22 January 2021: Animal Study
Evaluation of Demineralized Bone Matrix Particles Delivered by Alginate Hydrogel for a Bone Graft Substitute: An Animal Experimental Study
Zhiqiang Yang1ABCDEF, Lingfei Xiao1BDF, Zhouming Deng1AC, Lin Cai1AG, Yuanlong Xie1ACDEF*DOI: 10.12659/MSM.928617
Med Sci Monit 2021; 27:e928617






Abstract
BACKGROUND: Our objective was to explore a synthetic alginate hydrogel delivery system for the delivery of demineralized bone matrix (DBM) particles for bone graft substitutes.
MATERIAL AND METHODS: The physiochemical properties of surface morphology, porosity measurements, in vitro degradation, equilibrium swelling, and mechanical testing of combined DBM powder and alginate in amounts of 0 mg/1 mL, 25 mg/1 mL, 50 mg/1 mL, and 100 mg/1 mL were detected. In vitro cell culture and in vivo studies using Sprague-Dawley rats were performed to evaluate the biocompatibility and osteoinductivity of DBM-alginate (ADBM) composites.
RESULTS: DBM particles were uniformly scattered in all composites, and macro-scale pores were omnipresent. All composites showed a similar low degradation rate, with approximately 85% of weight remaining after 15 days. As the concentration of DBM particles in composites increased, degradation in collagenase and elastic modulus increased and the pore area and swelling ratio significantly decreased. No cytotoxicity of ADBM or alginate on mesenchymal stem cells (MSCs) was observed. Cell cultivation with ADBM showed greater osteogenic potential, evidenced by the upregulation of alkaline phosphatase and alizarin red staining activity and the mRNA expression level of marker genes RUNX2, OCN, OPN, and collagen I compared with the cells grown in alginate. Evaluation of ectopic bone formation revealed the osteoinductivity of the ADBM composites was significantly greater than that of DBM particles. Osteoinduction of the composites was demonstrated by a cranial defect model study.
CONCLUSIONS: The delivery of DBM particles using a synthetic alginate hydrogel carrier may be a promising approach in bone tissue engineering for bone defects.
Keywords: Alginates, Bone Demineralization Technique, Bone Substitutes, Bone Matrix, Hydrogels, Tissue Engineering
Background
Patients with bone loss and defects caused by trauma and genetic disorders require surgical intervention, especially when the bone defects exceed a critical size [1]. Although autogenous bone grafts are currently regarded to be the criterion standard for the treatment of bone defects, they are limited by graft availability, risk of donor site morbidity, and difficulty in molding to the defect [2]. Demineralized bone matrix (DBM), which mainly contains collagen and bone morphogenetic proteins (BMPs), is a promising bone graft material, which has been used for the enhancement treatment of bone defects since the 1960s [3,4]. DBM, in the most osteoinductive form with a maximum surface area, can facilitate the interaction with the humoral substance and targeting cells at the graft site. Nevertheless, the clinical application of DBM powder is limited owing to its lack of stability, tendency to migrate from graft sites, and difficulties in remolding [5].
Carrier materials including hyaluronic acid, glycerol, lecithin, chitosan, polyorthoester, and PLGA have been used to improve the handling of DBM powder [6]. Furthermore, these carrier materials have been used to produce several commercial DBM carrier products [7]. Currently, moldable putty, which is the most popular clinical DBM form, can be suitable for bone defects and resisting dispersion from irrigation and blood [8]. The ideal delivery carrier of DBM should control release the active substance, have maximized functions of bone induction and conduction, and be amendable to clinical applications [9–11]. However, the optimal carrier has not been found or designed as yet.
Alginate (C5H7O4COONa), comprised of sequences of M (M-blocks) and G (G-blocks) residues interspersed with MG sequences (MG-blocks), is a natural copolymer obtained from algal and bacterial sources. Because of its excellent biocompatibility and biodegradability, alginate has been applied in cell and drug delivery, bone implants, and wound covering [12–14]. The method of crosslinking alginate with divalent cations to make hydrogels for cell encapsulation has been shown to be advantageous for biomedical applications. This behavior of alginate demonstrates its potential as a carrier for the delivery of DBM particles.
In this study, we used alginate as the carrier to deliver DBM particles. The physiochemical properties, such as surface morphology, porosity measurements,
Material and Methods
PREPARATION OF DBM-ALGINATE COMPOSITES:
Alginate (CAS NO. 9005-38-3, Sigma-Aldrich, USA) and CaCl2 (Sigma-Aldrich) were dissolved in calcium-free phosphate-buffered saline (PBS) to acquire 2 wt% alginate and 2 wt% CaCl2 stock solutions. Our study was approved by the Institutional Review Board, and all the animal experiments were approved by the Medical Ethics Committee of Zhongnan Hospital of Wuhan University. The long bones of 4 limbs were obtained from 40 euthanized male Sprague-Dawley (SD) rats. Then, the technical process of converting rat bones to DBM was performed by Hubei Osteolink Biomaterial Co., Ltd. (Wuhan, China), which has the exclusive certificate of DBM approved by the China Food and Drug Administration (CFDA). Next, the DBM particles were added slowly to the alginate solution (2 wt%) and stirred for 8 h to obtain a mixture with a homogeneous distribution of DBM particles. To obtain the ADBM gel scaffold, 2 wt% CaCl2 was added to the ADBM mixture solution, and crosslinking (>8 h reaction) of calcium and hydroxyl of alginate was maintained. The upper panels of Figure 1A show, from left to right, the images of synthesized ADBM gel scaffold with various amounts of DBM and 1 mL alginate: DBM/alginate in amounts of 0 mg/1 mL, 25 mg/1 mL, 50 mg/1 mL, and 100 mg/1 mL. All samples were 4 mm in diameter and 1 mm in height. Next, ADBM gel scaffold was placed in microfuge tubes (Thermo Fisher Scientific, USA) and frozen at minus 80°C. To obtain dry ADBM composite, the frozen ADBM gel scaffold was immediately transferred to a vacuum freeze drier (Labconco, USA) at minus 80°C. ADBM composites with various amounts of DBM and 1 mL alginate were prepared as shown in the Table 1 and Figure 1A. The lower panels of Figure 1A, from left to right, show images of dry ADBM composites in various amounts. The following in vitro assays were done on a comparative alginate volume.
