18 January 2021: Clinical Research
Effect of Lung Recruitment Maneuvers on Reduction of Atelectasis Determined by Lung Ultrasound in Patients More Than 60 Years Old Undergoing Laparoscopic Surgery for Colorectal Carcinoma: A Prospective Study at a Single Center
Yujiao Yang1ABCDEFG*, Yuan Geng1BC, Donghang Zhang2E, Yong Wan1E, Rurong Wang2CEFGDOI: 10.12659/MSM.926748
Med Sci Monit 2021; 27:e926748






Abstract
BACKGROUND: Atelectasis occurs in patients of all ages during various surgeries. Previous studies have mainly focused on perioperative atelectasis in infants. However, research on the incidence of atelectasis among elderly patients, particularly those undergoing laparoscopic surgeries, is limited. Therefore, this prospective study aimed to investigate the effect of lung recruitment maneuvers (LRMs) on the reduction of atelectasis determined by lung ultrasound in patients more than 60 years old undergoing laparoscopic surgery for colorectal carcinoma.
MATERIAL AND METHODS: In this evaluator-blinded clinical study, 42 patients more than 60 years old diagnosed with colorectal carcinoma were randomly grouped either into a lung recruitment maneuver (RM) group or control (C) group. All patients were scheduled for laparoscopic surgery under general anesthesia using the lung-protective ventilation strategy. Lung ultrasonography was carried out at 3 predetermined time intervals. Patients in the RM group received ultrasound-guided recruitment maneuvers once atelectasis was discovered by lung ultrasound. Scores of lung ultrasound were used for assessing the severity of lung atelectasis.
RESULTS: At the end of the operation, the occurrence of atelectasis was 100% in the RM group and 95% in the C group. After RMs, the frequency of atelectasis in the RM group and C group was 50% and 95%, respectively (P<0.01). Postoperative pulmonary complications were not different between the 2 groups.
CONCLUSIONS: At a single center, patients more than 60 years old undergoing laparoscopic surgery for colorectal carcinoma had a prevalence of lung atelectasis of 100% and although LRMs significantly reduced the incidence of pulmonary atelectasis, they did not improve postoperative pulmonary complications.
Keywords: Colorectal Neoplasms, pulmonary atelectasis, Ultrasonography, Doppler, Laparoscopy, Monitoring, Intraoperative, Postoperative Complications, Respiration, Artificial, Ultrasonography
Background
Atelectasis is among the most frequent postoperative pulmonary complications of general anesthesia and can be observed in all types of surgery and all ages of patients [1,2]. Atelectasis impairs gas exchange, thus causing hypoxemia and likely other respiratory disorders such as acute lung injury and pneumonia. These complications in turn lead to prolonged intensive care unit stay and increased mortality rates of hospitalized patients [3].
A systematic review found that utilization of lung recruitment maneuvers (LRMs) under general anesthesia may reduce postoperative pulmonary complications (PPCs) and improve patient outcomes [4]. A meta-analysis by Goligher et al. [5] examined 1423 acute respiratory distress syndrome patients and suggested that LRMs in combination with a higher positive end-expiratory pressure (PEEP) ventilation strategy reduced mortality, but confidence in this finding is limited [5]. A multicenter study compared 4 lung-protective ventilation strategies with standard protective ventilation. No benefit was seen in the groups receiving lung-protective ventilation strategies and PPCs were equally high (about 45%) [6]. In 2019, as systematic review and meta-analysis reported by Cui et al. [7] showed that when LRMs were combined with lung-protective ventilation strategies there was a reduced incidence of PPCs and oxygenation improved in nonobese patients, but the variations in LRMs and ventilation patterns may affect the outcome. Conversely, data on how these strategies can be implemented in older patients are insufficient. Multiple studies have confirmed that patients more than 60 or 65 years old are more likely to develop PPCs after general anesthesia [8].
Currently, a growing number of abdominal operations are performed using endoscopy, which has the superiority of minimal trauma and bleeding, a light stress reaction, and enhanced postoperative recovery [9]. However, the adverse effects of the long operation time, special position, and artificial pneumoperitoneum on the physiological functions of respiration and circulation are much more serious in patients undergoing laparoscopic surgery than laparotomy [10].
Lung ultrasound has become a powerful method for assessing different pulmonary diseases and is a valuable approach in critical and emergency care [11]. In a recent randomized controlled trial study, Kim et al. used lung ultrasound score to determine the effect of fraction of inspired oxygen (FIO2) during LRM on absorption atelectasis in laparoscopic surgery. They revealed that a high FIO2 (1.0) during RM led to a higher degree of postoperative atelectasis [12]. In addition, several systematic reviews focused on the chest ultrasound for the diagnosis of pulmonary diseases, revealing that lung ultrasonography is a valuable tool in diagnosing pulmonary disorders [13– 15]. Lung ultrasound has the advantages of being noninvasive, portable, easy to use, and radiation-free compared with thoracic computed tomography. Therefore, this prospective study aimed to investigate the effect of LRM on the reduction of atelectasis determined by lung ultrasound in patients more than 60 years old undergoing laparoscopic surgery for colorectal carcinoma.
