22 January 2021: Clinical Research
Cross-Cultural Adaptation and Validation of the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians of the Polish Population (MPIIQM-P)
Anna Katarzyna Cygańska1ABCDEFG*, Aleksandra Truszczyńska-Baszak1ADE, Paweł Tomaszewski2CDEDOI: 10.12659/MSM.928038
Med Sci Monit 2021; 27:e928038






Abstract
BACKGROUND: The aim of the study was the cross-cultural adaptation and validation of the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians.
MATERIAL AND METHODS: The process consisted of the following stages: forward translation, backward translation, analysis by committee of experts, pretest of Polish-language version of questionnaire, and cross-cultural validation: psychometric evaluation. In the last step, a convenience sample of 31 professional orchestra musicians (professional experience 16.7±9.5 years) was used to validate the new tool. The primary study outcome measurements were construct validity and internal consistency as measured by exploratory factor analysis (EFA) and Cronbach’s alpha, respectively.
RESULTS: A final Polish version of the questionnaire was developed. Using EFA, the 2-factor structure (pain intensity and pain interference) was obtained, taking into account all 9 items, explaining about 76% of the total variance. The pain interference and pain intensity factors were characterized by high internal consistency (Cronbach’s alpha 0.923 and 0.784, respectively). The lifetime prevalence of playing-related musculoskeletal disorders was 87%.
CONCLUSIONS: Translation and a cross-cultural adaptation of the Polish version of the questionnaire was successfully completed. The results obtained show a correctly carried-out validation process, but further testing of the tool is suggested. The Polish-language version of the validated tool can be used in scientific and clinical practice. The next step would be to estimate cutoff values for severity of health status in orchestra musicians.
Keywords: Musculoskeletal Diseases, Pain Measurement, Physical Therapy Modalities, Questionnaires, Validation Studies, Culturally Competent Care, musculoskeletal pain, Music, Occupational Diseases, Poland, Psychometrics, Reproducibility of Results, Translations
Background
Playing-related musculoskeletal disorders (PRMDs) are a common phenomenon among instrumentalists, and in several studies 73–89.5% of musicians reported pain related to playing an instrument [1–5]. This is reflected in increasingly numerous publications on artists’ health problems, as well as strategies for their prevention and treatment [6–10]. The most frequently analyzed parameter regarding musculoskeletal problems is pain and difficulties associated with playing the instrument [7,11–13].
In the available literature, no standardized Polish-language tools for assessing ailments of this professional group were found. Only the English-language MSK Load and Physical Health Questionnaire for Musicians and Musculoskeletal Pain Questionnaire for Musicians is available [14, 15]. To best assess and monitor the actions taken, Berque et al. [16] indicated the need to develop a standardized tool in this group of patients. The Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians (MPIIQM) is an objective, specific, and standardized questionnaire using the principles set out by the World Health Organization on the basis of the International Classification of Functioning, Disability and Health (ICF) [16]. It was developed as a tool dedicated for professional musicians, taking into account the specificity of the studied group. In creating MPIIQM, Berque et al. [16] used existing English-language questionnaires (Brief Pain Inventory and Disabilities of the Arm, Shoulder, and Hand [DASH] questionnaires), analyzing them and grouping the items in accordance with 3 components of ICF classifications (function, activity, and participation). After creating the MPIIQM questionnaire, it was psychometrically validated, taking into account construct validity, internal consistency, and test-retest reliability. The translation and cross-cultural validation of the German-language version of the MPIIQM questionnaire was completed by Möller et al. [17]. To evaluate construct validity, they used 3 German-language questionnaires (Brief Pain Inventory, Quick DASH, and Fatigue Severity Scale). The authors of the study emphasized the need to use valid and reliable research tools in prevalence studies [16,18,19]. The process of translation, cross-cultural adaptation, and validation of research tools enables the use of the same research tools among populations differing both linguistically and culturally [20–22].
The aim of the study was the cross-cultural adaptation and validation of the MPIIQM, thus providing a professional tool for studying the Polish population of musicians.
