19 September 2020: Clinical Research
Risk Factor Analysis and Risk Prediction Model Construction of Pressure Injury in Critically Ill Patients with Cancer: A Retrospective Cohort Study in China
Zhong-Wen Sun1ADG*, Min-Ru Guo1BCE, Li-Zi Yang1DEF, Ze-Jun Chen1BCEF, Zhu-Qing Zhang1FDOI: 10.12659/MSM.926669
Med Sci Monit 2020; 26:e926669






Abstract
BACKGROUND: The aim of this study was to analyze the risk factors of pressure injury (PI) in critically ill patients with cancer to build a risk prediction model for PI.
MATERIAL AND METHODS: Between January 2018 and December 2019, a total of 486 critically ill patients with cancer were enrolled in the study. Univariate analysis and binary logistic regression analysis were used to explore risk factors. Then, a risk prediction equation was constructed and a receiver operator characteristic (ROC) curve analysis model was used for prediction.
RESULTS: Of the 486 critically ill patients with cancer, 15 patients developed PI. Risk factors found to have a significant impact on PI in critically ill patients with cancer included the APACHE II score (P<0.001), semi-reclining position (P=0.006), humid environment/moist skin (P<0.001), and edema (P<0.001). These 4 independent risk factors were used in the regression equation, and the risk prediction equation was constructed as Z=0.112×APACHE II score +2.549×semi-reclining position +2.757×moist skin +1.795×edema–9.086. From the ROC curve analysis, the area under the curve (AUC) was 0.938, sensitivity was 100.00%, specificity was 83.40%, and Youden index was 0.834.
CONCLUSIONS: The PI risk prediction model developed in this study has a high predictive value and provides a basis for PI prevention and treatment measures for critically ill patients with cancer.
Keywords: Critical Illness, Pressure Ulcer, Risk Factors, Models, Biological, Neoplasms, Risk Assessment
Background
Pressure injury (PI), refers to skin or subcutaneous tissue damage caused by violent impact, long-term pressure, or pressure combined with shear force [1]. The clinical manifestation of PI can be intact skin or open injury. PIs not only further aggravate a clinical condition and prolong treatment time, but they can also easily lead to infection, threatening patient safety [2,3]. Among the types of PIs, hospital-acquired pressure injury (HAPI) is regarded as an important indicator that reflects patient quality of care; HAPI can be prevented to a large extent, mainly with stage II PI. However, due to critical illness and other select situations, the probability of PI occurrence in the hospital Intensive Care Unit (ICU) is 3.8 times higher than that in patients in general wards [4]. A meta-analysis of 10 retrospective survey studies showed that the cumulative incidence of PI in critically ill patients in ICU is 10.00% to 25.90% [5]. According to the literature, HAPI not only causes serious harm to the physical and mental health of patients, it also creates an economic burden to society. In the US alone, the medical expenditure from PI reached $26.8 billion in 2016 [6]. Similarly, PI medical expenditure accounted for 1.9% of total expenditures in public hospitals in Australia in 2012 and 2013 [7]. Anticancer therapy includes various methods such as surgery, radiotherapy, chemotherapy, and targeted therapy. It is well known that skin damage could be present in cancer patients receiving chemotherapy and antineoplastic radiotherapy [8,9]. The treatment methods for critically ill patients with cancer are complex and diverse. Therefore, the risk of PI in critically ill patients with cancer is higher than in patients without cancer. According to observational research reports of dying patients, cancer history was associated with the occurrence of PI at the end of life [10]. However, 76% of patients with cancer had PI during hospitalization [11]. Longitudinal study results of the PI incidence rate of patients in oncological ICU showed that the incidence rate per 100 patient-days is 1.32%, and the cumulative incidence rate is 29.5%; moreover, it showed that the incidence of PI is higher in critically ill patients with cancer who had at least 1 episode of diarrhea, received enteral nutrition, and took vasoactive or sedative drugs for an extended period of time [12]. At present, PI risk prediction is mainly evaluated by the Waterlow PI risk assessment form and Braden scale for PI risk, but the evaluation content of these assessments is limited, and nursing practice data showed that the results of these assessments need to be combined with an overall evaluation of clinical data to provide more accurate risk prediction [13,14]. The aims of this study are to analyze PI risk factors and build a risk prediction model for critically ill patients with cancer to help clinical nurses screen high-risk populations of PI and carry out relevant care and intervention at an early stage.
