11 January 2021: Clinical Research
Magnetic Resonance Imaging has Better Accuracy in Detecting New-Onset Rib Fractures as Compared to Computed Tomography
Tao Zhang1ABCDEF, Jing Wu1ABCDEF, Yu-Chen Chen1CEF, Xinying Wu1AD, Lingquan Lu1ABCDEF*, Cunnan Mao1ABCDDOI: 10.12659/MSM.928463
Med Sci Monit 2021; 27:e928463






Abstract
BACKGROUND: The aim of this study was to explore the magnetic resonance imaging (MRI) manifestations of new-onset rib fractures and determine the utility of MRI through a comparative study of MRI and computed tomography (CT).
MATERIAL AND METHODS: Twenty-one patients with mild chest trauma who sought medical care from February 2019 to June 2020 were included in this study. The patients were subjected to CT and MRI scanning within 2 weeks after the trauma, and CT rescanning was scheduled 4–8 weeks later to classify rib fractures and determine the diagnostic accuracy of MRI and CT for new-onset rib fractures.
RESULTS: Seventy-seven rib fractures were confirmed by CT rescanning, of which 72 (93.51%) were type I fractures and 5 (6.49%) were type II. MRI identified 76 fractures, of which 3 were false positive, with the diagnostic accuracy rate of 91.25% and sensitivity rate of 94.81%. Among them, type I fractures (n=71, 3 were false positive) showed the MRI “sandwich” sign (heterogeneous high-signal shadow within bone marrow of the inner layer, low-signal bony cortex of the middle layer, and high-signal subperiosteal effusion of the outer layer) in T2-weighted fat-suppressed sequences; type II fractures (n=5) displayed intramedullary high-signal intensities and no subperiosteal effusion. Forty-four fractures (all type I) were discovered in the initial CT examination, and the corresponding diagnostic accuracy rate and sensitivity rate were 57.14%, which were lower than that of MRI.
CONCLUSIONS: MRI is highly sensitive for new-onset rib fractures, especially type I, so it is a preferred method for patients with mild chest trauma.
Keywords: Magnetic Resonance Imaging, Rib Fractures, Tomography, Spiral Computed, Sensitivity and Specificity, Tomography, X-Ray Computed
Background
Approximately 10% of chest trauma patients have rib fractures [1]. Reported morbidity and mortality rates after chest wall injury vary widely, but they clearly increase with age and number of rib fractures [2,3]. In addition, the number of rib fractures is also an important indicator of the degree of disability in forensic examination [4]. Each rib has a complex shape with a diagonal course across numerous CT sections and a twist along its longitudinal axis [5], which makes computed tomography (CT) evaluation of the rib cage a meticulous and time-consuming process if the angle and plane are not appropriate [6]. The use of angulated, thin-section helical CT offers the possibility to obtain several CT sections of any selected rib and to analyze the rib similarly to examination of a long tubular bone. De Maeseneer et al. [7] showed that the section taken along the long axis of the rib, that is, in oblique-axial plane, facilitated detection of rib fractures.
Information obtained from different diagnostic imaging tools is essential in management of chest trauma patients. At present, there is a marked increase in use of chest computed tomography (CT) scans for initial evaluation of patients with chest trauma [8]. However, among various types of rib fractures (unicortical, bicortical, hair-like, and trabecular only), some types are difficult to diagnose on CT [6], especially in cases of occult rib fracture. Despite negative CT findings, when the fracture is suspected and the patient has obvious tenderness points, further examination should be carried out. Magnetic resonance imaging (MRI) has been used frequently in patients with acute musculoskeletal trauma, as it is superior to other radiological modalities such as plain radiography and ultrasonography in revealing bone and soft-tissue lesions [9]. Increasing attention is being devoted to the potential advantage of MRI for detecting occult rib fractures and bone contusion [10–12]. Nevertheless, there were few reports on the application of MRI in cases of new-onset, traumatic rib fractures, and available studies have focused primarily on the application of MRI for detecting stress fractures of the ribs [13,14]. To improve the early detection rate of rib fracture, the present study systematically applied MRI to new-onset thoracic trauma, emphasizing the MRI manifestations of new-onset rib fractures and comparing the diagnostic accuracy and sensitivity of CT and MRI for assessment of new-onset rib fracture. We hypothesized that MRI could be a viable alternative to increase the diagnostic accuracy for new-onset rib fractures.
