15 March 2021: Clinical Research
Risk Factors and Safety Analyses for Intrapartum Fever in Pregnant Women Receiving Epidural Analgesia During Labor
Jie Ren1ABCDEFG, Tao Wang1BCF, Bo Yang1ABD, Lihua Jiang1ABEG*, Linglan Xu1CDF, Xiaoyuan Geng1CDE, Qian Liu1CFDOI: 10.12659/MSM.929283
Med Sci Monit 2021; 27:e929283






Abstract
BACKGROUND: We aimed to explore the factors leading to epidural-related maternal fever and the influence of intrapartum fever on neonates.
MATERIAL AND METHODS: A retrospective analysis was performed on data from pregnant women who received epidural analgesia during labor. The primary aim was to determine the influence of epidural labor analgesia on the incidence of intrapartum fever in pregnant women. The secondary aim was to determine the influence of intrapartum fever on neonates.
RESULTS: Logistic regression analysis showed that premature rupture of membranes (OR=2.008, 95% CI: 1.551–2.600), vaginal examination performed more than 6 times (OR=1.681, 95% CI: 1.286–2.197), long duration of labor (OR=1.090, 95% CI: 1.063–1.118), and long time from rupture of membranes to delivery (OR=1.048, 95% CI: 1.010–1.087) were all risk factors for intrapartum fever in pregnant women with epidural labor analgesia. Regarding the secondary research outcome, the incidence of intrapartum fever was significantly associated with the number of neonates with Apgar score of 10 delivered from pregnant women with epidural labor analgesia (P<0.05). There was no statistically significant difference in the transfer rate of newborns to the Neonatal Intensive Care Unit (NICU) (P>0.05).
CONCLUSIONS: Premature rupture of membranes, vaginal examination performed more than 6 times, long duration of labor, and long time from rupture of membranes to delivery are all factors raising the risk of fever during epidural labor analgesia. Although intrapartum fever in the mothers had a significant influence on the number of neonates with Apgar score of 10, it did not affect the outcome of neonates in terms of NICU transfer rate.
Keywords: Anesthesia, Caudal, Factor Analysis, Statistical, Fever, Logistic Models, Anesthesia, Epidural, Apgar Score, Infant, Newborn, Labor, Obstetric, Obstetric Labor Complications, Pregnancy, Pregnant Women, Risk Factors
Background
Epidural analgesia is regarded as the criterion standard for labor analgesia, and has considerable analgesic effects. Compared with other analgesic methods, epidural analgesia yields higher levels of satisfaction in pregnant women [1]. In general, epidural analgesia causes a reduction in body core temperature due to peripheral vasodilatation [2]. However, epidural-related maternal fever (ERMF) has been observed in multiple studies [3–5]. Approximately 20% to 30% of pregnant women who receive epidural labor analgesia will develop intrapartum fever. Although the mechanism underlying ERMF is not known, several studies suggest a non-infectious cause [6,7]; for example, an exaggerated non-infectious inflammatory response by proinflammatory cytokines in women laboring with an epidural [6]. Kozlov [8] recently proposed a role for the TRPV1 receptor (also known as the capsaicin receptor). The author hypothesized that local anesthetics act as agonists/antagonists at this receptor, that antagonist actions may cause hyperthermia through changes in thermoregulation, and that agonist actions may cause the release of IL-6 and other inflammatory cytokines, which are known to cause fever. In a word, these studies support the potential involvement of non-infectious inflammation. ERMF may lead to poor pregnancy outcomes and increase the incidence of neonatal complications [9,10]. Accumulating evidence has confirmed that epidural analgesia is independently responsible for maternal fever during labor [6,11]. What are the other risk factors besides epidural analgesia? Here, we carried out a retrospective analysis of a large number of pregnant women to identify the factors that induce fever during the administration of labor analgesia. Our intention was to provide reference guidelines to help physicians take appropriate measures to reduce the adverse effects of fever during labor.
Material and Methods
STUDY DESIGN, SETTING, AND POPULATION:
This was a retrospective study carried out in our hospital that reviewed the risk factors associated with ERMF and evaluated the influence of intrapartum fever on neonates. Ethics approval for this study was provided by the institutional review board of the Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China (Approval number: 2020); the requirement for informed consent was waived. The study was carried out between January 2019 and October 2019. The included patients were pregnant women who fulfilled the inclusion criteria (below) and had received epidural analgesia during labor. The included patients were divided into 495 pregnant women who had a fever during labor (Group F) and 1556 pregnant women who had a normal temperature during labor (Group C).