PHYSIOCHEMICAL PROPERTIES OF THE ADBM:
The physiochemical properties of the lyophilizated ADBM composites, namely, the micro-morphology, porosity (evaluated as previously described [15]), compressive modulus, swelling ratio, and degradation rate (weight remaining ratio=[Wt/W0]×100%, where Wt and W0 were the weights of the composites at setting time and beginning time, respectively [16]), were detected by scanning electron microscopy (SEM), porosity measurement, mechanical testing, equilibrium swelling, and in vitro degradation, respectively.
PROCUREMENT AND CULTURE OF RAT BONE MARROW-DERIVED MESENCHYMAL STEM CELLS:
Primary rat bone marrow-derived mesenchymal stem cells (rBMSCs) were extracted from the femurs of 4-week-old male rats. Next, the cells were resuspended in α-MEM (HyClone) medium containing 10% fetal calf serum (Gibco) and cultured in a 95% humidified incubator at 37°C in 5% CO2. Cellular immunofluorescence was used to verify the phenotype of the rBMSCs with mouse anti-rat monoclonal antibody CD45 (ab33923) and rabbit anti-rat monoclonal antibody CD44 (ab24504).
3-(4,5-DIMETHYLTHIAZOL-2-YL)-2,5-DIPHENYLTETRAZOLIUM BROMIDE ASSAY:
The cytotoxicity of the composite scaffolds was assessed by the 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay. All the composites were immersed in α-MEM medium for 3 days, and the extracted medium was used in the cell-based assay
OSTEOGENIC DIFFERENTIATION:
For osteogenic differentiation, the cells were divided into 3 subgroups according to the culture media and ADBM composite medium extract. The cells were cultured for 7 or 14 days, and the media was replaced every 3 days.
ALKALINE PHOSPHATASE AND ALIZARIN RED STAINING ASSAY:
The osteogenic ability of the rBMSCs was measured by alkaline phosphatase (ALP) and alizarin red staining (ARS) after 7 or 14 days of culture in osteogenic media, respectively [17].
ECTOPIC BONE FORMATION AND CRANIAL DEFECT MODEL:
Fifteen male SD rats (200–250 g, 6–8 weeks old), purchased from Beijing HFK Bioscience Co, Ltd (Beijing, China), were used for the ectopic bone formation and cranial defect model. ADBM composite, DBM, or alginate was implanted in a muscle pouch of the SD rats’ back for 8 weeks (n=5 in each group). The DBM particles and alginate scaffold were used as the control groups. Eight weeks after the implantation, the rats were administered pentobarbital sodium anesthesia and euthanized by dislocation of the spine. The sample tissues were then removed. The tissue samples were examined by X-ray (DigitalDiagnost, Philips Healthcare, the Netherlands) to evaluate the level of ectopic bone formation. The density of the bone regeneration area containing the newly formed bone was determined with the Lane and Sandhu radiological scoring system [18]. Images were photographed with an optical microscope and the level of bone tissue regeneration was calculated based on hematoxylin and eosin (H&E) staining images according to Lane and Sandhu histological scoring criteria [19].
STATISTICAL ANALYSIS:
All statistical analyses were carried out using SPSS for Windows version 17.0 (SPSS, Chicago, IL, USA). Measurement data are expressed as mean±standard error of the mean. An independent
Results
CHARACTERIZATION OF THE ADBM COMPOSITES:
The microstructure of the freeze-dried ADBM composite with various amounts of DBM and 1 mL alginate was observed using SEM to further illustrate the interconnected porous structure. The pore size of the freeze-dried pure alginate scaffold was 300 to 480 μm and that of the composite with a DBM/alginate amount of 25 mg/1 mL was 150 to 400 μm, as shown in Figure 1B. The pore size of composites with DBM/alginate amounts of 50 mg/1 mL and 100 mg/1 mL were 100 and 400 μm, respectively, according to the SEM images, as shown in Figure 1B. These macro-scale sized pores were omnipresent, and DBM particles were uniformly scattered in the 3 ADBM composites. These characteristics are advantageous for MSCs to attach in 3-dimensional cell culture, as well as for substance transport and diffusion. As the amount of DBM particles in the composites increased, the pore area decreased; porosities of 81.9%, 62.3%, 45.7%, and 32.6% were found for the composites with DBM/alginate amounts of 0 mg/1 mL, 25 mg/1 mL, 50 mg/1 mL, and 100 mg/1 mL, respectively.
Degradation was reported in terms of normalized composites relative to the dry composites of each group, as shown in Figure 1C and 1D. Figure 1C shows the degradation characteristics of composites in collagenase. Within each group, the remaining weight decreased with progressive culture in 5 U/mL collagenase. After 15 days, the remaining weight rate was 83.17±4.96%, 56.20±3.40%, 40.27±0.64%, and 27.23±2.57% for composites in DBM/alginate amounts of 0 mg/1 mL, 25 mg/1 mL, 50 mg/1 mL, and 100 mg/1 mL, respectively, which was proportional to DBM with collagen as the major component. The composite with the DBM/alginate amount of 100 mg/1 mL was degraded thoroughly in as little as 12 days, whereas the composites with DBM/alginate amounts of 50 mg/1 mL and 25 mg/1 mL had remaining weights of 44.93±3.31% and 57.50±2.27%, respectively, after 12 days. The degradation rate gradually accelerated as the DBM mass concentration amount in composites increased. Analysis of the in vitro degradation in PBS first showed that all composites had a similar degradation speed of ~85% remaining weight after 15 days, as shown in Figure 1D. This suggests that the hydrolysis rate of the ADMB complex is mild in PBS. Alginate is insensitive to collagenase, resulting in a similar high remaining weight in collagenase in PBS after 15 days.
