13 January 2021: Clinical Research
Analysis of Root Canal Curvature and Root Canal Morphology of Maxillary Posterior Teeth in Guizhou, China
Xin Qiao123CDEF, Tingting Xu4BC, Liang Chen123D, Deqin Yang123AG*DOI: 10.12659/MSM.928758
Med Sci Monit 2021; 27:e928758






Abstract
BACKGROUND: We investigated the root canal curvature and morphology of maxillary posterior teeth in Guizhou, China, to provide references for clinical practice.
MATERIAL AND METHODS: We collected 274 maxillary posterior teeth in Guizhou Province, China. The root canal curvature was observed by X-ray film measurement. Two hundred teeth were selected to make transparent tooth models, and root canal configuration was recorded according to Vertucci classification criteria. The position of the MB2 root canal orifice and the mesiobuccal root canal configuration were observed by micro-computed tomographic (micro-CT) scanning. The t test and the chi-square test were used for statistical analysis.
RESULTS: The root canals of the maxillary posterior teeth showed more significant curvature in the mesiodistal direction than in the buccolingual direction (P<0.05). The MB2 root canal of maxillary molars showed severe bending in the mesiodistal direction: 25.16±6.6 degrees and 28.05±8.65 degrees in first and second molars, respectively. The detection rate of MB2 was 48% in maxillary first molars and 32% in maxillary second molars. The results of micro-CT showed that the vertical distances between the MB2 and MB-P line were 0.64±0.34 mm and 0.57±0.28 mm in first and second molars, respectively.
CONCLUSIONS: The root canal morphology and curvature of maxillary posterior teeth varied greatly in the Guizhou population, which increases the difficulty of treatment. It is necessary for clinicians to gain understanding of the root canal and to improve the success rate of root canal therapy.
Keywords: Tooth Root, X-Ray Microtomography, anatomic variation, Bicuspid, Maxilla, Molar
Background
Dental caries is the most widespread chronic infectious disease of humans. Inflammation in pulp tissues caused by dental caries leads to periapical granulomas, bone erosion, tooth loss, and severe pain [1]. Root canal therapy is the most commonly used and effective treatment for pulp and periapical disease [2], involving the removal of inflamed or necrotic pulp tissues and cleaning and shaping of the root canals, followed by obturation of the prepared canals. The wide range of variations in root canal morphological configuration complicate endodontic treatment if any of the root canal is left [3–5]. An untreated missed root canal can lead to persistent presence of microorganisms and necrotic tissue inside the canal, accounting for the high rate of root canal failure [6]. The prevalence of untreated maxillary first molar MB2 canals in endodontic treatment failures was reported to be 66.0%, whereas the prevalence of MB2 canals in primary treatments was 57.9%. This difference was statistically significant and suggested the cause of persistent disease [7].
One of the important indices to evaluate the difficulty of root canal therapy is root canal curvature [8]. The preparation of a curved root canal is particularly complex and is more likely to cause complications such as root canal deviation, formation of steps, and separation of instruments [9]. In clinical practice, it is common to take X-rays film to observe the curved shape of the root canal and evaluate difficulties of root canal treatment before surgery. There have been few studies on root canal curvature of the maxillary posterior teeth in Guizhou, China.
Maxillary posterior teeth have a highly diverse canal configuration that varies among races and geographic regions. Mohara et al. reported that the incidence of MB2 in the first permanent molar and the second permanent molar of the maxillary in Brazilians is 64.2% and 33.5%, respectively [10]. Buchanan et al. reported that according to the Vertucci classification of the root canal, type IV root canal is the most common in the maxillary first molar in South Africa, and type I root canal is the most common in the maxillary second molar [11]. Li et al. found that the most common anatomy of maxillary first premolars is 1 root with 2 canals (58.0%), and the typical canal morphology is type IV (42.7%) in the Chinese population [12]. In addition, Guo et al. performed an evaluation of maxillary first molar morphology in a North American subpopulation, found that Asians presented a higher prevalence of Vertucci type I (35.0%) and type IV (45.0%) configurations when compared with white people (type I: 23.4%, type IV: 36.3%) [13]. Thus, there are some regional differences of root canal morphology. Relevant research in local populations can help clinicians to increase understanding and evaluation of root canal therapy and enrich the body of research on human root canals.
Therefore, the present study collected data on the maxillary posterior permanent teeth (including all maxillary premolars and molars, except the third molars) of people in Guizhou, China and observed the buccolingual and the mesiodistal root canal curvature with Schneider’s X-rays method [14]. We also studied root canal morphology of various teeth using transparent tooth staining technology according to Vertucci’s classification. Then, we used micro-computed tomography (micro-CT) to analyze the location of the MB2 root canal orifice in maxillary molars in order to provide a meaningful reference for the root canal treatment in people in Guizhou, China.
Material and Methods
MAIN EXPERIMENTAL MATERIALS:
In Guizhou Province, China (including Zunyi City, Guiyang City, Renhuai City, Duyun City, Kaili City, Jinsha County, Tongzi County, Suiyang County, Yaxi Town, and Tuanxi Town), maxillary posterior molars were collected from stomatological hospital and stomatological clinic. This procedure has been confirmed by the Ethics Committee of the Stomatological Hospital Affiliated with Chongqing Medical University.
Inclusion criteria were: no caries, completed root formation, no pulp treatment, and no internal and external absorption of the collected maxillary posterior teeth.
Exclusion criteria were: incomplete apical development, apical absorption, and any pulp treatment.
X-RAY MEASUREMENT OF ROOT CANAL CURVATURE:
We selected 274 teeth (including 172 premolars and 102 molars) according to the inclusion criteria. The sample size was estimated and calculated. After ultrasonic (NEWTRON® P5 BLED, SATELEC, Paris, France) removal of the soft tissue and stones adhered to the surface of the teeth, the top of the whole pulp chamber was uncovered, the contents of the pulp chamber and the calcification in the pulp chamber were removed by dental fissure bur (Dentsply, New York, Pennsylvania, USA), the pulp chamber bottom and the root canal orifice were fully exposed, and the root canal was inserted with a 15# K-file. When the K-file just exposed the apical foramen, the operation was stopped to try to preserve the original appearance of the root canal. The method of parallel projection was used: the buccal surface of the tooth was fixed with the K-file on the cardboard with double-sided tape, the plane of the cardboard was parallel to the long axis of the tooth, the cardboard was then placed on the receiver, and the receiver was fixed 30 cm below the ball tube mouth of the Kodak 2100 integrated X-ray system (Kodak, Rochester, New York, USA), and the mesiodistal (form mesial to distal) and buccolingual (from buccal to lingual) areas were photographed for the same tooth. Under the condition of 60 kV, 7 Ma, and 0.16 s, the obtained X-ray dental film was saved as a digital image, and then it was imported into the electronic measuring ruler software (CASS, SOUTH DIGITAL TECHNOLOGY COMPANY, Guangzhou, China) to measure the root canal curvature of the maxillary posterior teeth.
Measurements were performed using the method of Schneider [14], in which a line was scribed from the root canal orifice (Figure 1 Point A) on the X-ray parallel to the long axis of the canal. A second line was drawn from the apical foramen (Figure 1 Point C) to intersect with the first at the point where the canal began to leave the long axis of the tooth (Figure 1 Point B). The acute angle formed was measured and recorded.
The same experimenter measured the root canal curvature according to the above method, and took the average value of 3 measurements to reduce bias between observers.
