17 August 2020: Clinical Research
Correlation Between Parameters of Intervertebral Disc and Cervical Lordosis in Cervical Spondylotic Myelopathy
Zhuxi Huang12BCDE, Yue Zhu1AG, Wei Yuan1ACE*DOI: 10.12659/MSM.924857
Med Sci Monit 2020; 26:e924857






Abstract
BACKGROUND: In cervical disc degeneration, cervical disc height (CDH) and cervical disc angle (CDA)have a certain but unidentified relationship with cervical lordosis (CL). This study aimed to reveal the relationship among CDH, CDA, and CL in patients diagnosed with cervical spondylotic myelopathy (CSM).
MATERIAL AND METHODS: A retrospective analysis was conducted using the data of 212 CSM patients (136 males and 76 females). According to CL angle, patients were classified into 2 groups: patients with CL ≤10° constituted Group 1 (n=102); patients with CL >10° constituted Group 2 (n=110). The CDH, CDA, and CL were measured using X-ray imaging. Pearson correlation analysis measured the correlation between CDH, CDA, and CL. Multiple linear regression was utilized to analyze the effects of CDH and CDA on CL.
RESULTS: The CDAs in every level were higher in Group 2 than those in Group 1 (P<0.05).CDH and CDA gradually increased with the increase in vertebral level and dropped at C5–C6 level in both groups. We found statistically significant correlations between C3/4H, C4/5H, C3/4A,C4/5A, C5/6A, and C6/7Aand CL in Group 1 (P<0.05), and between C4/5H, C3/4A, and C4/5Aand CL in Group 2 (P<0.05). C3/4A and C4/5A predicted CL in Group 1 (adjusted R²=0.176, P<0.001), while C4/5A predicted CL with high sensitivity in Group 2 (adjusted R²=0.198, P<0.001).
CONCLUSIONS: CDA contributes more than CDH to CL in CSM. Further studies are necessary to reveal the relationship between CL and cervical disc degeneration.
Keywords: Cervical Vertebrae, intervertebral disc degeneration, Lordosis, spondylosis, intervertebral disc, X-Rays
Background
Cervical spondylotic myelopathy (CSM) is a common type of cervical degenerative disease, and disc degeneration is the initial event in spondylotic changes, which can cause abnormalities in cervical spine biomechanics and changes in cervical sagittal parameters [1–3]. Also, the loss of cervical sagittal alignment may be associated with pain and neurological disorders via a number of mechanisms, such as compression, repeated flexion/extension injury, and vascular compromise [4,5]. Several studies have revealed that cervical sagittal parameters, including cervical lordosis (CL), C2–C7 sagittal vertical axis, T1 slope, neck tilt, and thoracic inlet angle, correlate to each other in certain ways, and some of these parameters could predict the severity of myelopathy in CSM [1,6]. Due to the degeneration of the cervical disc in CSM, CL could theoretically decrease with narrowed cervical disc height (CDH) and cervical disc angle (CDA), but this relationship has not been fully elucidated. This study aims to reveal the relationship among CDH, CDA, and CL, and to explore which parameter contributes more to CL in CSM.
Material and Methods
PATIENT POPULATION:
Our retrospective study included 212 patients with CSM (136 males and 76 females) with an average age of 54.5±10 years that received surgical interventions in our department between January 2014 and August 2016. The patients were at a later stage of CSM and presented more featured radiological results compared to patients requiring no surgical interventions. The patients were divided into 2 groups according to CL angle: patients with CL ≤10°were placed in Group 1 (n=102), while those with CL >10° were placed in Group 2(n=110). All participants had a cervical spine X-ray examination performed prior to undergoing surgical treatment. Patients with a history of cervical spine surgery, cervical spine trauma, congenital cervical abnormality, and hip or knee surgery were excluded from this study. The study was approved by the hospital’s institutional review board (No: 20182542). Written informed consent was obtained from all the participants in the study.