Material and Methods
PATIENTS:
Twenty-one patients (17 men and 4 women) with mild chest trauma who sought medical care from February 2019 to May 2020 were included. Inclusion criteria were: (a) clear history of chest trauma without obvious signs of complications, (b) the time since trauma less than 2 weeks, and (c) confirmed rib fracture on CT rescanning. Exclusion criteria were: (a) clearly displaced rib fracture, (b) patients cannot hold breath, such as the in elderly and infirm patients, (c) prior history of fractured ribs; (d) history of metastases involving the ribs, (e) a history of metabolic bone diseases, and (f) other patients not suitable for MRI scanning, such as those with heart stents or metal internal fixators. Their mean age was 44.76±9.75 years (range, 27–63 years). The CT scan was performed first and the MRI was completed within 2 weeks after trauma, followed by another CT review 4-8 weeks after the injury. All of the patients were recorded to have a clear medical history of trauma, including 8 cases of traffic accident injury, 8 cases of fight injury, and 5 cases of fall injury. The study was approved by the Hospital Ethics Committee and all of the recruited patients signed an informed consent.
SCANNING METHOD AND TECHNICAL REQUIREMENTS:
All of the patients underwent 128-slice spiral CT scanning (Shanghai Lianying Medical Technology Co., LTD, China). Patients were asked to lift their arms, inhale, and hold their breath during the scan. Scans ranged from the thoracic opening to the lower edge of the 12th rib. The scanning parameters were set as follows: tube voltage of 120 kV, pitch of 1.0875, anode rotation time of 0.5 s, and scan thickness of 5 mm in 5-mm intervals. A bone reconstruction algorithm was employed (window width 1500 HU, window level 550 HU). Axial reconstruction was performed automatically, with the layer thickness of 1.0 mm at 0.8-mm intervals. Thin-slice axial images were sent to a Philips workstation (Ingenia, Philips Medical Systems, Netherlands) for oblique-axial reconstruction. The slice thickness and slice gap were 3 mm, and the reconstruction angle was approximately parallel to the long axis of the rib, to display the target rib on the same plane.
All of the subjects were scanned with a Philips 3.0 T MRI scanner (Ingenia, Philips Medical Systems, Netherlands) and 8-channel phased array abdominal coil in the following 2 sequences in the oblique-axial plane: (1) T2-weighted short-tau inversion recovery (T2-STIR), TR 2182 ms, TE 60 ms, FOV 35.0×42.2 cm, slice thickness: 3 mm, slice gap: 3 mm; Time: 5 min. (2) T2 spectral adiabatic inversion recovery (T2-SPAIR), TR 1100 ms, TE 70 ms, FOV 40.0×35.6 cm, slice thickness: 3 mm, slice gap: 3 mm; breath-holding 3 times for 45 s. The first scan was performed with T2-STIR sequence, and the scanning area stretched from the thoracic opening to the lower edge of the 12th rib. The scope of rib fractures was then determined based on T2-STIR imaging, and T2-SPAIR scanning was performed in the end within the specified scope. Two separate scans could be performed in the case of a larger range.
CLASSIFICATION CRITERIA FOR THE FRACTURE:
The diagnostic criterion for rib fracture was callus formation in the ribs, regardless of whether the cortical bone was broken or not. Rib fractures assessed in this study were divided into 2 types according to the presence of cortical bone fracture during callus formation. Specifically, type I rib fracture (Figure 1A, 1B) showed complete or incomplete cortical fracture with extraosseous and/or intraosseous callus formation. In contrast, type II fracture (Figure 2A, 2B) had an intact cortical bone with intraosseous callus formation, indicating the occurrence of trabecular microfracture without involving the cortical bone.
IMAGE ASSESSMENT AND STATISTICAL ANALYSIS:
All of the images were read and analyzed independently by 2 experienced radiologists, and only oblique-axial images were observed. To limit recall bias, the radiologists had to make the diagnosis without knowing the patient’s information and the result of CT rescanning and in at least a 1-week interval between initial CT and MRI. In case of disagreements, the senior chief physician was consulted to make the final diagnosis.
The results of CT rescanning were used as the criterion standard to calculate the diagnostic accuracy and sensitivity of MRI and the initial CT for new-onset rib fractures. The diagnostic accuracy is the proportion of the correct diagnosis in the total number of cases, and the sensitivity is the probability of positive diagnosis in the patients. SPSS 19.0 software was used for statistical analysis. Fisher’s exact test was conducted on the number of fractures detected by MRI and the initial CT examination.
Results
Seventy-seven rib fractures were confirmed by CT rescanning. They consisted of type I (n=72, 93.51%) and type II (n=5, 6.49%) fractures. Type I rib fractures showed complete or incomplete cortical fracture with extraosseous and/or intraosseous callus formation (Figure 1C), whereas type II had an intact cortical bone with intraosseous callus formation (Figure 2C).