According to the Schneider method [14,15], the calculated curvature of root canal can be divided into 3 categories: 0–5 degrees of root canal curvature is category I (also known as basically no curvature), 5–20 degrees of root canal curvature is category II (moderate curvature of root canal), and more than 20 degrees of root canal curvature is category III (severe curvature of root canal). The combination of class II and class III is indicted a curved root canal.
OBSERVATION OF ROOT CANAL MORPHOLOGY BY TRANSPARENT TOOTH METHOD:
We selected 200 teeth (100 premolars and 100 molars) according to the inclusion criteria. The sample size was estimated and calculated. The adhered soft tissues and stones on the surface of the teeth were removed
Root canal morphology was classified according to the Vertucci classification standard (Figure 2). The mesiobuccal root canals of maxillary molars vary greatly, so the mesiobuccal root was chosen for observation and analysis in maxillary molars.
MICRO-CT OBSERVATION OF ROOT CANAL ORIFICE POSITION: We randomly selected 21 maxillary first molars and 21 maxillary second molars from the teeth that met the inclusion criteria. The sample size was estimated and calculated. In vitro, the experimental teeth were put into the micro-CT device (Micro CT inveon; Siemens Medical Solutions, Knoxville, TN). The scanning track was perpendicular to the long axis of the teeth, and the three-dimensional accuracy was 15×15×15 μm. We imported the two-dimensional data (DICOM format) acquired after scanning into MICs 10.01 software (Materialise, Leuven, Belgium) for digital simulation three-dimensional reconstruction. To evaluate the distribution of MB2 orifices, we adjusted the transparency and magnification of the model, measured the distance MB-MB2, the vertical distance between the MB2 and MB-P lines, and the acute angle between the MB-MB2 and MB-P lines (Figure 3) with the measurement function attached to the software. The root canal morphology of mesiobuccal roots was observed and classified according to Vertucci method.
DATA ANALYSIS:
SPSS 19.0 (SPSS, Chicago, IL, USA) software was used to calculate the mean and standard deviation of the curvature of each root canal. We performed
Results
X-RAY MEASUREMENT OF ROOT CANAL CURVATURE:
As shown in Table 1, the mean curvature of the maxillary second premolar was slightly higher than that of the first premolar, and all of them had moderate curvature (5–20 degrees) in mesiodistal and buccolingual directions. However, we noted that the maximum curvature generally reached category III (more than 20 degree) in maxillary premolars, regardless of direction, indicating that root canal curvature varies greatly among individuals. There was a significant difference in palatal roots between mesiodistal (7.73±5.30 degree) and buccolingual (9.42±7.16 degree) directions of the first premolars (P<0.05) (Table 1).
Table 2 shows the root canal curvature of maxillary molars. Except for MB2 of the second molar, all the root canal curvatures of maxillary molars showed significant differences in mesiodistal and buccolingual directions (P<0.01). According to our results, the root canals of the maxillary posterior teeth showed a greater curvature in the mesiodistal direction than in the buccolingual direction, and the MB and MB2 of maxillary first molars and MB2 of maxillary second molars showed severe bending (more than 20 degrees) in the mesiodistal direction (20.84±7.16 degrees, 25.16±6.6 degrees, and 28.05±8.65 degrees, respectively). All root canals of maxillary posterior teeth showed moderate curvature (more than 5 degrees and less than 20 degrees) in the buccolingual direction, while palatal roots showed slight bending in mesiodistal directions, i.e., a straight root canal (less than 5 degree) (Table 2).
Figure 4 shows the types of root canal curvature in different tooth positions and different projection directions.
OBSERVATION OF ROOT CANAL MORPHOLOGY BY TRANSPARENT TOOTH METHOD:
The representative types of root canals observed by the transparent tooth method are shown in Figure 5. In the first premolar, the detection rate of type IV root canal was the highest, accounting for 44%, followed by type II root canal, accounting for 26%. In the second premolar, the detection rate of type I root canals was the highest (44%), followed by type II and type IV root canals (28% and 22%). The results showed that the detection rate of MB2 (type II, IV, and VI) in maxillary first molars was 48%, while it was 32% in maxillary second molars. The proportion of type I root canal in the mesiobuccal root of the second permanent molars was highest, accounting for 48%. The detailed classification of root canal configuration in different tooth positions is shown in Table 3.
MICRO-CT OBSERVATION OF ROOT CANAL ORIFICE POSITION:
MB2 orifice was found in 10 maxillary first molars and 8 maxillary second molars. The results of micro-CT showed that all the MB2 orifices were located at the lingual side of the MB, and the MB2-MB distances of the first molar and the second molar were (1.37±0.48) mm and (1.29±0.54) mm, respectively. Most of the MB2 orifices were located at mesial position of the line of MB-P, but in 1 case, the MB2 orifices were located at the distal position. In maxillary first molars and second molars, the vertical distances between MB2 and the line of MB-P were (0.64±0.34) mm, (0.57±0.28) mm, and the angles between the MB-MB2 line and MB-P line were (25.18±18.32)° and (23.31±15.86)°, respectively (Table 4).
The representative root canal morphology observed by micro-CT of the first and second maxillary molars mesiobuccal root is shown in Figure 6. According to the Vertucci method, the incidences of MB2 were 47.62% and 38.10%, respectively. When the allowable error is 20%, we compared the incidence of MB2 between micro-CT and transparent teeth method, and the chi-square test showed that there were no statistically significant differences (P>0.05) (Table 5).
In this study, although the sample size was not large, a tooth with a relatively rare shape was found. The report was as follows: the first permanent molar of the maxillary had 2 mesiobuccal roots, which were type I root canal type (Figure 6H). Micro-CT clearly showed that the branches of the root canal were complex and highly variable, especially in 1/3 of the apex (Figure 6).
Discussion
To improve the success rate of root canal therapy, it is necessary to understand the root canal curvature. In clinical practice, X-ray film is mainly used to evaluate the root canal curvature before root canal surgery, that can show root canal curvature in the mesiodistal direction. However, when there is curvature in the buccolingual direction, clinical X-ray films show little useful information to the dentist because of the limitation of a single-projection direction; moreover, the curvature of the palatal root canal is often not reflected due to buccal root obstruction. These undiscovered bends may result in poor root canal preparation, such as inaccurate measurement of working length, deviation during root canal expansion, and lateral or zonal perforation [16]. In this study, the digital X-ray dental film machine was used to project the maxillary posterior teeth
Importantly, endodontic instruments have the tendency to conform to a straight canal, causing over-preparation of the outer curvature in their apical portion and the inner curve of the root canal in the coronal parts of the curved roots [17]. With the increase of root canal curvature, this negative effect is especially obvious, which leads to more errors in root canal preparation. Furthermore, canal preparation errors hinder adequate cleaning, irrigation, and filling of root canals, and are thus likely to negatively affect treatment outcomes [18,19]. Therefore, root canal curvature is one of the important indexes used to evaluate the difficulty of root canal therapy. In our study, the root canals of maxillary premolars all showed moderate curvature, either in mesiodistal or buccolingual directions. However, the curvature in mesiodistal directions was significantly greater than that in buccolingual direction (except for MB2 of maxillary second molar) in maxillary molars, and the difference was statistically significant, which was consistent with the root anatomy. As is well known, the root of maxillary molars is mostly distally oriented [20], which explains why the flexion angles in the mesiodistal direction were significantly greater than that in the buccolingual direction. In addition, the bending angles were mostly moderate-to-severe in maxillary molars, which undoubtedly increases the difficulty and challenge for root canal therapy. When preparing the root canal of maxillary posterior teeth, we suggest that clinicians should use a softer nickel-titanium file to reduce complications such as needle breakage and apical deviation.