Material and Methods
STUDY POPULATION:
Between April and December 2019, eligible patients ≥60 years old scheduled for laparoscopic surgery for colorectal cancer in a Trendelenburg position were included in this prospective study. All the patients participating in this study were within the American Society of Anesthesiologists physical status classes I–III. The duration of surgery was expected to be ≥2 h [16, 17]. The exclusion criteria were as follows: (1) a body mass index >30 kg/m2, (2) patients with a history of thoracic procedures, (3) confirmed atelectasis at baseline, (4) a history of general anesthesia and ventilation 14 days before surgery, (5) chronic pulmonary disorder (forced expiration value <30% of the expected value in 1 s), (6) chronic obstructive pulmonary disease, (7) chronic heart disease, and (8) neuromuscular disease. The exit criteria were as follows: (1) severe subcutaneous emphysema occurred during the operation, (2) the surgical procedure was less than 2 h, and (3) the operation method changed from laparoscopy to laparotomy.
ANESTHESIA AND VENTILATION PROTOCOL:
After having instituted standard electrocardiogram, pulse oximetry monitoring, and noninvasive systemic arterial pressure (BeneVision N15, China), all included participants were preoxygenated for 5 min with 100% oxygen. Next, they were anesthetized with 0.04–0.05 mg/kg midazolam (intravenously [IV]), 0.15–0.3 mg/kg etomidate and 0.4 μg/kg sufentanil, and 0.15 mg/kg cisatracurium was given for smooth endotracheal intubation. Adopting the surgical procedure, patients were kept in a Trendelenburg position after anesthesia. Anesthesia was retained through incessant IV infusion of 0.1–0.3 μg·kg−1·min −1 remifentanil, 4–12 mg·kg−1·h−1 propofol, and 0.05–0.1 mg·kg−1·h−1 cisatracurium combined with 1–3% inhaled sevoflurane. Neurophysiologic monitoring (Veryark-TOF, China) was used to assess the depth of anesthesia with a bispectral index of 40–60 in all patients during surgery.
Mechanical ventilation was set in a volume-control mode with a
LUNG ULTRASONOGRAPHY:
Lung ultrasonography was done by 2 skilled anesthetists (YG and YY, having 6 months and 24 months of experience respectively) through a portable device (Sonosite, USA) having a 2- to 5-MHz probe. Sonograms were obtained at 3 predefined time points: 5–10 min before anesthesia (T1), at the end of the surgery (T2), and 30 min after extubation (T3). As previously reported [10, 16], the thorax was alienated into 12 quadrants. Posterior, lateral, and anterior zones were divided through the posterior and anterior axillary positions as anatomical areas, and each area was divided into superior and inferior zones for the right and left lung (Supplementary Figure 1). The ultrasound probe was located upright to the costal space to scan the 1 to 4 areas and was placed parallel to the costal space for scanning the 5 to 6 areas with patients in the supine position with the arm abducted, which helped to effectively observe the situation of the lungs in the 5 to 6 areas.
DEFINED LUNG ULTRASOUND SCORE:
The severity of atelectasis was evaluated by calculating the modified lung ultrasound score from Monastesse et al. [11], with scores between 0 and 3 (0=≤2 B lines; 1=≥3 B lines or multiple areas of subpleural consolidation separated by a normal pleural line; 2=multiple coalescent B lines, or multiple areas of subpleural consolidation separated by a thickened pleura; 3=consolidation or small areas of subpleural consolidation >1×2 cm in diameter (Supplementary Table 1). Lung ultrasound score 0 to 36 was estimated by summing the 12 individual quadrant scores, with higher scores suggesting chronic atelectasis, and we defined pulmonary atelectasis to be significant when the lung ultrasound score ≥2 in any region. We assumed that the lung ultrasound score on T2 can reflect the primary outcomes.
SAMPLE SIZE ESTIMATION AND LRMS:
Previous studies were adopted to measure the sample size used in this study [18]. The occurrence of atelectasis in adults after general anesthesia is approximately 90% according to the previous report [19]. In another pediatric report, the frequency of atelectasis was as high as 100% in patients under magnetic resonance imaging examination [20]. Our preliminary experimental results showed that the rate of atelectasis was 95% in adults after laparoscopic colorectal surgery, and the atelectasis incidence could be reduced to 50% through an LRM. A previous study reported that the sensitivity of lung ultrasound in detecting atelectasis was 88% [20]. In this study, we assumed a 0.05 alpha error and 80% power, and we allowed for a dropout rate of 20%. The sample size needed would then be 20 patients per group.
The only difference in interventions between the groups was whether the alveolar RMs were performed. At point T2, individuals in the RM group received alveolar enrollment maneuvers under ultrasound guidance. The alveolar RMs were performed with a gradual rise in airway pressure from 10 cmH 2O by 5 cmH2O increments, and a FIO2 of 0.4 was applied manually until no collapsed lung areas were visible on the sonogram. Then, the pressure was maintained for 40 s. Airway maximum pressure was limited to 40 cmH2O. Patients in the C group did not receive RMs.
POSTOPERATIVE PULMONARY COMPLICATIONS:
The PPCs of the patients were defined by a previous study [3], including respiratory failure, described a postoperative arterial partial oxygen level (PaO2) just under 60 mmHg on room air, a PaO2: FIO2 ratio less than 300 mmHg, or peripheral oxygen concentration as calculated by pulse oximetry less than 90% and requiring oxygen therapy. Patients with 2 L or less of supplementary oxygen are graded as having a mild failure; reacting only to oxygen greater than 2 L, moderate failure. Other pulmonary complications include bronchospasm, pulmonary infection, and acute respiratory distress syndrome. Patients were followed daily after surgery until they were discharged from the hospital.
STATISTICAL ANALYSIS:
Anthropometric data and demographics were collected from the individual patient. Following the normality of data testing, the Mann-Whitney
Results
From April until December 2019, 62 individuals were evaluated for enrollment in the study, 20 of whom were excluded before surgery for reasons shown in Figure 1. Forty-two patients were randomly distributed to the RM group and the C group (
All lung ultrasound examinations were completed with per time point of average 10 (8.0–13.2) min. A total of 1440 images was acquired during the study. Representative lung ultrasound images at various periods are shown in Figure 2.
