09 February 2021: Clinical Research
Evaluation of Mitral and Aortic Valvular Disease and Left Ventricular Dysfunction in a Lebanese Population: Retrospective Single-Center Experience
Vanessa Nader12ABCDEF, Anthony Matta13ABDEF, Ronan Canitrot1ADEF, Romain Itier1DEF, Pascale Salameh2ACF, Olivier Lairez1EF, Meyer Elbaz1AEF, Michel Galinier1AEF, Rania Azar2ADEF, Jerome Roncalli1ADEF*DOI: 10.12659/MSM.928218
Med Sci Monit 2021; 27:e928218






Abstract
BACKGROUND: Recently, new therapeutic approaches have revolutionized the management of left ventricular dysfunction (LVD) and valvular heart disease (VHD), which are a growing public health problem. In parallel, there are no available epidemiological data about LVD and VHD in developing countries, especially in the Mediterranean area. This retrospective study was conducted at a single center and aimed to evaluate the associations between mitral and aortic valvular disease and left ventricle systolic and diastolic dysfunction in the Lebanese population.
MATERIAL AND METHODS: A retrospective study was conducted of 4520 consecutive patients aged >18 years who were referred to the Cardiovascular Department of Notre Dame de Secours-University Hospital in Jbeil-Lebanon for transthoracic echocardiography between December 2016 and December 2019. The study population was divided into different groups based on types of LVD and VHD. Left ventricle systolic dysfunction was defined as a left ventricle ejection fraction (EF) ≤40%. Statistical analysis was carried out using SPSS software version 20.
RESULTS: VHD and systolic dysfunction were more common in men, whereas diastolic dysfunction was more common in women. Being older than age 65 years and smoking were significantly associated with heart failure with preserved EF, whereas female sex was a significant preventive factor against heart failure with reduced EF. Systemic hypertension was correlated with mitral stenosis and tricuspid regurgitation, whereas diabetes mellitus was associated with tricuspid regurgitation (TR). Smoking and older age also appeared to be associated with aortic stenosis.
CONCLUSIONS: Mitral valve disease (regurgitation and stenosis) was significantly correlated with systolic dysfunction, whereas aortic and mitral regurgitation were associated with diastolic dysfunction. Better monitoring of cardiovascular disease risk factors may lead to a reduced burden of LVD and VHD.
Keywords: Heart Valve Diseases, Risk Factors, Ventricular Dysfunction, Left, Age Factors, Aortic Valve Insufficiency, Diabetes Mellitus, Echocardiography, Hypertension, Lebanon, Mitral Valve Insufficiency, Mitral Valve Stenosis, Smoking, Stroke Volume, Tricuspid Valve Insufficiency, young adult
Background
Cardiovascular disease is a major cause of mortality. The global increase in life expectancy has resulted in a rising incidence of valvular heart disease (VHD) and left ventricular dysfunction (LVD) among populations, and their impacts on health systems constitute a growing public health problem [1].
VHD is damage to any cardiac valve that alters its capacity to fully open or close. LVD is mainly divided into 2 groups: systolic LVD, characterized by a depressed ejection fraction (EF), and diastolic LVD (LVDD), characterized by stiff heart muscles that cause inadequate relaxation. Statistics from published epidemiological data have shown an increasing prevalence of VHD and heart failure in European and American populations, and the trend is expected to continue [2,3]. Moreover, the widespread use of echocardiography – a simple, noninvasive diagnostic tool – has led to discovery of silent cases of VHD and LVD, which suggests that these 2 independent clinical entities progress slowly over time, from an asymptomatic stage to physical disability or sudden death [4–6].
Transthoracic echocardiography is the diagnostic tool recommended for first-line assessment of left ventricle function, valvular stenosis, and regurgitation [7,8]. Quantitative evaluation of left ventricle EF is usually calculated by dividing the stroke volume by the end-diastolic volume. A value ≤40% is defined as left ventricular systolic dysfunction (LVSD) [8,9]. Transesophageal echocardiography is usually performed to grade the severity of valvular stenosis or regurgitation, particularly in patients with heart failure who have regurgitation [7].