Commonly used methods to observe the root canal system include X-ray, transparent tooth, CBCT, and micro-CT. At present, CBCT is often used in the study of root canal morphology [21–23]. However, transparent teeth can directly and comprehensively observe the three-dimensional morphology of the root canal system, which helps find subtle structures such as lateral branch root canal and apical divergence. Zhang Zhiyong et al. showed that the display of transparent teeth on the branch structure of root canal was significantly higher than that of CBCT [24]. In the present study, we used transparent tooth method to observe the root canal morphology. The current study showed that maxillary posterior teeth among residents of Guizhou, China, presented with a variety of Vertucci types of canal configurations, with similarities and differences to other reported studies [10,25,26] in different populations.
We revealed that the incidence of single root canal (type I) in maxillary first premolar was only 12%, and the 2-canal configuration was the most prevalent observation (88%), which is similar to that of the Shandong population (89%) assessed by Wu et al. [6]. According to Vertucci classification, type IV had the highest detection rate (44%) in maxillary first premolars, slightly higher than that reported by Wolf et al. in a Swiss-German population (30%) [27]. Previous studies [28,29] suggested that type I was the most prevalent in the second premolars in Brazil (49.9%) and Saudi Arabia (49.4%), which is consistent with the present study (44%) in Guizhou, China.
In maxillary molars, MB2 exists in type II, IV, and VI root canal configurations of the mesiobuccal root, which was estimated to be 48% in first maxillary molars and 32% in maxillary second molars, consistent with a study on MB2 incidence of maxillary second molars (35.97%) in Taiwan [25]. These results are higher than the incidence of MB2 (in maxillary first and second molars were 36.3% and 8.5%, respectively) in a Malaysian subpopulation [30], but lower than that in a white population (71% in maxillary first molars and 44% in second molars) [31] and in a Brazilian subpopulation (85.7% in maxillary first molars) [32]. These differences suggest that the incidence of MB2 varies by region and race. No C-shaped roots or canals were found in the present study, although cases have been reported [33], and the incidence of C-shaped roots in maxillary molars in China is low.
In the present study, we used micro-CT technology to reconstruct the first and second maxillary molars in three-dimensional digital simulation. According to the measured related values to locate the MB2 orifice, the approximate position of MB2 can be inferred: most MB2 are located at the lingual side of the root canal orifice of MB, and the mesial of the line of MB-P (occasionally in the distal), the length from MB2 to MB-P line is about 0.6 mm, the distance between MB and MB2 is about 1–1.5 mm, and the angle between MB-P and MB-MB2 is about 23–25 degrees. When exploring maxillary molars, clinicians can look for MB2 in the above range, so as to improve the success rate of root canal therapy.