IMAGING DATA COLLECTION:
Patient imaging data from a lateral X-ray examination included the C2–C7 cobb angle as well as the cervical disc height (CDH) and cervical disc angle (CDA) at 5different levels: C2/3, C3/C4, C4/C5, C5/C6, and C6/C7. The C2–C7 cobb angle was the angle formed by the lower endplate of C2 and the lower endplate of C7, representing CL (Figure 1A). CL was defined as positive and cervical kyphosis was defined as negative. The cervical disc anterior height (CDAH) was defined as the distance between the anterior points of the endplates, while the cervical disc middle height (CDMH)was defined as the distance between the middle points of the endplates. Furthermore, the cervical disc posterior height (CDPH) was defined as the distance between the posterior points of the endplates. The following formula was used to calculate the CDH: (CDAH+CDMH+CDPH)/3 (Figure 1B). The CDA was defined as the angle formed by the endplates of the upper and lower vertebrae (Figure 1C). Surgimap (Version 2.2.13.1) was used as the measurement tool, and 2 independent spine surgeons with extensive experience in radiograph measurement techniques performed the measurements twice. The mean values of the measurements were used in the analysis.
STATISTICAL ANALYSIS:
The statistical analysis was performed using SPSS 20.0 (SPSS, Chicago, IL, USA). Quantitative data was denoted as mean±standard deviation, and correlation analysis was conducted with Pearson’s correlation coefficient to measure the correlation between the variables (CL, CDH, and CDA). Linear regression analysis was applied to identify the parameters that could predict CL. Values of
Results
The CL, CDH, and CDA for both groups are shown in Table 1. The results indicated that there was a statistical difference in CL between the 2 groups (
Regarding the correlations between the parameters, we observed a notable correlation between CL and several variables (Table 2, Figure 4) in Group 1: C3/4H (r=0.25,
Multiple linear regression was used to model the relationship between CL and C3/4H, C4/5H, C3/4A, C4/5A, C5/6A, and C6/7A in Group 1 and CL and C4/5H, C3/4A, and C4/5A in Group 2. Other parameters that correlated with each other were excluded to avoid multicollinearity. The results showed that C3/4A and C4/5A predicted CL in Group 1 (adjusted R2=0.176,
Discussion
By analyzing the contribution of each cervical disc to the formation of CL, we observed that the CDA is more important than the CDH, and the angle of C3/4 and C4/5predicted CL when CL ≤10°, while the angle of C4/5 predicted CL when CL >10°.
The maintenance of a normal CL is dependent on the muscles, ligaments, and elasticity of the cervical disc. Hence, CL is one of the important indicators of the general function of the cervical spine. Abnormal CL is an indicator in patients with CSM and can be easily identified in a lateral X-ray image of the cervical spine. Studies have demonstrated that patients with severe CSM or neck pain showed obvious CL abnormalities [7,8]. Such abnormalities change the cervical biomechanics, increasing its load and accelerating degenerative changes [9]. Overall, we believe that patients with CSM first experience change in the disc before CL occurs [2,10].
Although several methods to measure CL exist, the C2–C7 cobb angle method has been proven to show a relatively high interobserver reliability, and is thus one of the most common methods for clinical measurement of CL [1,11,12]. While there is currently no clear definition of a disc angle, it is worth noting that the sum of the 5 CDAs does not equal the C2–C7 cobb angle because the upper and lower endplates of each vertebrae are not exactly parallel. In other words, each vertebra is wedge-shaped and has a certain vertebral angle [13].
To evaluate the vertebral levels that are most likely to cause CSM, Pan et al. [14] analyzed the MRIs of 539 patients with CSM. Changes in the cervical cartilage endplate, called “modic change,” were visualized using MRI and used as an indicator of cervical degeneration. The results revealed that the largest modic change occurred at the C5/6 level disc. In the present study, the height of the C5/6level disc decreased significantly when CL <10°, indicating tha tC5/6 level disc degeneration is most common in patients with CSM. Hussain et al. [15] used a finite element model for biomechanical analysis and reported a reduction in the range of motion activity in the C5/6 segment; thus, the disc degeneration at this level was most pronounced, which is in line with our results.