Initial CT discovered 44 fractures (all type I fractures) with corresponding diagnostic accuracy and sensitivity rate of 57.14%. Of the discovered 44 fractures, 9 showed a complete fracture of the cortex, and 35 showed protrusion, depression, or fracture of the bone cortex unilaterally (Figure 1D). Type II fractures were all negative on the initial CT (Figure 2D).
MRI identified 76 fractures, of which 3 were false positive and 4 were false negative, with the diagnostic accuracy rate of 91.25% and sensitivity rate of 94.81%. Among them, cases with the type I fracture (n=71, 3 were false positive) showed the “sandwich” sign in T2-STIR and T2-SPAIR sequences (Figure 1E, 1F). Specifically, there was a heterogeneous high-signal shadow within bone marrow of the inner layer, low-signal bone cortex of the middle layer, and high-signal subperiosteal effusion of the outer layer. Type II fracture (n=5) displayed intramedullary high-signal intensities and no subperiosteal effusion in T2-STIR and T2-SPAIR sequences (Figure 2E, 2F). The diagnostic rate was the same in T2-STIR and T2-SPAIR sequences.
Compared with the results of CT rescanning, the diagnostic accuracy and sensitivity rate of MRI for new-onset rib fractures were significantly higher than on the initial CT. There was a significant difference in the diagnosis results of the 2 inspection methods by Fisher’s exact test (
Discussion
In recent years, CT has been a preferred examination method for patients with chest trauma. However, missed diagnosis of rib fracture remains a common problem in hospitals [15]. In China, most patients with rib fracture are involved in the determination of criminal responsibility and compensation, and the number of fractures is directly related to the amount of compensation. In particular, the number of rib fractures in cases of fights has a significant bearing on the qualification of the case. In this regard, it is necessary to determine the presence of rib fractures early and to record the number of fractures.
Previously, traumatic rib fractures were mainly divided into the complete or incomplete types [16] or the displaced and non-displaced types [17]. These types were mainly classified according to the cortical changes on CT imaging; however, early CT examination of occult rib fracture is negative, suggesting that those classifications are not suitable for the present study. Here, a new classification was proposed, in which type I rib fracture was defined as complete or incomplete cortical fracture with extraosseous and/or intraosseous callus formation. The fracture of bone cortex causes subperiosteal effusion, and the fracture of trabecular bone induces bone marrow hemorrhage and edema. Nevertheless, the early CT examination may be negative [18], which could be related to diverse fracture morphologies and low brightness of the fracture plane. Type II fracture shows an intact cortical bone layer and there is intraosseous callus formation, which indicates that the trabecular bone had microfractures. Hence, only hemorrhage and edema occurred in the bone marrow in the early stage of injury. Some scholars [19] suggested the trabecular microfracture as a sign of bone contusion. However, we think it is an intraosseous fracture, belonging to a special occult fracture type.
CT can evaluate the integrity of bone cortex, the existence of soft-tissue mass, and the location and form of fracture fragments, while offering a clear image, high resolution, and fast scanning. There are many kinds of reconstruction methods of CT, such as multiplanar reformatting (MPR), volume rendering (VR), and curved planar reformatting (CPR). Because the transverse sections obtained with standard CT technique are oblique with regard to both the long and the short axes of the rib, interpretation may be difficult. As early as 2004, some scholars [7] proposed that the use of angulated thin-section helical CT offered the possibility to obtain several CT sections of any selected rib and to analyze the rib. In this way, the ribs can be viewed as if one is looking at a long tubular bone, and imaging abnormalities can be better analyzed than the transverse sections. We think the usage of angulated thin-section helical CT was the early application of oblique-axial reconstruction. Therefore, the oblique-axial reconstruction, a form of MPR displaying the most of the rib on the same inclined plane by adjusting its angle, was used to visually demonstrate the position, shape, and number of fractures in this study. However, CT exposes patients to radiation, and, even more important, the initial CT may result in missed diagnosis of rib fractures [20] as it cannot display occult fractures.
