20 February 2021: Clinical Research
A Retrospective Study of Factors Associated with Restoration of Thoracic Kyphosis in 43 Patients with Adolescent Idiopathic Scoliosis with Lenke Type 1 Curvature
Liyi Chen1ABCDEFG, Chong Liu1ABC, Shian Liao1BC, Chaojie Yu1DE, Tuo Liang1BC, Zhaojie Qin1BD, Shengsheng Huang1AB, Xuhua Sun1BC, Ming Yi1AB, Zhaojun Lu1AD, Zequn Wang1A, Guoyong Xu1B, Zide Zhang1C, Jiarui Chen1D, Jie Jiang1C, Xinli Zhan1AFG*DOI: 10.12659/MSM.929149
Med Sci Monit 2021; 27:e929149






Abstract
BACKGROUND: This retrospective study aimed to identify the factors associated with successful surgical correction of thoracic kyphosis (TK) in 43 patients with adolescent idiopathic scoliosis (AIS) with Lenke type 1 curvature, in which the major curve with the largest Cobb angle was mainly in the thoracic region.
MATERIAL AND METHODS: We collected data from patients with Lenke 1 AIS. The following parameters were measured: Cobb angle, side-bending Cobb angle, cervical lordosis (CL), TK, lumbar lordosis (LL), pelvic incidence (PI), sacral slope (SS), pelvic tilt (PT), the sagittal vertical axis (SVA), the center of a C7 plumb line to the center sacral vertical line (C7-CSVL), correction rate, Ponte osteotomy, flexibility, and screw density. Univariate analysis and multivariate logistic regression analyses were performed.
RESULTS: Among the 43 cases analyzed, the mean postoperative Cobb angle at the last follow-up, C7-CSVL, SVA, CL, TK, LL, PI, SS, and PT were respectively 21.33±9.47°, 10.41±8.45 mm, 19.68±14.33 mm, 16.19±7.45°, 23.12±7.45°, 50.33±11.37°, 49.70±9.83°, 39.42±8.11°, and 10.16±6.63°. Univariate analysis suggested that preoperative TK, preoperative LL, and Ponte osteotomy were statistically significant (P<0.05), and multivariate analysis suggested that preoperative LL and Ponte osteotomy were statistically significant (P<0.05).
CONCLUSIONS: The results of this study demonstrated that preoperative TK, preoperative LL, and Ponte osteotomy were related factors for maintaining normal TK. Multivariate analysis suggested that preoperative LL and the use of Ponte osteotomy with full-thickness segmental resection of the spinal posterior column resulted in the successful surgical correction of TK in patients with AIS with Lenke type 1 curvature.
Keywords: Factor Analysis, Statistical, Scoliosis, Thoracic Surgery, Adolescent, Cervical Vertebrae, Child, Kyphosis, Lumbar Vertebrae, Osteotomy, Postoperative Period, postural balance, Posture, Scheuermann Disease, Spinal Fusion, Thoracic Vertebrae
Background
Adolescent idiopathic scoliosis (AIS) involves multiple deformed planes generally, not only with coronal curvature and a decrease or increase of sagittal kyphosis on X-ray film, but also with an obvious axial rotation on computed tomography (CT) [1]. AIS is usually divided into Lenke types: curve type (1 through 6), a lumbar spine modifier (A, B, or C), and a sagittal thoracic modifier (−, N, or +), depending on the curvature and its degree within the different segments [2,3]. Although routine screening for scoliosis exposes adolescents to unnecessary radiographs, the potential benefits of early detection of scoliosis justify screening regimens [4]. According to the International Scientific Society on Scoliosis Orthopaedic and Rehabilitation Treatment guidelines, bracing, specific physiotherapeutic exercises to prevent scoliosis progression during growth, specific physiotherapeutic exercises during brace treatment and surgical therapy, and other conservative treatments are often performed [5]. Recently, more attention is being paid to the restoration and maintenance of the normal sagittal plane and coronal alignments of the main thoracic curvature [6,7]. The treatment of AIS with pedicle screw internal fixation can achieve a curative effect in a clinical application [8]. Previous studies have focused on obtaining the maximum coronal and surgical correction for AIS to improve cosmesis and function [3,9]. A study of 273 cases reviewed by Trobisch et al [10] indicated that coronal balance was closely related to the degree of correction of lumbar vertebrae after operation, based on logistic regression analysis. Surgical treatment of scoliosis should account for the effect of self-tension in the coronal plane, as well as compensation arising from the imbalance of the body [11].
However, to the best of our knowledge, little research has used multivariate logistic regression analysis of the sagittal plane parameters in Lenke type 1 AIS. Sagittal balance is equally important compared with coronal balance in terms of the overall evaluation of AIS. Currently, more attention is being paid to achieving a proper sagittal balance because it is critical to the successful surgical management of AIS [12,13]. Two surgical methods for maintaining sagittal balance are used in the treatment of AIS, including anterior and posterior approaches [14,15]. Some literature has reported that the kyphotic angle of the thoracic vertebrae usually cannot be restored effectively. Lonstein and Winter [16] found that the posterior orthopedic procedure did not achieve the purpose of surgery in 60% of cases if the patient’s preoperative thoracic kyphosis (TK) was less than 20°. At present, pedicle screws are widely used in the surgical correction of scoliosis, but there is no consensus on postoperative TK. For example, one study reported that TK decreased after the operation [17], but another reported that TK increased [18].
Although many studies have assessed TK in AIS, no generalized consensus has been reached on whether its restoration can be achieved after spinal surgical correction [12–18]. In addition, there are no known reports on the multivariate logistic regression analysis of coronal and sagittal plane parameters in Lenke type 1 AIS. Therefore, this retrospective study aimed to identify the factors associated with successful surgical correction of TK in 43 patients with AIS with Lenke type 1 curvature, in which the major curve with the largest Cobb angle was mainly in the thoracic region.
Material and Methods
PATIENT POPULATION:
This study to review 43 consecutive cases with Lenke 1 AIS was approved by the Institutional Review Board of Ethics Committee of the First Affiliated Hospital, Guangxi Medical University. Each participant and his or her parents were informed, and written consent was obtained. According to a new classification system, Lenke types can be divided into 6 curve types: Lenke 1 (main thoracic curvature), Lenke 2 (double thoracic curvature), Lenke 3 (double main curvature), Lenke 4 (3 main curvatures), Lenke 5 (thoracic lumbar curvature/lumbar curvature), and Lenke 6 (thoracic lumbar curvature/lumbar bending-structural main thoracic curvature) [2]. According to the relationship of the center sacral vertical line to the apex of the lumbar curve, and the sagittal curve measurement from the 5th to the 12th thoracic level, the lumbar spine modifier can be classified as A, B, or C [2]. A sagittal thoracic modifier can be divided into – (<10°), N (10–40°), and + (>40°) [2]. These patients (18 females and 25 males) included 35 cases of Lenke 1A, 2 cases of Lenke 1B, and 6 cases of Lenke 1C. The patients underwent posterior correction and instrumental spinal fusion with pedicle screws between May 2012 and August 2017. The inclusion criteria were patients with Lenke 1 AIS of the main thoracic curvature, with at least 1-year follow-up, for whom complete standing whole spine radiographs were available. The exclusion criteria were patients with a previous medical history of spinal surgery and manipulations that might affect flexibility. The included cases were separated into 3 groups based on their preoperative TK; group A had thoracic hypokyphosis (TK <20°), group B had normal TK (TK 20–40°), and group C had thoracic hyperkyphosis (TK >40°). Additionally, the patients were also divided into 2 groups according to postoperative TK for further analysis of factors: group 1 with a TK angle <20° after surgery and group 2 with a TK angle between 20° and 40° after surgery. All patients’ informed consent was obtained before the project was started.