Material and Methods
TRANSLATION PROCESS AND CROSS-CULTURAL ADAPTATION:
After obtaining written permission for translation from the authors of the original version of the MPIIQM questionnaire, the process of validating the described tool was undertaken. The consent of the Scientific Research Ethics Committee (SKE 01-37/2017) was also obtained for conducting the research. The study was conducted in accordance with the guidelines of the Helsinki Declaration. The validation process proceeded according to stages based on the guidelines of Guillemin et al. [23] and Beaton et al. [20]. The process consisted of the following stages: forward translation, backward translation, analysis by committee of experts, pretest of Polish-language version of the questionnaire, and cross-cultural validation: psychometric evaluation.
The first stage (forward translation, from English to Polish) was the execution of 4 Polish-language translations by 4 independent translators whose native language was Polish. One of the translators was familiar with the specificity of the translated tool, and the others did not have medical knowledge or were not familiar with the specificity of the translated tool. The second stage (backward translation, from Polish to English) was the execution of 4 English-language translations based on previously developed Polish-language versions of the questionnaire by 4 independent translators whose native language was English. None of the translators had either medical knowledge or knowledge of the specificity of the translated tool, or awareness of the purpose of performing the translation, to obtain the most reliable version [24]. The back translators were blinded to the original version of the questionnaire. The third stage (analysis carried out by a committee of experts) was the development of the prefinal version of the questionnaire on the basis of all translations received (8 in total) and the original version. All aspects and details related to the creation of the prefinal version of the validated tool were discussed by the committee of experts: author AC (physiotherapist; scientist; basic music education) and author AT-B (physiotherapist; scientist) and translators involved in the study (they were language experts and professional translators). The committee of experts focused on preserving semantic, idiomatic, experimental, and conceptual equivalence. The fourth stage, referred to as the pretest, was the preliminary assessment of the developed prefinal version of the questionnaire by 40 professional orchestra musicians. The musicians were asked to fill in the questionnaire and a table provided, to describe their understanding of each item of the questionnaire and add comments. These comments were intended to address comprehensibility, relevance, completeness, clarity, wording, conciseness of the items, and burden for the respondent. The authors then analyzed the results and comments and used this information in designing the final version of the questionnaire. In the third and fourth stages, a written report was completed by the expert committee as a documentation of all decisions and changes for achieving the most accurate version of the translation.
PARTICIPANTS:
Musicians from one of the Polish professional philharmonic orchestras were invited to take part in the study (n=70). The musicians were asked to complete the prepared questionnaire twice with an interval of several days. The inclusion criteria for the study were: age over 18, Polish as the native language, playing in a professional orchestra. Amateur musicians were excluded from the study. All subjects were informed about the purpose and procedure of the study and gave informed consent to participate in the study.
PROCEDURE:
Cross-cultural validation: psychometric evaluation consisted of completing and assessing the psychometric properties of the final version of the questionnaire by a target group of professional musicians. The musicians were asked to complete the prepared questionnaire twice with an interval of several days. Questionnaires were personally distributed and collected by the first author during breaks in rehearsals. During the study, the author was present to provide instructions if necessary.