Compared with CT, the major advantages of MRI include excellent soft-tissue contrast, high spatial resolution, and lack of ionizing radiation [21]. In this group of patients, the diagnostic rate of MRI for rib fracture was evidently higher than that of CT. Admittedly, MRI is not as clear as CT in imaging of the fracture morphology. However, MRI can evaluate the damage status of the cortical and trabecular bone based on indirect signs such as subperiosteal effusion and bone marrow edema, respectively. MRI has significant advantages in the early diagnosis of occult fractures and is the optimal choice for examining occult fractures [11]. However, MRI imaging of rib injury is not applied routinely in the clinical setting, and the diagnosis may be affected by artifacts related to respiration [17]. Thus, it is necessary to inform patients to hold their breath to reduce the breathing artifacts. MRI also has some disadvantages. MRI examination is time-consuming, and in emergency cases, such as patients with pneumothorax, doctor should actively deal with complications instead of performing MRI examination. When undergoing MRI examination, we need to place a certain weight of the abdominal coil on the patient’s chest, which may aggravate the pain caused by the rib fractures, so it is not suitable for patients with severe chest trauma. In addition, MRI is not appropriate for some patients who cannot hold their breath well.
Considering the special direction of the ribs and the application of oblique-axical section in CT, the oblique-axial scanning was adopted in MRI to show the morphology of a rib at the same level, which would be conducive to observing the change of rib signal intuitively. In our study, the T2-STIR sequence, which is a fat-suppression sequence with low requirements for field strength, was applied first. Scanning with a large field of view can achieve both good a fat-suppression effect [22] and a full scanning range covering 12 pairs of ribs. Moreover, it allows patients to breathe freely during the process. In this context, we chose T2-SPAIRsequence – a sequence that can both clearly display a high signal of bone marrow edema and suppress a high signal of fat in the bone marrow – for the second scan, and scanning areas were designated according to abnormal signals in T2-STIR sequence. This sequence required patients to hold their breath 3 times for 15 s each time. Fractures of larger scopes could be scanned in 2 divided areas. Therefore, it took much less time than T2-STIR sequence. In our study, however, no significant difference in the diagnosis of fractures was found between the 2 sequences. Importantly, in terms of image definition, T2-STIR sequence provided a clear display of the abnormal signal caused by fracture, and was superior to T2-SPAIR sequence in the definition of imaging the surrounding soft-tissue structure. Khurana et al. [23] suggested that a single T2-STIR sequence was sufficient to enable detection of radiographically occult fractures. Accordingly, we suggest that the single T2-STIR sequence with oblique-axial scanning is sufficient for the diagnosis of rib fracture in patients with chest trauma.
There were 3 false positives in this group of patients, all of which were misdiagnosed as type I fractures. Analysis of the reasons found that this kind of misdiagnosis was located on the same side of the injury and appeared around the next rib next to the fracture. It may be because the patient’s injured area was large and the edema was severe, causing the edema to spread around the normal ribs, which was mistaken for subperiosteal effusion. In addition, the inappropriate scanning angle caused the counting error, and the intercostal soft-tissue edema was mistakenly judged as bone marrow edema of the lower rib. In this case, careful counting should be performed according to the low-signal costal cartilage, which can greatly reduce the misdiagnosis rate.
Of the 4 undiscovered fractures, 2 were located on the fifth anterior rib on the left. The main reason was that the heartbeat artifacts were serious, resulting in poor image quality. The other 2 were located on the 11th and 12th posterior ribs on the left. The 2 ribs were relatively short, and the surrounding soft-tissue swells lead to signal disturbance, which affects the doctor’s judgment and caused a missed diagnosis.
It is worth noting that due to the inhomogeneity of the magnetic field, some patients have high signal shadows at the front of the ribs near the costal cartilage. Unlike the fracture signal, the signal is uniform and bilaterally symmetrical, and there was no subperiosteal effusion.
This study had some limitations. First, due to the limited sample size of type II fractures, we cannot completely confirm the conclusion that MRI is a more effective tool for diagnosis of type II rib fractures. Hence, we will continue adding patients to validate our findings in a larger cohort. Second, to shorten the examination time, T1-weighted sequence was not used in the study, which resulted in inability to distinguish hemorrhage from edema. Therefore, in the subsequent study, we will add this sequence appropriately without affecting the health of the patients. Third, fracture types were limited to patients with mild chest trauma, because MRI is not recommended for patients with severe trauma. Accordingly, another major limitation of MRI is use in patients with severe trauma, which limits the applicability of the findings of this study to a certain extent during emergencies.
Conclusions
MRI has high sensitivity and accuracy for assessing new-onset rib fracture, especially type I, and can clearly show bone marrow edema and subperiosteal effusion, which may facilitate the identification of the damaged cortical and trabecular bone, respectively, especially in T2-STIR sequence. Therefore, MRI is a preferred method for patients with mild chest trauma without obvious signs of complications.