The inclusion criteria were as follows: (1) singleton, vertex presentation, full-term pregnancy; (2) voluntary choice of epidural labor analgesia; (3) vaginal delivery assisted by the obstetrician; (4) pregnant but without the use of nonsteroidal analgesics in the delivery room; (5) American Society of Anesthesiologists (ASA) physical status II or III.
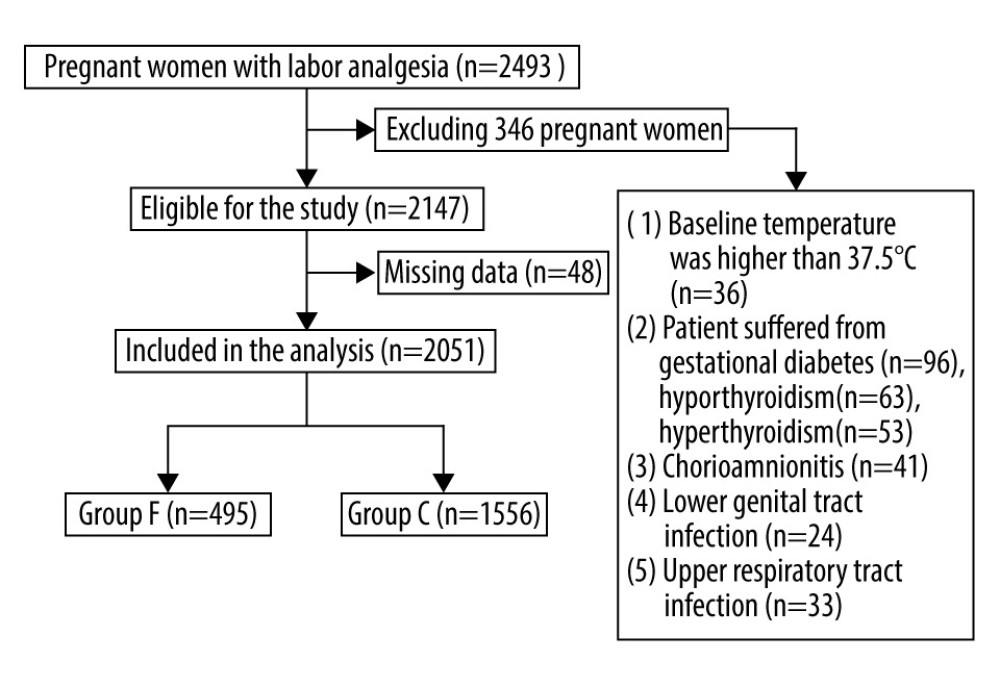
Pregnant women were excluded for the following reasons: (1) baseline body temperature in the delivery room was higher than 37.5°C; (2) metabolic diseases such as gestational diabetes, hypothyroidism, or hyperthyroidism; (3) lower genital tract infection or upper respiratory tract infection; (4) placental pathology examination results indicating a diagnosis of chorioamnionitis; (5) cesarean section due to emergency situations such as fetal distress during labor; (6) electronic records were not complete.
ANALGESIA METHODS:
By evaluating the regular contractions of each pregnant woman, the attending obstetrician determined those who could deliver vaginally and enter the delivery room for labor. An intravenous line was placed in one of the upper arms, and maternal blood pressure was monitored in the other arm. Maternal heart rate was monitored as well as fetal heart rate. Epidural labor analgesia was administered according to the needs of each pregnant woman at any time point. For this, the pregnant women were placed in left lateral decubitus position. We then performed an epidural puncture in the L3–4 intervertebral space. We then fitted a reinforced epidural catheter and injected 5 ml of 1.5% chloroprocaine with 1: 200 000 adrenaline. The pregnant women were then observed for 5 min. If the pregnant women did not show any adverse reactions during this observation period, we then started the electronic patient-controlled epidural analgesia pump. The analgesia pump delivers 240 ml of 0.08% ropivacaine and 0.4 μg/ml sufentanil. The model of patient-controlled epidural analgesia (PCEA) was adopted. The PCEA mode settings were as follows: The first dose was 6–10 ml/instance, the loading dose was 6 ml/h, the lock-out interval was 20 min, and the single supplementary patient-controlled analgesia (PCA) dose was 5 ml/instance. During the first and second stages of labor, we kept the level of analgesia no higher than T10. After the third stage of labor, we set the analgesia pump to a background infusion dose of 6 ml/h and cancelled the PCA dose; this allowed us to inhibit the pain associated with uterine contraction after delivery. Finally, the epidural catheter was removed after all the prepared solutions had been used up.