The incidence of pulmonary atelectasis at different steps is summarized in Table 1. At T3, statistically less atelectasis in the RM group than in the C group (Table 1) was reported. The score of lung ultrasound of total areas was obtained in the 2 groups during the 3 steps, as shown in Figure 3. At T1 and T2, the lung ultrasound scores of the RM group and C group were not statically different (
Lung ultrasound scores of the 2 groups in different areas are shown in Figure 4. At T2, no significant difference in lung ultrasound scores between the RM group and C group was observed (
There were no statistical differences in PPCs between the 2 groups ( Table 2).
Discussion
In this evaluator-blinded prospective clinical study, we found a high incidence of atelectasis in patients more than 60 years old undergoing laparoscopic surgery for colorectal cancer. The methodological part of this study is similar to a previous study by Monastesse et al. [11] in many ways; both used ultrasound to assess the atelectasis during laparoscopic surgery. The aim of the previously published study was to investigate the feasibility of lung ultrasonography in the perioperative period, whereas this study aimed to investigate the effect of LRMs on the reduction of atelectasis determined by lung ultrasound. The occurrence of atelectasis in the C group and the RM group was 95% and 100%, respectively. The incidence of atelectasis in the RM group decreased to 50% after the recruitment of maneuvers with ultrasound guidance. The frequency of postoperative atelectasis is higher than in previous studies [21]. We speculate that the special position and pneumoperitoneum of this type of surgery may be the major causes for this high incidence of atelectasis. The Trendelenburg position can cause the diaphragm to lift, resulting in lung compression and atelectasis [22]. Moreover, induction of carbon dioxide pneumoperitoneum may cause cranial displacement of the diaphragm, leading to decrease in volume of the lung, and a rise in mean atelectasis volume [23].
In this study, we found that the main areas of atelectasis existed in zones 5 and 6 (the patient’s dorsum in a supine state), which is consistent with previous results [20]. This is primarily due to the lung tissue deformation caused by the cranial dislocation of the crippled diaphragm [20]. There was no significant difference in the C group between the degree of atelectasis at T2 and T3, indicating that atelectasis will not disappear in a short time without intervention. It has been reported that atelectasis caused by general anesthesia can last for several days after surgery and in some cases can even lead to serious complications such as hypoxemia and pulmonary infection [24]. At T2, all patients in the RM group received an alveolar RM under lung ultrasound guidance until atelectasis disappeared. However, approximately 50% of the patients still exhibited varying degrees of atelectasis at T3. This may be explained by the following causes. First, patients were maintained in the supine position in the PACU, which may have reduced functional residual capacity and resulted in the cranial displacement of the diaphragm. Second, the degree of awaking from anesthesia impaired the removal of the patient’s sputum and other secretions, which may have blocked the airway and then caused atelectasis. Third, other influencing factors, such as the neuromuscular blockade degree, could also have affected atelectasis [25].
There are many methods used to reverse alveolar collapse, such as gradually increasing airway pressure and gradually increasing PEEP for lung recruitment [26]. As shown by a previous study, ultrasound-guided RMs are effective in raising anesthesia-induced atelectasis in children [11]. Considering that many elderly patients may have pulmonary bullae, the lung enrollment approach may enhance the pulmonary bullae rupture risk. Therefore, in this study, we gradually increased the airway pressure by 5 mmH2O to prevent collapse under the real-time guidance of ultrasound. We found that the incidence of atelectasis 30 min after extubation was significantly lower in the RM group than in the control group, indicating that alveolar RMs can effectively prevent atelectasis. However, there were still some disadvantages, as we selected the most serious area of atelectasis as the monitoring site [27]. When this lung area was completely recovered, other lung areas may have been hyperinflated, but no perioperative O 2 desaturation in any patient was observed, nor did any patients develop hemodynamic instability or lung injury in the enrollment maneuvers in our study.
Postoperative pulmonary complications within the hospital stay occurred in 8 patients (40%) in the C group compared with 7 patients (35.0%) in the RM group. The rate of pulmonary disorders was higher than that reported in previous studies [28,29]. The causes for this may be related to the higher number of male patients, smokers, and underlying pulmonary diseases in our population, which could have had a poor effect on lung function [30]. The incidence of pulmonary complications in the current study suggested that the combination of PEEP and RMs directing to shrink atelectasis did not avoid PPCs compared with a strategy with PEEP and no RMs. We found that there were differences in lung ultrasound scores between the 2 groups at T3, but no statistical differences between the 2 groups in PPCs were reported. The possible causes were as follows: (1) In our protocol, we performed the RMs only at T2; thus, the frequency may not have been sufficient. However, Généreux et al. [31], who performed RMs every 30 min, found that PEEP and RMs prevented the loss of intraoperative aeration, but this loss did not continue after extubation, so other factors need to be explored. (2) The sample size may not have been sufficient because we calculated the sample size on the basis of the incidence of atelectasis, not complications. (3) Multiple interacting factors contribute to PPCs, and the influence of incidence and severity of atelectasis assessed by lung ultrasound on PPCs is still not clear.