Absorption of body fluid is another feature of DBM composites. The swelling ratios of composites were measured as a function of immersion time in PBS at 37°C, as shown in Figure 1E. After 16 h of immersion in PBS, all composites with DBM/alginate amounts of 0 mg/1 mL, 25 mg/1 mL, 50 mg/1 mL, and 100 mg/1 mL reached their maximum equilibrium swelling state with swelling ratios of 38.95±2.17%, 29.95±4.27%, 24.23±2.42%, and 15.46±1.043%, respectively. The swelling ratio significantly declined with increasing DBM particles in the composites. The compressive mechanical test showed that the elastic modulus significantly increased as the concentration of DBM particles were increased in the composites. The compressive modulus of the composites with DBM/alginate amounts of 0 mg/1 mL, 25 mg/1 mL, 50 mg/1 mL, and 100 mg/1 mL were 29.44±2.128, 72.59±3.29, 167.30±9.56, and 206.75±15.91, respectively, as shown in Figure 1F. These results indicated that as ADBM content increased, the structure became denser (the results of electron microscopy analysis were the same) and the compressive modulus was also higher.
Here, we produced an alginate hydrogel carrier to transport DBM powder (ADBM composite). We found that, with increasing DBM content, the physical properties of degradation and modulus of elasticity increased, while porosity and swelling rate decreased. These characteristics are beneficial for the use of ADBM complex in the treatment of bone defect.
:
Because it had superior phenotypic characteristics compared to the other groups, we used the 100 mg DBM+1 mL alginate (ADBM-100) group in the following experiments and compared it to a control group.
CYTOTOXICITY ASSAY RESULTS:
The BMSC phenotype was verified by CD44-positive and CD45-negative expression (Figure 2A). MTT assays were performed on the MSCs in the 4 groups to determine whether the composites had cytotoxic effects, as shown in Figure 2B. There were no significant differences in the optical density (OD) values among the groups at each time point.
:
ALP staining intensity in the ADBM-100 composite group was greater than that in the control (alginate) group (Figure 2C). Induced ALP activity in the ADBM-100 group was distinctly higher than that in the control group (Figure 2D). As determined by ARS quantification, exposure of MSCs in the ADBM-100 group to osteogenic medium induced a 50% to 60% increase in calcium deposition (1.39±0.23 OD/mL), which was larger than the increase in the control group (0.78±0.16 OD/mL), as shown in Figure 2E. The formation of calcium deposits was significantly higher in the ADBM group than in the control group. ARS staining showed that the number of black nodules was higher in the ADBM-100 group than in the DBM control group (Figure 2C). These results suggested the ADBM-100 composite had a greater capacity to promote osteogenic differentiation and mineralization than the control.
:
Reverse transcription-polymerase chain reaction was used to analyze the variation of mRNA expression of the 3 groups on day 7. The mRNA expression levels of marker genes including RUNX2, OPN, OCN and collagen I were markedly upregulated by ADBM-100 compared with the control (Figure 2F). Our results showed that, in vitro, ADBM-100 significantly promoted the expression of osteogenesis-related genes including RUNX2, OPN, OCN, and collagen I compared with the control.
:
In the plain radiographs, mineralized calcified tissue formation of the ADBM-100, DBM, and control groups was observed at 8 weeks. However, the radio-opacity of the ADBM-100 group showed a greater intensity than that of the DBM and control groups, as shown in Figure 3. This outcome indicates that the ectopic bone formation induction activity of the ADBM-100 group was greater than that of the DBM and control groups.
:
According to the results of the decalcified H&E staining and Masson’s trichrome staining, newly formed mineralized ectopic calcified tissues were present in the ADBM-100 and DBM groups, indicating that DBM is osteoinductive, as shown in Figure 3. In contrast, no bone marrow, bone, or cartilage was observed around the alginate in the alginate-only group. Furthermore, the volume of mineralization of newly formed bone tissue in the ADBM-100 group was greater than that in the DBM and control groups. Immunohistochemistry was used to semi-quantitatively analyze maker gene expression for each group. Osteopontin (OPN) and osteocalcin (OCN) are markers of the mature Ob phenotype and are involved in bone mineral deposition. Immunohistochemistry analysis revealed that the expression of OPN and OCN in the ADBM-100 group was greater than that in the DBM and control groups.
:
A cranial defect model was used to demonstrate the bone regeneration of ADBM-100 composites in vivo. As detected in plain radiographs, newly formed bone tissue that filled the largest portion of the bone defect was observed in the site implanted with the ADBM-100 composite scaffold after 8 weeks, while no newly formed bone was found in the sham control group (Figure 4A). The Lane and Sandhu radiological score in the ADBM-100 group (5.34±1.32) was significantly higher than that of the control group (0.97±0.28). This was further demonstrated by H&E staining (Figure 4B). The bone defect area of the sham control group was filled with fibrous tissue; however, newly formed bone was observed in the bone defect area of the ADBM-100 group. The Lane and Sandhu histological score in the ADBM-100 group (6.98±1.44) was significantly higher than that of the control group (1.46±0.58).