DATA COLLECTION:
All data were acquired from the electronic medical records system of the Third Affiliated Hospital of Zhengzhou University, including age, height, weight, gestational time in weeks, body temperature, length of labor process, membrane rupture mode and time to delivery, number of vaginal examinations, dilatation of the uterine cervix during epidural labor analgesia, duration of labor, amniotic fluid status, weight of newborn, and the use of oxytocin. Body mass index (BMI) and the duration of analgesia were calculated by the researchers. (The time of epidural labor analgesia refers to the interval between the timepoint at which the pregnant woman first received the epidural analgesia and the timepoint at the end of her third stage of labor).
EXPOSURE:
Monitoring and temperature evaluations of the pregnant women were conducted as follows. After a 30-min rest period in the delivery room, we began a series of temperature measurements. The temperature of the tympanic membrane was measured using an infrared cochlear thermometer at 1-h intervals for 2 h after delivery. The probe was placed into the external auditory canal; the tympanic membrane is directly opposite this location. If the body temperature during this time period exceeded 37.5°C, then a diagnosis of intrapartum fever was made, and we carried out physical cooling and asked the pregnant woman to drink more water. If the body temperature exceeded 38.5°C, then we removed 5 ml of venous blood as a sample for routine blood tests and a C-reactive protein test. If there was obvious infection, then antipyretics were used as a treatment option. We monitored the effects of drug treatment and whether any adverse reactions occurred. We then sent the placenta to the pathology department for pathological examination. The temperature of the labor room and delivery room was 20–24°C and the relative humidity was 45–60%. Pregnant women who developed fever during labor analgesia were designated as group F, whereas those who did not were designated as group C.
The vital signs of all the pregnant women were monitored closely, along with changes in fetal heart rate. The attending obstetrician selected the mode of delivery according to the fetal heart rate, the progression of labor, the position of the fetus, and the downward movement of the fetal head. Cases involving fetal distress and other emergencies were treated immediately by cesarean section to terminate the pregnancy. (The indications for fetal distress were strictly observed.)
OUTCOMES:
The main outcomes were: duration of labor, premature rupture of membranes, time from rupture of membranes to delivery, number of vaginal examinations, dilatation of the uterine cervix during epidural labor analgesia, delivery times, amniotic fluid status, weight of the newborn, use of oxytocin, BMI, and the duration of epidural analgesia. The secondary outcome was the influence of intrapartum fever on the neonate, including Neonatal Intensive Care Unit (NICU) admission rate and Apgar scores of 10 at 1 min and 5 min.
STATISTICAL ANALYSIS:
SPSS version 21.0 statistical software was used for all statistical analyses. The
Results
PREGNANT WOMEN T TEST CHARACTERISTICS:
The Figure 1 shows the flow diagram of the study. A total of 2493 pregnant women utilized labor analgesia in our facility during the study period. After excluding 346 of them, 2147 pregnant women were eligible for the study. Among these, 48 had missing data. In the end, 2051 pregnant women were included in the analysis.
General information relating to the pregnant women involved in this study is given in Table 1. There were no significant differences between group F and group C (P>0.05). A comparison of the risk factors for fever between the 2 groups of pregnant women is presented in Table 2.
We then analyzed the risk factors for fever in the 2 groups and made comparisons using the independent-samples
Logistic regression analysis of the risk factors for intrapartum fever is presented in Table 3. Taking intrapartum fever as the dependent variable, the independent-samples t test identified several significantly associated variables: duration of labor, time from rupture of membranes to delivery, duration of epidural labor analgesia, premature rupture of the membranes, and vaginal examination performed more than 6 times. These significant independent variables were then included in our multivariate logistic regression analysis. The results showed that premature rupture of membranes, vaginal examination performed more than 6 times, long duration of labor, and long time from rupture of membranes to delivery were all identified as risk factors for fever during labor; however, long duration of epidural analgesia was not identified as a risk factor for fever.