Figures
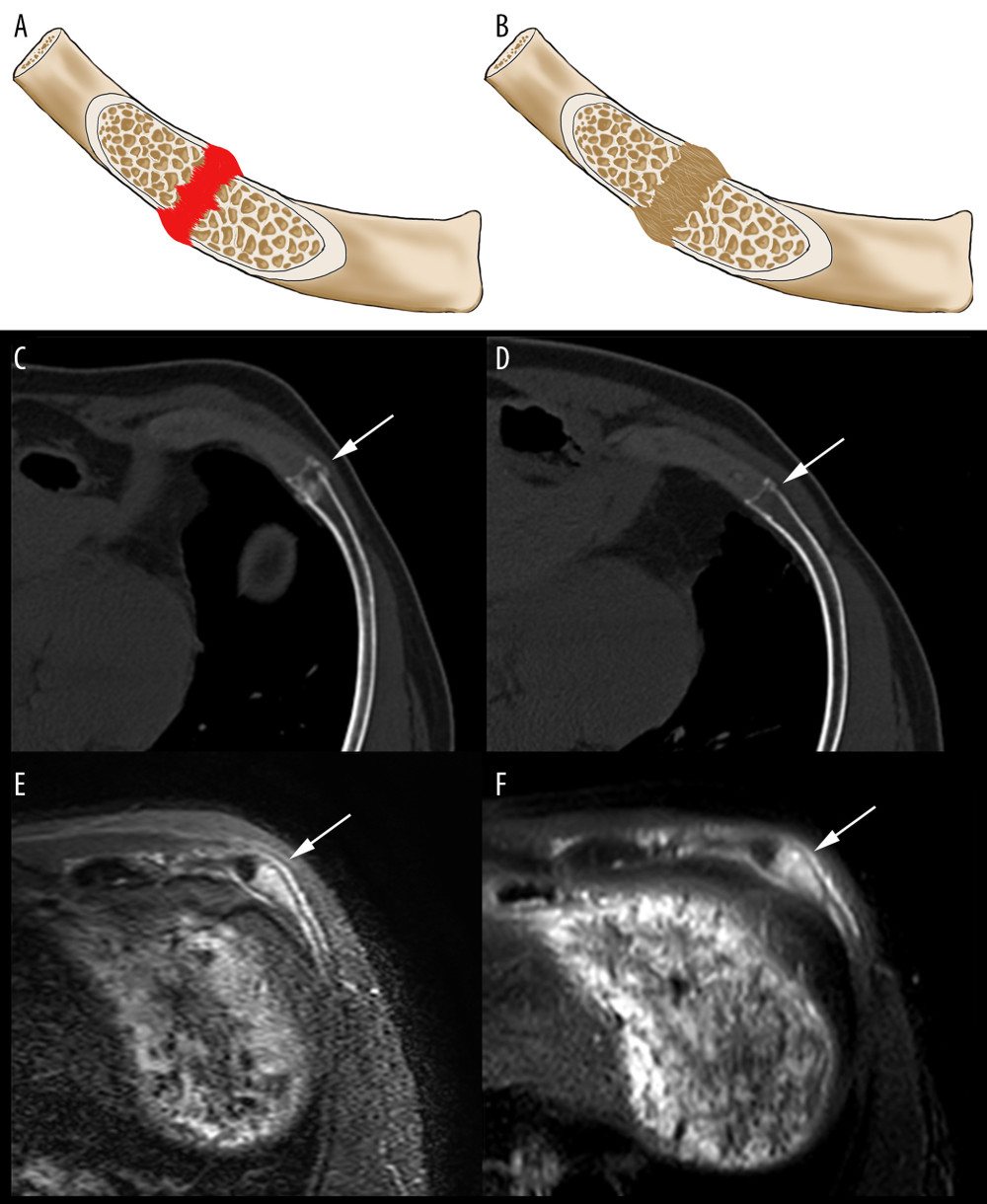 Figure 1. A 40-year-old male patient, admitted to the Thoracic Surgery Department after a traffic accident, was found to have a type I rib fracture. (A, B) Schematic diagram of type I fracture in the inflammatory stage and the callus-forming stage. (C) At 32 days after the trauma, the left seventh rib fracture with callus formation (arrow) was observed in the CT rescanning; oblique-axial plane. (D) Two days after the trauma, a cortical fracture of the left seventh rib (arrow) was observed in the initial CT. (E, F) Two days after the trauma, the corresponding rib fractures showed “sandwich” signs (arrow) on MRI T2-STIR and T2-SPAIR sequences with oblique-axial scanning.
