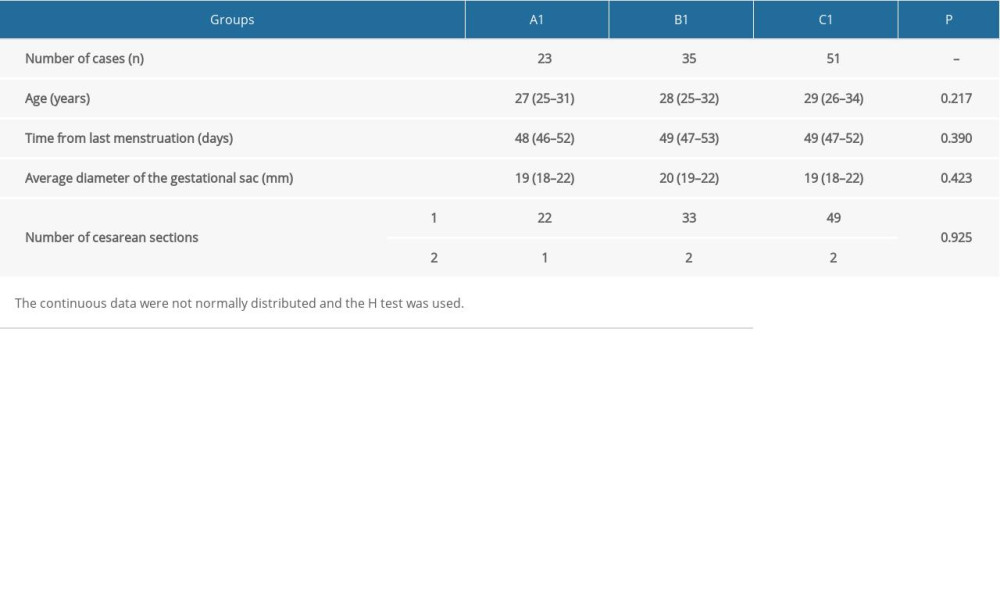 Table 2. Comparison of general data of patients with type III CSP.
Table 2. Comparison of general data of patients with type III CSP.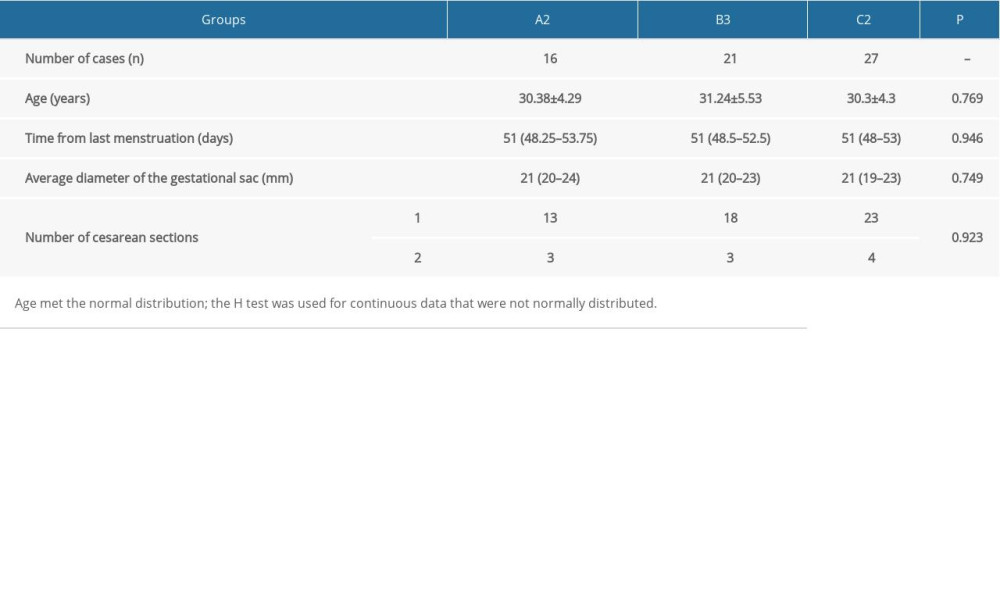 Table 3. Comparison of different surgical indicators for type II CSP patients.