Finally, we compared the effect of fever on the neonates, between the 2 groups of pregnant women; these data are presented in Table 4. There were no significant differences between the 2 groups with regard to NICU admission rate (P>0.05). However, the number of neonates with Apgar scores of 10 at 1 min and 5 min was significantly lower in group F than in group C (P<0.05).
Discussion
With the increased popularization of labor analgesia, ERMF has begun to attract significant attention from obstetricians and anesthesiologists. In 1989, Fusi [5] was the first to propose that epidural labor analgesia was closely associated with fever in pregnant women, although the specific mechanism involved remained unclear. Our present results identified several risk factors for intrapartum fever: premature rupture of membranes, vaginal examination performed more than 6 times, long duration of labor, and long time from rupture of membranes to delivery.
We found that long duration of labor and vaginal examination performed more than 6 times were both related to fever during labor; these findings are similar to those in previous research described by Curtin et al [11,12]. It is possible that long periods of labor consume a greater proportion of physical resources. This may reduce immunity and thus increase the likelihood of infection [13]. Excessive vaginal examinations can lead to mechanical damage to the vaginal mucosa and the destruction of the vagina’s natural protective barrier, thus increasing the risk of infection and fever [14]. The premature rupture of membranes also results in a loss of fetal protection. We found that the risk of intrapartum fever was also associated with increased lengths of time between premature membrane rupture and fetal delivery. This increased time serves to exacerbate exposure of the uterine cavity or fetus to potential microbial threats, including those associated with vaginal infection [14].
Most scholars believe that prolonged periods of epidural analgesia increase the risk of fever during labor and that this may be related to changes in the thermoregulatory center or mechanisms associated with non-infectious inflammation or the specific role of local anesthetics [15]. For example, epidural labor analgesia can reduce heat dissipation by blocking the sympathetic nerves and thus causing the contraction of blood vessels above the level of analgesia. Epidural analgesia can also reduce pain, skeletal muscle activity, and respiratory rate, and increase the threshold for sweating. Epidural labor analgesia is not synchronous to cold and warm blocks; these occur earlier, although cold stimulation continues to operate. As a consequence, the thermoregulation center begins to show biological changes that result in an increase in body heat [16]. In the present study, we found that the duration of epidural analgesia in the F group was significantly longer than that in the C group, as determined by the independent-samples
In the present study, we determined that the rate of maternal fever associated with epidural labor analgesia was approximately 20%. In a previous study, Segal et al [20] reported that maternal fever can lead to a lower vaginal delivery rate and a higher incidence rate of neonatal disease. This may be related to an increase in heart rate, cardiac output, oxygen consumption, and catecholamine release when pregnant women develop fever during childbirth [21], thus resulting in an increased uterine temperature, abnormal fetal heat dissipation caused by the high temperature environment, and adverse outcomes such as fetal distress [22]. Collectively, these factors can increase the rate of cesarean section in pregnant women. Among the neonatal complications, the most noteworthy factors are that maternal fever is related to low Apgar scores, high oxygen demand, a high supplemental ventilation rate, hypotonia, and neonatal encephalopathy [23,24]. Although we did identify some effects on the number of neonates with Apgar scores of 10, we observed no other serious complications; these findings are consistent with previous studies, such as that reported by Sharma et al [25]. However, possible detrimental effects of maternal fever on the fetus have been a subject of significant controversy [26].
There were limitations to the present study that should be considered. For example, the investigators had no control over the quality of the recorded temperature. Furthermore, there are some other risk factors that were not included, such as types and concentrations of local anesthetics. These were not included because the types and concentrations of local anesthetics used in our hospital have not changed. The next step is to proceed to a prospective study that includes neonatal body temperature as an observational indicator.
Comfortable and safe delivery is the expectation of parturients and the goal of maternal healthcare during delivery. The emergence of epidural analgesia increased the possibility of achieving these goals. However, the potential adverse maternal and neonatal effects induced by intrapartum fever require further investigation [27]. Although we found some risk factors associated with ERMF, we can reduce the occurrence of ERMF by controlling these factors. The mechanism of ERMF needs more attention, which will be a long and difficult process. ERMF is a noteworthy issue for which more attention is needed.