Material and Methods
STUDY PARTICIPANTS:
A total of 486 critically ill patients with cancer admitted to the ICU of Sun Yat-Sen University Cancer Center in Guangzhou, China, from January 2018 to December 2019 were selected as the study participants, and the clinical data of all the participants were retrospectively analyzed. The participants included in the study met the following inclusion criteria: (1) age ≥18 years; (2) ICU hospital stay ≥24 h; and (3) patient diagnosed with cancer by pathological biopsy; and exclusion criteria: (1) existing PI at admission to the ICU; (2) patient had skin disease at the same time; and (3) clinical data was incomplete.
STUDY DESIGN AND SETTING:
This study was approved by the Sun Yat-sen University Cancer Center IRB (Approval No. B2020-167-01). The clinical data from January 2018 to December 2019 were collected from the patients’ medical records for retrospective analysis using a self-designed Microsoft Excel spreadsheet. Because of the retrospective data collection procedure, the ethics committee did not deem it necessary for patient consent to be obtained from the study participants. Duly trained intensivist nurses collected the following clinical data from the patients’ medical records: (1) general patient information: age and sex; (2) disease information: diagnosis of cancer complications, history of anticancer therapy, acute physiology and chronic health evaluation (APACHE II) score, Waterlow score, laboratory test results; (3) treatment situation: use of mechanical ventilation, blood purification treatment, medications taken, and length of ICU hospital stay; (4) skin situation: skin abnormality and PI occurrence.
PI, diarrhea, and recurrent fever were evaluated by the ostomy therapist and intensivist nurses as follows: (1) PI was characterized according to the definition and staging of PI issued by the National Pressure Ulcer Advisory Panel (NPUAP) in 2016 [15]. Only PIs with stage II and above were included in this study, including stages II, III, IV, non-staging, and suspected deep tissue damage; (2) diarrhea was determined when the number of stools per day exceeded 3 times, with trait changes [16]; (3) recurrent fever was determined according to previous reports and defined as an abnormal increase in body temperature resulting in higher than 38°C that occurred 3 or more times during the stay in the ICU [17,18]. For each patient, the APACHE II score was calculated within 24 h of admission from patient age and 12 routine physiological measurements: PaO2, temperature (rectal), mean arterial pressure, arterial pH, heart rate, respiratory rate, Glasgow Coma Scale, and serum sodium, serum potassium, creatinine, hematocrit, and white blood cell levels. The Waterlow score was calculated by weight for height, skin type, sex, age, continence, mobility, appetite, and a malnutrition screening tool. Critically ill patients with cancer were divided into 2 groups according to whether or not PI occurred, and the age, sex, complications, history of anticancer therapy, APACHE II score, Waterlow score, laboratory test results (hemoglobin), the presence or absence of mechanical ventilation, blood purification treatment, medications, and ICU hospitalization were compared between the 2 groups for statistical differences.
STATISTICAL ANALYSIS:
SPSS version 22.0 was used for statistical analysis. For continuous variables, we described the data as means and standard deviations, and for categorical variables, as number of cases and percentages. The independent
Results
PREVALENCE OF PI IN CRITICALLY ILL PATIENTS WITH CANCER:
Among the 486 critically ill patients with cancer enrolled in this study, 15 patients had stage II PI or above. The cumulative incidence rate was 3.09%, the patient-day incidence rate was 3.14%, and the occurrence time range was 3 to 50 days after ICU admission, with PI occurring in 8 cases in the ICU between day 5 and day 20. Table 1 shows the specific locations and stages of PI occurrence. One patient with unstageable PI presented as stage III with removing slough.
UNIVARIATE ANALYSIS OF PI IN CRITICALLY ILL PATIENTS WITH CANCER:
Results of the analysis showed statistically significant differences in APACHE II scores (P<0.001), shock (P=0.030), semi-reclining position (P=0.006), enteral nutrition (P=0.010), sedative drugs (P=0.034), vasoactive drugs (P=0.026), recurrent fever (P=0.033), diarrhea (P<0.001), moist skin (P<0.001), and edema (P<0.001) between the 2 groups. The detailed results are shown in Table 2.
MULTI-FACTOR ANALYSIS OF PI IN CRITICALLY ILL PATIENTS WITH CANCER AND CONSTRUCTION OF THE RISK PREDICTION EQUATION:
The independent variables are shown in Table 3, and the results of the logistic regression analysis are shown in Table 4. The risk prediction equation was Z=0.112×APACHE II score +2.549×semi-reclining position +2.757×moist skin +1.795×edema–9.086. The goodness-of-fit Nagelkerke R-square value was 0.469.