There are also some limitations to this study. First, we did not perform lung ultrasonography after the induction of anesthesia. A previous study found that O2 is a key feature affecting the degree of atelectasis development, because the portion of inspired O2 during preoxygenation and the induction of anesthesia, rather than the continuation of anesthesia, plays a vital part in atelectasis formation [32]. In our study, to improve the safety of intubation, patients were preoxygenated with 100% O2. Therefore, it was impossible to determine the process of atelectasis formation. Second, we did not perform postoperative follow-up by lung ultrasound for these patients with atelectasis. It was thus impossible to evaluate the change in atelectasis after the operation or to evaluate whether atelectasis had a longer-term impact on the postoperative pulmonary condition of the patient. Third, this was a single-center study with a small sample size, which may not be easily extrapolated to other patients undergoing other types of surgery. Further multicenter studies with large sample sizes are required to evaluate the utility of lung ultrasound in assessing atelectasis.
Conclusions
At a single center, patients more than 60 years old undergoing laparoscopic surgery for colorectal carcinoma had a prevalence of lung atelectasis of 100%, and although LRMs significantly reduced the incidence of pulmonary atelectasis, they did not improve PPCs.
Figures
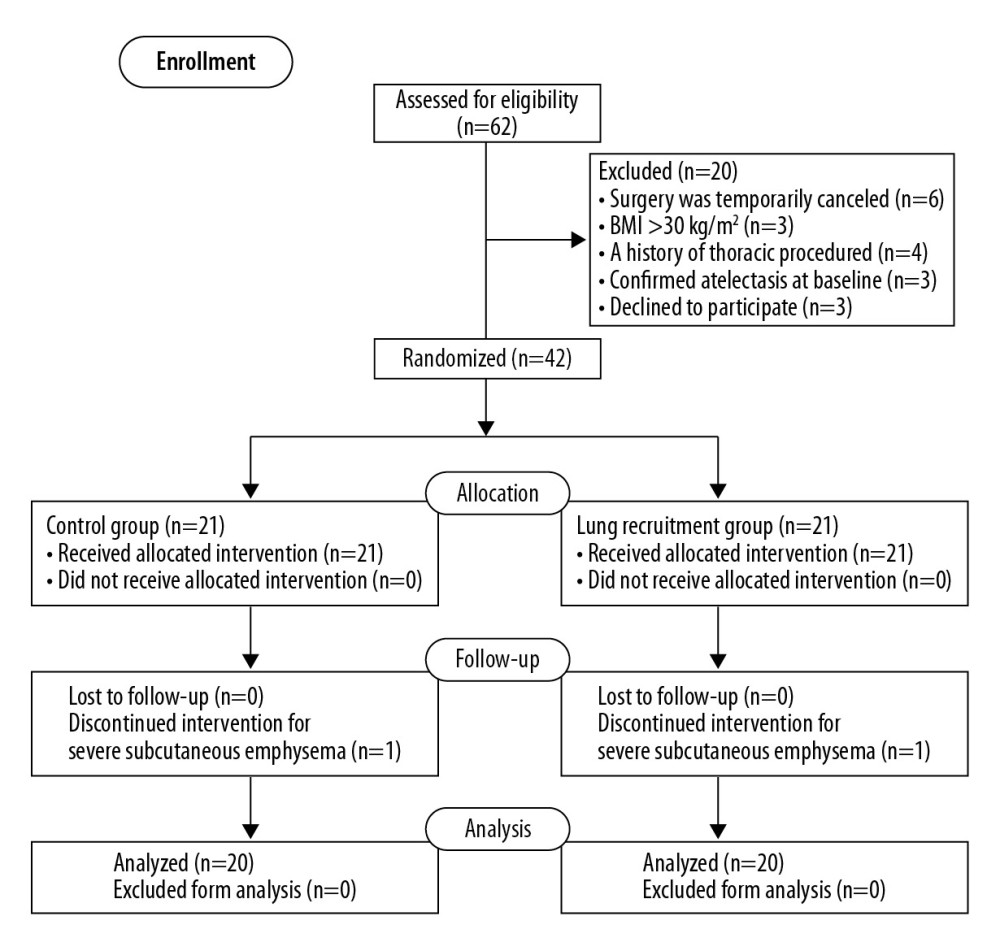 Figure 1. Flow diagram of patient screening and enrollment.
Figure 1. Flow diagram of patient screening and enrollment. 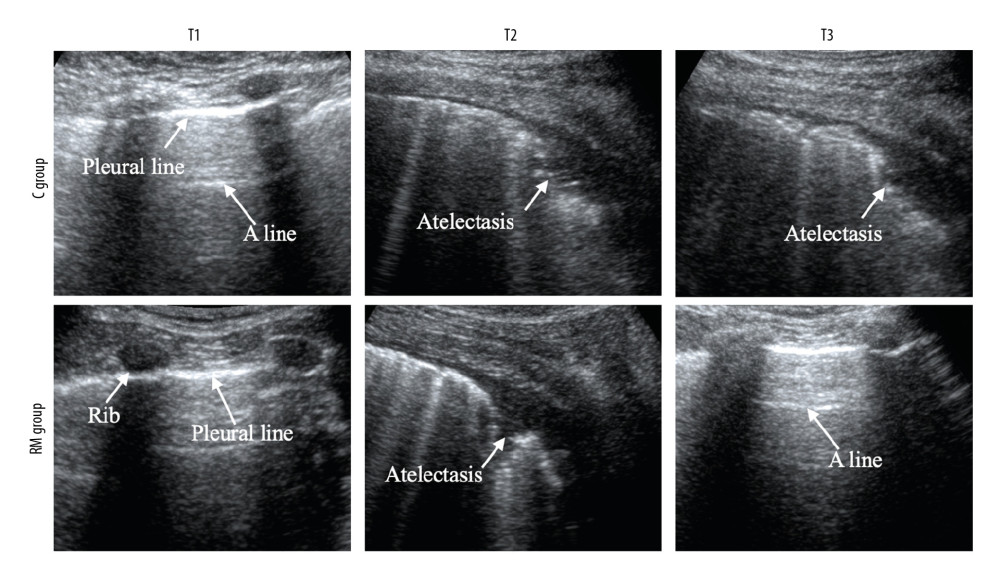 Figure 2. Lung ultrasound images of 1 representative patient per group. C group – control group; RM group – lung recruitment maneuver group. T1 – before the induction of anesthesia; T2 – at the end of the surgical procedure; T3 – 30 min after extubation.