Different imaging modalities are integrated into the management of VHD. For example, exercise testing unmasks symptoms, particularly in asymptomatic patients with severe aortic stenosis (AS), and exercise echocardiography identifies the cardiac origin of dyspnea in addition to assessing the prognosis for mitral regurgitation (MR) and AS [8]. Cardiac magnetic resonance imaging is useful in patients with when echocardiogram quality is poor or results are conflicting, and it is the criterion standard imaging modality for evaluating right ventricle function, which is important in cases of tricuspid regurgitation (TR) [8].
In parallel, novel medical and interventional therapeutic approaches recently have revolutionized the management of VHD and LVD, improving the quality of life and survival of patients. However, critically ill patients are not candidates for surgery or standard treatments and they may be unable to afford the new transcatheter therapies [10].
Historically, VHD has been a main cause of and poor prognostic predictor for LVD and it is associated with high rates of morbidity and mortality [11,12]. Given the paucity of epidemiological data in the Mediterranean area and the absence of surveys in Lebanon, cardiology data for that population have been extrapolated from experience in the United States or Europe. Therefore, the aim of the present study, which was retrospective and single-center, was to evaluate associations between mitral valve disease (MVD) and aortic valve disease (AVD) and LVSD and LVDD in the Lebanese population.
Material and Methods
STUDY DESIGN AND POPULATION:
A retrospective, observational, single-center study was conducted of patients referred for transthoracic echocardiography to the Cardiovascular Department of Notre Dame de Secours-University Hospital (NDS-UH), Jbeil-Lebanon between December 2016 and December 2019. All patients aged >18 years who were not known to have or not being followed for LVD and VHD and who underwent echocardiography during the study period were consecutively enrolled. Patients previously diagnosed with rheumatic heart disease, LVD, and/or VHD were excluded. Patients with physiological or insignificant valvular regurgitation and LVSD with mid-range EF (40% to <50%) were excluded so that LVSD and LVDD could be compared. The study population was divided into groups, based on the different types of VHD: 1) AVD (AS or aortic regurgitation [AR]); 2) Mitral valve disease [MVD] (mitral stenosis [MS] or MR); 3) Combined aorto-mitral valve disease and TR; and LVD (LVSD or LVDD).
DATA COLLECTION AND ENDPOINTS:
Echocardiographic studies were performed by the same reference physicians using a General Electric machine. Standard gray-scale and color Doppler images were acquired at a depth of 16 cm in the parasternal (standard long and short axis) and apical views (2- and 4-chamber and apical long axis). The semi-quantitative and quantitative methods recommended by the American Society of Echocardiography were used to assess VHD (regurgitation or stenosis). LVSD was defined as an EF ≤40% and diastolic LVD as an early mitral inflow velocity (E)-to-tissue Doppler mitral annular early diastolic velocity (E’) ratio (E/E’) <8 and EF ≥50%. EF was calculated in the apical view by using Simpson’s biplane method [13]. In the present study, significant VHD was defined as MS or AS of any severity and mild, moderate, or severe MR, AR, or TR. The primary aim was to evaluate the associations between LVD and VHD in a Lebanese population based on echocardiographic criteria. Our study was approved by the Ethics Committees at NDS-UH and written consent for data collection was obtained from the hospital.
STATISTICAL ANALYSIS:
Quantitative data were summarized with means and standard deviations, whereas qualitative data were summarized with counts and percentages. A chi-square test was used during the first step in statistical analysis to assess the differences between the groups. Multivariate logistic regression was performed to investigate the association between each type of VHD and LVD as a dependent variable.
Results
Baseline characteristics of the 4520 patients included in the study are shown in Table 1. Of the patients, 2575 (57%) were men with a mean age of 65.70±38.60 and 1945 (43%) were women with a mean age of 64.87±40.61, 1355 (30%) had arterial hypertension, 1040 (23%) had diabetes mellitus (DM), 1045 (23.1%) had dyslipidemia, and 1900 (42%) were smokers. Nearly half of the studied population (49.2%; 2225/4520) were age >65 years and 50.8% (2295/4520) were age <65 years, with an overall mean age of 63.7 years. Regarding the different types of VHD, AVD was present in 1440 patients (31.9%), of whom 1040 (23%) had AR and 400 (8.9%) had AS. MVD was present in 2110 (46.7%), of whom 2100 (46.5%) had MR and 50 (1.1%) had MS. Aorto-MVD was present in 970 (21.5%) and 1870 (41.4%) had TR. Of the patients, 2705 (59.8%) were diagnosed with diastolic dysfunction and 810 (17.9%) with systolic dysfunction (Table 1). The incidences of LVSD and LVDD in the Lebanese population we studied were 11.9 per 100 person per year and 39 per 100 person per year, respectively.