SURGICAL TECHNIQUE:
All surgeries were performed by 2 similarly trained senior surgeons at our medical facility. Patients were placed in a prone position for the posterior approach, and an incision was then made to expose the transverse processes, the bilateral lamina, and articular processes. A Ponte osteotomy was performed, and the lower vertebral articular process and the superior vertebral body articular process were removed with a rongeur, with resection of the ligamentum flavum. Pedicle screw insertion methods for scoliosis surgery were carried out by the freehand technique [19]. Key vertebral pedicle screw strategy was applied in this study, following the operative procedure in previous literature [8]. Long-segment fusion was performed in this study. The spinal cord was detected using somatosensory evoked potentials and motor evoked potentials for all patients. The diameter and length of the screw were evaluated preoperatively by CT scan and measured during the operation. Lifting tools were used to lift both ends toward the middle, followed by a slightly concave distraction and convex compression, and then used for the curvature correction. This procedure simultaneously corrected the axial balance through the proper rotation of the rod. There were no observed deviations from the screw placements planned before surgery.
RADIOGRAPHIC MEASUREMENT:
A complete radiographic history consisting of preoperative and postoperative radiographs reviewed by certified radiologists was obtained. Two professional surgeons then used a picture archiving and communication system (Shenzhen Annet Information System, China) and Surgimap (Nemaris, Inc., New York, NY, USA) to take measurements, and the average value was obtained to avoid systematic deviations. The imaging data included the Cobb angle, side-bending Cobb angle, cervical lordosis (CL) [20], TK, lumbar lordosis (LL), pelvic incidence (PI), sacral slope (SS), and pelvic tilt (PT) [21]. The distance parameters measured included the sagittal vertical axis (SVA) and the center of a C7 plumb line to the center sacral vertical line (C7-CSVL). The ratio was calculated as follows: flexibility (%)=(preoperative Cobb–side-bending Cobb)/preoperative Cobb×100%, and correction rate (%)=(preoperative Cobb–postoperative Cobb)/preoperative Cobb×100% [17]. Screw density was equal to the number of screws per fusion segment times 2.
STATISTICAL ANALYSIS:
All the indexes are expressed as the mean±standard deviation. Measurements were assessed twice by a third spinal surgeon who did not participate in any of the surgical procedures, and the average value of the 2 measurements was calculated. SPSS version 20 (IBM Corporation, Armonk, New York, USA) was used for statistical analysis. The
Results
This study included a total of 43 patients with Lenke 1 AIS (18 females and 25 males), with a mean Risser sign of 2.12±1.48. Among the reviewed cases, there were 35 cases of Lenke 1A, 2 cases of Lenke 1B, and 6 cases of Lenke 1C, with a mean age of 14.70±2.47 years (range 11 to 19 years). In addition, the averages for the length of the follow-up period, length of hospital stays, operative time, and the number of pedicle screws were 34.84±19.77 months (12–74 months), 12.95±3.16 days, 169.84±36.60 min, and 13.44±2.71 (Table 1). The mean Cobb angle of the main thoracic curvature of the 43 Lenke 1 AIS patients in the coronal plane was 62.65±15.80° before surgery and 21.33±9.47° after surgical correction (Table 1). The correction rate acquired was 66.11%, and the preoperative flexibility was 45.77%. Orthopaedic effects can be seen (Figures 1, 2). A comparison of data between the preoperative and postoperative Cobb angles of the main thoracic curvature demonstrated a statistically significant result (
All patients were divided into 3 groups according to their preoperative TK to investigate the restoration of postoperative TK: group A had 25 patients, group B had 15 patients, and group C had 3 patients. The TK of the 25 patients in group A increased from 10.28±4.53° to 20.52±6.17°, and the preoperative TK and the last follow-up TK had a statistically significant difference in this group (
Additionally, the patients were divided into 2 groups according to postoperative TK; group 1 included 16 patients, and group 2 had 27 patients. Statistical differences were not observed for weight, age, height, sex, or Risser sign between the 2 groups (Table 4). Meanwhile, no significant difference was found in the number of pedicle screws, hospital days, operative time, or follow-up time in a comparison of the 2 groups (Table 4).
Univariate analysis showed that there was no statistical difference between group 1 and group 2 (
The parameters with statistically significant differences in the univariate analyses were subsequently included in a multivariate logistic regression analysis. Preoperative LL and Ponte osteotomy were noted to have statistically significant differences in the multivariate analysis (
Discussion
AIS generally involves multiple deformed planes, with not only coronal curvature and a decrease or increase of sagittal kyphosis on X-ray, but also an obvious axial rotation on CT [1]. A variety of surgical options are available in clinical surgery based on preoperative flexibility [22]. There are numerous studies on Lenke type 1 AIS regarding the types of curvature; the anatomical locations, structural features, and other features; and its natural history [1,2,23]. Several previous studies have focused on the coronal balance in AIS patients; however, there are no known reports on the independent factors that favor normal TK for Lenke 1 AIS. Consequently, no consensus has been reached on whether effective restoration of TK can be attained after spinal correction.
In this study, the mean Cobb angle of the main thoracic curvature decreased from 62.65±15.80° preoperatively to 21.33±9.47° postoperatively. The correction rate acquired was 66.11%. Satisfactory correction rates reported previously were based on the comparison of preoperative and postoperative results for 5 years, with 73% in one paper and 72.7% in another [24,25]. The difference could be because TK is mainly related to the shape and orientation of the thoracic vertebrae and intervertebral discs, while the thoracic vertebrae, ribs, and sternum help to enforce a relatively stable thoracic contour through bone or cartilage connections [26]. Although the cases reviewed for this study had follow-up for at least 1 year, the findings of the main thoracic curvature correction rate and those in other studies did not vary too much. However, a higher curvature correction rate might be achieved with prolonged follow-up time.
In this study, we found that the use of a pedicle screw system achieved a relatively satisfactory outcome for TK restoration, but previous studies debated the validity and value of TK restoration using a pedicle screw system. Different points of view were apparent in multiple groups of studies according to Liu et al [27], with the result that TK was increased in one set of follow-up data, but decreased in another. Similar results were reported in another study on pedicle screw therapy, where there was not a statistically significant difference between the preoperative and postoperative TK [28,29]. However, when Liu et al [27] analyzed data from different hospitals, they found that TK decreased after surgical correction. Postoperative TK was reported to decrease when segmental pedicle screw instrumentation was used for posterior correction owing to various factors, such as prone positioning, compressing maneuver, screw density, and direct vertebral derotation [30,31]. Nevertheless, Tao et al [18] reported that TK increased from before to after surgical correction, although the position of terminal fusion was different [18]. Similarly, a review of 92 cases by Dumpa et al [32] showed satisfactory recovery of TK in all groups of studies. The results of the current study showed that TK increased in comparison with preoperative and postoperative TK, and the sagittal plane was effectively restored. In this study, an increase in TK might cause a compensatory increase in CL and PT, so that the LL change was not obvious. This result was consistent with the results of the study by Roussouly et al [33]. TK was positively correlated with the increase of CL in the hypokyphotic group, and increased PT could maintain the patient’s spinal balance in lower PI [34].