Figure 1. A 40-year-old male patient, admitted to the Thoracic Surgery Department after a traffic accident, was found to have a type I rib fracture. (A, B) Schematic diagram of type I fracture in the inflammatory stage and the callus-forming stage. (C) At 32 days after the trauma, the left seventh rib fracture with callus formation (arrow) was observed in the CT rescanning; oblique-axial plane. (D) Two days after the trauma, a cortical fracture of the left seventh rib (arrow) was observed in the initial CT. (E, F) Two days after the trauma, the corresponding rib fractures showed “sandwich” signs (arrow) on MRI T2-STIR and T2-SPAIR sequences with oblique-axial scanning. 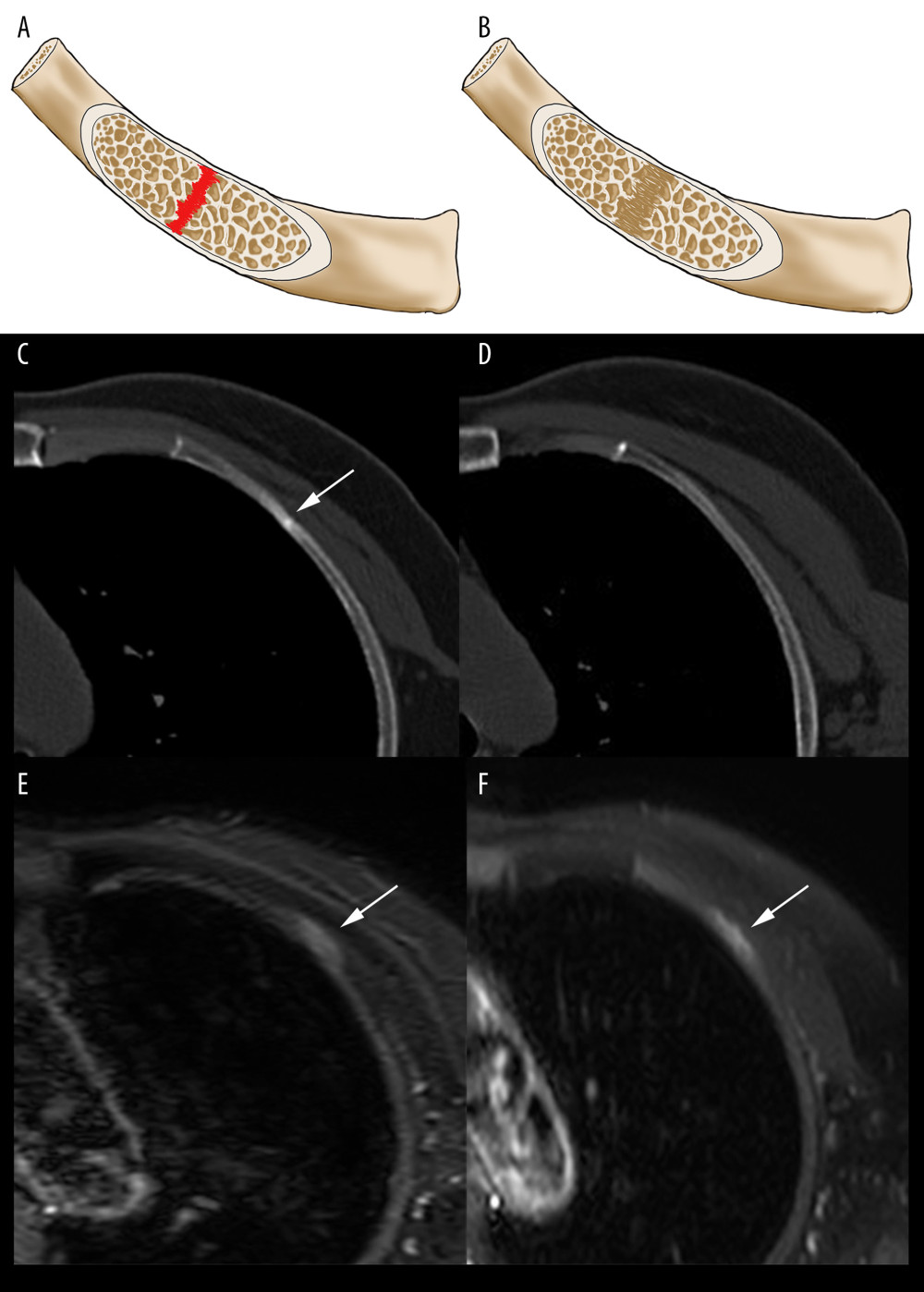 Figure 2. A 51-year-old female patient, admitted to the Emergency Department after a traffic accident, was found to have a type II rib fracture. (A, B) Schematic diagram of type I fracture in the inflammatory stage and the callus-forming stage. (C) At 33 days after the trauma, intraosseous callus formation (arrow) in the left third rib and no obvious cortical fracture were observed in the CT rescanning, oblique-axial plane. (D) On the day of the trauma, CT scanning revealed no obvious abnormalities of the third rib. (E, F) MRI 2 days after the trauma showed intramedullary high-signal intensities (arrow) on T2-STIR and T2-SPAIR sequences with oblique-axial scanning.