There is obvious variation of the root canal curvature and morphology of maxillary posterior teeth in Guizhou, China, which is very complex and requires careful assessment for endodontic treatment. Our study has certain limitations. For example, the sample size was not large enough, and a study with a larger sample size may provide a more convincing and reliable result in the study of a specific population. In addition, this study only discussed the root canal anatomy, but not the root anatomy. As an important structure of teeth, roots also play an important role in clinical practice, not only for endodontic purposes, but also when certain clinical procedures are planned. Implant placement [34], miniscrew insertion [35], or complex disinclusion orthodontic therapy [36] gain in predicability with deeper knowledge of variations in tooth anatomy. These issues need to be further studied in the future.
Conclusions
Within the limitations of the present report, complex structures and large variation can be found in the root canal morphology of maxillary posterior teeth in Guizhou, China. The maxillary posterior teeth showed obvious root canal bending variation and root canal configuration differences. Mostly, the root canals of maxillary premolars showed moderate curvature, while the root canals of maxillary molars showed moderate-to-severe bending. In the Guizhou population, the incidence of double root canals in maxillary premolars is high. The endodontic doctors should carefully explore to avoid missing root canals when performing root canal therapy. The incidence of 2 canals in the MB roots in the first molars was higher than that of the second molars. The root canal configuration of maxillary second molars was more variable than those of the first molars. Before root canal treatment, doctors should be fully aware of the possibility of root canal variation, and explore carefully to avoid missing root canals, so as to improve the success rate of treatment.
Figures
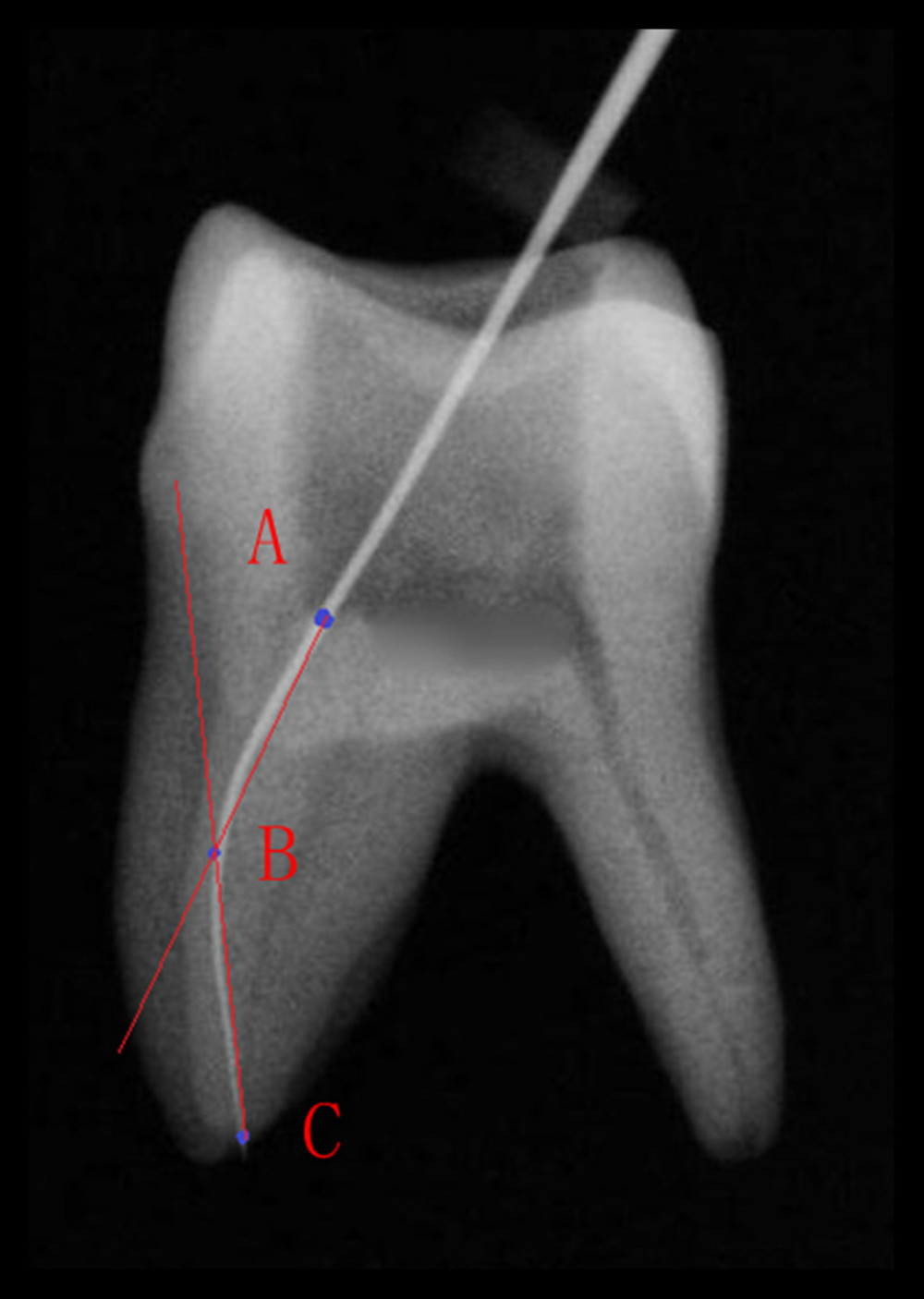 Figure 1. Root canal curvature measurement (Point A) the root canal orifice (Point B) the canal began to leave the long axis of the tooth (Point C) the apical foramen
Figure 1. Root canal curvature measurement (Point A) the root canal orifice (Point B) the canal began to leave the long axis of the tooth (Point C) the apical foramen 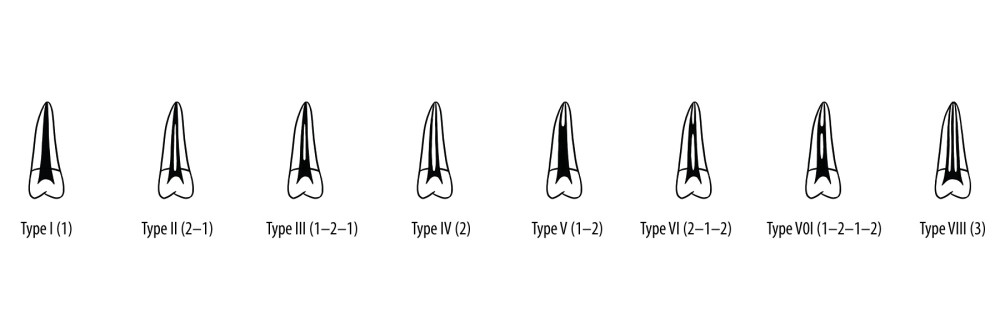 Figure 2. Illustration showing the categories of root canal morphologies in human permanent teeth according to the method by Vertucci.
Figure 2. Illustration showing the categories of root canal morphologies in human permanent teeth according to the method by Vertucci. 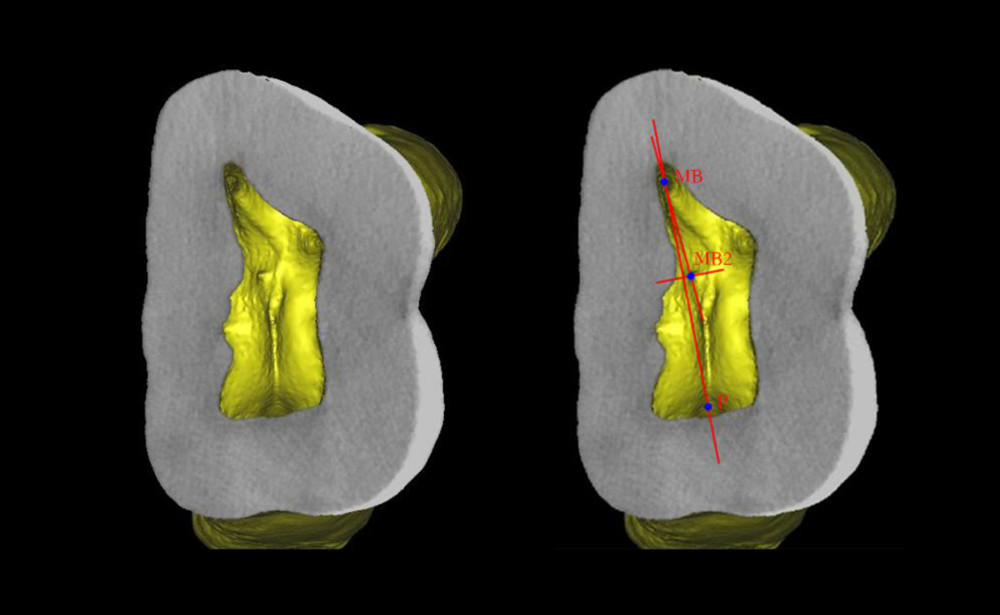 Figure 3. Diagram of MB2 root canal orifice positioning measurement.
Figure 3. Diagram of MB2 root canal orifice positioning measurement. 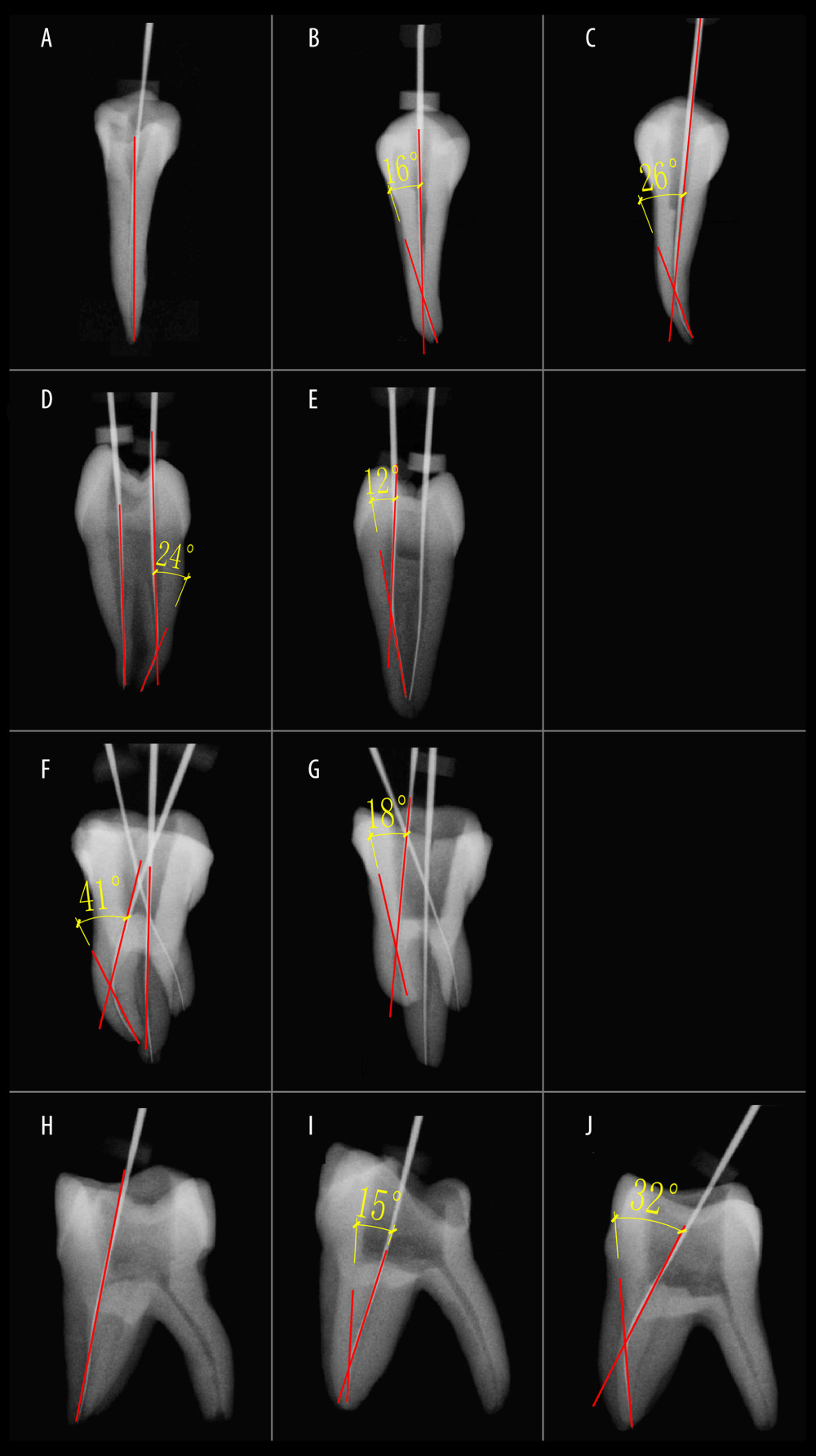 Figure 4. Representation of root canal curvature in different tooth positions and different observation directions. (A–C) Buccolingual direction of premolar (A) straight root canal (category I). (B) Moderately curved root canal (category II). (C) Severely curved root canal (category III). (D, E) Mesiodistal direction of premolar. (D) Straight root canal (category I) and severely curved root canal (category III). (E) Moderately curved root canal (category II). (F, G) Buccolingual direction of molar. (F) Straight root canal (category I) and severely curved root canal (category III). (G) Moderately curved root canal (category II). (H–J) Mesiodistal direction of molar. (H) Straight root canal (category I). (I) Moderately curved root canal (category II). (J) Severely curved root canal (category III).