The results of the current study demonstrated that preoperative TK, preoperative LL, and Ponte osteotomy were related factors for maintaining normal TK. Multivariate analysis suggested that preoperative LL and the use of Ponte osteotomy with full-thickness segmental resection of the spinal posterior column, resulted in successful surgical correction of TK in patients with AIS with Lenke type 1 curvature. With thoracic pedicle screw instrumentation used as the primary anchor, the Ponte procedure was successfully performed in 17 patients in a previous study [35]. In the process of osteotomy, the posterior skeletal structure of the spine is loosened, and the flexible structure of the spine is increased [36]. For patients with thoracic hypokyphosis, the orthopedics are appropriately extended. For patients with hyperkyphosis, proper orthopedics are performed to effectively maintain the sagittal plane of the spine balance. Feng et al [34] studied the sagittal balance of osteotomy and nonbone, and found that both groups could maintain TK. However, the TK correction angle in the osteotomy group was better than in the nonbone group, with the result of reducing the TK of patients with hyperkyphosis and increasing the TK of patients with thoracic hypokyphosis [34]. The Ponte osteotomy orthopedic technique was performed by Zhang et al [37], who achieved a coronal correction rate and sagittal correction rate of 57.73% and 41.23%, respectively. Ponte osteotomy was found to be an effective orthopedic treatment for patients with scoliosis [37]. Some patients in the current study underwent Ponte osteotomy, and the results showed that Ponte osteotomy was beneficial to maintain the normal curvature of TK. Further research is needed to increase the number of Ponte osteotomy cases.
In addition, the results of this study found that a larger preoperative LL surgery was conducive to maintaining the normal curvature of TK. A study review by Matsumoto et al [38] found evidence for a correlation between the decrease of TK and a decrease of LL [38]. Another study exploring the relationship between them also clearly stated that the findings followed the expected outcomes, and it additionally revealed that TK was closely connected to age [39]. Similarly, clinical imaging data from 180 cases indicated that the TK angle is connected to age to a certain extent before entering adulthood [40]. However, this study could not establish that TK was correlated with age. Also, the results of the univariate analysis did not reveal any significant difference between the proportion of pedicle screws and postoperative TK. These findings were confirmed by a pervious review of 269 cases in which a weak negative correlation was found between maintenance of TK balance and the number of implanting pedicle screws [6].
Several limitations should be considered in the current study, including the insufficient statistical power due to the relatively small number of cases reviewed. This article aimed to investigate the factors in maintaining normal TK in the coronal and sagittal parameters, but it did not include enough parameters such as axial position parameters and surgical segments. Since some of the reviewed cases underwent radiographic scans in other hospitals before their referral, those imaging data were not available for the current study. Also, even though all operations were conducted by 2 experienced surgeons, there might still have been some slight differences in their approaches. And finally, this study was a single-center retrospective study; therefore, a multicentered prospective study is needed to confirm the findings.
Conclusions
The results revealed that a normal TK could be effectively maintained after surgical correction. We found that preoperative TK, preoperative LL, and Ponte osteotomy were related factors for maintaining a normal TK. Multivariate analysis suggested that preoperative LL and the use of Ponte osteotomy with full-thickness segmental resection of the spinal posterior column resulted in successful surgical correction of TK in patients with AIS with Lenke type 1 curvature.
Figures
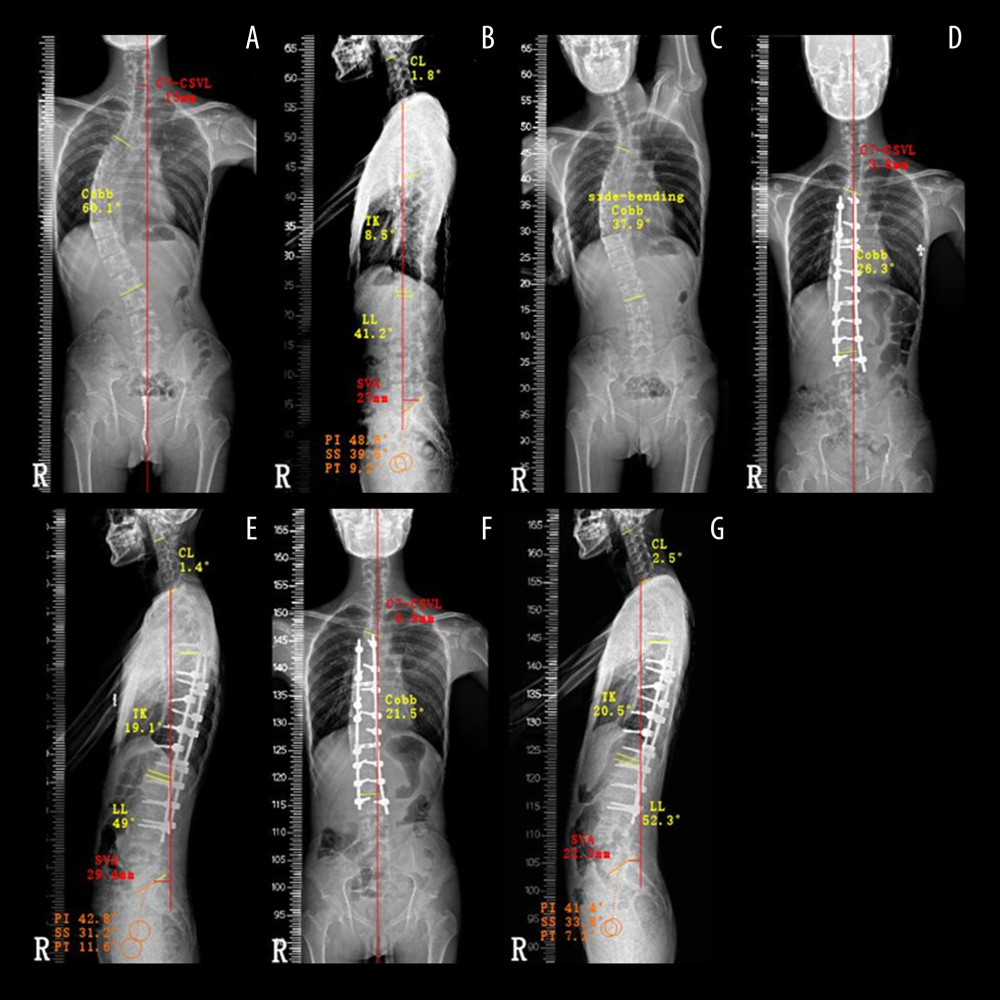 Figure 1. Representative case 1: an 18-year-old man with Lenke 1A adolescent idiopathic scoliosis. (A) Preoperative standing film showed a 15-mm center of a C7 plumb line to the center sacral vertical line (C7-CSVL) and a 60.1° main thoracic curve Cobb angle in the coronal plane. (B) Preoperative standing film showed a 27-mm sagittal vertical axis (SVA), 1.8° cervical lordosis (CL), 8.5° thoracic kyphosis (TK), 41.2° lumbar lordosis (LL), 48.8° pelvic incidence (PI), 39.6°sacral slope (SS), and 9.2° pelvic tilt (PT) in the sagittal plane. (C) Preoperative side-bending Cobb angle was 37.9°. (D) At 6 months after posterior thoracic fusion, the postoperative standing film showed a 3.8-mm C7-CSVL and a 26.3° main thoracic curve Cobb angle. (E) At 6 months after posterior thoracic fusion, the postoperative standing film showed a 29.4-mm SVA, 1.4° CL, 19.1° TK, 49° LL, 42.8° PI, 31.2° SS, and 11.6° PT. (F) At the last follow-up, the postoperative standing film showed a 0.9-mm C7-CSVL and a 21.5° main thoracic curve Cobb angle. (G) At the last follow-up, the postoperative standing film showed a 22.2-mm SVA, 2.5° CL, 20.5° TK, 52.3° LL, 41.4° PI, 33.8° SS, and 7.2° PT.