Considering sex, MR was the most common type of VHD and was equally distributed among men (46.4%) and women (46.5%). However, diastolic dysfunction was more common in women (62% vs 58%) while systolic dysfunction was more common in men (22% vs 12%). No statistically significant association was found between sex and VHD, but being female was positively correlated with diastolic dysfunction (odds ratio [OR]=1.17; 95% confidence interval [CI] 1.04–1.33) and negatively correlated with systolic dysfunction (OR=0.48; CI 0.41–0.57]). The incidence of systolic dysfunction was 8% in women and 14.9% and for diastolic dysfunction, it was 41.4% in women and 38.7% in men.
Regarding age, VHD (52.6% vs 47.4%), diastolic (65% vs 55%), and systolic dysfunction (20% vs 16%) were significantly more common in patients age >65 years compared with those age ≤65 years. MR was the most common VHD in both age groups. Age >65 years was positively correlated with incidence of AS (OR=2.65; CI 2.09–3.37), TR (OR=1.1; 95% CI 1.05–1.3), MS (OR=3.83; 95% CI 1.9–7.7), MR (OR=1.16; 95% CI 1.03–1.3), systolic dysfunction (OR=1.3; 95% CI 1.1–1.5), and diastolic dysfunction (OR=1.4; 95% CI 1.2–1.6). The incidence of systolic dysfunction was 13.5% in patients age >65 years and 10.4% in those ≤65 years, whereas the incidence of diastolic dysfunction was 43% in those age >65 years and 37% in those age ≤65 years.
LVD and VHD were more likely in patients with multiple risk factors. Indeed, multivariate logistic regression showed a positive correlation between smoking and all types of VHD and between systemic arterial hypertension and MS (OR=10.8; 95% CI 3.9 to 29.3) and TR (OR=1.5; 95% CI 1.2 to 1.8). It also showed a negative association between DM and TR (OR=0.55; 95% CI 0.4 to 0.7). Moreover, smoking and arterial hypertension were the 2 CVD risk factors studied that were positively correlated with diastolic dysfunction (OR=1.4; 95% CI 1.2 to 1.7;
Discussion
LIMITATIONS:
The present study has some limitations, in that it was not population-based and it was retrospective, observational, and performed at a single center. Only written medical records and not echocardiograms were reviewed. Data from results of testing for N-terminal pro b-type natriuretic peptide, on use of medication, and for scales reflecting clinical manifestations were not collected for 2 reasons: 1) A large proportion of the patients studied were outpatients, so that information was lacking; and 2) No computerized medical files were available.
Conclusions
The incidence and epidemiological characteristics of LVD in a Mediterranean Lebanese population are similar to those found in patients in Europe. Modifiable CVD risk factors play a significant role in development of LVD and VHD. Our results underscore the need for better management of CVD risk factors to reduce the impact of VHD and LVD on the public health system.