Figure 4. Representation of root canal curvature in different tooth positions and different observation directions. (A–C) Buccolingual direction of premolar (A) straight root canal (category I). (B) Moderately curved root canal (category II). (C) Severely curved root canal (category III). (D, E) Mesiodistal direction of premolar. (D) Straight root canal (category I) and severely curved root canal (category III). (E) Moderately curved root canal (category II). (F, G) Buccolingual direction of molar. (F) Straight root canal (category I) and severely curved root canal (category III). (G) Moderately curved root canal (category II). (H–J) Mesiodistal direction of molar. (H) Straight root canal (category I). (I) Moderately curved root canal (category II). (J) Severely curved root canal (category III). 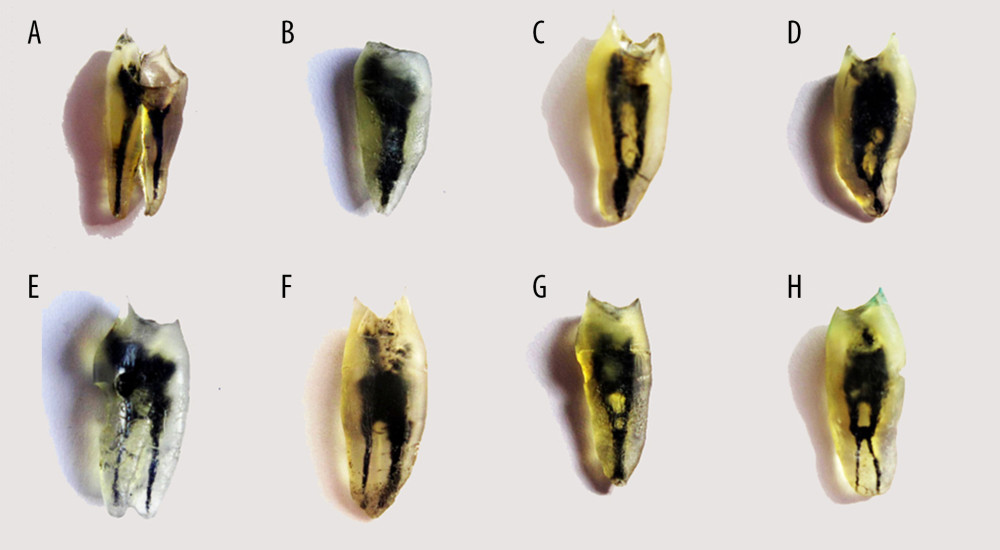 Figure 5. Representation of root canal types observed by transparent tooth method (A) Type I (1-1 double roots) (B) type I (1-1 single root) (C) type II (2-1) (D) type III (1-2-1) (E) Type IV (2-2) (F) type V (1-2) (G) type VI (2-1-2) (H) type VII (1-2-1-2).
Figure 5. Representation of root canal types observed by transparent tooth method (A) Type I (1-1 double roots) (B) type I (1-1 single root) (C) type II (2-1) (D) type III (1-2-1) (E) Type IV (2-2) (F) type V (1-2) (G) type VI (2-1-2) (H) type VII (1-2-1-2). 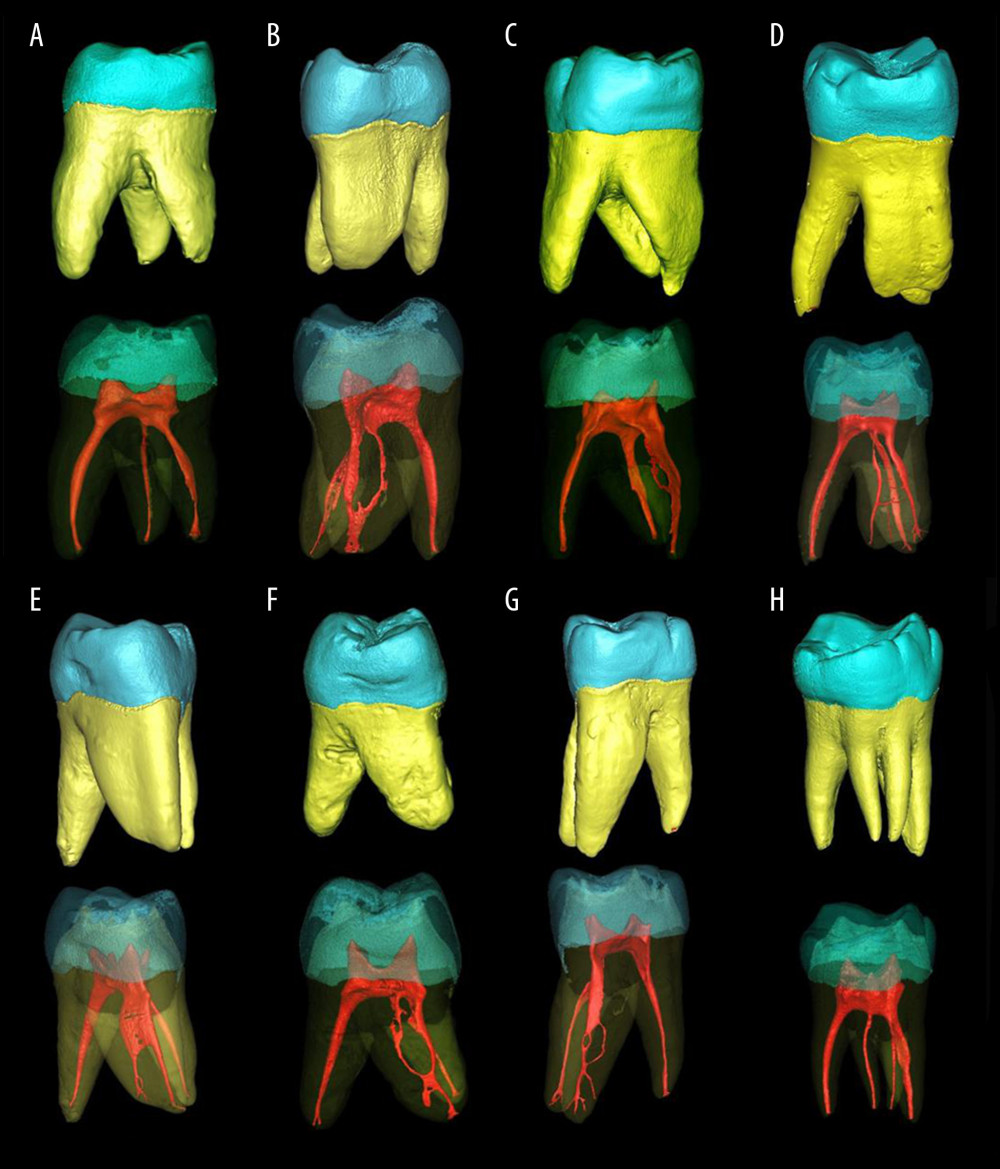 Figure 6. Representation root canal morphology by micro-CT (A) Type I (1-1) (B) Type II (2-1) (C) Type III (1-2-1) (D) Type IV (2-2) (E) type V (1-2) (F) type VI (2-1-2) (G) type VII (1-2-1-2) (H) Double root of mesial buccal (1-1 root canal).