Conclusions
Our analysis identified several risk factors for fever during labor in women receiving epidural analgesia: premature rupture of membranes, vaginal examination performed more than 6 times, long duration of labor, and long time from rupture of membranes to delivery. Therefore, we should take active measures to reduce the number of unnecessary vaginal examinations, adopt strict asepsis measures, and make reasonable use of oxytocin to reduce the time taken for the labor process. We should also take steps to actively manage labor to reduce the incidence of fever.
Tables
Table 1. Comparison of general information for the pregnant women in the F group and the C group. Table 2. Comparison of the risk factors for fever between the 2 groups of pregnant women.
Table 2. Comparison of the risk factors for fever between the 2 groups of pregnant women.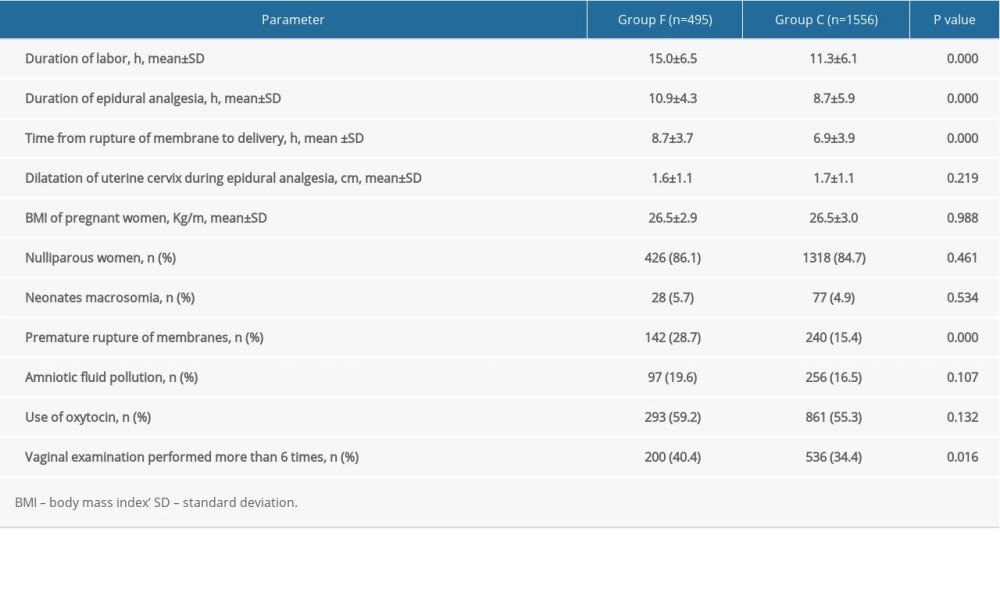 Table 3. Logistic regression analysis of the risk factors for intrapartum fever.
Table 3. Logistic regression analysis of the risk factors for intrapartum fever.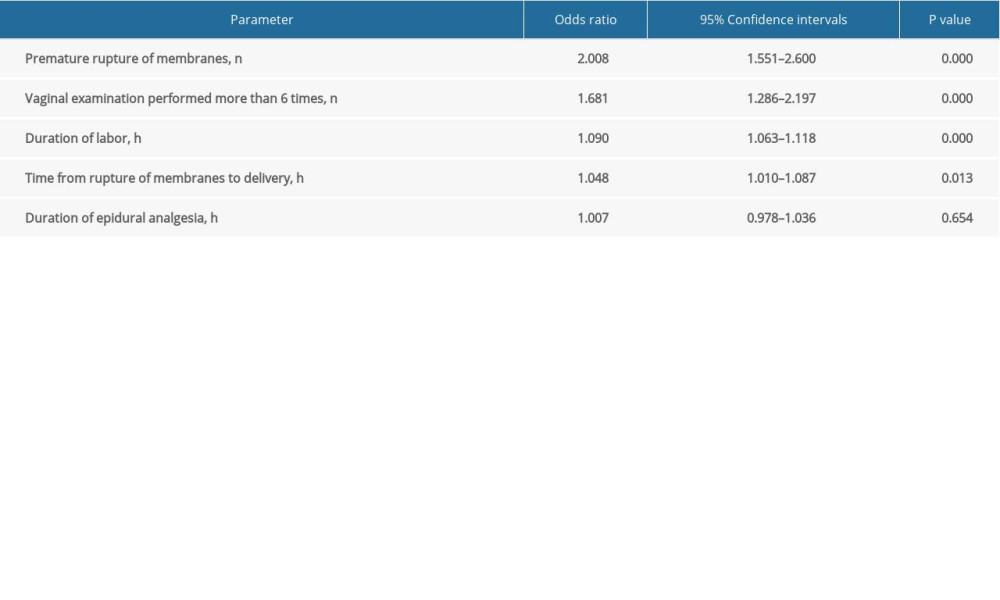 Table 4. The effect of fever between the 2 groups of pregnant women with regards to neonates.