In our study, the Pearson correlation coefficients of the CDA at the C3/4 and C4/5 levels were larger than those of the other variables, indicating that the C3/4 and C4/5 level CDAs make the greatest contribution to CL. Similarly, Mashasi et al. [16] used MRI to study the cervical spines of 201 patients with neck pain and found that when CL was relatively mild, level C2/3 and C3/4 CDAs could largely influence the changes in CL, whereas level C4/5, C5/6, and C6/7 CDAs largely affected CL when it was normal. Based on these results, we speculate that due to the degeneration at the C5/6 level, the CDH and the CDA decreased; thus, maintaining a relatively normal CL requires a compensatory increase in the elasticity of the adjacent C5/6 disc [17]. In the cervical spine, greater mobility is observed at the C3/4 and C4/5 levels [18],and for patients with a prolonged course of disease, the C4/5 and C3/4 levels have poor elasticity causing the discs to collapse, which in turn leads to degeneration. The results of grouped linear regression performed in our study revealed that among CSM patients with more severe CL, the CDAs at the C3/4 and C4/5 levels contributed notably to CL, while among CSM patients with less severe CL, the CDA of the C4/5 level contributed more notably to CL.
Katsuura et al. [19] retrospectively analyzed patients who underwent anterior cervical surgery and reported that there was a notable correlation between degeneration of the adjacent disc and a decrease in CL. We therefore speculate that if the C5/6 level were used as the target for surgery and CL was less than 10 degrees, there would be a larger probability of degenerative changes occurring at the C4/5 level after surgery. Furthermore, if the CL of the patient in the preoperative period was greater than 10 degrees, the probability of degenerative changes occurring at the C3/4 level would increase. Nonetheless, our study did not find a specific relationship between the CDH and CL.
There were a number of limitations in the current study. First, the study lacked a normal population control group. Second, the design of the current study did not include sagittal parameters of the cervical spine, thoracolumbar spine, and pelvis. Finally, due to the nature of retrospective studies, the measurements performed were based on imaging results, which could have led to bias. A further prospective study is necessary.
Conclusions
The current study showed that the CDA contributes more than CDH to CL inpatients with CSM. Although these results present a clear correlation between disc angle and CL, further research is needed to explore the relationship among disc angle, height, and disc degeneration.
Figures
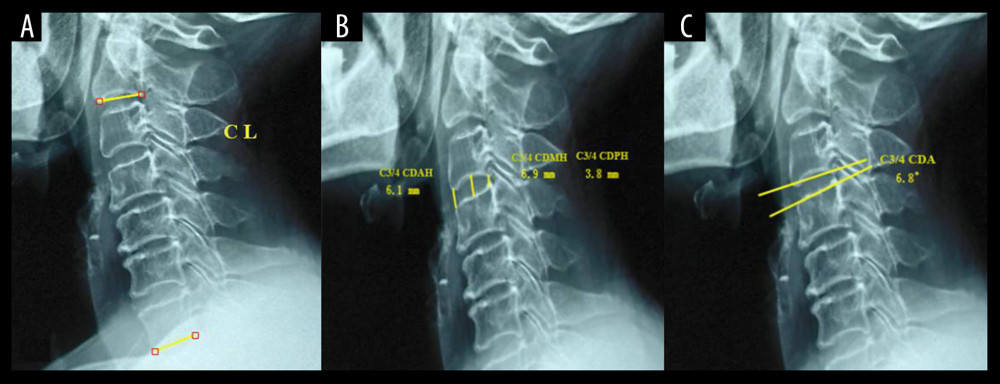 Figure 1. The CL, CDH, and CDA measurement methods in lateral X-ray images. (A) CL was defined as the angle formed by the lower endplates of C2 and C7, with lordosis defined as positive and kyphosis defined as negative. (B) CDAH was defined as the distance between the anterior point of the endplates, CDMH was defined as the distance between the middle point of endplates, and CDPH was defined as the distance between the posterior point of endplates, while CDH=(CDAH+CDMH+CDPH)/3. (C) The CDA was defined as the angle formed by the endplates of the upper and lower vertebrae.