Figure 2. Lung ultrasound images of 1 representative patient per group. C group – control group; RM group – lung recruitment maneuver group. T1 – before the induction of anesthesia; T2 – at the end of the surgical procedure; T3 – 30 min after extubation. 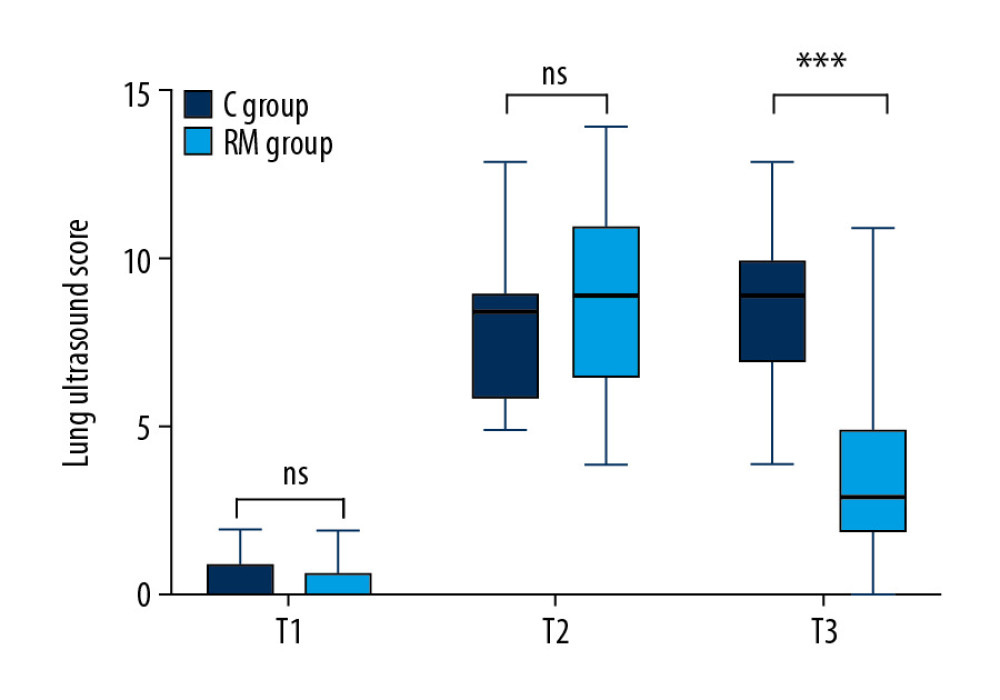 Figure 3. Lung ultrasound score of the total lung area in the control (C) group and lung recruitment maneuver (RM) group at the 3 time points. The data are presented as the median (thick line across the box), interquartile range (box), and range (whiskers). *** P<0.001 (independent-samples Mann-Whitney U test); ns – not significant.
Figure 3. Lung ultrasound score of the total lung area in the control (C) group and lung recruitment maneuver (RM) group at the 3 time points. The data are presented as the median (thick line across the box), interquartile range (box), and range (whiskers). *** P<0.001 (independent-samples Mann-Whitney U test); ns – not significant. 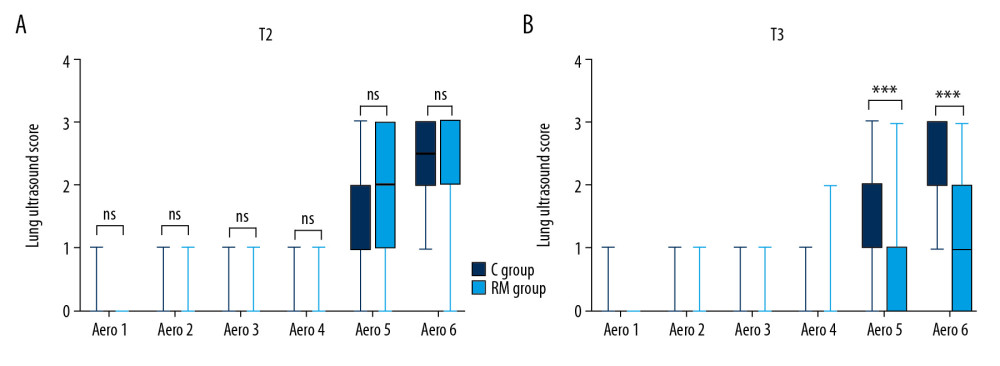 Figure 4. Lung ultrasound score of each lung area in the control (C) group and lung recruitment maneuver (RM) group. T2 – at the end of the surgical procedure; T3 – 30 min after extubation. (A) Scores in the 2 groups at T2. (B) Scores in the 2 groups at T3. The data are presented as the median (the thick line across the box), interquartile range (box), and range (whiskers). *** P<0.001 (independent-samples Mann-Whitney U test); ns – not significant.