Figure 1. Representative case 1: an 18-year-old man with Lenke 1A adolescent idiopathic scoliosis. (A) Preoperative standing film showed a 15-mm center of a C7 plumb line to the center sacral vertical line (C7-CSVL) and a 60.1° main thoracic curve Cobb angle in the coronal plane. (B) Preoperative standing film showed a 27-mm sagittal vertical axis (SVA), 1.8° cervical lordosis (CL), 8.5° thoracic kyphosis (TK), 41.2° lumbar lordosis (LL), 48.8° pelvic incidence (PI), 39.6°sacral slope (SS), and 9.2° pelvic tilt (PT) in the sagittal plane. (C) Preoperative side-bending Cobb angle was 37.9°. (D) At 6 months after posterior thoracic fusion, the postoperative standing film showed a 3.8-mm C7-CSVL and a 26.3° main thoracic curve Cobb angle. (E) At 6 months after posterior thoracic fusion, the postoperative standing film showed a 29.4-mm SVA, 1.4° CL, 19.1° TK, 49° LL, 42.8° PI, 31.2° SS, and 11.6° PT. (F) At the last follow-up, the postoperative standing film showed a 0.9-mm C7-CSVL and a 21.5° main thoracic curve Cobb angle. (G) At the last follow-up, the postoperative standing film showed a 22.2-mm SVA, 2.5° CL, 20.5° TK, 52.3° LL, 41.4° PI, 33.8° SS, and 7.2° PT. 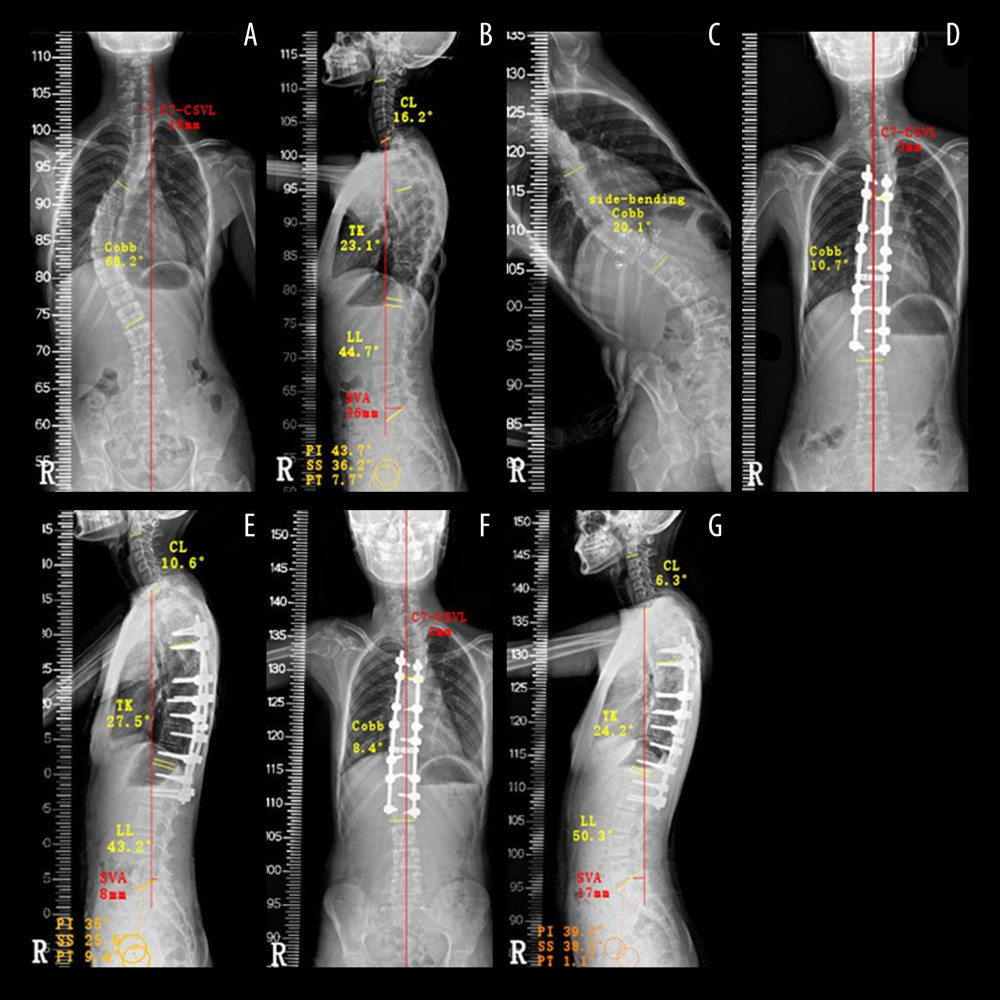 Figure 2. Representative case 2: a 13-year-old girl with Lenke 1A adolescent idiopathic scoliosis. (A) Preoperative standing film showed an 18-mm center of a C7 plumb line to the center sacral vertical line (C7-CSVL) and a 68.2° main thoracic curve Cobb angle in the coronal plane. (B) Preoperative standing film showed a 26-mm sagittal vertical axis (SVA), 16.2° cervical lordosis (CL), 23.1° thoracic kyphosis (TK), 44.7° lumbar lordosis (LL), 43.7° pelvic incidence (PI), 36.2° sacral slope (SS), and 7.7° pelvic tilt (PT) in the sagittal plane. (C) Preoperative side-bending Cobb angle was 20.1°. (D) At 6 months after posterior thoracic fusion, the postoperative standing film showed a 3-mm C7-CSVL and a 10.7° main thoracic curve Cobb angle. (E) At 6 months after posterior thoracic fusion, the postoperative standing film showed an 8-mm SVA, 10.6° CL, 27.5° TK, 43.2° LL, 35° PI, 25.6° SS, and 9.4°PT. (F) At the last follow-up, the postoperative standing film showed a 2-mm C7-CSVL and an 8.4° main thoracic curve Cobb angle. (G) At the last follow-up, the postoperative standing film showed a 17-mm SVA, 6.3° CL, 24.2° TK, 50.3° LL, 39.2° PI, 38.1° SS, and 1.1° PT.