Figure 1. The CL, CDH, and CDA measurement methods in lateral X-ray images. (A) CL was defined as the angle formed by the lower endplates of C2 and C7, with lordosis defined as positive and kyphosis defined as negative. (B) CDAH was defined as the distance between the anterior point of the endplates, CDMH was defined as the distance between the middle point of endplates, and CDPH was defined as the distance between the posterior point of endplates, while CDH=(CDAH+CDMH+CDPH)/3. (C) The CDA was defined as the angle formed by the endplates of the upper and lower vertebrae. 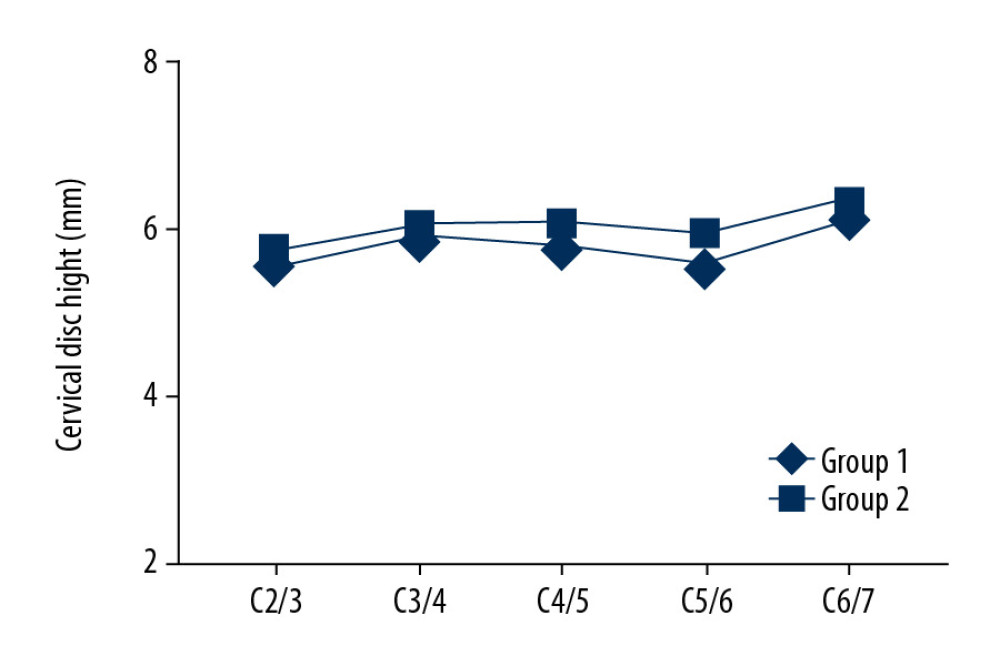 Figure 2. The CDH of each disc in the 2 groups. There is no statistical difference between the2 groups.
Figure 2. The CDH of each disc in the 2 groups. There is no statistical difference between the2 groups. 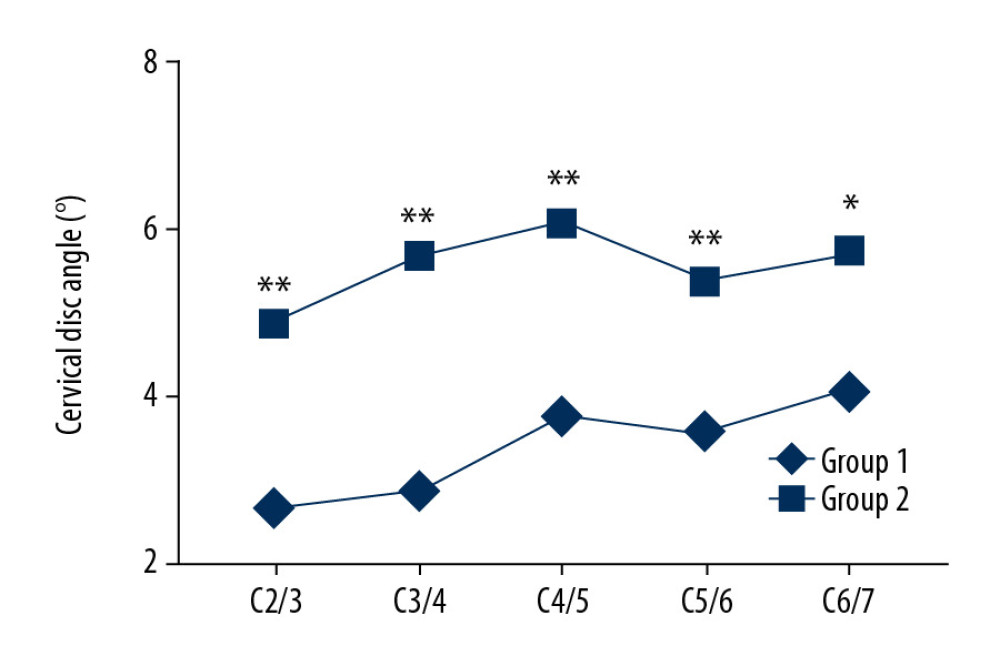 Figure 3. The CDA of each disc in the 2 groups. The CDA of all levels in Group 1 were significantly higher than those in Group 2.