Tables
Table 1. Baseline characteristics of the studied population.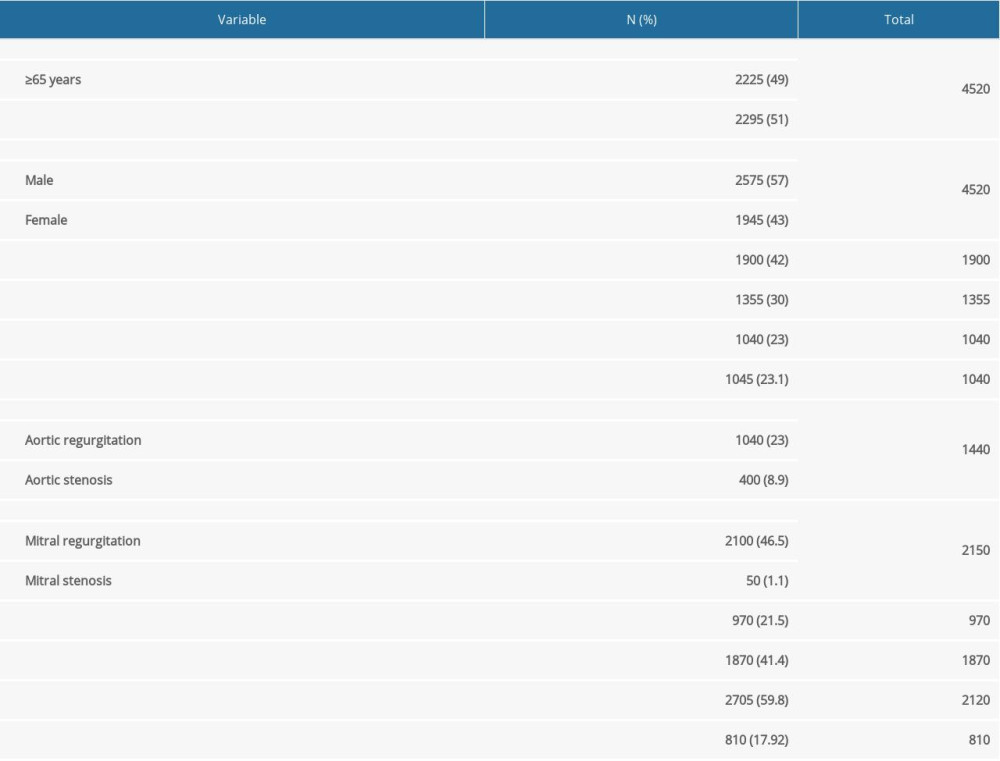 Table 2. Prevalence of valvular heart disease and left ventricular dysfunction according to several cardiovascular risk factors.
Table 2. Prevalence of valvular heart disease and left ventricular dysfunction according to several cardiovascular risk factors.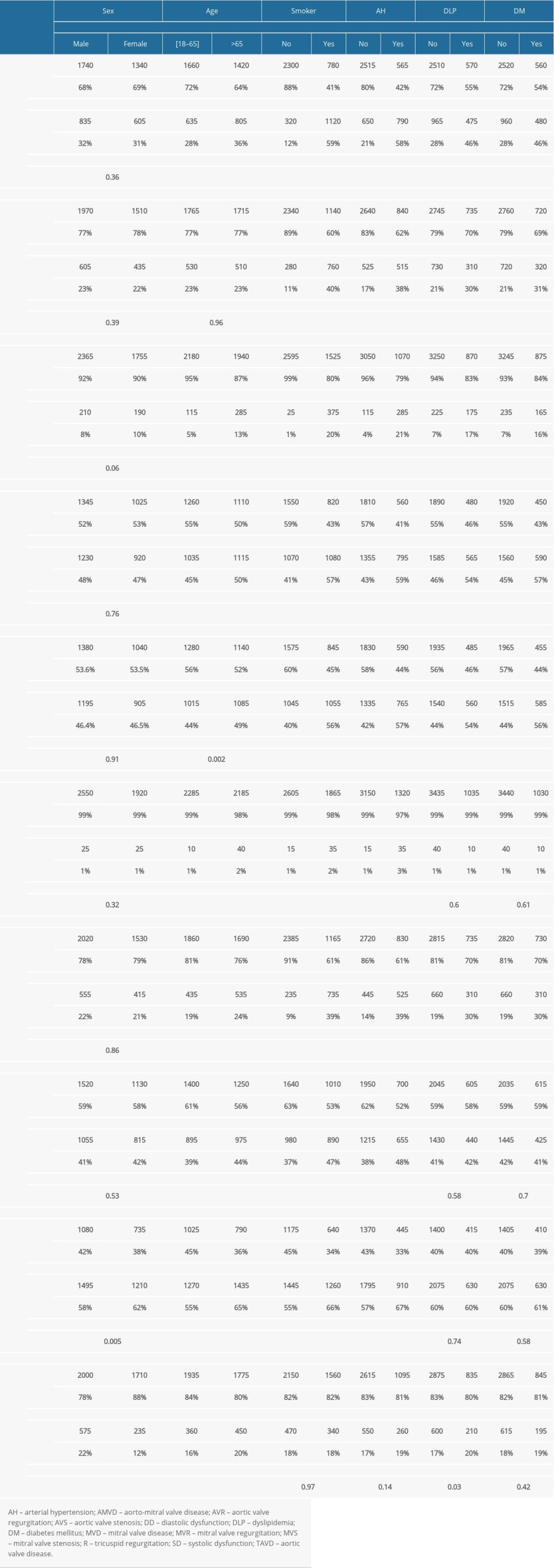 Table 3. Multivariate logistic regression for each type of valvular heart disease and left ventricular dysfunction, with cardiovascular risk factors as independent variables.