Figure 6. Representation root canal morphology by micro-CT (A) Type I (1-1) (B) Type II (2-1) (C) Type III (1-2-1) (D) Type IV (2-2) (E) type V (1-2) (F) type VI (2-1-2) (G) type VII (1-2-1-2) (H) Double root of mesial buccal (1-1 root canal). Tables
Table 1. Root canal curvature of maxillary premolar.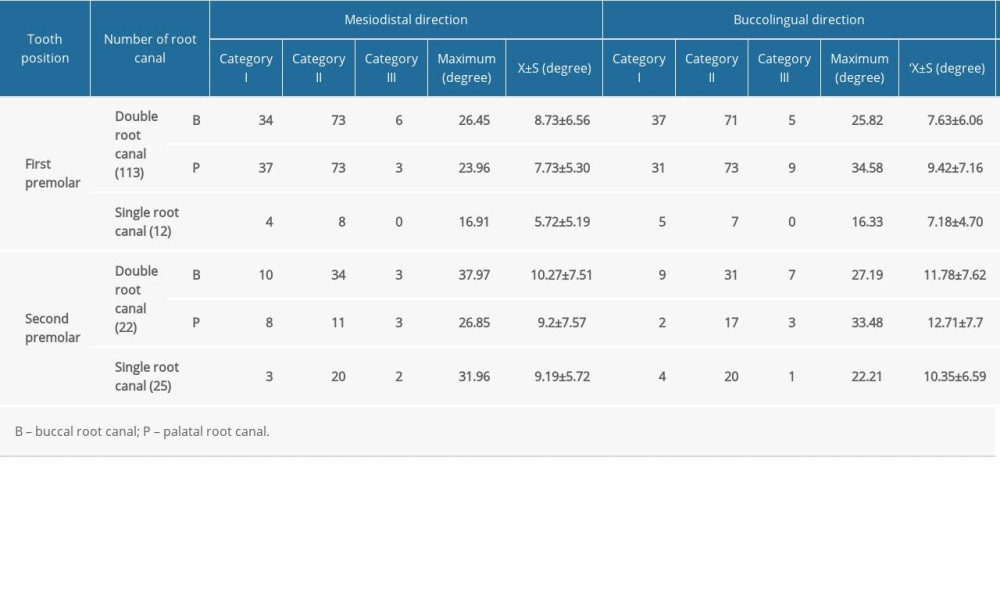 Table 2. Root canal curvature of maxillary molar.
Table 2. Root canal curvature of maxillary molar.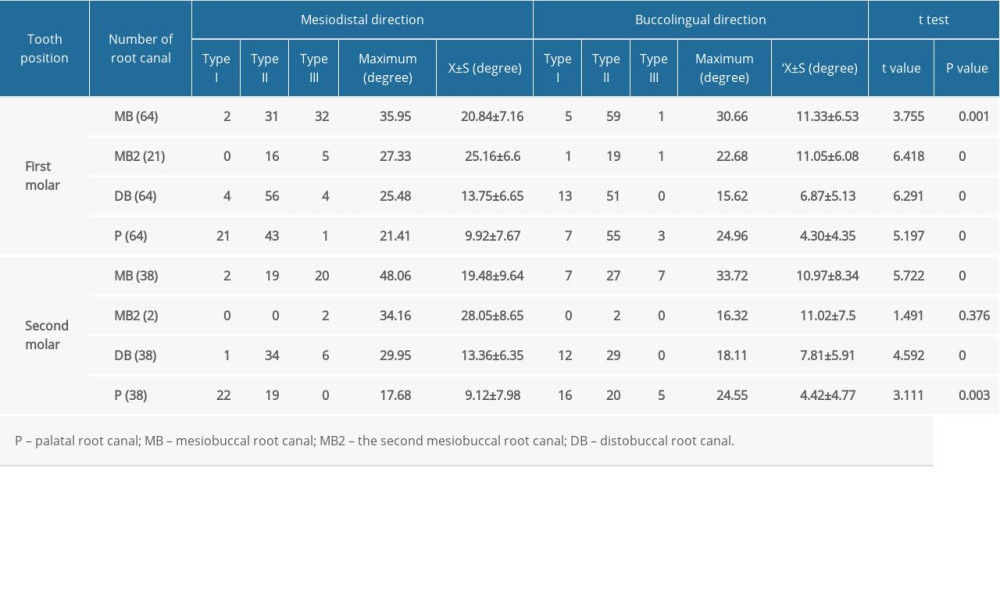 Table 3. Distribution of main root canal configuration of 200 maxillary posterior teeth (n %).
Table 3. Distribution of main root canal configuration of 200 maxillary posterior teeth (n %).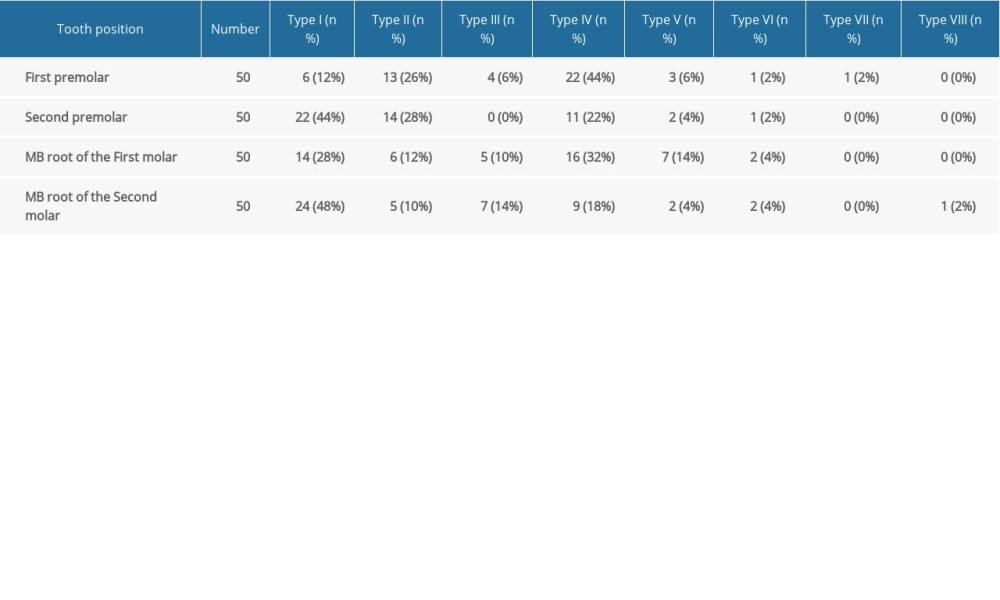 Table 4. Measurement results of MB2 orifice in micro-CT.