QUESTIONNAIRE:
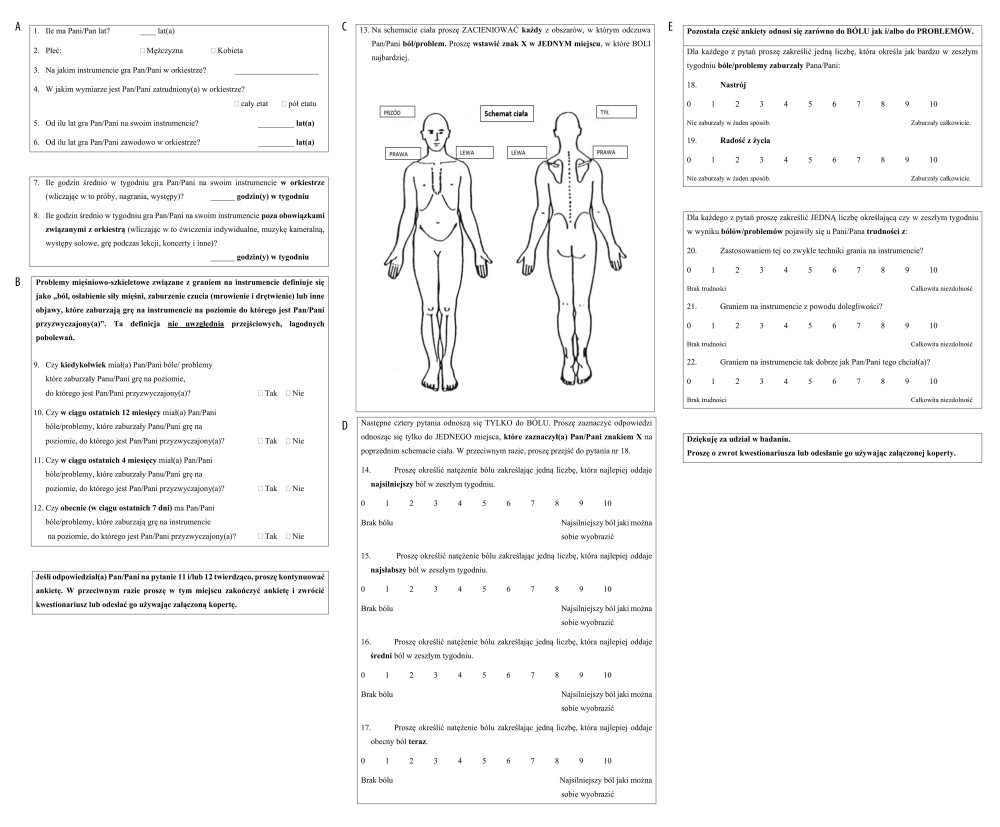
The questionnaire contains 22 items and consists of the following parts: demographic and practice habits (8 items), prevalence periods of PRMD (4 “yes/no” items); item 13 is a body chart for indicating pain location. Items 14 to 17 (pertaining to pain intensity indicated on the body chart) concern pain intensity and items 18 to 22 concern pain interference (pain affective interference and pain activity interference). These questions are measured by a numeric rating scale (from 0 to 10) and can be analyzed as a sum of answers (pain intensity or pain interference) or separate answers.
STATISTICAL ANALYSIS:
Sample size guidelines suggest subject-to-variable ratio of 5: 1 [25] or 10: 1 [26] in studies using exploratory factor analysis (EFA). Therefore, in this study, the EFA on the 9 items would require between 45 and 90 participants.
Descriptive statistics were used, including mean and standard deviation, median, min-max (continuous data), and percentages (categorical data).
Construct validity refers to whether the scores of a test or instrument measure the distinct dimension (construct) they are intended to measure. It determines the dimensions and internal structure of an instrument and reduces its size by removing items that do not show clear contribution to the construct [27]. EFA is a statistical method used to uncover the underlying structure of a relatively large set of variables. In this study EFA with principal axis factoring was used to assess the dimensionality of the MPIIQM. EFA is usually considered a preferable method to principal component analysis (PCA) [26] as it accounts for common variance in the data and not the total variance. This is in contrast to PCA, which is mainly considered a data reduction method [25]. The Kaiser Meyer Olkin (KMO) sampling adequacy test and Bartlett’s sphericity test were applied to determine that the data were suitable to run EFA. KMO values greater than 0.5 indicate that the data are appropriate for EFA and the analysis should produce distinct and reliable factors for the given sample size. A significant Bartlett’s test (P<0.05) shows that a correlation matrix of variables included is not an identity matrix, which indicates that variables are unrelated and therefore unsuitable for structure detection [28]. The number of factors was determined on the basis of the Kaiser criterion (eigenvalue ≥1).