Discussion
The present study explored the novel synthetic hydrogel carrier alginate for the delivery of DBM particles. Composites were fabricated with DBM particles that were homogeneously dispersed within biodegradable alginate hydrogel. First, the physiochemical characteristics of the composites were investigated. SEM demonstrated that macro-scale pores were omnipresent and DBM particles were uniformly scattered in the composites with various amounts of DBM and 1 mL alginate. As the concentration of DBM particles increased in the composite, the pore area and swelling ratio decreased because the DBM particles partially occupied the pore area formed by the alginate. Alginate is gaining significance, particularly as a bone tissue biomaterial, owing to its biocompatibility and gel-forming properties. To date, several composites such as alginate-protein [20], alginate-bone morphogenetic protein-2 [21], alginate-polymer [22], alginate-ceramic [23], alginate-bioglass [24], and alginate-biosilica [25] composites have been investigated. These alginate composites show improved biochemical properties including biocompatibility, cell proliferation and adhesion, porosity, mechanical strength, alkaline phosphatase enhancement, excellent mineralization, and osteogenic differentiation [26].
Moreover, the elastic modulus significantly increases with an increased concentration of DBM particles in the composites. These features are advantageous for MSC attachment a in 3-dimensional cell culture, as well as in substance transport and diffusion. In the present study, as the concentration of DBM particles increased in the composite, the pore area decreased. DMB is mainly composed of collagen and is sensitive to collagenase, whereas alginate is insensitive to collagenase; this characteristic causes the gradual acceleration of the degradation rate of ADBM composites as DBM content increases. Thus, ADBM composites are degradable, which is the key feature for DBM delivery. Further, ADBM composites have a low degradation rate in PBS solution. This suggests that, in physiological conditions, the hydrolysis rate of the ADBM composites is low where various enzymes are present. Furthermore, its
To further investigate biomedical function in the present study, the MTT assay was performed; no cytotoxicity of ADBM or alginate on MSCs was observed. Compared with the control group, ADBM and DBM particles induced osteogenic formation on MSCs and ectopic implantation, indicating that the established methods for composite preparation maintained the bioactivity of the DBM particles. Moreover, cell culture with ADBM-100 showed greater osteogenic potential, as evidenced by the upregulation of ALP activity, the OD value of calcium deposits in ARS staining, and the mRNA expression level of marker genes compared with only DBM particles. Additionally, ectopic bone formation in our
The following factors may contribute to the intended effects of
Conclusions
The present study represents a novel application of a synthetic alginate hydrogel for the delivery of DBM particles. The delivery system maintains a higher level of osteogenic bioactivity than DBM particles alone, owing to its specific spatial structure and advantages in handling and shaping. We also demonstrated that ADBM composites can promote ectopic osteogenesis
Figures
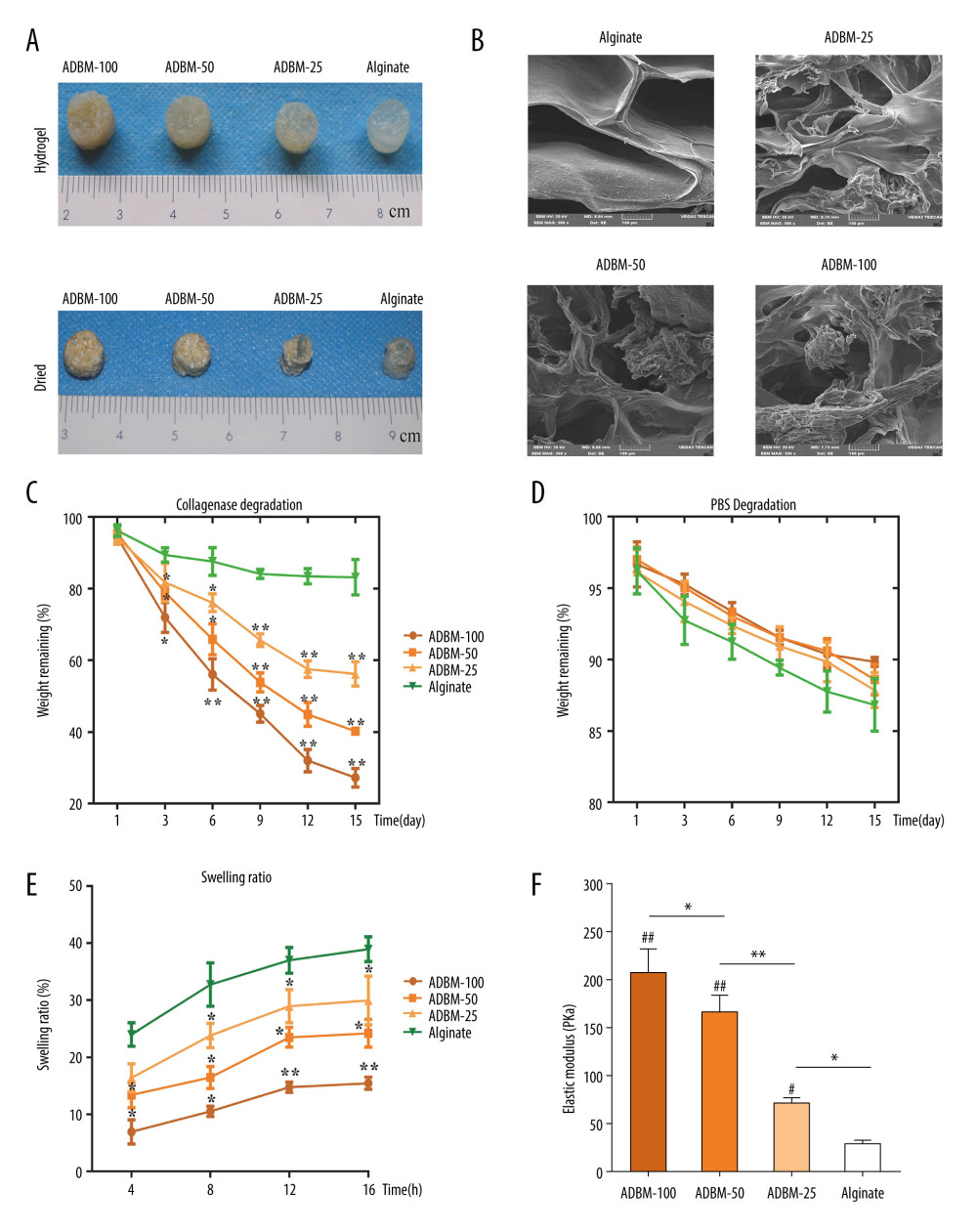 Figure 1. Characterization of demineralized bone matrix-alginate (ADBM) composites. (A) The appearance of the prepared composites gel with various DBM/alginate amounts in hydrogel and dried status: 100 mg/1 mL, 50 mg/1 mL, 25 mg/1 mL, and alginate only (0 mg/1 mL). (B) Scanning electron microscope (SEM) images of the ADBM composites with various DBM/alginate amounts: alginate only (0 mg/1 mL), 25 mg/1 mL, 50 mg/1 mL, and 100 mg/1 mL; cross-sectional morphology as shown in Figure 1B. Scale bar: 100 μm. (C, D) In vitro degradation of ADBM composites in collagenase (C) and phosphate-buffered saline (D); n=3; * compared with the alginate; P<0.05. (E) The swelling ratio of ADBM composites. (F) The compressive modulus of ADBM composites. All error bars represent the mean±SEM for n=3, P<0.05.