Table 3. Multivariate logistic regression for each type of valvular heart disease and left ventricular dysfunction, with cardiovascular risk factors as independent variables.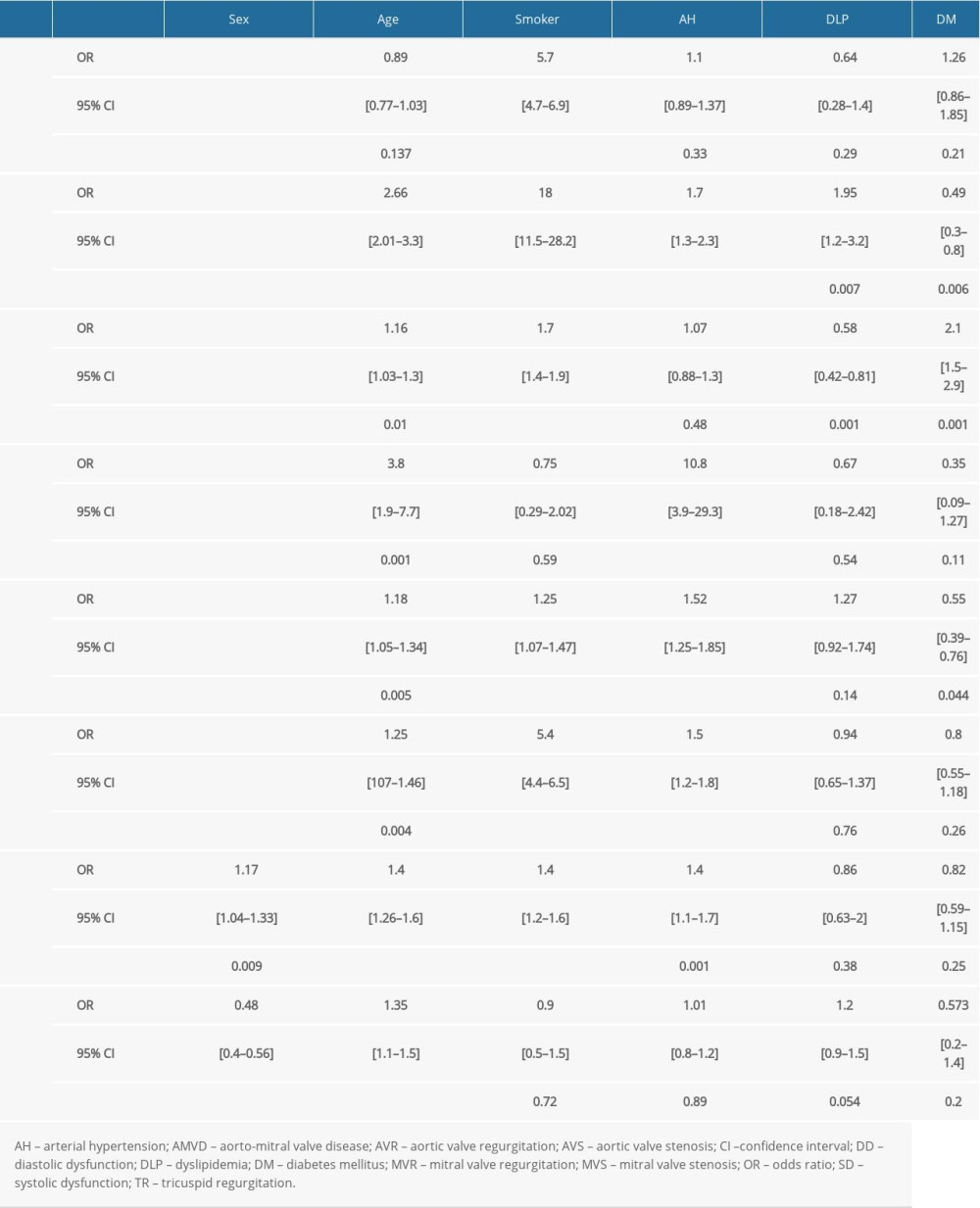 Table 4. Distribution of valvular heart disease according to types of left ventricular dysfunction.