EFA was performed taking into account 9 items of the MPIIQM (4 items related to pain intensity and 5 items about pain interference) among participants who reported the occurrence of current PRMD (n=19). To find the best solution, no rotation, an orthogonal Varimax, and oblique (direct oblimin) rotations were used, as was done in the study of Berque et al. [16]. Factor loadings are correlation coefficients between observed variables and latent common factors; the squared factor loading is the percentage of variance in that variable explained by the factor [28]. The cutoff value for factor loading of 0.4 is considered to meet the minimal level for interpretation of structure [29]; however, factor loading as high as 0.70 is sometimes recommended [30]. In this study a cutoff value of 0.6 for factor loadings was applied to obtain a greater amount of the variable’s total variance attributable to the factor (squared loading) and to partially compensate for small sample size.
Internal consistency was assessed by using Cronbach’s alpha statistics; calculations were performed for each dimension/factor separately [31]. Cronbach’s alpha values exceeding 0.70 were considered adequate [32]. Item-to-total correlations and changes to alpha after individual item deletion were tested [27].
Analyses were performed using SPSS software version 25 (SPSS, Inc., Chicago, Illinois, USA). The level of significance was set at a=0.05.
Results
TRANSLATION PROCESS AND CROSS-CULTURAL ADAPTATION:
While working on the prefinal version of the questionnaire, the expert committee introduced a change because of cultural differences, consisting of adding the “Pan/Pani” honorific (similar to Mr/Ms in English) to items. This form of address is commonly used in Poland both in writing and in speech when addressing someone formally. The committee of experts also encountered several language interpretation difficulties. For clarification purposes certain words were changed or additionally explained. The word “weakness” literally meaning “weakness” was replaced by the words “diminished muscle strength.” The words “numbness and tingling” have no unambiguous equivalent in Polish and the words “sensory disturbance” were used instead, explaining in brackets that it relates to “numbness and tingling.” The words “aches and pains,” also having no equivalent in Polish, were translated as “pain.” However, after evaluating the prefinal version of the questionnaire, the musicians admitted to using the word “ache” more often, which was finally chosen by the committee of experts. While analyzing the results and comments of the musicians regarding the prefinal version of the questionnaire, item no. 4 was also modified because the word “position” in Polish refers to position held at work; the musicians suggested changing it to “working time” because it refers to full- or part-time hours worked. The musicians also suggested that item nos. 7 and 8 do not fully reflect the specifics of work in the profession of orchestra musician, because so-called down times often occur, which, according to them, does not quite reflect the average number of hours per week; however, the committee of experts decided that a change in the content of the item would be an interference with the tool itself and left this item unchanged. This is an interesting issue that is worth exploring in further study. The final version of the MPIIQM-P is presented in Figure 1.
PARTICIPANTS: Thirty-one professional musicians from 1 of the Polish symphony orchestras (n=70), 17 (54.8%) women and 14 (45.2%) men, took part in cross-cultural validation. The response rate was 44% (verified on the basis of the musicians’ attendance at rehearsal, n=70). Subjects’ data are presented in Table 1. Lifetime prevalence of PRMD was 87%, 12-month prevalence was 81%, 1-month prevalence was 71%, point-prevalence was 52%. Twenty-three subjects completed the MPIIQM-P after item 12 (11 or 12 items). Missing scores concerned 4 subjects (lack of some data). Ultimately, 19 participants were included in the EFA. The questionnaire took about 15 min to complete.