Figure 1. Characterization of demineralized bone matrix-alginate (ADBM) composites. (A) The appearance of the prepared composites gel with various DBM/alginate amounts in hydrogel and dried status: 100 mg/1 mL, 50 mg/1 mL, 25 mg/1 mL, and alginate only (0 mg/1 mL). (B) Scanning electron microscope (SEM) images of the ADBM composites with various DBM/alginate amounts: alginate only (0 mg/1 mL), 25 mg/1 mL, 50 mg/1 mL, and 100 mg/1 mL; cross-sectional morphology as shown in Figure 1B. Scale bar: 100 μm. (C, D) In vitro degradation of ADBM composites in collagenase (C) and phosphate-buffered saline (D); n=3; * compared with the alginate; P<0.05. (E) The swelling ratio of ADBM composites. (F) The compressive modulus of ADBM composites. All error bars represent the mean±SEM for n=3, P<0.05. 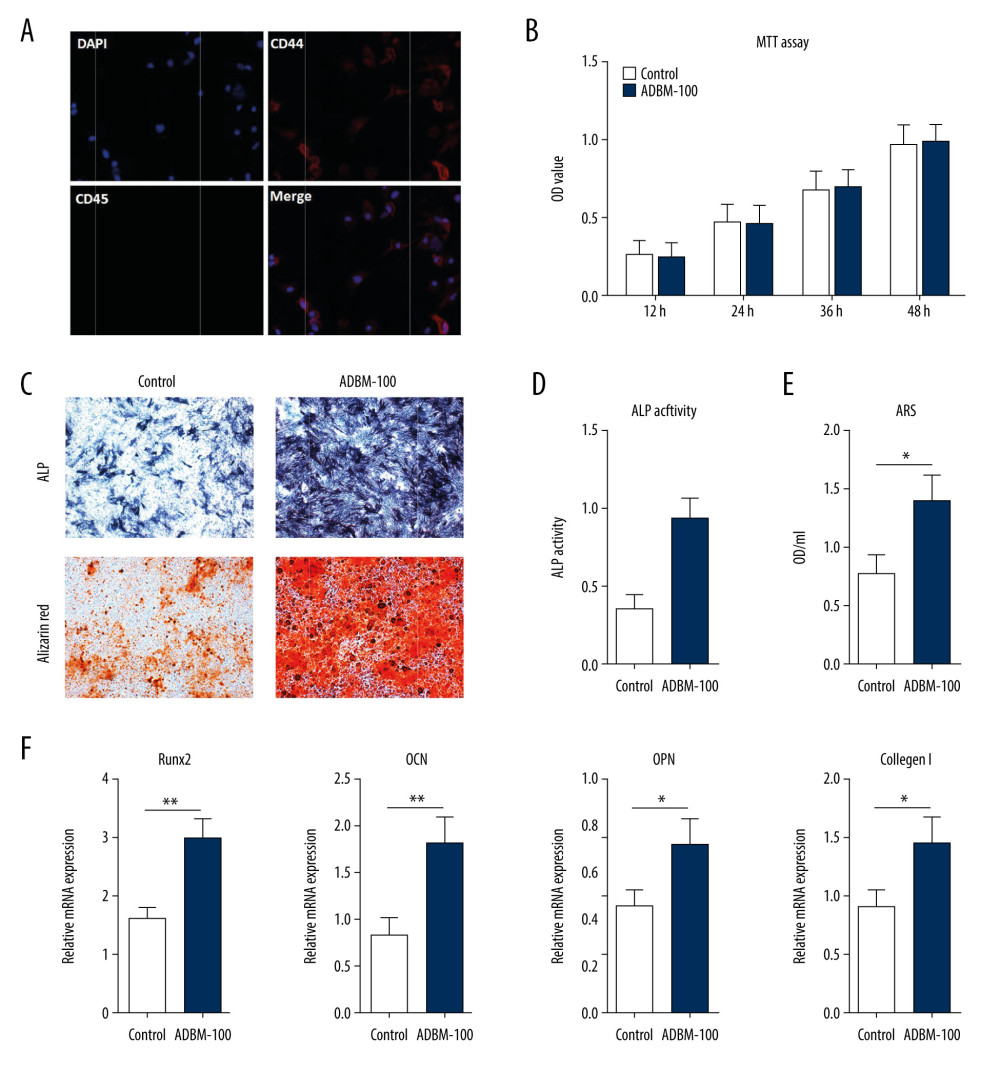 Figure 2. In vitro cell study. (A) Phenotypic verification of bone marrow mesenchymal stem cells (MSCs) and immunofluorescence against CD44, CD45, and DAPI. (B) 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay of demineralized bone matrix-alginate (ADBM)-100 composites on MSCs and the statistical histogram of optical density (OD) values in the control and ADBM groups. (C) ADBM-100 composite promoted osteogenic differentiation in vitro. Representative images of alkaline phosphatase (ALP) and alizarin red staining (ARS) are displayed. (D) ALP activity. (E) The OD value of calcium deposits detected with ARS. (F) The effects of the ADBM-100 composite on MSCs. RUNX2, OPN, OCN, and collagen I, which are marker genes of osteogenic differentiation, were upregulated.