Figure 4. Lung ultrasound score of each lung area in the control (C) group and lung recruitment maneuver (RM) group. T2 – at the end of the surgical procedure; T3 – 30 min after extubation. (A) Scores in the 2 groups at T2. (B) Scores in the 2 groups at T3. The data are presented as the median (the thick line across the box), interquartile range (box), and range (whiskers). *** P<0.001 (independent-samples Mann-Whitney U test); ns – not significant. Tables
Table 1. Incidence of atelectasis per group and per protocol step assessed by lung ultrasound.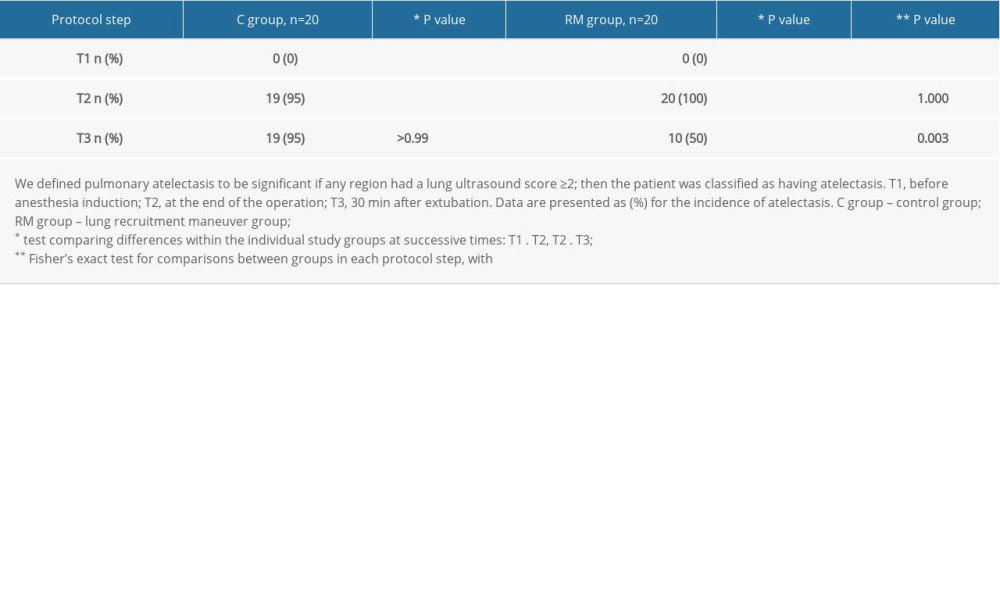 Table 2. Postoperative pulmonary complications.
Table 2. Postoperative pulmonary complications. Supplementary Table 1. Lung ultrasound (LUS) score.
Supplementary Table 1. Lung ultrasound (LUS) score.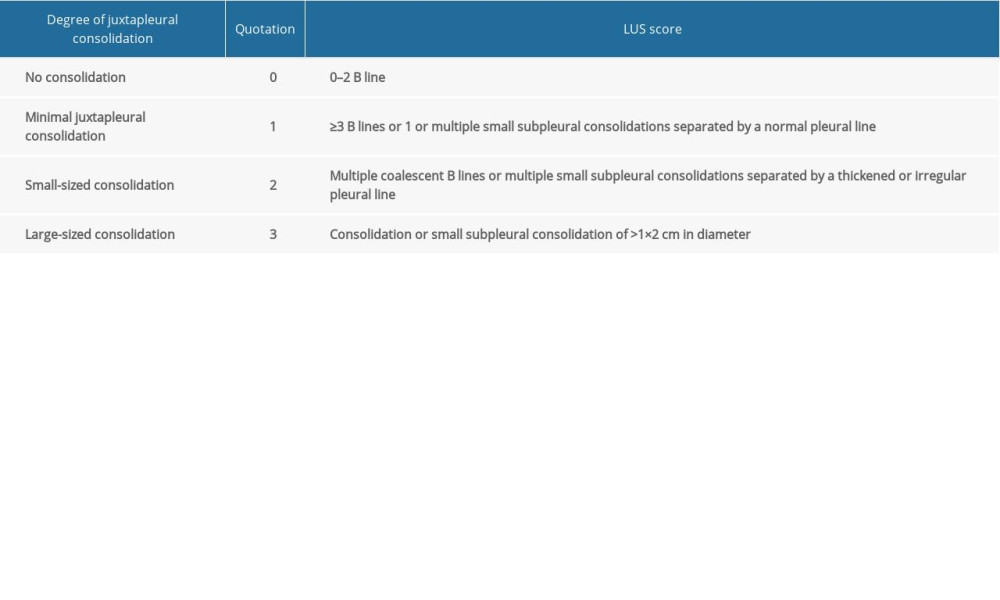 Supplementary Table 2. Demographic data of the enrolled patients.
Supplementary Table 2. Demographic data of the enrolled patients.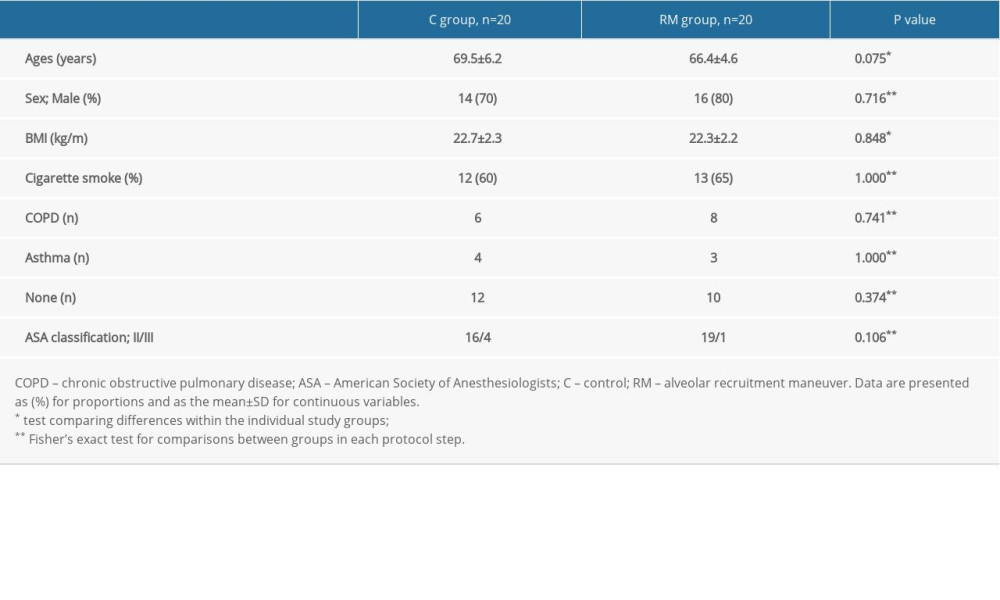 Supplementary Table 3. Intraoperation parameters of the enrolled patients.