Table 3. Comparison of different surgical indicators for type II CSP patients.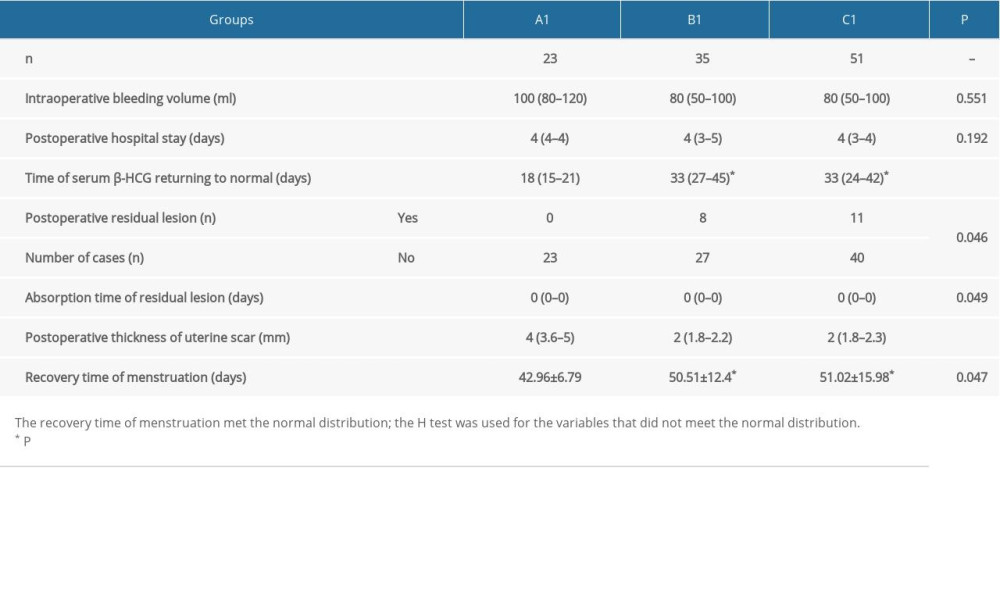 Table 4. Comparison of outcome measures with different surgical methods in patients with type III CSP.
Table 4. Comparison of outcome measures with different surgical methods in patients with type III CSP.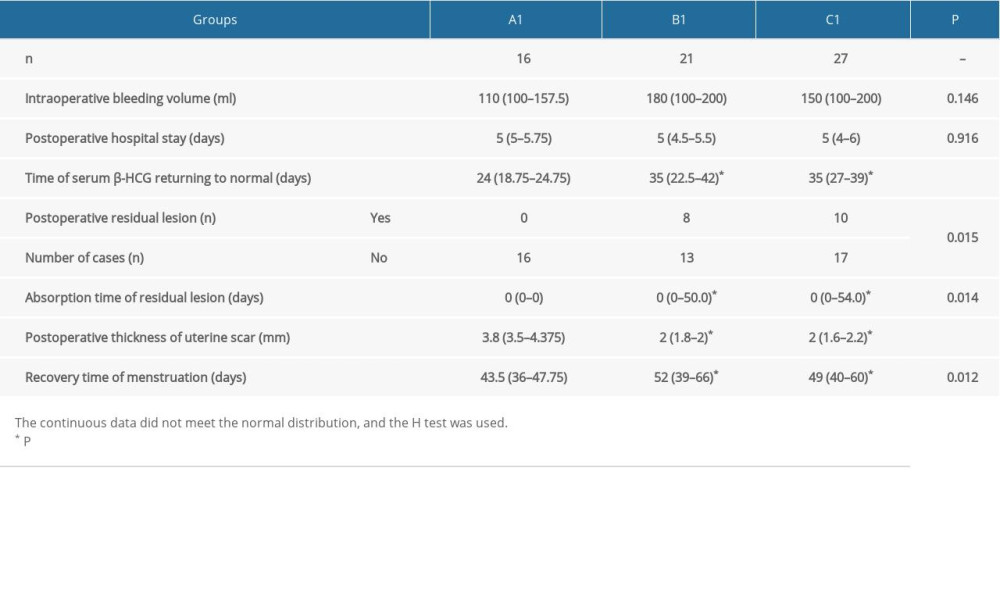
References
1. Expert opinion of diagnosis and treatment of cesarean scar pregnancy (2016): Zhonghua Fu Chan Ke Za Zhi, 2016; 51; 568-72
2. Jurkovic D, Hillaby K, Woelfer B, First-trimester diagnosis and management of pregnancies implanted into the lower uterine segment Cesarean section scar: Ultrasound Obstet Gynecol, 2003; 21; 220-27
3. Ash A, Smith A, Maxwell D, Caesarean scar pregnancy: BJOG, 2007; 114; 253-63
4. Gonzalez N, Tulandi T, Cesarean scar pregnancy: A systematic review: J Minim Invasive Gynecol, 2017; 24; 731-38
5. Kanat-Pektas M, Bodur S, Dundar O, Bakir VL, Systematic review: What is the best first-line approach for cesarean section ectopic pregnancy?: Taiwan J Obstet Gynecol, 2016; 55; 263-69
6. Osborn DA, Williams TR, Craig BM, Cesarean scar pregnancy: Sonographic and magnetic resonance imaging findings, complications, and treatment: J Ultrasound Med, 2012; 31; 1449-56
7. Wu R, Klein MA, Mahboob S, Magnetic resonance imaging as an adjunct to ultrasound in evaluating cesarean scar ectopic pregnancy: J Clin Imaging Sci, 2013; 3; 16
8. Kong D, Dong X, Qi Y, Ultrasonography-guided multidrug stratification interventional therapy for cesarean scar pregnancy: Arch Gynecol Obstet, 2015; 292; 143-48
9. Yuan Y, Dai Q, Cai S, Diagnostic value of ultrasound in cesarean scar pregnancy: Chin J Ultrasonogr, 2010; 19; 321-24
10. Birch Petersen K, Hoffmann E, Rifbjerg Larsen C, Svarre Nielsen H, Cesarean scar pregnancy: A systematic review of treatment studies: Fertil Steril, 2016; 105; 958-67
11. Grechukhina O, Deshmukh U, Fan L, Cesarean scar pregnancy, incidence, and recurrence: Five-year experience at a single tertiary care referral center: Obstet Gynecol, 2018; 132; 1285-95
12. Maheux-Lacroix S, Li F, Bujold E, Cesarean scar pregnancies: A systematic review of treatment options: J Minim Invasive Gynecol, 2017; 24; 915-25
13. Le A, Shan L, Xiao T, Transvaginal surgical treatment of cesarean scar ectopic pregnancy: Arch Gynecol Obstet, 2013; 287; 791-96
14. Qian ZD, Huang LL, Zhu XM, Curettage or operative hysteroscopy in the treatment of cesarean scar pregnancy: Arch Gynecol Obstet, 2015; 292; 1055-61
15. Wang G, Liu X, Wang D, Yang QClinical analysis on selective uterine artery embolization combined with hysteroscopic surgery for exogenous cesarean scar pregnancy in 67 cases: Zhonghua Fu Chan Ke Za Zhi, 2015; 50; 576-81