Figure 2. In vitro cell study. (A) Phenotypic verification of bone marrow mesenchymal stem cells (MSCs) and immunofluorescence against CD44, CD45, and DAPI. (B) 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay of demineralized bone matrix-alginate (ADBM)-100 composites on MSCs and the statistical histogram of optical density (OD) values in the control and ADBM groups. (C) ADBM-100 composite promoted osteogenic differentiation in vitro. Representative images of alkaline phosphatase (ALP) and alizarin red staining (ARS) are displayed. (D) ALP activity. (E) The OD value of calcium deposits detected with ARS. (F) The effects of the ADBM-100 composite on MSCs. RUNX2, OPN, OCN, and collagen I, which are marker genes of osteogenic differentiation, were upregulated. 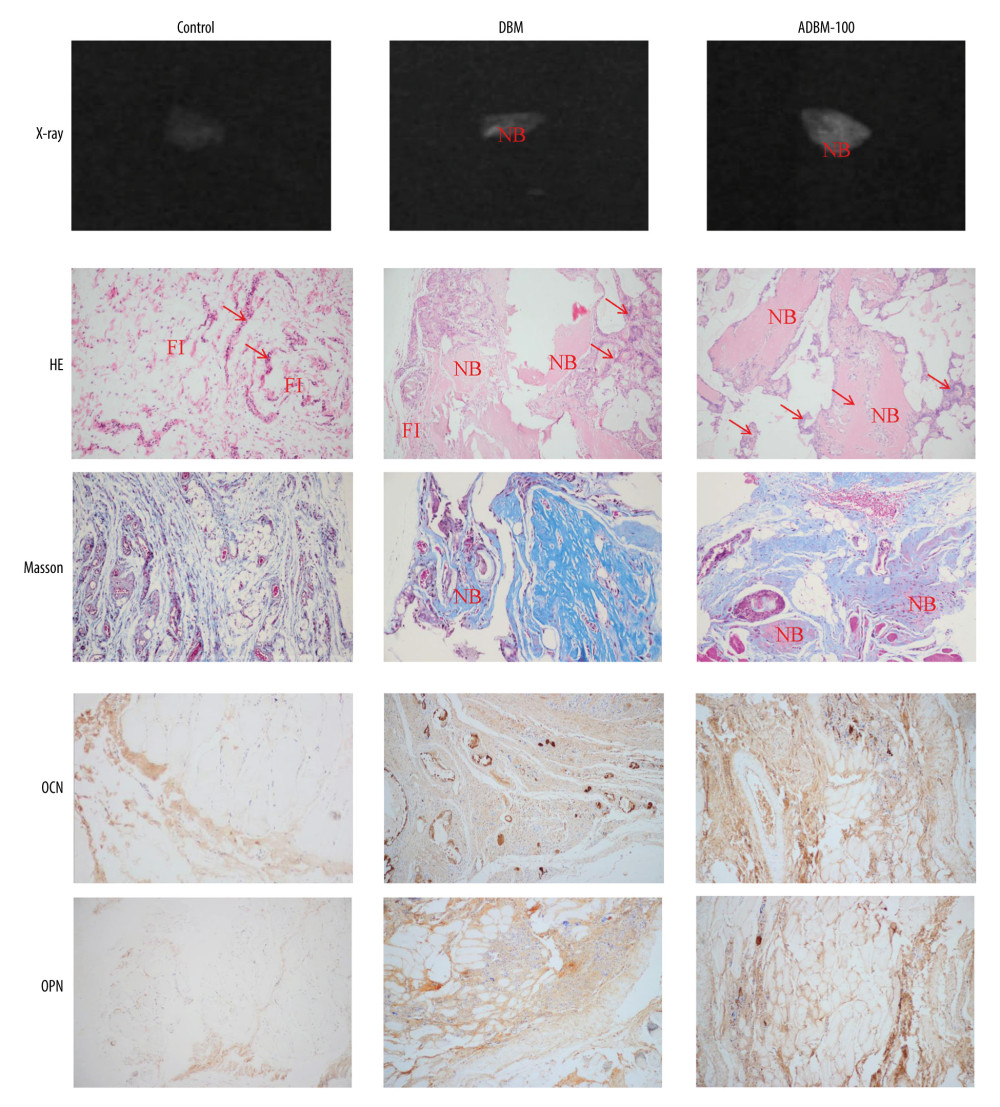 Figure 3. Representative images of X-ray, hematoxylin and eosin staining, Masson’s trichrome staining, and immunohistochemistry of ectopically formed bone tissue. “NB” represents the newly formed bone. “FI” represents the fibrous tissue. The red arrow refers to the inflammatory cells.