EXPLORATORY FACTOR ANALYSIS:
EFA was performed among participants who reported the occurrence of current PRMD (n=19). The value of the KMO coefficient was at an acceptable level (0.703>0.5); also, the Bartlett sphericity test proved to be significant (χ2=114.25;
The results of the EFA conducted without rotation did not return satisfactory results. An easy-to-interpret solution was not obtained; moreover, for 3 of 9 analyzed items (least pain, average pain, and enjoyment of life), the simple factor structure criterion was not met; these items showed quite high factor loadings (>0.5) for both separate factors. After the Varimax rotation, the first factor consisted of 5 items related to the pain interference and, surprisingly, the item “pain right now,” with high factor loadings (≥0.8) for most items. The second factor was formed by the other pain-intensity items (worst pain, least pain, average pain). Since the pain-intensity and pain-interference dimensions are related and therefore are believed to correlate with one another [28], an oblique rotation was performed. Unexpectedly, direct oblimin rotation yielded virtually the same structure as obtained in Varimax rotation and did not result in transfer of the pain-right-now item to factor 2. Table 2 shows the factor loadings after Varimax and oblique rotation (direct oblimin). After Varimax rotation, 7 of 9 items had high communality values (range 0.725–0.867) after separating 2 factors; slightly lower values, although at an acceptable level, were observed for the items average pain and enjoyment of life (0.587 and 0.475, respectively). After oblimin rotation, the communality values ranged from 0.384 (enjoyment of life) to 0.864 (mood). The solution taking into account 2 factors explained about 76% and 73% of the total variance after Varimax and oblimin rotations, respectively. This indicates slightly better estimates for an orthogonal rotation; therefore, the Varimax solution was used in internal consistency analyses.
INTERNAL CONSISTENCY:
The Cronbach’s alpha values obtained for the 6 items making up factor 1 and the 3 items making up factor 2 (Varimax rotation) were 0.923 and 0.784, respectively. For factor 1, the lowest correlation value with the overall score (0.525) was found for the enjoyment-of-life item; removing it resulted in an increase in Cronbach’s alpha value to 0.938. Removing the other items from factor 1, as well as any of the items that settled factor 2, did not increase Cronbach’s alpha value. Cronbach’s alpha for the entire scale consisting of 9 items was 0.923. A dependable analysis of test-retest reliability results based on intraclass correlation coefficient (ICC) values was not possible because of the smaller-than-recommended (n=50) number of people completing the questionnaire again (n=10).
Discussion
This work presents the results of translation, cross-cultural adaptation, and validation of the MPIIQM questionnaire into Polish. This process was based on guidelines [20,23] and preserved semantic, idiomatic, experimental, and conceptual equivalence of the questionnaire. Analysis of the results obtained in the pilot study indicates a correctly carried-out process.
EFA identified 2 factors, pain intensity and pain interference, in the structure of items, similarly to the work by Berque et al. [16] and Möller et al. [17], but with the difference that in this work the pain-right-now item has been included in the pain interference factor, despite using the same rotation procedures. The slightly different structure is thus difficult to interpret and may be due to small sample size used in this study. It is also possible that participants perceived the pain-right-now item as being related to items concerning mood, enjoyment of life, and playing an instrument (items 18–22), as these are based on present symptoms (pain right now). Nevertheless, the resulting structure is largely consistent with the biopsychosocial ICF model, which allows use of this tool both in scientific research and for the clinical evaluation of musicians. At the same time, it shows a high internal consistency of both subscales, measured by the Cronbach’s alpha index (>0.78). In further research, it would be worth examining the population of orchestra musicians to estimate cutoff values so as to facilitate the assessment of changes in the health of the subjects to implement the necessary medical care or preventive measures.
Strengths: The indisputable advantage of the presented work is the creation of the first Polish-language tool for assessing the occurrence of musculoskeletal problems in a group of musicians. The authors validated a standardized questionnaire dedicated to instrumentalists, and the resulting tool shows very good understanding by the respondents. The development of the Polish-language version of the MPIIQM questionnaire will allow for further development of research in this area. It will also allow comparison and analysis of research results with researchers from other language and cultural areas.
Limitations: The presented results should also be analyzed taking into account the limitations of the study. Because of the lack of consent of the respondents to complete several questionnaires, the authors of the study could not compare the results of the newly created tool and thus assess the convergent and divergent validity of the Polish-language MPIIQM questionnaire. The author of the English version was not asked to check the back-translated version. An insufficient number of respondents who returned questionnaires made the test-retest reliability analysis impossible. This seems to be an important aspect that needs to be addressed in further studies. Moreover, the sample size available for EFA (n=19) was considerably smaller than the recommended size (n≥45), which may have affected the stability of the factor pattern [25]. This is probably why the results in this study do not fully correspond to the results presented by Berque et al. [16] and Möller et al. [17]. Therefore, the model needs to be studied again at a later stage with more participants.