Table 4. The effect of fever between the 2 groups of pregnant women with regards to neonates.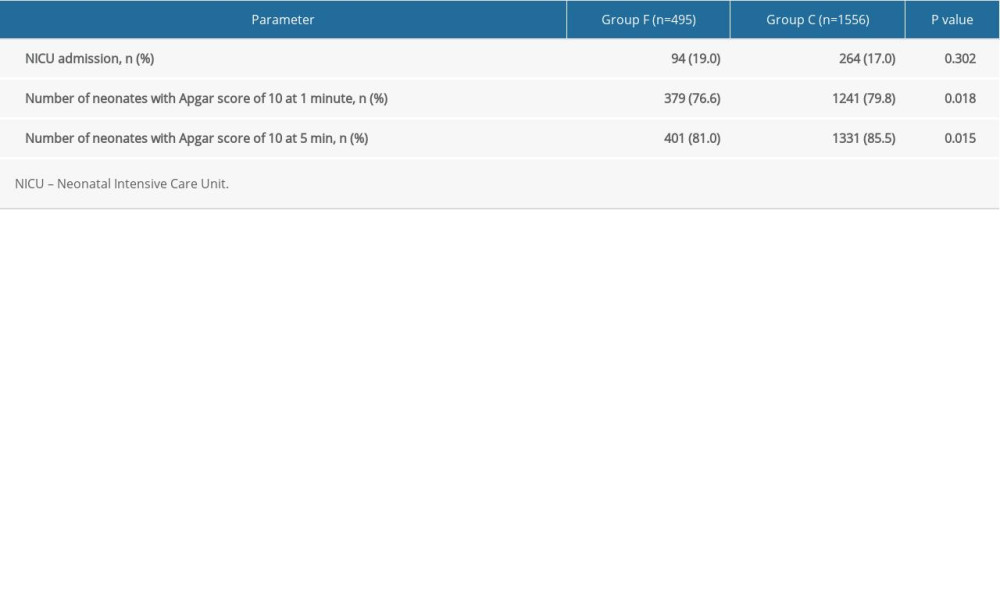
References
1. Wong CA, Scavone BM, Peaceman AM, The risk of cesarean delivery with neuraxial analgesia given early versus late in labor: N Engl J Med, 2005; 352(7); 655-65
2. Matsukawa T, Sessler DI, Christensen R, Heat flow and distribution during epidural anesthesia: Anesthesiology, 1995; 83(5); 961-67
3. Goetzl L, Rivers J, Zighelboim I, Intrapartum epidural analgesia and maternal temperature regulation: Obstet Gynecol, 2007; 109(3); 687-90
4. Smulian JC, Bhandari V, Vintzileos AM, Intrapartum fever at term: Serum and histologic markers of inflammation: Am J Obstet Gynecol, 2003; 188(1); 269-74
5. Fusi L, Steer PJ, Maresh MJ, Beard RW, Maternal pyrexia associated with the use of epidural analgesia in labour: Lancet, 1989; 1(8649); 1250-52
6. Sultan P, David AL, Fernando R, Ackland GL, Inflammation and epidural-related maternal fever. Proposed mechanisms: Anesth Analg, 2016; 122(5); 1546-53
7. , Practice Bulletin No. 177. Obstetric analgesia and anesthesia: Obstet Gynecol, 2017; 129(4); e73-89
8. Kozlov I, Why labor epidural causes fever and why lidocaine burns on injection? Role of TRPV1 receptor in hyperthermia: Possible explanation of mechanism of hyperthermia during labor epidural and burning sensation on injection of local anesthetics: Open J Anesthesiol, 2012; 2; 134-37
9. Sultan P, Segal S, Epidural-related maternal fever: Still a hot topic, but what are the burning issues?: Anesth Analg, 2020; 130(2); 318-20
10. Frölich MA, Esame A, Zhang K, What factors affect intrapartum maternal temperature? A prospective cohort study: Maternal intrapartum temperature: Anesthesiology, 2012; 117(2); 302-8
11. Curtin WM, Katzman PJ, Florescue H, Intrapartum fever, epidural analgesia and histologic chorioamnionitis: J Perinatol, 2015; 35(6); 396-400
12. Sharma SK, Epidural analgesia during labor and maternal fever: Curr Opin Anaesthesiol, 2000; 13(3); 257-60
13. Goetzl L, Cohen A, Frigoletto F, Maternal epidural use and neonatal sepsis evaluation in afebrile mothers: Pediatrics, 2001; 108(5); 1099-102
14. , Practice bulletins No. 139. Premature rupture of membranes: Obstet Gynecol, 2013; 122(4); 918-30
15. Sharpe EE, Arendt KW, Epidural labor analgesia and maternal fever: Clin Obstet Gynecol, 2017; 60(2); 365-74
16. Banerjee S, Steer PJ, The rise in maternal temperature associated with regional analgesia in labour is harmful and should be treated: Int J Obstet Anesth, 2003; 12(4); 280-84