Figure 3. Representative images of X-ray, hematoxylin and eosin staining, Masson’s trichrome staining, and immunohistochemistry of ectopically formed bone tissue. “NB” represents the newly formed bone. “FI” represents the fibrous tissue. The red arrow refers to the inflammatory cells. 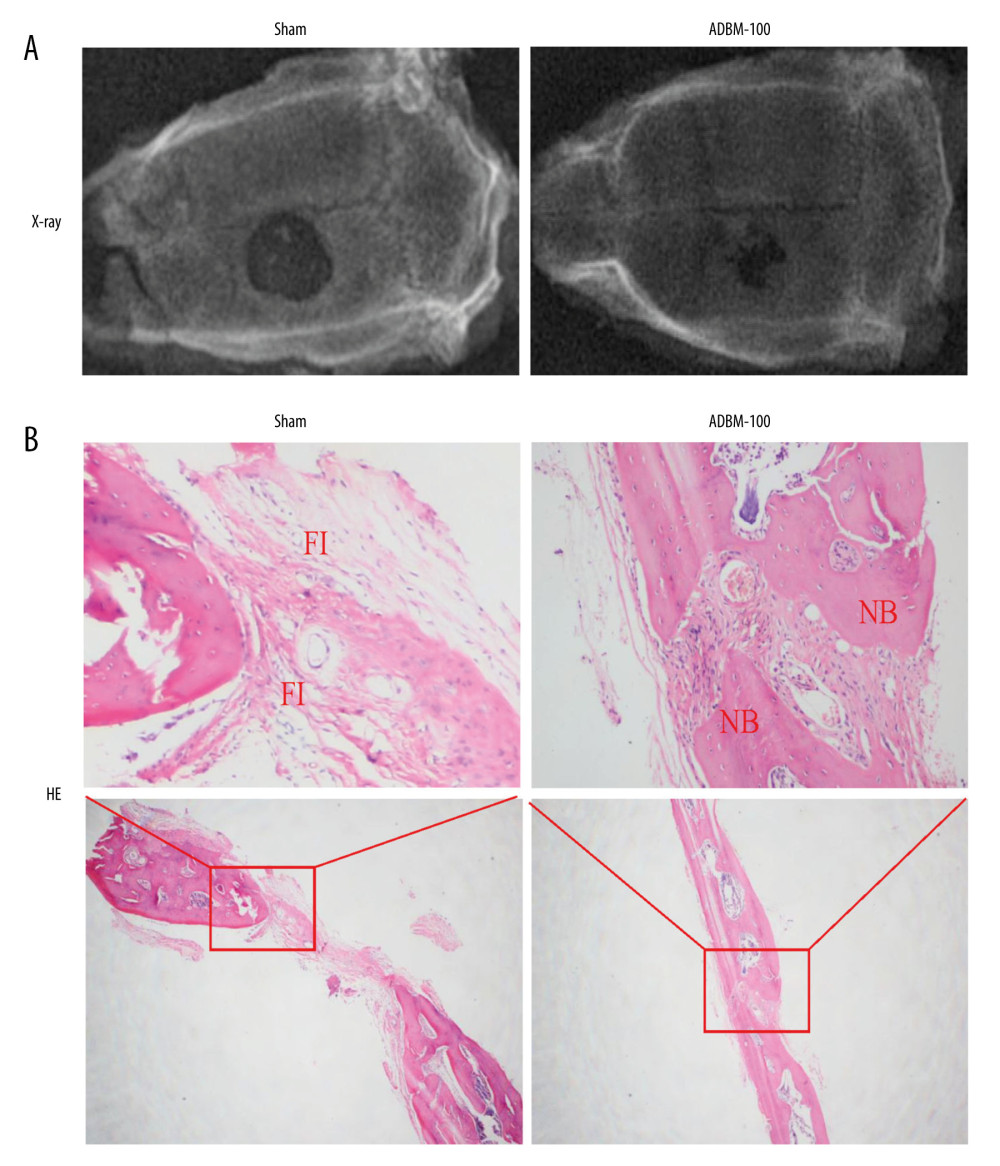 Figure 4. (A, B) Representative images of X-ray and hematoxylin and eosin staining of cranial defects. “NB” represents the newly formed bone. “FI” represents the fibrous tissue.
Figure 4. (A, B) Representative images of X-ray and hematoxylin and eosin staining of cranial defects. “NB” represents the newly formed bone. “FI” represents the fibrous tissue. 
References
1. Morris R, Hossain M, Evans A, Pallister I, Induced membrane technique for treating tibial defects gives mixed results: Bone Joint J, 2017; 99-B; 680-85
2. Nauth A, Lane J, Watson JT, Giannoudis P, Bone graft substitution and augmentation: J Orthop Trauma, 2015; 29(Suppl 12); S34-38
3. Grabowski G, Cornett CA, Bone graft and bone graft substitutes in spine surgery: Current concepts and controversies: J Am Acad Orthop Surg, 2013; 21; 51-60
4. Grgurevic L, Pecina M, Vukicevic S, Marshall R, Urist and the discovery of bone morphogenetic proteins: Int Orthop, 2017; 41; 1065-69
5. Meng Q, Man Z, Dai L, A composite scaffold of MSC affinity peptide-modified demineralized bone matrix particles and chitosan hydrogel for cartilage regeneration: Sci Rep, 2015; 5; 17802
6. Kinard LA, Dahlin RL, Lam J, Synthetic biodegradable hydrogel delivery of demineralized bone matrix for bone augmentation in a rat model: Acta Biomater, 2014; 10; 4574-82
7. Holt DJ, Grainger DW, Demineralized bone matrix as a vehicle for delivering endogenous and exogenous therapeutics in bone repair: Adv Drug Deliv Rev, 2012; 64(12); 1123-28
8. Schallenberger M, Lovick H, Locke J, The effect of temperature exposure during shipment on a commercially available demineralized bone matrix putty: Cell Tissue Bank, 2016; 17; 677-87
9. Galjour C, Dzugan S, Graves M, Stimulation of fracture healing by continuous delivery of demineralized bone matrix proteins and tobramycin: Biomed Sci Instrum, 2005; 41; 122-27
10. Leszczak V, Place LW, Franz N, Nanostructured biomaterials from electrospun demineralized bone matrix: A survey of processing and crosslinking strategies: ACS Appl Mater Interfaces, 2014; 6; 9328-37
11. Benghuzzi H, Wilson G, White J, The effects of sustained delivery of estrogen and demineralized bone matrix proteins on bone in ovariectomized female rats – biomed 2013: Biomed Sci Instrum, 2013; 49; 85-93
12. Jana S, Sen KK, Gandhi A, Alginate based nanocarriers for drug delivery applications: Curr Pharm Des, 2016; 22; 3399-410
13. Wiegand C, Buhren BA, Bunemann E, A novel native collagen dressing with advantageous properties to promote physiological wound healing: J Wound Care, 2016; 25; 713-20
14. Ketabat F, Karkhaneh A, Mehdinavaz Aghdam R, Hossein Ahmadi Tafti S, Injectable conductive collagen/alginate/polypyrrole hydrogels as a biocompatible system for biomedical applications: J Biomater Sci Polym Ed, 2017; 28; 794-805
15. Kreuzeder M, Abad MD, Primorac MM, Fabrication and thermo-mechanical behavior of ultra-fine porous copper: J Mater Sci, 2015; 50; 634-43
16. Tian M, Yang Z, Kuwahara K, Delivery of demineralized bone matrix powder using a thermogelling chitosan carrier: Acta Biomater, 2012; 8; 753-62
17. Li F, Song N, Tombran-Tink J, Niyibizi C, Pigment epithelium-derived factor enhances differentiation and mineral deposition of human mesenchymal stem cells: Stem Cells, 2013; 31; 2714-23
18. Sunay O, Can G, Cakir Z, Autologous rabbit adipose tissue-derived mesenchymal stromal cells for the treatment of bone injuries with distraction osteogenesis: Cytotherapy, 2013; 15; 690-702