Figure 3. The CDA of each disc in the 2 groups. The CDA of all levels in Group 1 were significantly higher than those in Group 2. 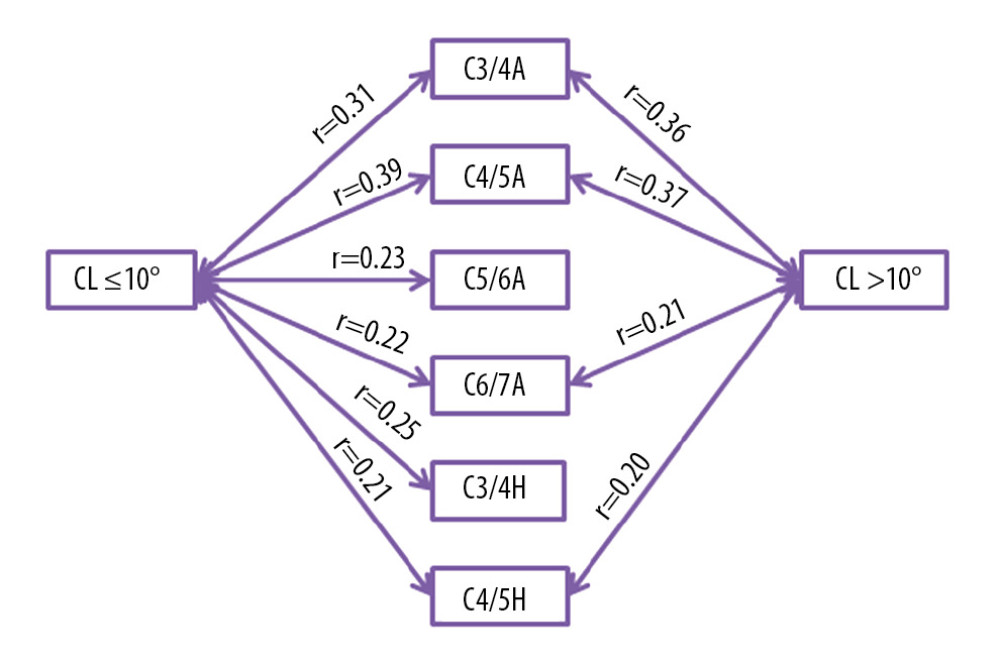 Figure 4. Correlation among CDA, CDH and CL.
Figure 4. Correlation among CDA, CDH and CL. References
1. Yuan W, Zhu Y, Zhu H, Preoperative cervical sagittal alignment parameters and their impacts on myelopathy in patients with cervical spondylotic myelopathy: A retrospective study: Peer J, 2017; 5; e4027
2. Smith JS, Lafage V, Ryan DJ, Association of myelopathy scores with cervical sagittal balance and normalized spinal cord volume: analysis of 56 preoperative cases from the AOSpine North America Myelopathy study: Spine (Phila Pa 1976), 2013; 38(22 Suppl 1); S161-70
3. Gore DR, Sepic SB, Gardner GM, Roentgenographic findings of the cervical spine in asymptomatic people: Spine (Phila Pa 1976), 1986; 11(6); 521-24
4. Tang JA, Scheer JK, Smith JS, The impact of standing regional cervical sagittal alignment on outcomes in posterior cervical fusion surgery: Neurosurgery, 2015; 76(Suppl 1); S14-21 discussion S21
5. Ames CP, Blondel B, Scheer JK, Cervical radiographical alignment: comprehensive assessment techniques and potential importance in cervical myelopathy: Spine (Phila Pa 1976), 2013; 38(22 Suppl 1); S149-60
6. Yang M, Yang C, Ni H, The relationship between T1 sagittal angle and sagittal balance: A retrospective study of 119 healthy volunteers: PLoS One, 2016; 11(8); e0160957
7. Yoshida G, Alzakri A, Pointillart V, Global spinal alignment in patients with cervical spondylotic myelopathy: Spine (Phila Pa 1976), 2018; 43(3); E154-62
8. Grob D, Frauenfelder H, Mannion AF, The association between cervical spine curvature and neck pain: Eur Spine J, 2007; 16(5); 669-78