Figure 2. Representative case 2: a 13-year-old girl with Lenke 1A adolescent idiopathic scoliosis. (A) Preoperative standing film showed an 18-mm center of a C7 plumb line to the center sacral vertical line (C7-CSVL) and a 68.2° main thoracic curve Cobb angle in the coronal plane. (B) Preoperative standing film showed a 26-mm sagittal vertical axis (SVA), 16.2° cervical lordosis (CL), 23.1° thoracic kyphosis (TK), 44.7° lumbar lordosis (LL), 43.7° pelvic incidence (PI), 36.2° sacral slope (SS), and 7.7° pelvic tilt (PT) in the sagittal plane. (C) Preoperative side-bending Cobb angle was 20.1°. (D) At 6 months after posterior thoracic fusion, the postoperative standing film showed a 3-mm C7-CSVL and a 10.7° main thoracic curve Cobb angle. (E) At 6 months after posterior thoracic fusion, the postoperative standing film showed an 8-mm SVA, 10.6° CL, 27.5° TK, 43.2° LL, 35° PI, 25.6° SS, and 9.4°PT. (F) At the last follow-up, the postoperative standing film showed a 2-mm C7-CSVL and an 8.4° main thoracic curve Cobb angle. (G) At the last follow-up, the postoperative standing film showed a 17-mm SVA, 6.3° CL, 24.2° TK, 50.3° LL, 39.2° PI, 38.1° SS, and 1.1° PT. 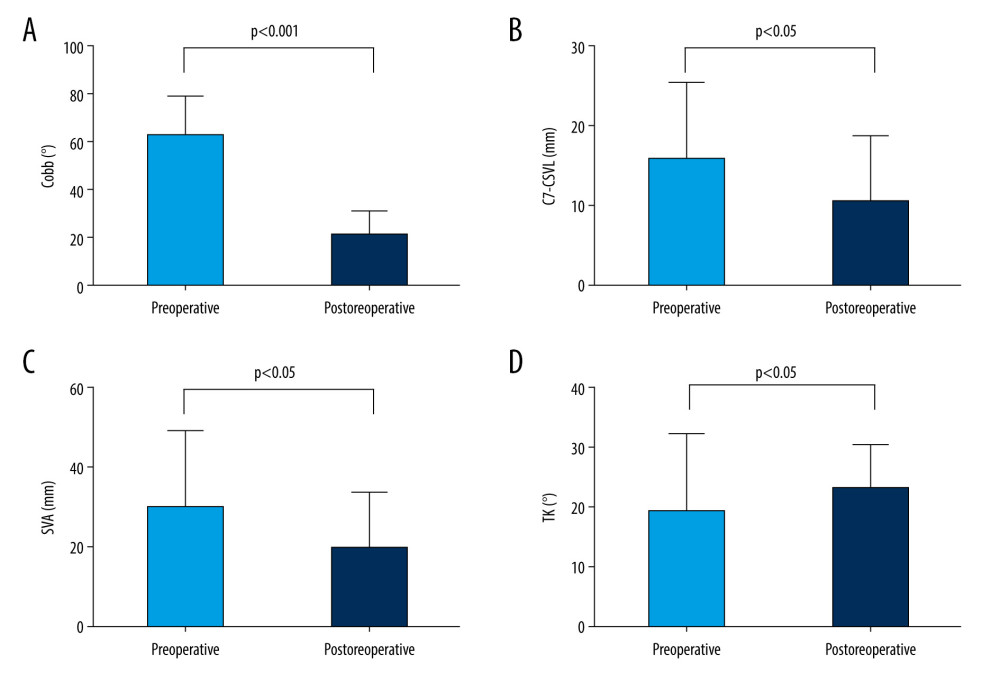 Figure 3. Comparison of parameters before and after surgery: (A) Cobb, (B) the center of a C7 plumb line to the center sacral vertical line (C7-CSVL), (C) sagittal vertical axis (SVA), and (D) thoracic kyphosis (TK).
Figure 3. Comparison of parameters before and after surgery: (A) Cobb, (B) the center of a C7 plumb line to the center sacral vertical line (C7-CSVL), (C) sagittal vertical axis (SVA), and (D) thoracic kyphosis (TK). 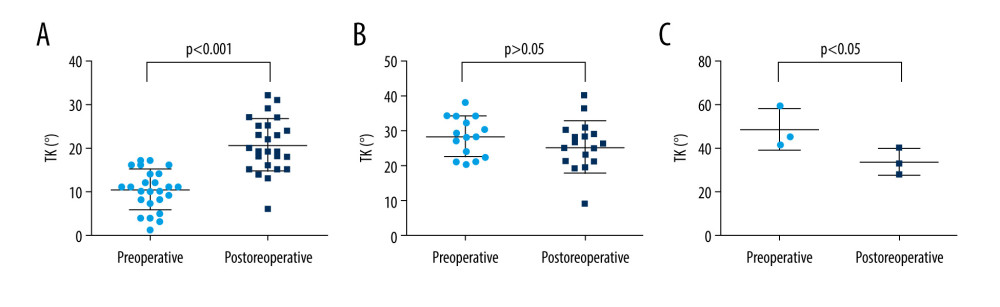 Figure 4. Comparison of thoracic kyphosis (TK): (A) group A (TK <20°), (B) group B (TK 20–40°), and (C) group C (TK > 40°).
Figure 4. Comparison of thoracic kyphosis (TK): (A) group A (TK <20°), (B) group B (TK 20–40°), and (C) group C (TK > 40°). Tables
Table 1. Mean±standard deviation (SD) of the patients’ clinical data. Table 2. Comparison of preoperative and postoperative measurements of parameters (mean±standard deviation).
Table 2. Comparison of preoperative and postoperative measurements of parameters (mean±standard deviation).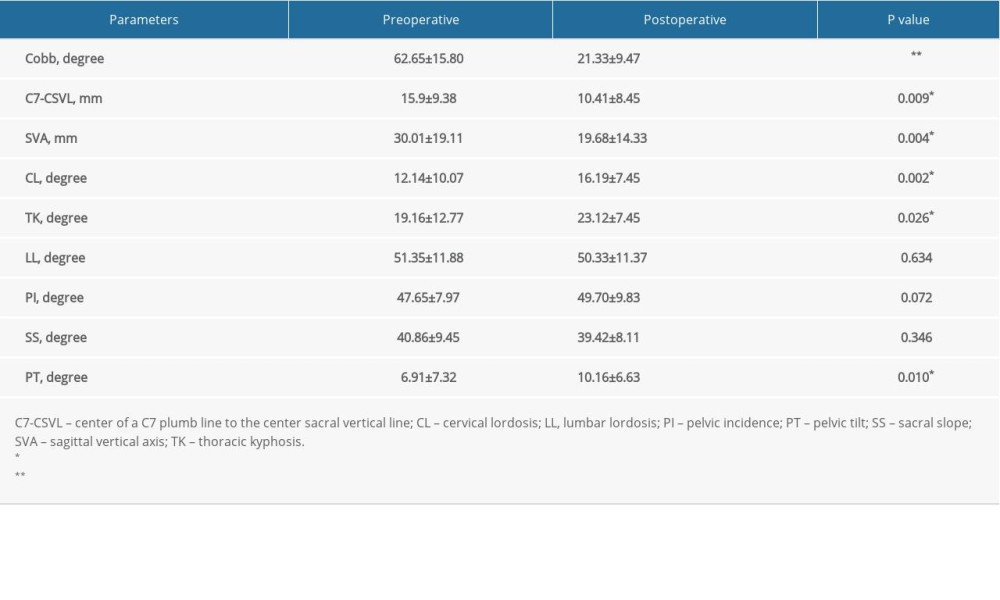 Table 3. Comparison of measurements of parameters between preoperative and last follow-up (mean±standard deviation)#.