Despite the awareness that the interventions are an important element in understanding and treating the health problems of musicians, artists with professional obligations cannot afford to undertake subsequent time-consuming commitments arising from participation in scientific research and are reluctant to participate in research. Other researchers also point to similar difficulties [14,33,34]. The indicated constraints, however, do not diminish the value of the work done, which fills a gap in the existing Polish literature.
Conclusions
Translation and a cross-cultural adaptation of a Polish version of a questionnaire was successfully completed. The results obtained show a correctly carried-out validation process, but further testing of the tool is suggested. The Polish-language version of the validated tool can be used in scientific and clinical practice. The next step would be to estimate cutoff values for severity of health status in orchestra musicians.
References
1. Steinmetz A, Scheffer I, Esmer E, Frequency, severity and predictors of playing-related musculoskeletal pain in professional orchestral musicians in Germany: Clin Rheumatol, 2015; 34; 965-73
2. Viljamaa K, Liira J, Kaakkola S, Musculoskeletal symptoms among Finnish professional orchestra musicians: Med Probl Perform Art, 2017; 32; 195-200
3. Sousa CM, Machado JP, Greten HJ, Occupational diseases of professional orchestra musicians from northern Portugal: A descriptive study: Med Probl Perform Art, 2016; 31; 8-12
4. Jones CM, Griffiths PC, Mellalieu SD, Training load and fatigue marker associations with injury and illness: A systematic review of longitudinal studies: Sports Med, 2017; 47; 943-74
5. Lonsdale K, Boon OK, Playing-related health problems among instrumental music students at a university in Malaysia: Med Probl Perform Art, 2016; 31; 151-59
6. Martín López T, Farías Martínez J, Strategies to promote health and prevent musculoskeletal injuries in students from the high conservatory of music of Salamanca, Spain: Med Probl Perform Art, 2013; 28; 100-6
7. Ioannou CI, Altenmüller E, Approaches to and treatment strategies for playing-related pain problems among Czech instrumental music students: An epidemiological study: Med Probl Perform Art, 2015; 30; 135-42
8. Baadjou VA, Verbunt JA, van Eijsden-Besseling MD, PREvention STudy On preventing or reducing disability from musculoskeletal complaints in music school students (PRESTO): Protocol of a randomised controlled trial: J Physiother, 2014; 60; 232