PI RISK PREDICTION EQUATION VERIFICATION:
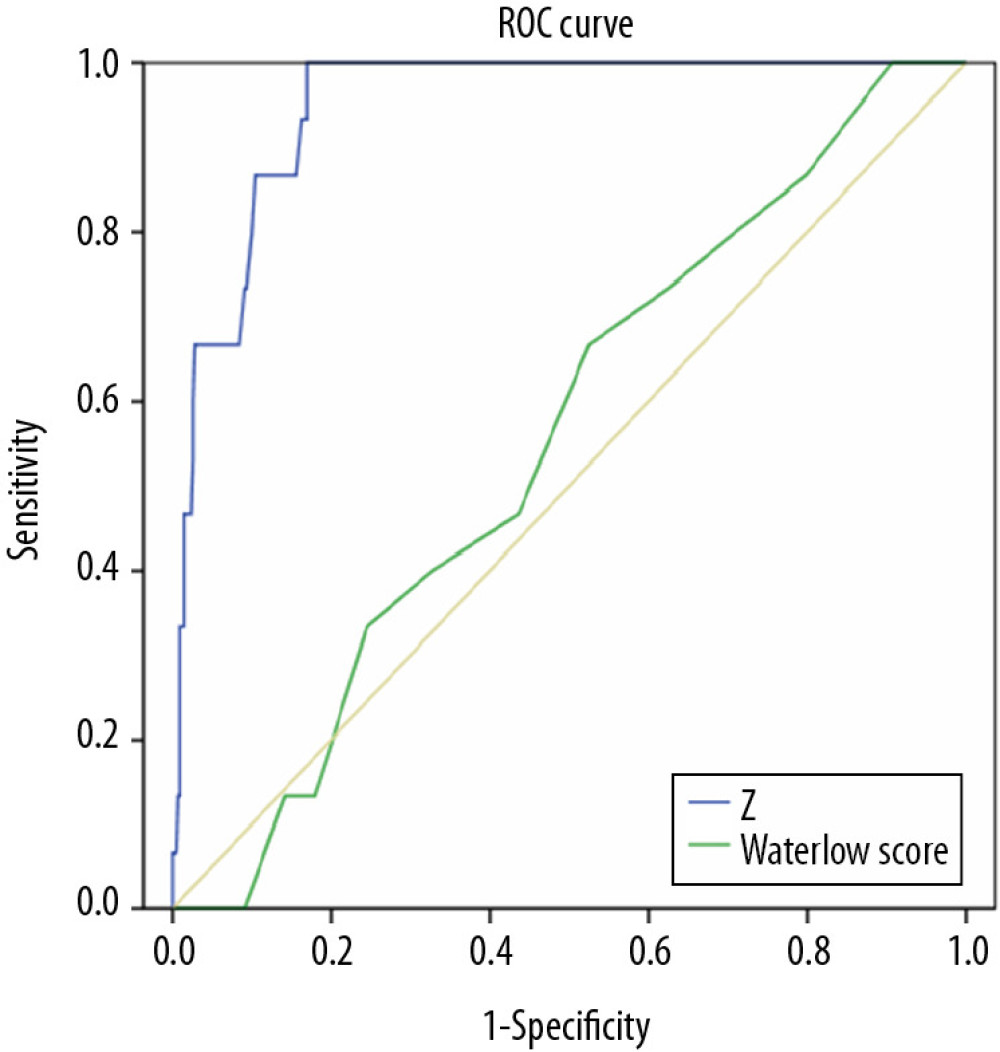
The areas under the curve (AUC) of the 2 ROC curves were 0.938 and 0.555, suggesting that the constructed risk prediction model had good discrimination (Figure 1). The detailed results are shown in Table 5. The risk prediction model constructed in this study had a Youden index of 0.834. The maximum value of the Youden index was used as the optimal critical value of the risk prediction equation. Its sensitivity and specificity were 100.00% and 83.40%, respectively.
Discussion
PREVALENCE OF PI IN CRITICALLY ILL PATIENTS WITH CANCER:
In this study, the incidence rate of PI per 100 patient-days in critically ill patients with cancer was 3.14%, and the cumulative incidence rate was 3.09%. Our results are quite different from the results of Jomar et al. in Brazil, who reported a patient-day incidence rate of PI in oncological ICU patients of 1.32%, and a cumulative incidence rate of 29.50% [12]. A PubMed, Web of Science, and Google Scholar search by the present authors did not produce relevant reports on the incidence of PI in critically ill patients with cancer. Therefore, the results of the study by Jomar et al. cannot be further discussed, and analysis of the differences between that study and the present one revealed that the difference may result from our exclusion of patients with stage I PI. In other studies, the incidence of PI in non-specialized ICU patients or immobilized hospitalized patients was reported as 1.23% to 31.4% ]19–22]. For now, the cumulative incidence of PI in critically ill patients with cancer is 3.09% to 29.50%; however, studies with larger sample sizes are needed to provide more accuracy.