Figure 2. A 51-year-old female patient, admitted to the Emergency Department after a traffic accident, was found to have a type II rib fracture. (A, B) Schematic diagram of type I fracture in the inflammatory stage and the callus-forming stage. (C) At 33 days after the trauma, intraosseous callus formation (arrow) in the left third rib and no obvious cortical fracture were observed in the CT rescanning, oblique-axial plane. (D) On the day of the trauma, CT scanning revealed no obvious abnormalities of the third rib. (E, F) MRI 2 days after the trauma showed intramedullary high-signal intensities (arrow) on T2-STIR and T2-SPAIR sequences with oblique-axial scanning. 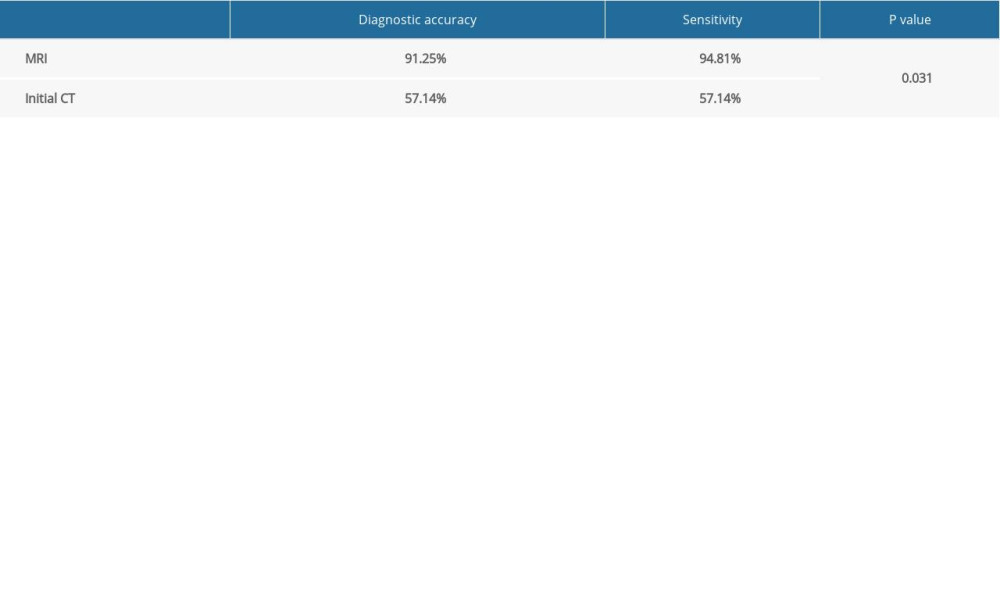
References
1. Henry TS, Donnelly EF, Boiselle PMExpert Panel on Thoracic Imaging: J Am Coll Radiol, 2019; 16(5S); S227-34
2. Mai HT, Tran TS, Ho-Le TP, Low-trauma rib fracture in the elderly: Risk factors and mortality consequence: Bone, 2018; 116; 295-300
3. Bemelman M, Baal MV, Raaijmakers C, An interobserver agreement study with a new classification for rib fractures: Chirurgia, 2019; 114(3); 352-58
4. Jin L, Ge X, Lu F, Low-dose CT examination for rib fracture evaluation: A pilot study: Medicine, 2018; 97(30); e11624
5. Ringl H, Lazar M, Topker M, The ribs unfolded – a CT visualization algorithm for fast detection of rib fractures: Effect on sensitivity and specificity in trauma patients: Eur Radiol, 2015; 25(7); 1865-74
6. Urbaneja A, De Verbizier J, Formery AS, Automatic rib cage unfolding with CT cylindrical projection reformat in polytraumatized patients for rib fracture detection and characterization: Feasibility and clinical application: Eur J Radiol, 2019; 110; 121-27
7. De Maeseneer M, De Mey J, Lenchik L, Helical CT of rib lesions: A pattern-based approach: Am J Roentgenol, 2004; 182(1); 173-79
8. Chardoli M, Hasan-Ghaliaee T, Akbari H, Rahimi-Movaghar V, Accuracy of chest radiography versus chest computed tomography in hemodynamically stable patients with blunt chest trauma: Chin J Traumatol, 2013; 16(6); 351-54
9. Henninger B, Kaser V, Ostermann S, Cervical disc and ligamentous injury in hyperextension trauma: MRI and intraoperative correlation: J Neuroimaging, 2020; 30(1); 104-9
10. Pejic A, Hansson S, Rogmark C, Magnetic resonance imaging for verifying hip fracture diagnosis why, when and how?: Injury, 2017; 48(3); 687-91
11. Haubro M, Stougaard C, Torfing T, Overgaard S, Sensitivity and specificity of CT- and MRI-scanning in evaluation of occult fracture of the proximal femur: Injury, 2015; 46(8); 1557-61
12. Baker JC, Hoover EG, Hillen TJ, Subradiographic foot and ankle fractures and bone contusions detected by MRI in elite ice hockey players: Am J Sports Med, 2016; 44(5); 1317-23
13. Knesek M, Walsh CP, Sabb B, Bedi A, Magnetic resonance imaging diagnosis of rib fracture in a competitive collegiate rower: A case report: JBJS Case Connect, 2012; 2(4); e56
14. Gerrie BJ, Harris JD, Lintner DM, McCulloch PC, Lower thoracic rib stress fractures in baseball pitchers: Phys Sportsmed, 2016; 44(1); 93-96