9. Nawrocka A, Mynarski W, Powerska A, Health-oriented physical activity in prevention of musculoskeletal disorders among young Polish musicians: Int J Occup Med Environ Health, 2014; 27; 28-37
10. Nawrocka A, Mynarski W, Grabara M, Weekday and weekend moderate to vigorous physical activity of young musicians in the context of public health recommendations: Ann Agric Environ Med, 2013; 20; 566-70
11. Jacukowicz A, Psychosocial work aspects, stress and musculoskeletal pain among musicians. A systematic review in search of correlates and predictors of playing-related pain: Work, 2016; 54; 657-68
12. Fotiadis DG, Fotiadou EG, Kokaridas DG, Prevalence of musculoskeletal disorders in professional symphony orchestra musicians in Greece: A pilot study concerning age, gender, and instrument-specific results: Med Probl Perform Art, 2013; 28; 91-95
13. Nawrocka A, Mynarski W, Powerska-Didkowska A, Musculoskeletal pain among Polish music school students: Med Probl Perform Art, 2014; 29; 64-69
14. Lamontagne V, Bélanger C, Development and validation of a questionnaire on musculoskeletal pain in musicians: Med Probl Perform Art, 2012; 27; 37-42
15. Ackermann B, Driscoll T, Development of a new instrument for measuring the musculoskeletal load and physical health of professional orchestral musicians: Med Probl Perform Art, 2010; 25; 95-101
16. Berque P, Gray H, McFadyen A, Development and psychometric evaluation of the Musculoskeletal Pain Intensity and Interference Questionnaire for professional orchestra musicians: Man Ther, 2014; 19; 575-88
17. Möller D, Ballenberger N, Zalpour C, The German version of the musculoskeletal pain intensity and interference questionnaire for musicians (MPIIQM-G): Translation and validation in professional orchestral musicians: Musculoskelet Sci Pract, 2018; 37; 1-7
18. Blanco-Piñeiro P, Díaz-Pereira MP, Martínez A, Musicians, postural quality and musculoskeletal health: A literature’s review: J Bodyw Mov Ther, 2017; 21; 157-72
19. Baadjou VAE, Roussel NA, Verbunt JAMCF, Systematic review: Risk factors for musculoskeletal disorders in musicians: Occup Med (Chic Ill), 2016; 66; 614-22
20. Beaton DE, Bombardier C, Guillemin F, Guidelines for the process of cross-cultural adaptation of self-report measures: Spine (Phila Pa 1976), 2000; 25; 3186-91
21. Sousa VD, Rojjanasrirat W, Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline: J Eval Clin Pract, 2011; 17; 268-74
22. Borsa JC, Damásio BF, Bandeira DRAdaptação e validação de instrumentos psicológicos entre culturas: Algumas considerações: Paid (Ribeirão Preto), 2012; 22; 423-32 [in Portuguese]