APACHE II SCORE: The APACHE II score is the most popular clinical evaluation system of critical illness in use in ICUs; it is also an important indicator of disease development and rehabilitation of critically ill patients. It is composed of an acute physiology score, age score, and chronic health condition score. The theoretical maximum score is 71 points. A higher score means a higher risk of death [23]. Previous studies have shown that the APACHE II risk of death determination is associated with the incidence of PI in critically ill patients [24]. The present study found that the APACHE II score was an independent risk factor for the occurrence of PI in critically ill patients with cancer. The higher the APACHE II score, the more critical the patient’s condition and the higher the risk of PI. The score showed that the occurrence of PI in critically ill patients was affected by the basic condition of patients with cancer. The results of the present study were consistent with previous studies. The APACHE II score helped predict the occurrence of PI, and the incidence of PI in critically ill patients was relatively high [25,26].
SEMI-RECLINING POSITION: The oncological ICU is a special ward that monitors and actively treats patients with various cancer-related acute and critical illnesses and multiple system organ dysfunction or failure. Because of the need for treatment, it is difficult to avoid intervention by mechanical ventilation. Studies recommended an upper body elevation >30° and have shown that a head of bed elevation angle <30° is an independent risk factor for ventilator-associated pneumonia in patients with tracheal intubation and mechanical ventilation [27,28]. The head of bed elevation is considered by the Joint Commission on Accreditation of Healthcare Organizations as one of the core measures to improve the quality of care for critically ill patients. The semi-reclining position is conducive to blood circulation and increases tidal volume; however, this particular position was associated with potential PI [29]. The results of the present study suggest that patients in a semi-reclining position may have PI, which is consistent with the aforementioned study.
MOIST SKIN:
Moist skin is an important contributing factor to the formation of PI. Our results suggest that skin in a wet environment is an independent risk factor for PI occurrence in critically ill patients with cancer. Moist skin is an item in the Braden scale, and studies have confirmed that it is related to the occurrence of PI [30]. Additionally, research showed that due to seasonal differences, skin is more likely to be in a humid environment in the summer. This environment weakens the barrier effect of the human skin stratum corneum, thereby causing local skin edema, allowing harmful substances to pass easily, and increasing cell reproduction, which further damages the skin and leads to different degrees of PI [31].
EDEMA:
Edema is excessive fluid retention in the interstitial space. Our results indicated that edema is an independent risk factor for PI in critically ill patients. Baker et al. conducted a survey of 20 nursing home residents through convenience sampling and found that even with patients receiving continuous high-quality care, there is still a risk of PI occurrence; however, edema did not frequently accompany PI in these patients [32]. NPUAP reached a consensus in a multidisciplinary team meeting on the risk of edema in PI occurrence and identified a direct correlation between PI and edema [33]. This supports the results obtained in the present study.
CONSTRUCTION AND VERIFICATION OF PI OCCURRENCE RISK PREDICTION MODEL FOR CRITICALLY ILL PATIENTS WITH CANCER:
In this study, binary logistic regression analysis was used to obtain a risk prediction model for PI in critically ill patients with cancer, and the prediction effect of the risk prediction model was tested by ROC curve analysis. The AUC was 0.938, which indicated that the model had a good prediction ability. Its sensitivity and specificity were 100.00% and 83.40%, respectively, and the Youden index was 0.834. That is to say, when the equation prediction value Z ≥0.834, patients with cancer were at high risk for PI. When the score approaches or reaches 0.745, medical staff should give targeted interventions to reduce the risk of PI.
STUDY LIMITATION:
This study was conducted in a single hospital, and the patient sample was relatively limited. The prediction effect of the risk model needs to be verified by further studies with larger sample sizes. Also, differences in nursing practices related to PI development were not investigated in this study.
Conclusions
Researchers in previous studies have developed prediction tools for hospital-acquired PI in different patient populations and found them helpful [34,35]. In the present study, we analyzed the risk factors related to PI occurrence and constructed a risk prediction model for critically ill patients with cancer. The model suggested the key points of screening for the risk of PI in critically ill patients with cancer and it had good predictive ability. We recommend that clinical nurses use risk prediction scores to implement targeted nursing interventions. For high-risk patients, we also recommended position change and shin care to prevent PI.