Table 4. Distribution of valvular heart disease according to types of left ventricular dysfunction.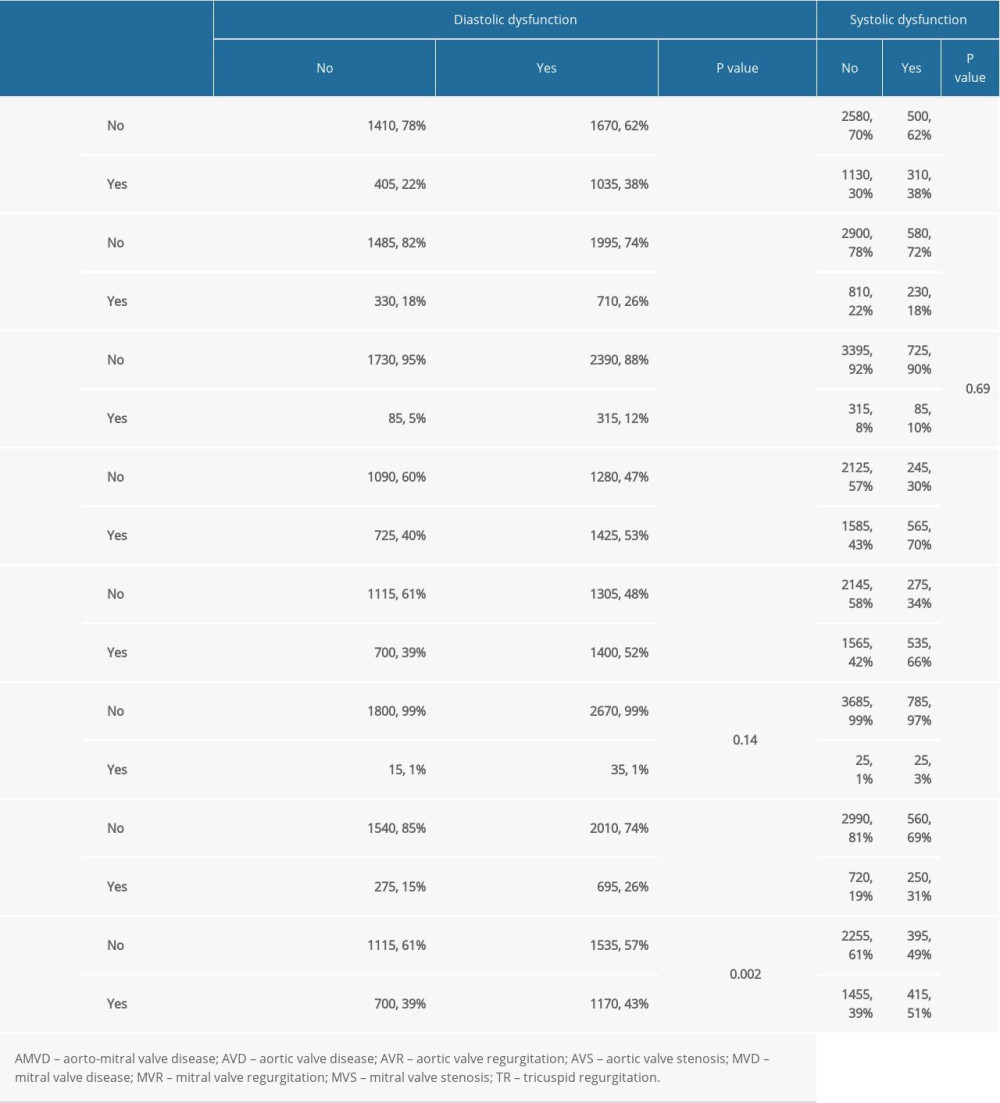 Table 5. Multivariate logistic regression taking using each type of left ventricular dysfunction as a dependent variable and different kinds of valvular heart disease as independent variables.