Table 3. Comparison of measurements of parameters between preoperative and last follow-up (mean±standard deviation)#.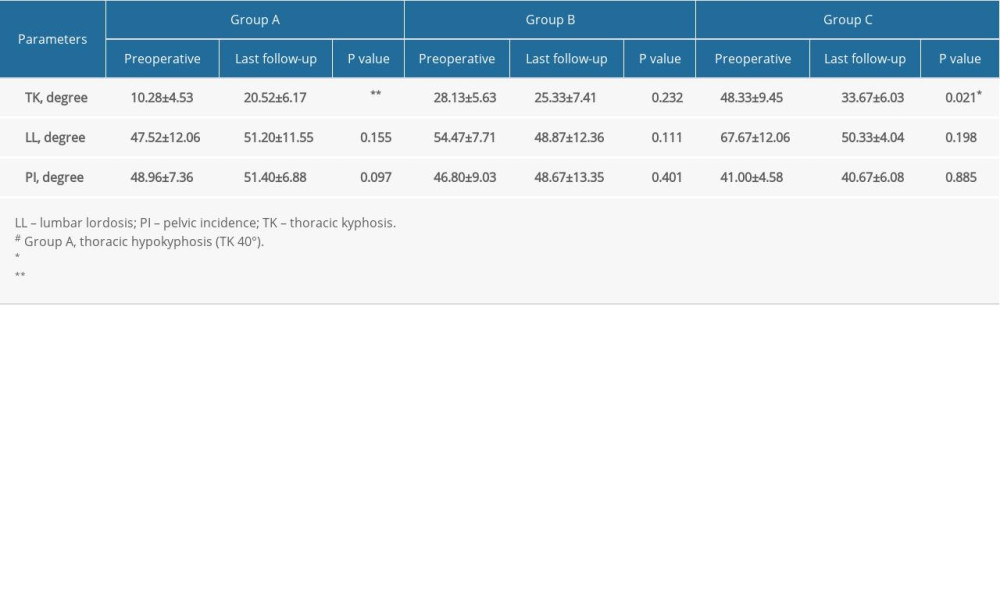 Table 4. Comparison of clinical parameters between group 1 and group 2 (mean±standard deviation)#.
Table 4. Comparison of clinical parameters between group 1 and group 2 (mean±standard deviation)#.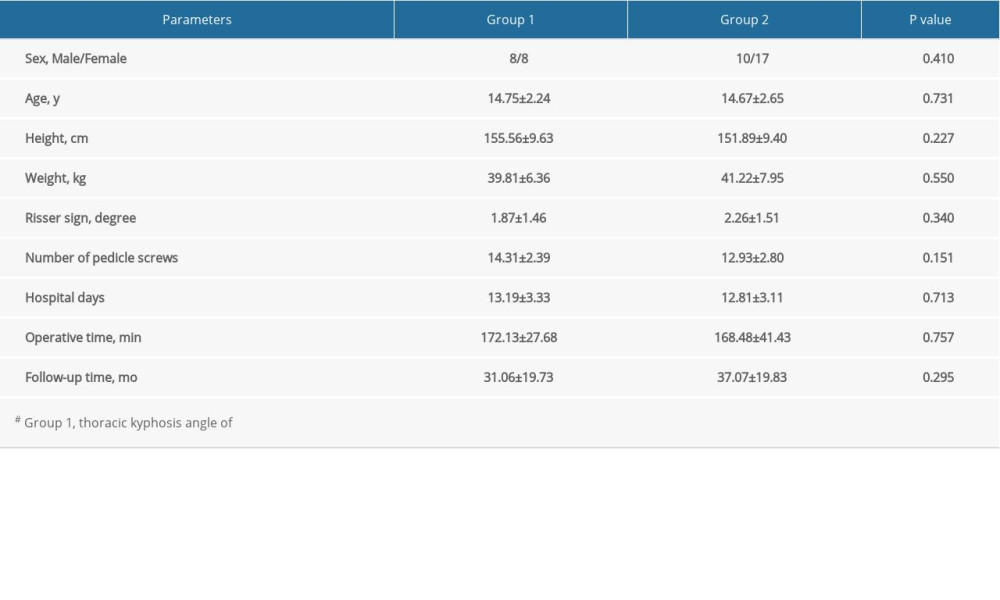 Table 5. Univariate analysis of parameters between the 2 groups (mean±standard deviation).
Table 5. Univariate analysis of parameters between the 2 groups (mean±standard deviation).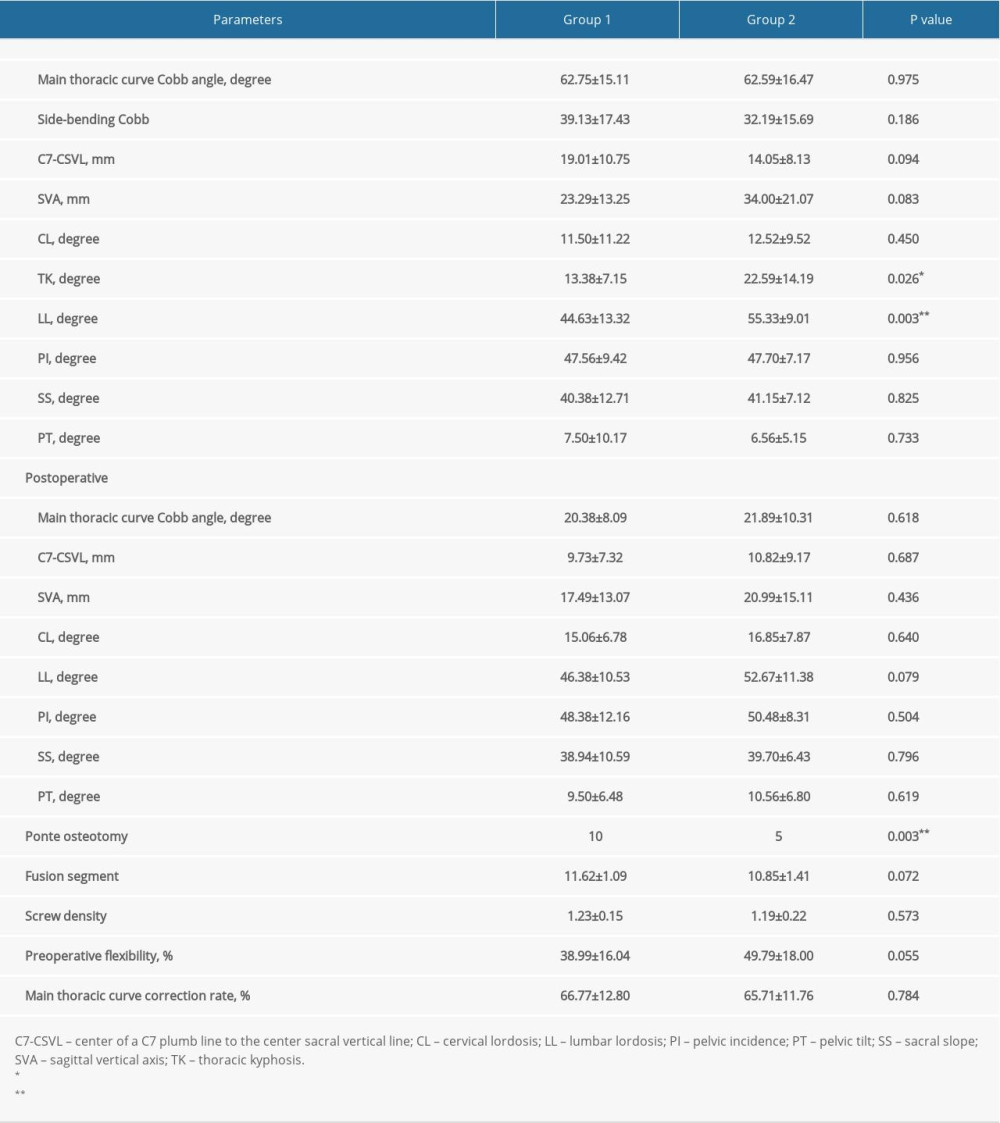 Table 6. Multivariate logistic regression analysis of parameters.