23. Guillemin F, Bombardier C, Beaton D, Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines: J Clin Epidemiol, 1993; 46; 1417-32
24. Epstein J, Santo RM, Guillemin F, A review of guidelines for cross-cultural adaptation of questionnaires could not bring out a consensus: J Clin Epidemiol, 2015; 68(4); 435-41
25. De Vellis R: Scale development: Theory and applications, 2012, London, Sage Publications Ltd
26. Costello AB, Osborne J, Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis: Pract Assess Res Eval, 2005; 10; 7
27. De Vet HCW, Terwee CB, Mokkink LB: Measurement in medicine: A practical guide, 2011, Cambridge University Press
28. Field A: Discovering statistics using SPSS, 2012, London, Sage Publications Ltd
29. Floyd FJ, Widaman KF, Factor analysis in the development and refinement of clinical assessment instruments: Psychol Assess, 1995; 7; 286-99
30. Hair J: Multivariate data analysis: A global perspective, 2010, London, Upper Saddle River, NJ: Pearson Education
31. Mokkink LB, Terwee CB, Patrick DL, The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study: Qual Life Res, 2010; 19; 539-49
32. Streiner DL, Norman GR: Health measurement scales: A practical guide to their development and use, 2008, Oxford University Press
33. Berque P, Gray H, McFadyen A, Playing-related musculoskeletal problems among professional orchestra musicians in Scotland: A prevalence study using a validated instrument, the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians (MPIIQM): Med Probl Perform Art, 2016; 31; 79-86
34. Davies J, Mangion S, Predictors of pain and other musculoskeletal symptoms among professional instrumental musicians: Elucidating specific effects: Med Probl Perform Art, 2002; 17; 155-69
Tables
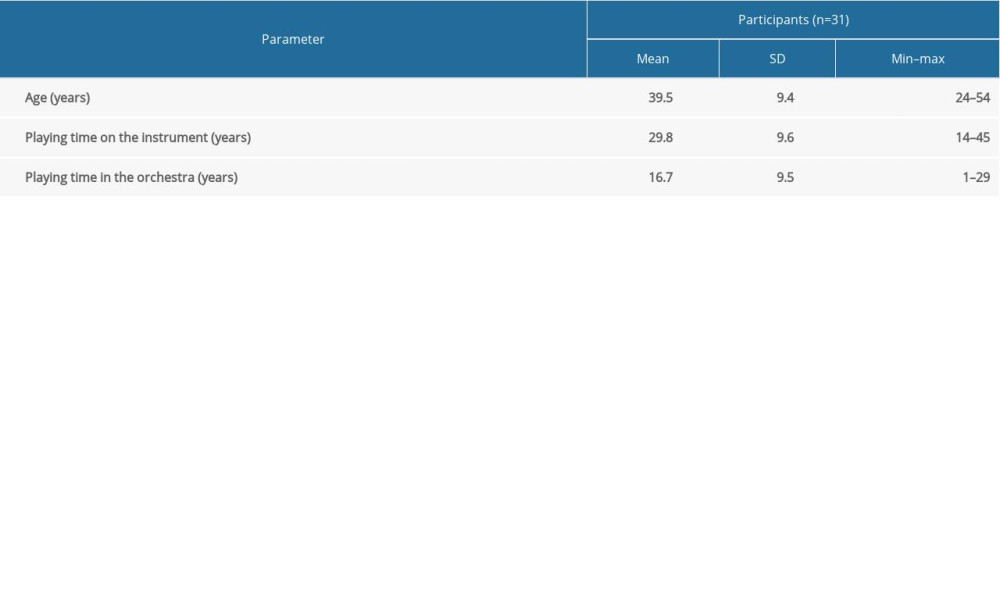 Table 1. Participant characteristics (mean, standard deviation [SD], min–max).
Table 1. Participant characteristics (mean, standard deviation [SD], min–max).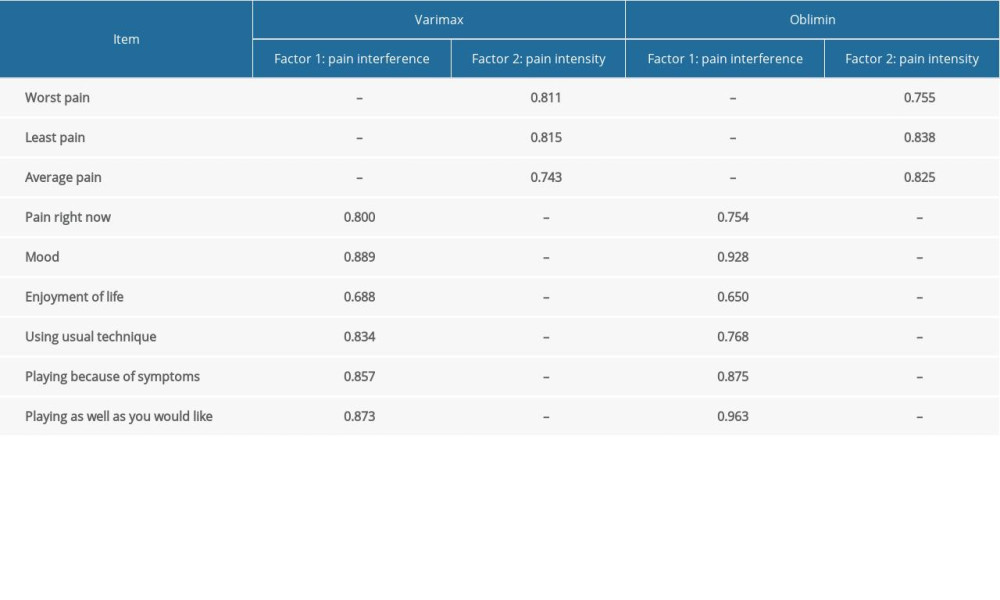 Table 2. Exploratory factor analysis results after Varimax and oblimin rotation. Values represent factor loadings.Table 1. Participant characteristics (mean, standard deviation [SD], min–max).Table 2. Exploratory factor analysis results after Varimax and oblimin rotation. Values represent factor loadings.
Table 2. Exploratory factor analysis results after Varimax and oblimin rotation. Values represent factor loadings.Table 1. Participant characteristics (mean, standard deviation [SD], min–max).Table 2. Exploratory factor analysis results after Varimax and oblimin rotation. Values represent factor loadings. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387