Supplementary Table 3. Intraoperation parameters of the enrolled patients.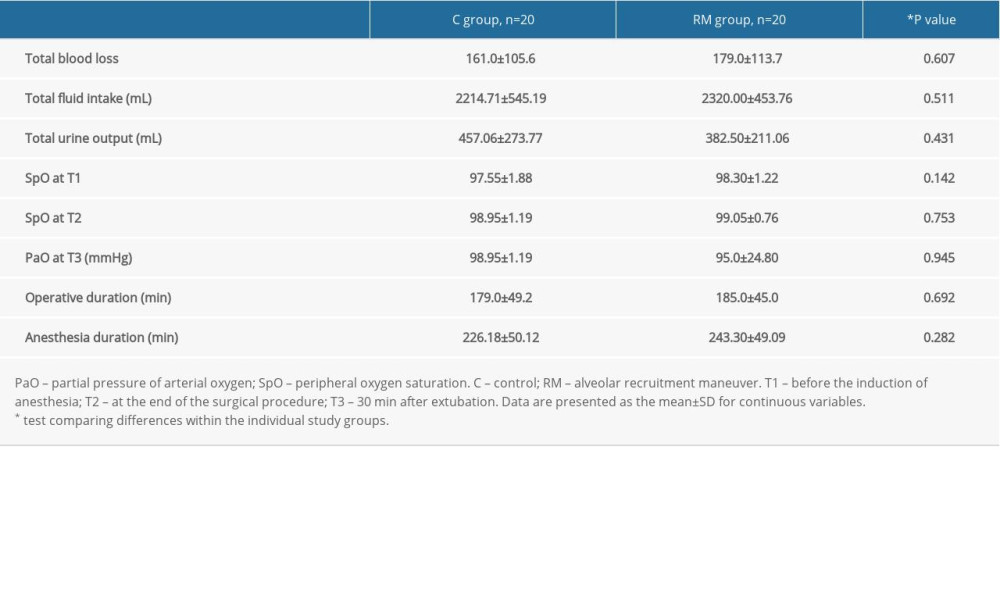
References
1. Forgiarini LA, Esquinas AMAtelectasis in postoperative bariatric surgery: How many understand them?: Rev Bras Anestesiol, 2018; 68(1); 109-10 [in Portuguese]
2. Fernandez-Bustamante A, Frendl G, Sprung J, Postoperative pulmonary complications, early mortality, and hospital stay following noncardiothoracic surgery: A multicenter study by the perioperative research network investigators : JAMA Surg, 2017; 152(2); 157-66
3. Miskovic A, Lumb AB, Postoperative pulmonary complications: Br J Anaesth, 2017; 118(3); 317-34
4. Hartland BL, Newell TJ, Damico N, Alveolar recruitment maneuvers under general anesthesia: A systematic review of the literature : Respir Care, 2015; 60(4); 609-20
5. Goligher EC, Hodgson CL, Adhikari NKJ, Lung recruitment maneuvers for adult patients with acute respiratory distress syndrome. A systematic review and meta-analysis : Ann Am Thorac Soc, 2017; 14(Suppl 4); S304-11
6. Ferrando C, Soro M, Unzueta C, Individualised perioperative open-lung approach versus standard protective ventilation in abdominal surgery (iPROVE): A randomised controlled trial : Lancet Respir Med, 2018; 6(3); 193-203
7. Cui Y, Cao R, Li G, The effect of lung recruitment maneuvers on post-operative pulmonary complications for patients undergoing general anesthesia: A meta-analysis : PLoS One, 2019; 14(5); e0217405
8. Hedenstierna G, Tokics L, Scaramuzzo G, Oxygenation Impairment during anesthesia: Anesthesiology, 2019; 131(1); 46-57
9. Mellor KL, Powell AGMT, Lewis WG, Laparoscopic surgery’s 100 most influential manuscripts: Surg Laparosc Endosc Percutaneous Tech, 2018; 28(1); 13-19
10. Arvizo C, Mehta ST, Yunker A, Adverse events related to trendelenburg position during laparoscopic surgery : Curr Opin Obstet Gynecol, 2018; 30(4); 272-78
11. Monastesse A, Girard F, Massicotte N, Lung ultrasonography for the assessment of perioperative atelectasis: A pilot feasibility study : Anesth Analg, 2017; 124(2); 494-504
12. Kim BR, Lee S, Bae H, Lung ultrasound score to determine the effect of fraction inspired oxygen during alveolar recruitment on absorption atelectasis in laparoscopic surgery: A randomized controlled trial : BMC Anesthesiol, 2020; 20(1); 173
13. Jaszczołt S, Polewczyk T, Dołęga-Kozierowska M, Comparison of lung ultrasound and chest X-ray findings in children with bronchiolitis : J Ultrason, 2018; 18(74); 193-97
14. Yousef N, De Luca D, The role of lung ultrasound in viral lower respiratory tract infections : Am J Perinatol, 2018; 35(6); 527-29
15. Supino MC, Buonsenso D, Scateni S, Point-of-care lung ultrasound in infants with bronchiolitis in the pediatric emergency department: A prospective study : Eur J Pediatr, 2019; 178(5); 623-32
16. Doyle DJ, Goyal A, Bansal P, Garmon EHAmerican Society of Anesthesiologists Classification (ASA Class): StatPearls July 4, 2020, Treasure Island (FL), StatPearls Publishing
17. Soyalp C, Yuzkat N, Kilic M, Operative and prognostic parameters associated with elective versus emergency surgery in a retrospective cohort of elderly patients : Aging Clin Exp Res, 2019; 31(3); 403-10
18. Song IK, Kim EH, Lee JH, Effects of an alveolar recruitment manoeuvre guided by lung ultrasound on anaesthesia-induced atelectasis in infants: A randomised, controlled trial : Anaesthesia, 2016; 72(2); 214-22
19. Gunnarsson L, Tokics L, Gustavsson H, Hedenstierna G, Influence of age on atelectasis formation and gas exchange impairment during general anaesthesia : Br J Anaesth, 1991; 66(4); 423-32
20. Tusman G, Böhm SH, Tempra A, Effects of recruitment maneuver on atelectasis in anesthetized children : Anesthesiology, 2003; 98(1); 14-22