Tables
Table 1. Locations and stages of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).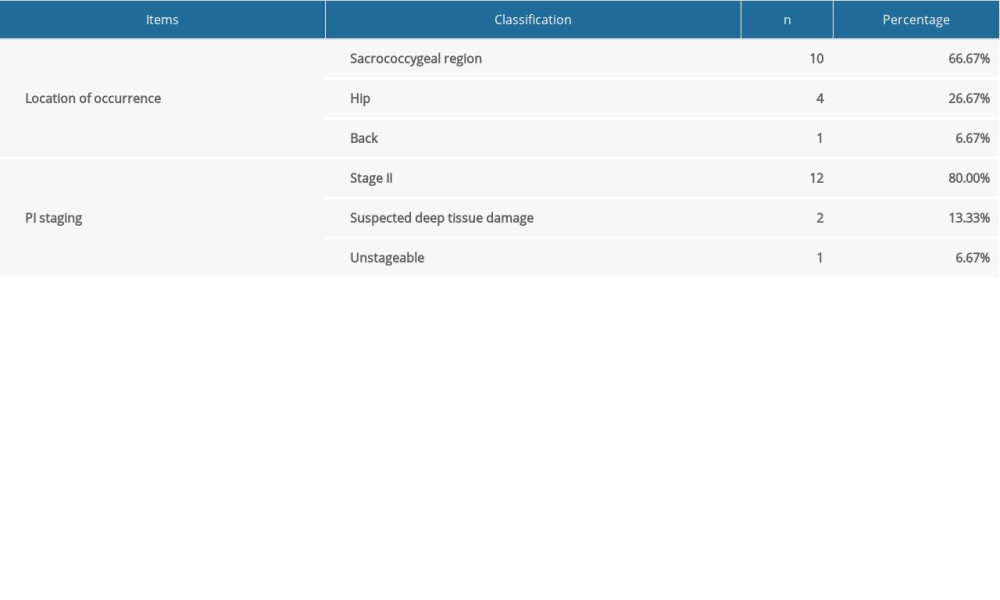 Table 2. Univariate analysis of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).
Table 2. Univariate analysis of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).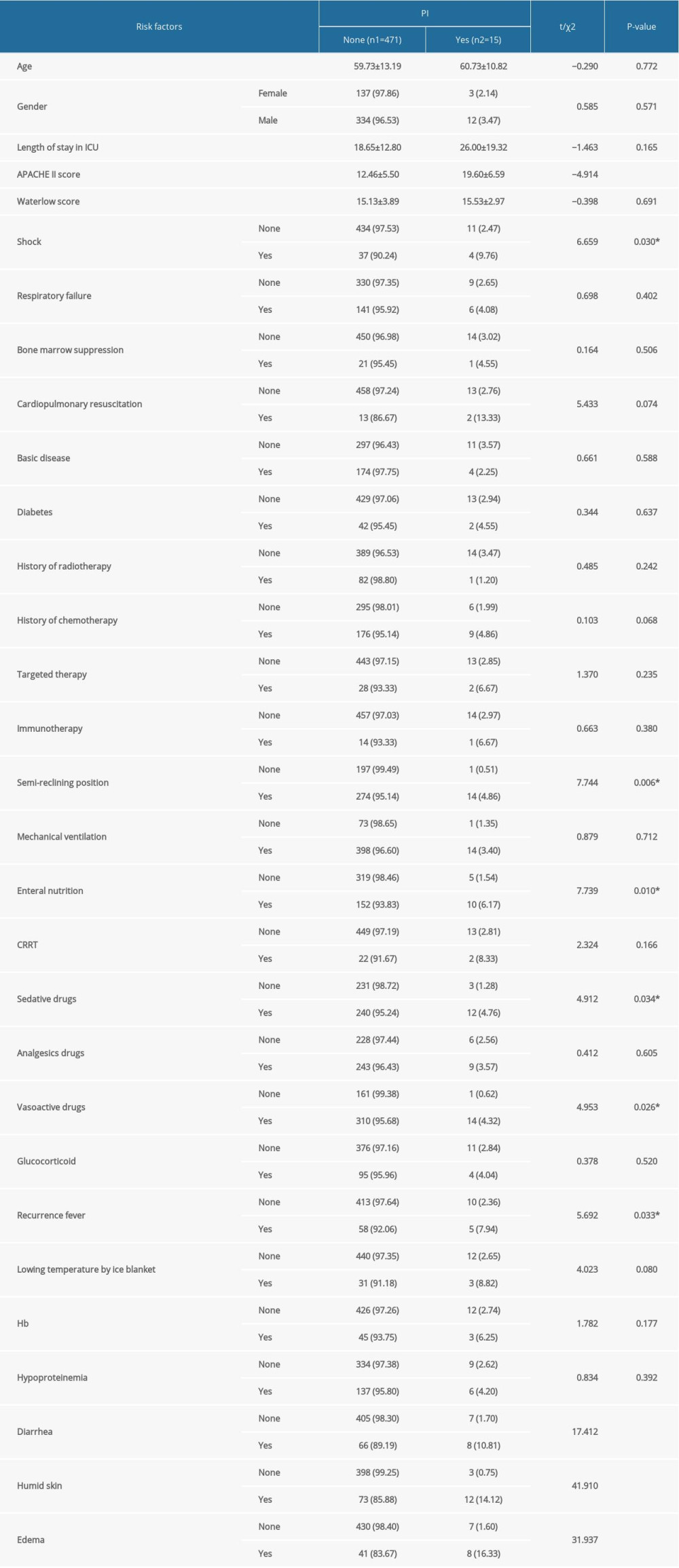 Table 3. Variable assignment table.