Table 6. Multivariate logistic regression analysis of parameters.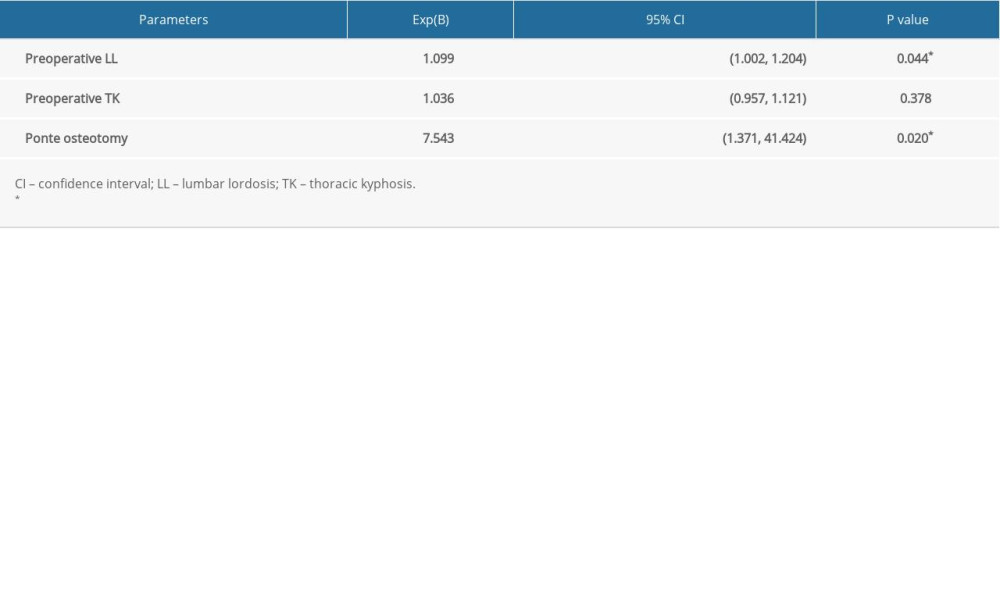
References
1. Weinstein S, Dolan L, Cheng J, Adolescent idiopathic scoliosis: Lancet, 2008; 371(9623); 1527-37
2. Lenke L, Betz R, Harms J, Adolescent idiopathic scoliosis. A new classification to determine extent of spinal arthrodesis: J Bone Joint Surg Am, 2001; 83(8); 1169-81
3. Lehman R, Lenke L, Keeler K, Operative treatment of adolescent idiopathic scoliosis with posterior pedicle screw-only constructs: Minimum three-year follow-up of one hundred fourteen cases: Spine (Phila Pa 1976), 2008; 33(14); 1598-604
4. Horne J, Flannery R, Usman S, Adolescent idiopathic scoliosis: Diagnosis and management: Am Fam Physician, 2014; 89(3); 193-98
5. Negrini S, Aulisa A, Aulisa L, 2011 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth: Scoliosis, 2012; 7(1); 3
6. Lonner B, Lazar-Antman M, Sponseller P, Multivariate analysis of factors associated with kyphosis maintenance in adolescent idiopathic scoliosis: Spine (Phila Pa 1976), 2012; 37(15); 1297-302
7. Lowenstein J, Matsumoto H, Vitale M, Coronal and sagittal plane correction in adolescent idiopathic scoliosis: A comparison between all pedicle screw versus hybrid thoracic hook lumbar screw constructs: Spine (Phila Pa 1976), 2007; 32(4); 448-52
8. Wei X, Zhou X, Yang Y, Key vertebral pedicle screw strategy for the correction of flexible Lenke type 1 adolescent idiopathic scoliosis: A preliminary study of a 5-year minimum radiographic follow-up: Spine (Phila Pa 1976), 2017; 42(16); 1226-32
9. Suk S, Lee S, Chung E, Selective thoracic fusion with segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis: More than 5-year follow-up: Spine (Phila Pa 1976), 2005; 30(14); 1602-9
10. Trobisch P, Samdani A, Pahys J, Cahill P, Postoperative trunk shift in Lenke 1 and 2 curves: How common is it? and analysis of risk factors: Eur Spine J, 2011; 20(7); 1137-40
11. Li M, Shen Y, Gao Z, Surgical treatment of adult idiopathic scoliosis: Long-term clinical radiographic outcomes: Orthopedics, 2011; 34(3); 180
12. Upasani V, Tis J, Bastrom T, Analysis of sagittal alignment in thoracic and thoracolumbar curves in adolescent idiopathic scoliosis: How do these two curve types differ?: Spine (Phila Pa 1976), 2007; 32(12); 1355-59
13. Hilibrand A, Tannenbaum D, Graziano G, The sagittal alignment of the cervical spine in adolescent idiopathic scoliosis: J Pediatr Orthop, 1995; 15(5); 627-32
14. Hempfing A, Ferraris L, Koller H, Is anterior release effective to increase flexibility in idiopathic thoracic scoliosis? Assessment by traction films: Eur Spine J, 2007; 16(4); 515-20
15. Kadoury S, Cheriet F, Beauséjour M, A three-dimensional retrospective analysis of the evolution of spinal instrumentation for the correction of adolescent idiopathic scoliosis: Eur Spine J, 2009; 18(1); 23-37
16. Lonstein J, Winter R, Comparison of anterior and posterior instrumentation for correction of adolescent thoracic idiopathic scoliosis: Spine (Phila Pa 1976), 1999; 24(19); 2067-68
17. Li M, Shen Y, Fang X, Coronal and sagittal plane correction in patients with Lenke 1 adolescent idiopathic scoliosis: A comparison of consecutive versus interval pedicle screw placement: J Spinal Disord Tech, 2009; 22(4); 251-56
18. Tao F, Shi Z, Xie Y, Determination of lowest instrumented vertebra by the location of apical vertebra in Lenke type 1 adolescent idiopathic scoliosis: Int Orthop, 2011; 35(4); 561-67
19. Kim Y, Lenke L, Bridwell K, Free hand pedicle screw placement in the thoracic spine: Is it safe?: Spine (Phila Pa 1976), 2004; 29(3); 333-42
20. Harrison D, Harrison D, Cailliet R, Cobb method or Harrison posterior tangent method: Which to choose for lateral cervical radiographic analysis: Spine (Phila Pa 1976), 2000; 25(16); 2072-78
21. Vidal C, Mazda K, Ilharreborde B, Sagittal spino-pelvic adjustment in severe Lenke 1 hypokyphotic adolescent idiopathic scoliosis patients: Eur Spine J, 2016; 25(10); 3162-69
22. Lee C, Hwang C, Lee D, Cho J, Five major controversial issues about fusion level selection in corrective surgery for adolescent idiopathic scoliosis: A narrative review: Spine J, 2017; 17(7); 1033-44
23. Glassman S, Sucato D, Carreon L, Does thoracic hypokyphosis matter in Lenke type 1 adolescent idiopathic scoliosis?: Spine Deform, 2013; 1(1); 40-45
24. Yu CH, Chen PQ, Ma SC, Pan CH, Segmental correction of adolescent idiopathic scoliosis by all-screw fixation method in adolescents and young adults. Minimum 5 years follow-up with SF-36 questionnaire: Scoliosis, 2012; 7; 5
25. Hwang S, Samdani A, Wormser B, Comparison of 5-year outcomes between pedicle screw and hybrid constructs in adolescent idiopathic scoliosis: J Neurosurg Spine, 2012; 17(3); 212-19
26. Mac-Thiong J, Labelle H, Charlebois M, Sagittal plane analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type: Spine (Phila Pa 1976), 2003; 28(13); 1404-9
27. Liu H, Li Z, Li S, Main thoracic curve adolescent idiopathic scoliosis: Association of higher rod stiffness and concave-side pedicle screw density with improvement in sagittal thoracic kyphosis restoration: J Neurosurg Spine, 2015; 22(3); 259-66
28. Sucato D, Agrawal S, O’Brien M, Restoration of thoracic kyphosis after operative treatment of adolescent idiopathic scoliosis: A multicenter comparison of three surgical approaches: Spine (Phila Pa 1976), 2008; 33(24); 2630-36
29. Liljenqvist U, Lepsien U, Hackenberg L, Comparative analysis of pedicle screw and hook instrumentation in posterior correction and fusion of idiopathic thoracic scoliosis: Eur Spine J, 2002; 11(4); 336-43
30. Watanabe K, Nakamura T, Iwanami A, Vertebral derotation in adolescent idiopathic scoliosis causes hypokyphosis of the thoracic spine: BMC Musculoskelet Disord, 2012; 13; 99