15. Cho SH, Sung YM, Kim MS, Missed rib fractures on evaluation of initial chest CT for trauma patients: Pattern analysis and diagnostic value of coronal multiplanar reconstruction images with multidetector row CT: Br J Radiol, 2012; 85(1018); e845-50
16. Kani KK, Mulcahy H, Porrino JA, Chew FS, Thoracic cage injuries: Eur J Radiol, 2019; 110; 225-32
17. Talbot BS, Gange CP, Chaturvedi A, Traumatic rib injury: Patterns, imaging pitfalls, complications, and treatment: Radiographics, 2017; 37(2); 628-51
18. Khung S, Masset P, Duhamel A, Automated 3D rendering of ribs in 110 polytrauma patients: Strengths and limitations: Acad Radiol, 2017; 24(2); 146-52
19. Pedersen DR, El-Khoury GY, Thedens DR, Bone contusion progression from traumatic knee injury: association of rate of contusion resolution with injury severity: Open Access J Sports Med, 2017; 8; 9-15
20. Sano A, Rib radiography versus chest computed tomography in the diagnosis of rib fractures: Thorac Cardiovasc Surg, 2018; 66(8); 693-96
21. Karantanas AH, What’s new in the use of MRI in the orthopaedic trauma patient?: Injury, 2014; 45(6); 923-33
22. Heynen B, Tamigneaux C, Pasoglou V, MRI detection of radiographically occult fractures of the hip and pelvis in the elderly: Comparison of T2-weighted Dixon sequence with T1-weighted and STIR sequences: Diagn Interv Imaging, 2019; 100(3); 169-75
23. Khurana B, Okanobo H, Ossiani M, Abbreviated MRI for patients presenting to the emergency department with hip pain: Am J Roentgenol, 2012; 198(6); W581-88
Figures
Figure 1. A 40-year-old male patient, admitted to the Thoracic Surgery Department after a traffic accident, was found to have a type I rib fracture. (A, B) Schematic diagram of type I fracture in the inflammatory stage and the callus-forming stage. (C) At 32 days after the trauma, the left seventh rib fracture with callus formation (arrow) was observed in the CT rescanning; oblique-axial plane. (D) Two days after the trauma, a cortical fracture of the left seventh rib (arrow) was observed in the initial CT. (E, F) Two days after the trauma, the corresponding rib fractures showed “sandwich” signs (arrow) on MRI T2-STIR and T2-SPAIR sequences with oblique-axial scanning.Figure 2. A 51-year-old female patient, admitted to the Emergency Department after a traffic accident, was found to have a type II rib fracture. (A, B) Schematic diagram of type I fracture in the inflammatory stage and the callus-forming stage. (C) At 33 days after the trauma, intraosseous callus formation (arrow) in the left third rib and no obvious cortical fracture were observed in the CT rescanning, oblique-axial plane. (D) On the day of the trauma, CT scanning revealed no obvious abnormalities of the third rib. (E, F) MRI 2 days after the trauma showed intramedullary high-signal intensities (arrow) on T2-STIR and T2-SPAIR sequences with oblique-axial scanning. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387