19. Lane JM, Sandhu HS, Current approaches to experimental bone grafting: Orthop Clin North Am, 1987; 18; 213-25
20. Park H, Lee HJ, An H, Lee KY, Alginate hydrogels modified with low molecular weight hyaluronate for cartilage regeneration: Carbohydr Polym, 2017; 162; 100-7
21. Ho SS, Vollmer NL, Refaat MI, Bone morphogenetic protein-2 promotes human mesenchymal stem cell survival and resultant bone formation when entrapped in photocrosslinked alginate hydrogels: Adv Healthc Mater, 2016; 5; 2501-9
22. Tong Z, Chen Y, Liu Y, Preparation, characterization and properties of alginate/poly(gamma-glutamic acid) composite microparticles: Mar Drugs, 2017; 15; 91
23. Seidenstuecker M, Ruehe J, Suedkamp NP, Composite material consisting of microporous beta-TCP ceramic and alginate for delayed release of antibiotics: Acta Biomater, 2017; 51; 433-46
24. Chen Q, Cabanas-Polo S, Goudouri OM, Boccaccini AR: Mater Sci Eng, 2014; 40; 55-64
25. Muller WE, Schroder HC, Feng Q, Development of a morphogenetically active scaffold for three-dimensional growth of bone cells: biosilica-alginate hydrogel for SaOS-2 cell cultivation: J Tissue Eng Regen Med, 2015; 9; E39-50
26. Venkatesan J, Bhatnagar I, Manivasagan P, Alginate composites for bone tissue engineering: A review: Int J Biol Macromol, 2015; 72; 269-81
27. Lee J, Perikamana SK, Ahmad T, Controlled retention of BMP-2-derived peptide on nanofibers based on mussel-inspired adhesion for bone formation: Tissue Eng Part A, 2017; 23; 323-34
28. El Bialy I, Jiskoot W, Reza Nejadnik M, Formulation, delivery and stability of bone morphogenetic proteins for effective bone regeneration: Pharm Res, 2017; 34(6); 1152-70
29. Bottlang M, Schemitsch CE, Nauth A, Biomechanical concepts for fracture fixation: J Orthop Trauma, 2015; 29(Suppl 12); S28-33
Figures
Figure 1. Characterization of demineralized bone matrix-alginate (ADBM) composites. (A) The appearance of the prepared composites gel with various DBM/alginate amounts in hydrogel and dried status: 100 mg/1 mL, 50 mg/1 mL, 25 mg/1 mL, and alginate only (0 mg/1 mL). (B) Scanning electron microscope (SEM) images of the ADBM composites with various DBM/alginate amounts: alginate only (0 mg/1 mL), 25 mg/1 mL, 50 mg/1 mL, and 100 mg/1 mL; cross-sectional morphology as shown in Figure 1B. Scale bar: 100 μm. (C, D) In vitro degradation of ADBM composites in collagenase (C) and phosphate-buffered saline (D); n=3; * compared with the alginate; P<0.05. (E) The swelling ratio of ADBM composites. (F) The compressive modulus of ADBM composites. All error bars represent the mean±SEM for n=3, P<0.05.Figure 2. In vitro cell study. (A) Phenotypic verification of bone marrow mesenchymal stem cells (MSCs) and immunofluorescence against CD44, CD45, and DAPI. (B) 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay of demineralized bone matrix-alginate (ADBM)-100 composites on MSCs and the statistical histogram of optical density (OD) values in the control and ADBM groups. (C) ADBM-100 composite promoted osteogenic differentiation in vitro. Representative images of alkaline phosphatase (ALP) and alizarin red staining (ARS) are displayed. (D) ALP activity. (E) The OD value of calcium deposits detected with ARS. (F) The effects of the ADBM-100 composite on MSCs. RUNX2, OPN, OCN, and collagen I, which are marker genes of osteogenic differentiation, were upregulated.Figure 3. Representative images of X-ray, hematoxylin and eosin staining, Masson’s trichrome staining, and immunohistochemistry of ectopically formed bone tissue. “NB” represents the newly formed bone. “FI” represents the fibrous tissue. The red arrow refers to the inflammatory cells.Figure 4. (A, B) Representative images of X-ray and hematoxylin and eosin staining of cranial defects. “NB” represents the newly formed bone. “FI” represents the fibrous tissue. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387