Table 4. Measurement results of MB2 orifice in micro-CT.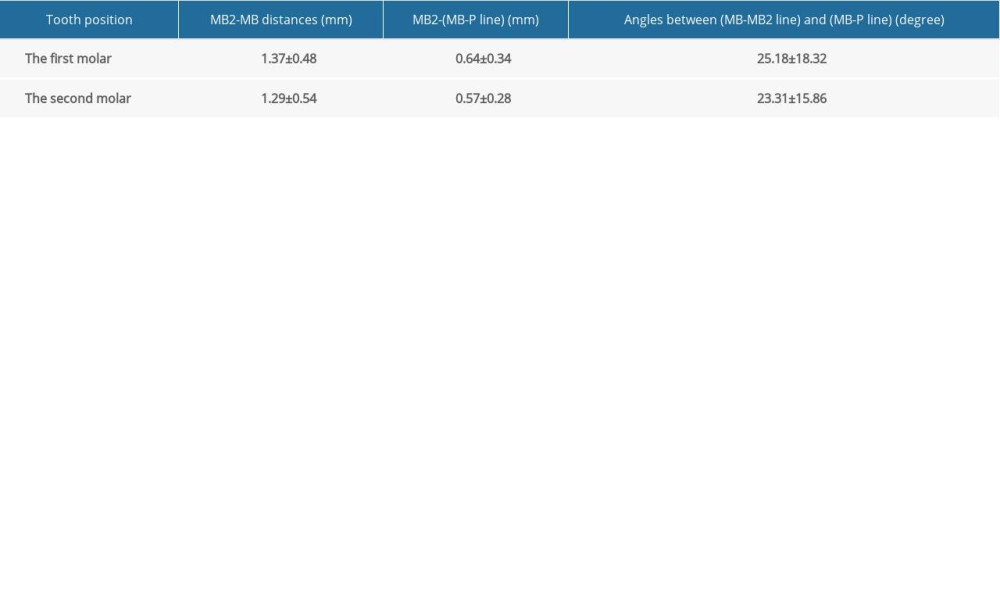 Table 5. Comparison of MB2 detection rate by micro-CT and tooth transparent method.
Table 5. Comparison of MB2 detection rate by micro-CT and tooth transparent method.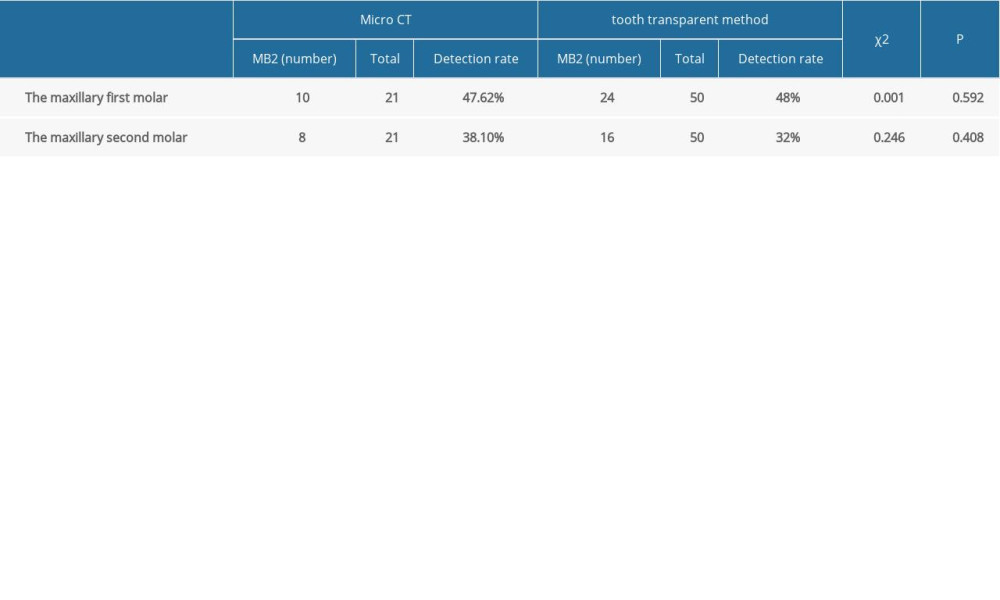
References
1. Pan J, Wang J, Hao L, The triple functions of D2 silencing in treatment of periapical disease: J Endod, 2017; 43; 272-78
2. Franciscatto GJ, Brennan DS, Gomes MS, Rossi-Fedele G, Association between pulp and periapical conditions and dental emergency visits involving pain relief: epidemiological profile and risk indicators in private practice in Australia: Int Endod J, 2020; 53; 887-94
3. Tomaszewska IM, Jarzębska A, Skinningsrud B, An original micro-CT study and meta-analysis of the internal and external anatomy of maxillary molars-implications for endodontic treatment: Clin Anat, 2018; 31; 838-53
4. Mazzi-Chaves J, Silva-Sousa Y, Leoni G, Micro-computed tomographic assessment of the variability and morphological features of root canal system and their ramifications: J Appl Oral Sci, 2020; 28; e20190393
5. Kulkarni V, Duruel O, Ataman-Duruel E, In-depth morphological evaluation of tooth anatomic lengths with root canal configurations using cone beam computed tomography in North American population: J Appl Oral Sci, 2020; 28; e20190103
6. Wu D, Hu DQ, Xin BC, Root canal morphology of maxillary and mandibular first premolars analyzed using cone-beam computed tomography in a Shandong Chinese population: Medicine, 2020; 99; e20116
7. Martins J, Alkhawas M, Altaki Z, Worldwide analyses of maxillary first molar second mesiobuccal prevalence: Amulticenter cone-beam computed tomographic study: J Endod, 2018; 44; 1641-49.e1641
8. Fu Y, Deng Q, Xie Z, Coronal root canal morphology of permanent two-rooted mandibular first molars with novel 3D measurements: Int Endod J, 2020; 53; 167-75
9. Hou BXComplications occurred in root canal mechanical preparation: the reason, prevention and management: Zhonghua Kou Qiang Yi Xue Za Zhi, 2019; 54(9); 605-11 [in Chinese]
10. Mohara NT, Coelho MS, de Queiroz NV, Root anatomy and canal configuration of maxillary molars in a Brazilian subpopulation: A 125-mum cone-beam computed tomographic study: Eur J Dent, 2019; 13; 82-87
11. Buchanan GD, Gamieldien MY, Tredoux S, Vally ZI, Root and canal configurations of maxillary premolars in a South African subpopulation using cone beam computed tomography and two classification systems: J Oral Sci, 2020; 62; 93-97
12. Li Y, Bao S, Yang X, Symmetry of root anatomy and root canal morphology in maxillary premolars analyzed using cone-beam computed tomography: Arch Oral Biol, 2018; 94; 84-92
13. Guo J, Vahidnia A, Sedghizadeh P, Enciso R, Evaluation of root and canal morphology of maxillary permanent first molars in a North American population by cone-beam computed tomography: J Endod, 2014; 40; 635-39
14. Schneider SW, A comparison of canal preparations in straight and curved root canals: Oral Surg Oral Med Oral Pathol, 1971; 32; 271-75
15. Zhang X, Xu N, Wang HG, A Cone-beam computed tomographic study of apical surgery-related morphological characteristics of the distolingual root in 3-rooted mandibular first molars in a Chinese population: J Endod, 2017; 43; 2020-24
16. Huang DM, Gao XJ, Tan H, Zhou XDAssociation of root canal therapy difficulty with canal anatomic factors in mandibular permanent incisors: Hua Xi Kou Qiang Yi Xue Za Zhi, 2006; 24(4); 366-69
17. Peters O, Current challenges and concepts in the preparation of root canal systems: A review: J Endod, 2004; 30; 559-67
18. Gorni F, Gagliani M, The outcome of endodontic retreatment: A 2-yr follow-up: J Endod, 2004; 30; 1-4
19. Lin LM, Rosenberg PA, Lin J, Do procedural errors cause endodontic treatment failure?: J Am Dent Assoc, 2005; 136; 187-93
20. Tomaszewska I, Jarzębska A, Skinningsrud B, An original micro-CT study and meta-analysis of the internal and external anatomy of maxillary molars-implications for endodontic treatment: Clin Anat, 2018; 31; 838-53
21. Pereria B, Martins JNR, Baruwa AO, Association between endodontically treated maxillary and mandibular molars with fused roots and periapical lesions: A cone-beam computed tomography cross-sectional study: J Endod, 2020; 46; 771-77
22. Magat G, Hakbilen S, Prevalence of second canal in the mesiobuccal root of permanent maxillary molars from a Turkish subpopulation: A cone-beam computed tomography study: Folia Morphol (Warsz), 2019; 78; 351-58
23. Kewalramani R, Murthy CS, Gupta R, The second mesiobuccal canal in three-rooted maxillary first molar of Karnataka Indian sub-populations: A cone-beam computed tomography study: J Oral Biol Craniofac Res, 2019; 9; 347-51