Table 5. Multivariate logistic regression taking using each type of left ventricular dysfunction as a dependent variable and different kinds of valvular heart disease as independent variables.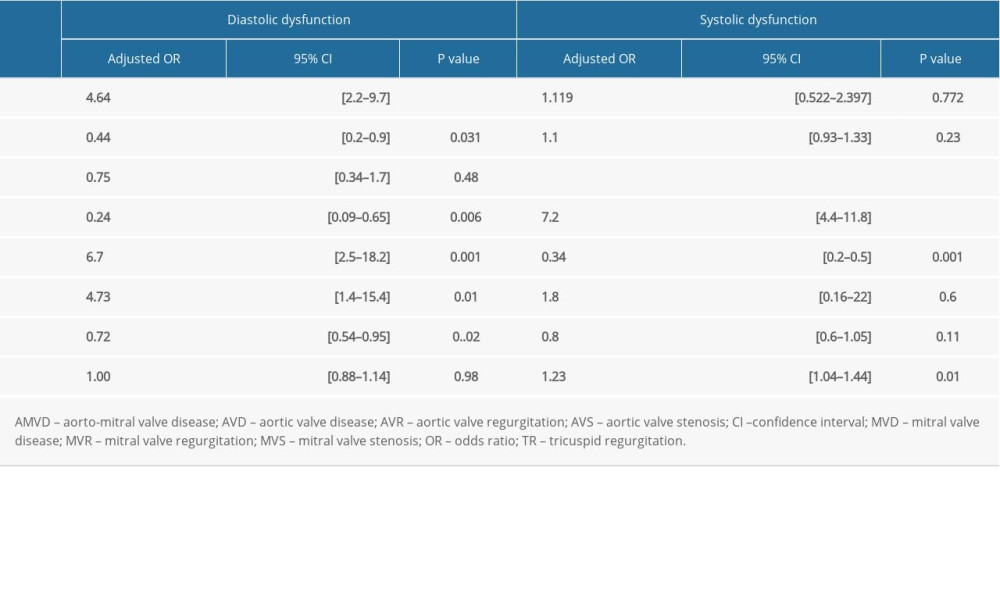
References
1. Supino PG, Borer JS, Yin A, The epidemiology of valvular heart disease: An emerging public health problem: Adv Cardiol, 2002; 39; 1-6
2. Virani S, Alonso A, Benjamin E, Heart disease and stroke statistics – 2020 update: A report from the American heart Association: Circulation, 2020; 141; e139-596
3. Groenewegen A, Rutten FH, Mosterd A, Epidemiology of heart failure: Eur J Heart Fail, 2020; 22; 1342-56
4. Supino PG, Borer JS, Preibisz J, The epidemiology of valvular heart disease: A growing public health problem: Heart Failure Clin, 2006; 2(4); 379-93
5. Reid CL, Anton-Culver H, Yunis C, Prevalence and clinical correlates of isolated mitral, isolated aortic regurgitation, and both in adults aged 21 to 35 years (from the cardia study): Am J Cardiol, 2007; 99(6); 830-34
6. Singh JP, Evans JC, Levy D, Prevalence and clinical determinants of mitral, tricuspid and aortic regurgitation (The Framingham heart study): Am J Cardiol, 1999; 83; 897-902
7. Podlesnikar T, Delgado V, Bax JJ, Imaging of valvular heart disease in heart failure: Card Fail Rev, 2018; 4(2); 78-86
8. Baumgartner H, Falk V, Bax JJESC Scientific Document Group, 2017 ESC/EACTS Guidelines for the management of valvular heart disease: Eur Heart J, 2017; 38; 2739-91
9. Lang RM, Badano LP, Mor-Avi V, Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging: J Am Soc Echocardiogr, 2015; 28(1); 1-39.e14
10. Kodali SK, Velagapudi P, Hahn RT, Valvular heart disease in patients ≥80 years of age: J Am Coll Cardiol, 2018; 71(18); 2058-72
11. Wilson PWF, An epidemiologic perspective of systemic hypertension, ischemic heart disease, and heart failure: Am J Cardiol, 1997; 80; 3-8
12. Mangion JR, Tighe DA, Aortic valvular disease in adults: Postgrad Med, 1995; 98; 127-40
13. Lang RM, Bierig M, Devereux RB, Recommendations for chamber quantification: J Am Soc Echocardiogr, 2005; 18; 1440-63
14. Ponikowski P, Voors AA, Anker S, 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC): Eur Heart J, 2016; 37(27); 2129-200
15. Savarese G, Lund LH, Global public health burden of heart failure: Card Fail Rev, 2017; 3(1); 7-11
16. Boully C, Vidal JS, Guibert Eon behalf of the SFGG study group, National survey on the management of heart failure in individuals over 80 years of age in French geriatric care units: BMC Geriatrics, 2019; 19; 204
17. Saudubray T, Hanslik TPrevalence and management of heart failure in France: National study among general practitioners of the sentinelles network: Rev Med Interne, 2005; 26(11); 845-50 [in French]