Table 3. Variable assignment table.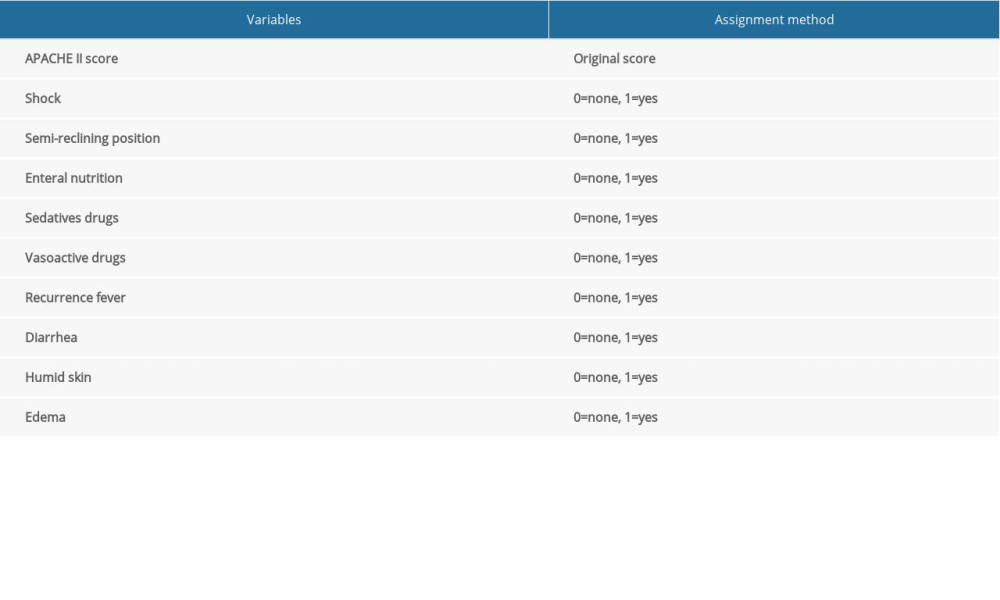 Table 4. Multivariate analysis of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).
Table 4. Multivariate analysis of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).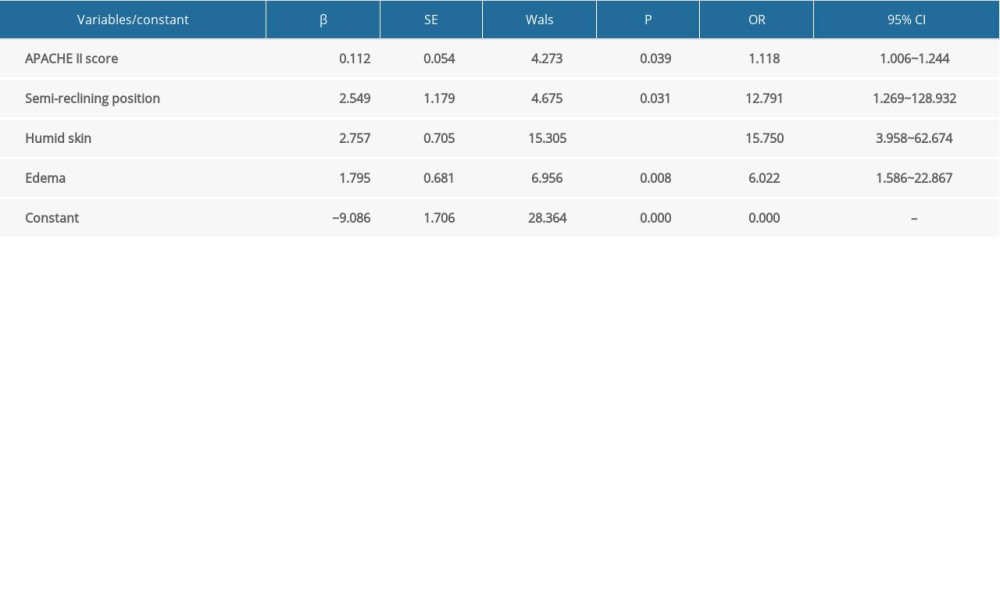 Table 5. Pressure injury (PI) risk prediction equation for critically ill patients with cancer and the area under the curve (AUC) of the Waterlow PI score.