9. Mohanty C, Massicotte EM, Fehlings MG, Shamji MF, Association of preoperative cervical spine alignment with spinal cord magnetic resonance imaging hyperintensity and myelopathy severity: Analysis of a series of 124 cases: Spine (Phila Pa 1976), 2015; 40(1); 11-16
10. Ferrara LA, The biomechanics of cervical spondylosis: Adv Orthop, 2012; 2012 493605
11. Vidal C, Ilharreborde B, Azoulay R, Reliability of cervical lordosis and global sagittal spinal balance measurements in adolescent idiopathic scoliosis: Eur Spine J, 2013; 22(6); 1362-67
12. Scheer JK, Tang JA, Smith JS, Cervical spine alignment, sagittal deformity, and clinical implications: A review: J Neurosurg Spine, 2013; 19(2); 141-59
13. Suh BG, Ahn MW, Kim HJ, Wedge-shaped resection of the posterior bony arch during open door laminoplasty to prevent postoperative motion limitation: Spine (Phila Pa 1976), 2017; 42(3); 143-50
14. Qiao P, Xu TT, Zhang W, Tian R, Modic changes in the cervical endplate of patients suffering from cervical spondylotic myelopathy: J Orthop Surg Res, 2018; 13(1); 90
15. Hussain M, Natarajan RN, An HS, Andersson GB, Motion changes in adjacent segments due to moderate and severe degeneration in C5-C6 disc: A poroelastic C3-T1 finite element model study: Spine (Phila Pa 1976), 2010; 35(9); 939-47
16. Miyazaki M, Hymanson HJ, Morishita Y, Kinematic analysis of the relationship between sagittal alignment and disc degeneration in the cervical spine: Spine (Phila Pa 1976), 2008; 33(23); E870-76
17. Yu J, Ha Y, Shin JJ, Influence of plate fixation on cervical height and alignment after one- or two-level anterior cervical discectomy and fusion: Br J Neurosurg, 2018; 32(2); 188-95
18. Yuan W, Zhang H, Zhou X, The influence of artificial cervical disc prosthesis height on the cervical biomechanics: A finite element study: World Neurosurg, 2018; 113; e490-98