24. Zhang Z, Sun JComparative study of the diagnostic values of radio visiography, cone-beam computed tomography, and transparent teeth in the diagnosis of the first molar root canal system: Hua Xi Kou Qiang Yi Xue Za Zhi, 2013; 31(5); 441-47
25. Tzeng L, Chang M, Chang S, Analysis of root canal system of maxillary first and second molars and their correlations by cone beam computed tomography: J Formos Med Assoc, 2020; 119; 968-73
26. Saber SEDM, Ahmed MHM, Obeid M, Ahmed HMA, Root and canal morphology of maxillary premolar teeth in an Egyptian subpopulation using two classification systems: A cone beam computed tomography study: Int Endod J, 2019; 52; 267-78
27. Wolf T, Kozaczek C, Siegrist M: J Endod, 2020; 46; 794-800
28. de Lima C, de Souza L, Devito K, Evaluation of root canal morphology of maxillary premolars: A cone-beam computed tomography study: Aust Endod J, 2019; 45; 196-201
29. Alqedairi A, Alfawaz H, Al-Dahman Y, Cone-beam computed tomographic evaluation of root canal morphology of maxillary premolars in a Saudi population: Biomed Res Int, 2018; 2018 8170620
30. Pan J, Parolia A, Chuah S, Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography: BMC Oral Health, 2019; 19; 14
31. Martins J, Marques D, Mata A, Caramês J, Root and root canal morphology of the permanent dentition in a Caucasian population: A cone-beam computed tomography study: Int Endod J, 2017; 50; 1013-26
32. Camargo Dos Santos B, Pedano M, Giraldi C, Mesiobuccal root canal morphology of maxillary first molars in a Brazilian sub-population – a micro-CT study: Eur Endod J, 2020; 5; 105-11
33. Martins J, Quaresma S, Quaresma M, Frisbie-Teel J, C-shaped maxillary permanent first molar: A case report and literature review: J Endod, 2013; 39; 1649-53
34. Hudieb MI, Wakabayashi N, Abu-Hammad OA, Biomechanical effect of an exposed dental implant’s first thread: A three-dimensional finite element analysis study: Med Sci Monit, 2019; 25; 3933-40
35. Sfondrini MF, Gandini P, Alcozer R, Failure load and stress analysis of orthodontic miniscrews with different transmucosal collar diameter: J Mech Behav Biomed Mater, 2018; 87; 132-37
36. Scribante A, Sfondrini MF, Gatti S, Gandini P, Disinclusion of unerupted teeth by mean of self-ligating brackets: Effect of blood contamination on shear bond strength: Med Oral Patol Oral Cir Bucal, 2013; 18; e162-67
Figures
Figure 1. Root canal curvature measurement (Point A) the root canal orifice (Point B) the canal began to leave the long axis of the tooth (Point C) the apical foramenFigure 2. Illustration showing the categories of root canal morphologies in human permanent teeth according to the method by Vertucci.Figure 3. Diagram of MB2 root canal orifice positioning measurement.Figure 4. Representation of root canal curvature in different tooth positions and different observation directions. (A–C) Buccolingual direction of premolar (A) straight root canal (category I). (B) Moderately curved root canal (category II). (C) Severely curved root canal (category III). (D, E) Mesiodistal direction of premolar. (D) Straight root canal (category I) and severely curved root canal (category III). (E) Moderately curved root canal (category II). (F, G) Buccolingual direction of molar. (F) Straight root canal (category I) and severely curved root canal (category III). (G) Moderately curved root canal (category II). (H–J) Mesiodistal direction of molar. (H) Straight root canal (category I). (I) Moderately curved root canal (category II). (J) Severely curved root canal (category III).Figure 5. Representation of root canal types observed by transparent tooth method (A) Type I (1-1 double roots) (B) type I (1-1 single root) (C) type II (2-1) (D) type III (1-2-1) (E) Type IV (2-2) (F) type V (1-2) (G) type VI (2-1-2) (H) type VII (1-2-1-2).Figure 6. Representation root canal morphology by micro-CT (A) Type I (1-1) (B) Type II (2-1) (C) Type III (1-2-1) (D) Type IV (2-2) (E) type V (1-2) (F) type VI (2-1-2) (G) type VII (1-2-1-2) (H) Double root of mesial buccal (1-1 root canal). Tables
Table 1. Root canal curvature of maxillary premolar.Table 2. Root canal curvature of maxillary molar.Table 3. Distribution of main root canal configuration of 200 maxillary posterior teeth (n %).Table 4. Measurement results of MB2 orifice in micro-CT.Table 5. Comparison of MB2 detection rate by micro-CT and tooth transparent method.Table 1. Root canal curvature of maxillary premolar.Table 2. Root canal curvature of maxillary molar.Table 3. Distribution of main root canal configuration of 200 maxillary posterior teeth (n %).Table 4. Measurement results of MB2 orifice in micro-CT.Table 5. Comparison of MB2 detection rate by micro-CT and tooth transparent method. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387