Table 5. Pressure injury (PI) risk prediction equation for critically ill patients with cancer and the area under the curve (AUC) of the Waterlow PI score.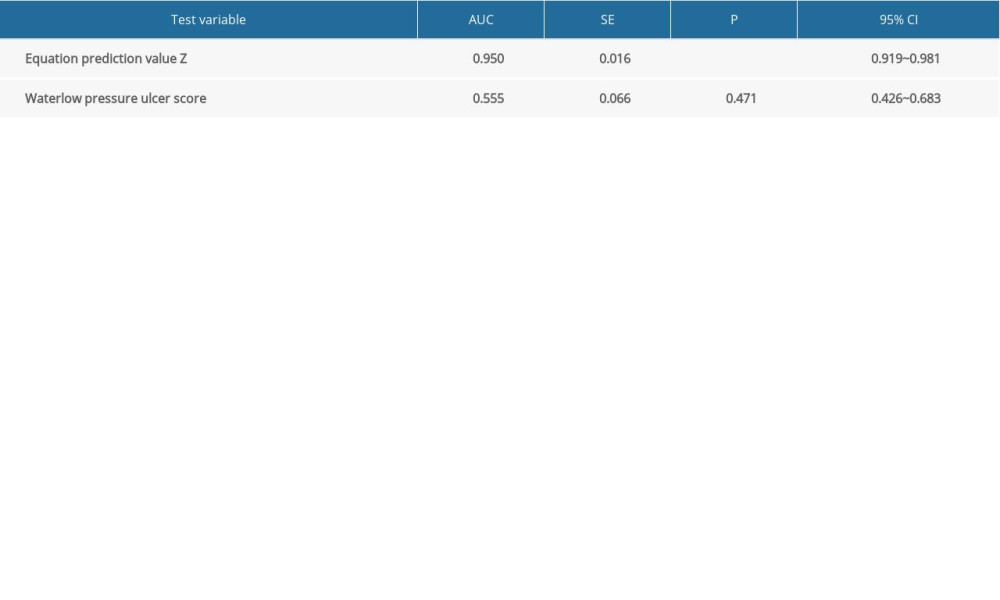
References
1. Edlich RF, Winters KL, Woodard CR, Pressure ulcer prevention: J Long Term Eff Med Implants, 2004; 14; 285-304
2. Hajhosseini B, Longaker MT, Gurtner GC, Pressure injury: Ann Surg, 2020; 271; 671-79
3. McGee WT, Nathanson BH, Lederman E, Pressure injuries at Untensive Care Unit admission as a prognostic indicator of patient outcomes: Crit Care Nurse, 2019; 39; 44-50
4. Coyer F, Miles S, Gosley S, Pressure injury prevalence in intensive care versus non-intensive care patients: A state-wide comparison: Aust Crit Care, 2017; 30; 244-50
5. Chaboyer WP, Thalib L, Harbeck EL, Incidence and prevalence of pressure injuries in adult intensive care patients: A systematic review and meta-analysis: Crit Care Med, 2018; 46; e1074-81
6. Padula WV, Delarmente BA, The national cost of hospital-acquired pressure injuries in the United States: Int Wound J, 2019; 16; 634-40
7. Nguyen KH, Chaboyer W, Whitty JA, Pressure injury in Australian public hospitals: A cost-of-illness study: Aust Health Rev, 2015; 39; 329-36
8. Masaki F, Riko K, Seiji H, Evaluation of pressure ulcers in 202 patients with cancer: Wounds, 2007; 19; 13-19
9. Criado PR, Brandt HR, Moure ER, Adverse mucocutaneous reactions related to chemotherapeutic agents: Part II: An Bras Dermatol, 2010; 85; 591-608
10. Li HL, Lin SW, Hwang YT, Using nursing information and data mining to explore the factors that predict pressure injuries for patients at the end of life: Comput Inform Nurs, 2019; 37; 133-41
11. Levine JM, Menezes R, Namagiri S, Wounds related to malignancy in postacute and long-term care: A case series: Adv Skin Wound Care, 2020; 33; 99-102
12. Jomar RT, Jesus RP, Jesus MP, Incidence of pressure injury in an oncological Intensive Care Unit: Revi Bras Enferm, 2019; 72; 1490-95
13. Charalambous C, Koulori A, Vasilopoulos A, Evaluation of the validity and reliability of the Waterlow pressure ulcer risk assessment scale: Med Arch (Sarajevo, Bosnia and Herzegovina), 2018; 72; 141-44
14. Liao Y, Gao G, Mo L, Predictive accuracy of the Braden Q Scale in risk assessment for paediatric pressure ulcer: A meta-analysis: Int J Nurs Sci, 2018; 5; 419-26
15. Edsberg LE, Black JM, Goldberg M, Revised national pressure ulcer advisory panel pressure injury staging system: Revised pressure injury staging system: J Wound Ostomy Continence Nurs, 2016; 43; 585-97
16. Schiller LR, Pardi DS, Sellin JH, Chronic diarrhea: Diagnosis and management: Clin Gastroenterol Hepatol, 2017; 15; 182-93.e183
17. Fernandez Guerrero ML, Jimenez Rodriguez A, de Julian Jimenez ARecurrent fever as presenting from of colon carcinoma: Rev Clin Esp, 2002; 202; 592-95 [in Spanish]
18. Torreggiani S, Filocamo G, Esposito S, Recurrent fever in children: Int J Mol Sci, 2016; 17; 448
19. He M, Tang A, Ge X, Pressure ulcers in the Intensive Care Unit: An analysis of skin barrier risk factors: Adv Skin Wound Care, 2016; 29; 493-98
20. Liu Y, Wu X, Ma Y, The prevalence, incidence, and associated factors of pressure injuries among immobile inpatients: A multicentre, cross-sectional, exploratory descriptive study in China: Int Would J, 2019; 16; 459-66