31. Kim Y, Lenke L, Cho S, Comparative analysis of pedicle screw versus hook instrumentation in posterior spinal fusion of adolescent idiopathic scoliosis: Spine (Phila Pa 1976), 2004; 29(18); 2040-48
32. Dumpa SR, Shetty AP, Aiyer SN, Reciprocal changes in sagittal alignment in adolescent idiopathic scoliosis patients following strategic pedicle screw fixation: Asian Spine J, 2018; 12(2); 300-8
33. Roussouly P, Labelle H, Rouissi J, Bodin A, Pre- and post-operative sagittal balance in idiopathic scoliosis: A comparison over the ages of two cohorts of 132 adolescents and 52 adults: Eur Spine J, 2013; 22(Suppl 2); S203-15
34. Feng J, Zhou J, Huang M, Clinical and radiological outcomes of the multilevel Ponte osteotomy with posterior selective segmental pedicle screw constructs to treat adolescent thoracic idiopathic scoliosis: J Orthop Surg Res, 2018; 13(1); 305
35. Geck M, Macagno A, Ponte A, Shufflebarger H, The Ponte procedure: Posterior only treatment of Scheuermann’s kyphosis using segmental posterior shortening and pedicle screw instrumentation: J Spinal Disord Tech, 2007; 20(8); 586-93
36. Gottlich C, Sponseller PD, Ponte osteotomy in pediatric spine surgery: JBJS Essent Surg Tech, 2020; 10(3); e19.00001
37. Zhang Y, Hai Y, Tao L, Posterior multiple-level asymmetrical Ponte osteotomies for rigid adult idiopathic scoliosis: World Neurosurg, 2019; 127; e467-73
38. Matsumoto H, Colacchio N, Schwab F, Flatback revisited: Reciprocal loss of lumbar lordosis following selective thoracic fusion in the setting of adolescent idiopathic scoliosis: Spine Deform, 2015; 3(4); 345-51
39. Liu S, Zhang Y, Bao H, Could pelvic parameters determine optimal postoperative thoracic kyphosis in Lenke type 1 AIS patients?: BMC Musculoskelet Disord, 2018; 19(1); 74
40. Mac-Thiong JM, Berthonnaud E, Dimar JR, Sagittal alignment of the spine and pelvis during growth: Spine (Phila Pa 1976), 2004; 29(15); 1642-47
Figures
Figure 1. Representative case 1: an 18-year-old man with Lenke 1A adolescent idiopathic scoliosis. (A) Preoperative standing film showed a 15-mm center of a C7 plumb line to the center sacral vertical line (C7-CSVL) and a 60.1° main thoracic curve Cobb angle in the coronal plane. (B) Preoperative standing film showed a 27-mm sagittal vertical axis (SVA), 1.8° cervical lordosis (CL), 8.5° thoracic kyphosis (TK), 41.2° lumbar lordosis (LL), 48.8° pelvic incidence (PI), 39.6°sacral slope (SS), and 9.2° pelvic tilt (PT) in the sagittal plane. (C) Preoperative side-bending Cobb angle was 37.9°. (D) At 6 months after posterior thoracic fusion, the postoperative standing film showed a 3.8-mm C7-CSVL and a 26.3° main thoracic curve Cobb angle. (E) At 6 months after posterior thoracic fusion, the postoperative standing film showed a 29.4-mm SVA, 1.4° CL, 19.1° TK, 49° LL, 42.8° PI, 31.2° SS, and 11.6° PT. (F) At the last follow-up, the postoperative standing film showed a 0.9-mm C7-CSVL and a 21.5° main thoracic curve Cobb angle. (G) At the last follow-up, the postoperative standing film showed a 22.2-mm SVA, 2.5° CL, 20.5° TK, 52.3° LL, 41.4° PI, 33.8° SS, and 7.2° PT.Figure 2. Representative case 2: a 13-year-old girl with Lenke 1A adolescent idiopathic scoliosis. (A) Preoperative standing film showed an 18-mm center of a C7 plumb line to the center sacral vertical line (C7-CSVL) and a 68.2° main thoracic curve Cobb angle in the coronal plane. (B) Preoperative standing film showed a 26-mm sagittal vertical axis (SVA), 16.2° cervical lordosis (CL), 23.1° thoracic kyphosis (TK), 44.7° lumbar lordosis (LL), 43.7° pelvic incidence (PI), 36.2° sacral slope (SS), and 7.7° pelvic tilt (PT) in the sagittal plane. (C) Preoperative side-bending Cobb angle was 20.1°. (D) At 6 months after posterior thoracic fusion, the postoperative standing film showed a 3-mm C7-CSVL and a 10.7° main thoracic curve Cobb angle. (E) At 6 months after posterior thoracic fusion, the postoperative standing film showed an 8-mm SVA, 10.6° CL, 27.5° TK, 43.2° LL, 35° PI, 25.6° SS, and 9.4°PT. (F) At the last follow-up, the postoperative standing film showed a 2-mm C7-CSVL and an 8.4° main thoracic curve Cobb angle. (G) At the last follow-up, the postoperative standing film showed a 17-mm SVA, 6.3° CL, 24.2° TK, 50.3° LL, 39.2° PI, 38.1° SS, and 1.1° PT.Figure 3. Comparison of parameters before and after surgery: (A) Cobb, (B) the center of a C7 plumb line to the center sacral vertical line (C7-CSVL), (C) sagittal vertical axis (SVA), and (D) thoracic kyphosis (TK).Figure 4. Comparison of thoracic kyphosis (TK): (A) group A (TK <20°), (B) group B (TK 20–40°), and (C) group C (TK > 40°). Tables
Table 1. Mean±standard deviation (SD) of the patients’ clinical data.Table 2. Comparison of preoperative and postoperative measurements of parameters (mean±standard deviation).Table 3. Comparison of measurements of parameters between preoperative and last follow-up (mean±standard deviation)#.Table 4. Comparison of clinical parameters between group 1 and group 2 (mean±standard deviation)#.Table 5. Univariate analysis of parameters between the 2 groups (mean±standard deviation).Table 6. Multivariate logistic regression analysis of parameters.Table 1. Mean±standard deviation (SD) of the patients’ clinical data.Table 2. Comparison of preoperative and postoperative measurements of parameters (mean±standard deviation).Table 3. Comparison of measurements of parameters between preoperative and last follow-up (mean±standard deviation)#.Table 4. Comparison of clinical parameters between group 1 and group 2 (mean±standard deviation)#.Table 5. Univariate analysis of parameters between the 2 groups (mean±standard deviation).Table 6. Multivariate logistic regression analysis of parameters. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387