16. Jurkovic D, Knez J, Appiah A, Surgical treatment of Cesarean scar ectopic pregnancy: Efficacy and safety of ultrasound-guided suction curettage: Ultrasound Obstet Gynecol, 2016; 47; 511-17
17. Zhang Y, Gu Y, Wang JM, Li Y, Analysis of cases with cesarean scar pregnancy: J Obstet Gynaecol Res, 2013; 39; 195-202
18. Roberge S, Boutin A, Chaillet N, Systematic review of cesarean scar assessment in the nonpregnant state: Imaging techniques and uterine scar defect: Am J Perinatol, 2012; 29; 465-71
19. Malvasi A, Cavallotti C, Gustapane S, Neurotransmitters and neuropeptides expression in the uterine scar after cesarean section: Curr Protein Pept Sci, 2017; 18; 175-80
20. Timor-Tritsch IE, Monteagudo A, Cali G, Cesarean scar pregnancy and early placenta accreta share common histology: Ultrasound Obstet Gynecol, 2014; 43; 383-95
21. Marotta ML, Donnez J, Squifflet J, Laparoscopic repair of post-cesarean section uterine scar defects diagnosed in nonpregnant women: J Minim Invasive Gynecol, 2013; 20; 386-91
22. Donnez O, Donnez J, Orellana R, Dolmans MM, Gynecological and obstetrical outcomes after laparoscopic repair of a cesarean scar defect in a series of 38 women: Fertil Steril, 2017; 107; 289-96.e2
23. He Y, Wu X, Zhu Q: BMC Womens Health, 2014; 14; 116
24. Wang G, Liu X, Bi F, Evaluation of the efficacy of laparoscopic resection for the management of exogenous cesarean scar pregnancy: Fertil Steril, 2014; 101; 1501-7
25. Yang Q, Piao S, Wang G, Hysteroscopic surgery of ectopic pregnancy in the cesarean section scar: J Minim Invasive Gynecol, 2009; 16; 432-36
26. Cok T, Kalayci H, Ozdemir H, Transvaginal ultrasound-guided local methotrexate administration as the first-line treatment for cesarean scar pregnancy: Follow-up of 18 cases: J Obstet Gynaecol Res, 2015; 41; 803-8
27. Kim CW, Shim HS, Jang H, Song YG, The effects of uterine artery embolization on ovarian reserve: Eur J Obstet Gynecol Reprod Biol, 2016; 206; 172-76
28. Karlsen K, Hrobjartsson A, Korsholm M, Fertility after uterine artery embolization of fibroids: A systematic review: Arch Gynecol Obstet, 2018; 297; 13-25
29. Cao GS, Liu RQ, Liu YY, Menstruation recovery in scar pregnancy patients undergoing UAE and curettage and its influencing factors: Medicine (Baltimore), 2018; 97; e9584
30. Alyeshmerni D, Banovac F, Pehlivanova M, Resolution of hydronephrosis after uterine artery embolization for fibroids: J Vasc Interv Radiol, 2011; 22; 865-69
Tables
Table 1. Comparison of general data of patients with type II CSP.Table 2. Comparison of general data of patients with type III CSP.Table 3. Comparison of different surgical indicators for type II CSP patients.Table 4. Comparison of outcome measures with different surgical methods in patients with type III CSP. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387