17. Zhou X, Li J, Deng S, Ropivacaine at different concentrations on intrapartum fever, IL-6 and TNF-α in parturient with epidural labor analgesia: Exp Ther Med, 2019; 17(3); 1631-36
18. Fan Y, Hou W, Feng S, Programmed intermittent epidural bolus decreases the incidence of intra-partum fever for labor analgesia in primiparous women: A randomized controlled study: Arch Gynecol Obstet, 2019; 300(6); 1551-57
19. Chen X, Ni X, Zhang Y, The association of labor epidural analgesia with low concentration of ropivacaine and maternal fever: A retrospective study: J Clin Anesth, 2020; 65; 109613
20. Segal S, Labor epidural analgesia and maternal fever: Anesth Analg, 2010; 111(6); 1467-75
21. Leighton BL, Halpern SH, The effects of epidural analgesia on labor, maternal, and neonatal outcomes: A systematic review: Am J Obstet Gynecol, 2002; 186(5 Suppl. Nature); S69-77
22. Macaulay JH, Bond K, Steer PJ, Epidural analgesia in labor and fetal hyperthermia: Obstet Gynecol, 1992; 80(4); 665-69
23. Törnell S, Ekéus C, Hultin M, Low Apgar score, neonatal encephalopathy and epidural analgesia during labour: A Swedish registry-based study: Acta Anaesthesiol Scand, 2015; 59(4); 486-95
24. Greenwell EA, Wyshak G, Ringer SA, Intrapartum temperature elevation, epidural use, and adverse outcome in term infants: Pediatrics, 2012; 129(2); e447-54
25. Sharma SK, Rogers BB, Alexander JM, A randomized trial of the effects of antibiotic prophylaxis on epidural-related fever in labor: Anesth Analg, 2014; 118(3); 604-10
26. Thierrin L, Mercier FJEpidural analgesia and fever during labor: J Gynecol Obstet Biol Reprod (Paris), 2005; 34(5); 423-26 [in French]
27. Li CJ, Xia F, Xu SQ, Shen XF, Concerned topics of epidural labor analgesia: Labor elongation and maternal pyrexia: A systematic review: Chin Med J (Engl), 2020; 133(5); 597-605
Tables
Table 1. Comparison of general information for the pregnant women in the F group and the C group.Table 2. Comparison of the risk factors for fever between the 2 groups of pregnant women.Table 3. Logistic regression analysis of the risk factors for intrapartum fever.Table 4. The effect of fever between the 2 groups of pregnant women with regards to neonates.Table 1. Comparison of general information for the pregnant women in the F group and the C group.Table 2. Comparison of the risk factors for fever between the 2 groups of pregnant women.Table 3. Logistic regression analysis of the risk factors for intrapartum fever.Table 4. The effect of fever between the 2 groups of pregnant women with regards to neonates. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387