21. Strazzieri-Pulido KC, Gonzales CVS, Nogueira PC, Pressure injuries in critical patients: Incidence, patient-associated factors, and nursing workload: J Nurs Manag, 2019; 27; 301-10
22. Feng H, Wu Y, Su C, Skin injury prevalence and incidence in China: A multicentre investigation: J Wound Care, 2018; 27; S4-9
23. Knaus WA, Draper EA, Wagner DP, APACHE II: A severity of disease classification system: Crit Care Med, 1985; 13; 818-29
24. Gulin FS, Menegueti MG, Auxiliadora-Martins M, APACHE II death risk and length of stay in the ICU are associated with pressure injury in critically ill patients: J Clin Med Res, 2018; 10; 898-903
25. Ulker E, Yapucu Gunes U, A prospective, descriptive study of risk factors related to pressure ulcer development among patients in Intensive Care Units: Ostomy Wound Manag, 2013; 59; 22-27
26. Catala Espinosa AI, Hidalgo Encinas Y, Cherednichenko TCorrelation between body mass index and development of pressure ulcers in intensive care medicine: Enferm Intensiva, 2014; 25; 107-13
27. Kollef MH, Prevention of nosocomial pneumonia in the Intensive Care Unit: Beyond the use of bundles: Surg Infect, 2011; 12; 211-20
28. Benhamou D, Cuvelier A, Muir JFPrevention of infections transmitted by CPAP and noninvasive ventilation: Rev Pneumol Clin, 2001; 57; 73-78 [in French]
29. Burlingame BL, Guideline implementation: Positioning the patient: AORN J, 2017; 106; 227-37
30. Zambonato BP, de Assis MC, Beghetto MGAssociation of Braden subscales with the risk of development of pressure ulcer: Rev Gaucha Enferm, 2013; 34; 21-28 [in Portuguese]
31. Chen HL, Zhu B, Wei R, A retrospective analysis to evaluate seasonal pressure injury incidence differences among hip fracture patients in a tertiary hospital in East China: Ostomy Wound Manag, 2018; 64; 40-44
32. Baker MW, Whitney JD, Lowe JR, Full-thickness and unstageable pressure injuries that develop in nursing home residents despite consistently good quality care: J Wound Ostomy Continence Nurs, 2016; 43; 464-70
33. Edsberg LE, Langemo D, Baharestani MM, Unavoidable pressure injury: State of the science and consensus outcomes: J Wound Ostomy Continence Nurs, 2014; 41; 313-34
34. Aloweni F, Ang SY, Fook-Chong S, A prediction tool for hospital-acquired pressure ulcers among surgical patients: Surgical pressure ulcer risk score: Int Wound J, 2019; 16; 164-75
35. Alderden J, Pepper GA, Wilson A, Predicting pressure injury in critical care patients: A machine-learning model: Am J Crit Care, 2018; 27; 461-68
Tables
Table 1. Locations and stages of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).Table 2. Univariate analysis of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).Table 3. Variable assignment table.Table 4. Multivariate analysis of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).Table 5. Pressure injury (PI) risk prediction equation for critically ill patients with cancer and the area under the curve (AUC) of the Waterlow PI score.Table 1. Locations and stages of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).Table 2. Univariate analysis of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).Table 3. Variable assignment table.Table 4. Multivariate analysis of pressure injury (PI) occurrence in critically ill patients with cancer (n, %).Table 5. Pressure injury (PI) risk prediction equation for critically ill patients with cancer and the area under the curve (AUC) of the Waterlow PI score. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387