18. Van Riet EES, Hoes AW, Wagenaar KP, Epidemiology of heart failure: The prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review: Eur J Heart, 2016; 18; 242-52
19. Kloch-Badelek M, Kuznetsova T, Sakiewicz W, Prevalence of left ventricular diastolic dysfunction in European populations based on cross-validated diagnostic thresholds: Cardiovasc Ultrasound, 2012; 10; 10
20. Shantsila A, Shantsila E, Gill PS, Predictors of diastolic dysfunction in ethnic groups: Observations from the hypertensive Cohort of the Ethnic-Echocardiographic Heart of England screening study (E-ECHOES): J Hum Hypertens, 2018; 32; 477-86
21. Azad N, Kathiravelu A, Minoosepeher S, Gender differences in the etiology of heart failure: A systematic review: J Geriatr Cardiol, 2011; 8(1); 15-23
22. Pomerance A, Pathogenesis of aortic stenosis and its relation to age: Br Heart J, 1972; 34(6); 569-74
23. Sanders D, Dudley M, Groban L, Diastolic dysfunction, cardiovascular aging, and the anesthesiologist: Anesthesiol Clin, 2009; 27(3); 497-517
24. Alshehri A, Azoz A, Shaheen H, Acute effects of cigarette smoking on the cardiac diastolic functions: J Saudi Heart Assoc, 2013; 25(3); 173-79
25. Obeyesekere HI, Dulake M, Demerdash H, Systemic hypertension and mitral valve disease: Brit Med J, 1965; 2; 441-45
26. Rahimi K, Mohseni H, Kiran A, Elevated blood pressure and risk of aortic valve disease: A cohort analysis of 5.4 million UK adults: Eur Heart J, 2018; 39(39); 3596-603
27. Nkomo V, Gardin JM, Skelton TN, Burden of valvular heart diseases: A population-based study: Lancet, 2006; 368(9540); 1005-11
28. Rossi A, Zoppini G, Benfari G, Mitral regurgitation and increased risk of all- cause and cardiovascular mortality in patients with type 2 diabetes: Am J Med, 2017; 130(1); 70-76
29. Marciniak A, Claus P, Sutherland G, Changes in systolic left ventricular function in isolated mitral regurgitation. A strain rate imaging study: Eur Heart J, 2007; 28(21); 2627-36
30. Bilen E, Kurt M, Tanboga IH, Severity of mitral stenosis and left ventricular mechanics: A speckle tracking study: Cardiology, 2011; 119; 108-15
Tables
Table 1. Baseline characteristics of the studied population.Table 2. Prevalence of valvular heart disease and left ventricular dysfunction according to several cardiovascular risk factors.Table 3. Multivariate logistic regression for each type of valvular heart disease and left ventricular dysfunction, with cardiovascular risk factors as independent variables.Table 4. Distribution of valvular heart disease according to types of left ventricular dysfunction.Table 5. Multivariate logistic regression taking using each type of left ventricular dysfunction as a dependent variable and different kinds of valvular heart disease as independent variables. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387