21. Acosta CM, Sara T, Carpinella M, Lung recruitment prevents collapse during laparoscopy in children: A randomised controlled trial : Eur J Anaesthesiol, 2017; 35; 573-80
22. Strang CM, Hachenberg T, Fredén F, Hedenstierna G, Development of atelectasis and arterial to end-tidal P co 2-difference in a porcine model of pneumoperitoneum : Br J Anaesth, 2009; 103(2); 298-303
23. Andersson LE, Bååth M, Thörne A, Effect of carbon dioxide pneumoperitoneum on development of atelectasis during anesthesia, examined by spiral computed tomography : Anesthesiology, 2005; 102(2); 293-99
24. van Kaam AH, Lachmann RA, Herting E, Reducing atelectasis attenuates bacterial growth and translocation in experimental pneumonia : Am J Respir Crit Care Med, 2004; 169(9); 1046-53
25. Wahba RWM, Perioperative functional residual capacity: Can J Anaesth, 1991; 38(3); 384-400
26. Lichtenstein DA, BLUE-protocol and FALLS-protocol: Chest, 2015; 147(6); 1659-70
27. Restrepo RD, Braverman J, Current challenges in the recognition, prevention and treatment of perioperative pulmonary atelectasis : Expert Rev Respir Med, 2014; 9(1); 97-107
28. Bluth T, Serpa Neto AWriting Committee for the PROBESE Collaborative Group of the PROtective VEntilation Network (PROVEnet) for the Clinical Trial Network of the European Society of Anaesthesiology: JAMA, 2019; 321(23); 2292-305
29. Talab HF, Zabani IA, Abdelrahman HS, Intraoperative ventilatory strategies for prevention of pulmonary atelectasis in obese patients undergoing laparoscopic bariatric surgery : Anesth Analg, 2009; 109(5); 1511-16
30. Wong J, Magun BE, Wood LJ, Lung inflammation caused by inhaled toxicants: A review: Int J Chronic Obstr Pulm Dis, 2016; 11; 1391-401
31. Généreux V, Chassé M, Girard F, Effects of positive end-expiratory pressure/recruitment manoeuvres compared with zero end-expiratory pressure on atelectasis during open gynaecological surgery as assessed by ultrasonography: A randomised controlled trial : Br J Anaesth, 2020; 124(1); 101-9
32. Nimmagadda U, Salem MR, Crystal GJ, Preoxygenation: Physiologic basis, benefits, and potential risks: Anesth Analg, 2017; 124(2); 507-17
Figures
Figure 1. Flow diagram of patient screening and enrollment.Figure 2. Lung ultrasound images of 1 representative patient per group. C group – control group; RM group – lung recruitment maneuver group. T1 – before the induction of anesthesia; T2 – at the end of the surgical procedure; T3 – 30 min after extubation.Figure 3. Lung ultrasound score of the total lung area in the control (C) group and lung recruitment maneuver (RM) group at the 3 time points. The data are presented as the median (thick line across the box), interquartile range (box), and range (whiskers). *** P<0.001 (independent-samples Mann-Whitney U test); ns – not significant.Figure 4. Lung ultrasound score of each lung area in the control (C) group and lung recruitment maneuver (RM) group. T2 – at the end of the surgical procedure; T3 – 30 min after extubation. (A) Scores in the 2 groups at T2. (B) Scores in the 2 groups at T3. The data are presented as the median (the thick line across the box), interquartile range (box), and range (whiskers). *** P<0.001 (independent-samples Mann-Whitney U test); ns – not significant. Tables
Table 1. Incidence of atelectasis per group and per protocol step assessed by lung ultrasound.Table 2. Postoperative pulmonary complications.Table 1. Incidence of atelectasis per group and per protocol step assessed by lung ultrasound.Table 2. Postoperative pulmonary complications.Supplementary Table 1. Lung ultrasound (LUS) score.Supplementary Table 2. Demographic data of the enrolled patients.Supplementary Table 3. Intraoperation parameters of the enrolled patients. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387