19. Katsuura A, Hukuda S, Saruhashi Y, Mori K, Kyphotic malalignment after anterior cervical fusion is one of the factors promoting the degenerative process in adjacent intervertebral levels: Eur Spine J, 2001; 10(4); 320-24
Figures
Figure 1. The CL, CDH, and CDA measurement methods in lateral X-ray images. (A) CL was defined as the angle formed by the lower endplates of C2 and C7, with lordosis defined as positive and kyphosis defined as negative. (B) CDAH was defined as the distance between the anterior point of the endplates, CDMH was defined as the distance between the middle point of endplates, and CDPH was defined as the distance between the posterior point of endplates, while CDH=(CDAH+CDMH+CDPH)/3. (C) The CDA was defined as the angle formed by the endplates of the upper and lower vertebrae.Figure 2. The CDH of each disc in the 2 groups. There is no statistical difference between the2 groups.Figure 3. The CDA of each disc in the 2 groups. The CDA of all levels in Group 1 were significantly higher than those in Group 2.Figure 4. Correlation among CDA, CDH and CL. Tables
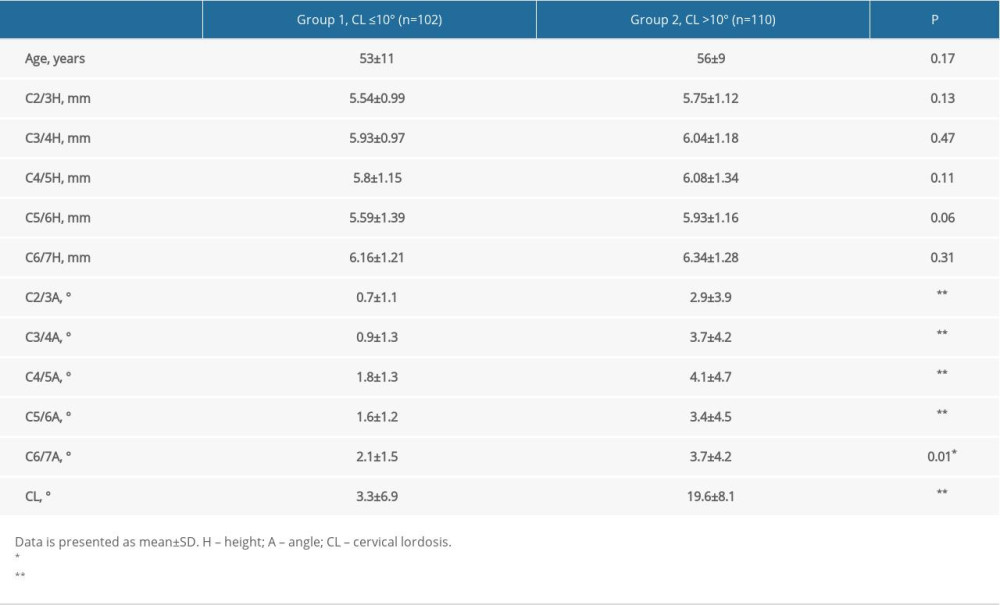 Table 1. Age, cervical disc height, angle, and cervical lordosis in 2 groups.
Table 1. Age, cervical disc height, angle, and cervical lordosis in 2 groups.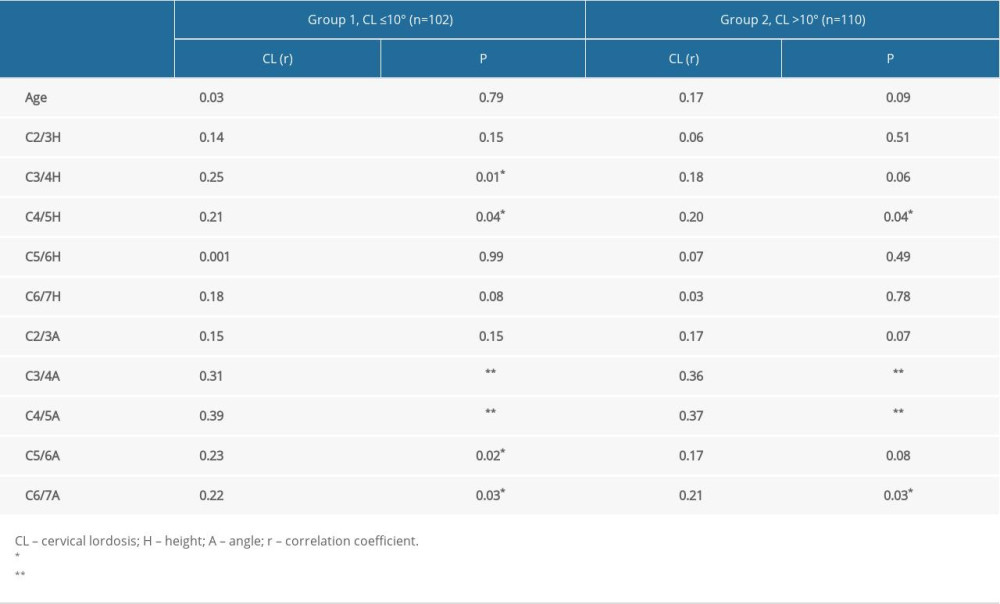 Table 2. Correlations of the age, cervical disc height and angle with cervical lordosis in 2 groups.Table 1. Age, cervical disc height, angle, and cervical lordosis in 2 groups.Table 2. Correlations of the age, cervical disc height and angle with cervical lordosis in 2 groups.
Table 2. Correlations of the age, cervical disc height and angle with cervical lordosis in 2 groups.Table 1. Age, cervical disc height, angle, and cervical lordosis in 2 groups.Table 2. Correlations of the age, cervical disc height and angle with cervical lordosis in 2 groups. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387