14 June 2021: Clinical Research
A Cluster Transmission of Coronavirus Disease 2019 and the Prevention and Control Measures in the Early Stage of the Epidemic in Xi’an, China, 2020
Hui Zhang1DE, Shuxuan Song2EF, Zhijun Chen3B, Miao Bai4B, Zhen He2C, Ting Fu2C, Kun Liu2AEG, Zhongjun Shao2AG*DOI: 10.12659/MSM.929701
Med Sci Monit 2021; 27:e929701






Abstract
BACKGROUND: At the beginning of the COVID-19 pandemic, a cluster outbreak caused by an imported case from Hubei Province was reported in Xi’an City, Shaanxi Province, China. Ten patients from 2 families and 1 hospital were involved in the transmission.
MATERIAL AND METHODS: We conducted an epidemiological investigation to identify the cluster transmission of COVID-19. The demographic, epidemiological, clinical, laboratory, and cluster characteristics were described and analyzed.
RESULTS: From January 27 to February 13, 2020, a total of 10 individuals were confirmed to be infected with SARS-CoV-2 by the nucleic acid testing of nasopharyngeal swabs from 2 families and 1 hospital. Among the confirmed cases, 7 had atypical clinical symptoms and 3 were asymptomatic. The median times from onset to diagnosis and to discharge were 3.5 days (range, 1-5 days) and 19.5 days (range, 16-38 days), respectively. There were 4 patients whose exposure dates were 1, 3, 3, and 2 days earlier than the onset dates of their previous-generation cases, respectively. Four prevention and control measures were effectively used to interrupt the disease transmission.
CONCLUSIONS: SARS-CoV-2 can be easily transmitted within families and in hospitals, and asymptomatic patients could act as a source of disease transmission. The results of this outbreak at the early epidemic stage support the recommendation that individuals with confirmed COVID-19 and all their close contacts should be subjected to medical quarantined observation and nucleic acid screening as early as possible, even if they do not have any symptoms. Meanwhile, people in high-risk areas should improve their protective measures.
Keywords: asymptomatic infections, Coronavirus Infections, Disease Outbreaks, Adolescent, Aged, 80 and over, COVID-19, COVID-19 Nucleic Acid Testing, Carrier State, Mass Screening, Pandemics, Quarantine, Real-Time Polymerase Chain Reaction, Reverse Transcriptase Polymerase Chain Reaction, SARS-CoV-2, young adult
Background
The fast spread of novel COVID-19 led to a global pandemic [1], and as of February 8, 2021, a total of 105 805 951 confirmed cases and 2 312 278 deaths were reported from 237 countries or regions worldwide [2]. There are several reasons explaining the rapid dissemination of COVID-19. First, SARS-CoV-2, the pathogen causing COVID-19, has high transmissibility and can be transmitted through the respiratory tract, particularly when individuals are in close contact, and other routes [3,4]. Second, there were large numbers of asymptomatic or minimally symptomatic carriers [5], and many studies demonstrated that asymptomatic cases play an important role in the disease transmission. Third, and most importantly, a lack of adoption of effective COVID-19 prevention and control measures made most countries vulnerable to the rapid spread of the disease, which in turn exacerbated further transmission.
There have been many studies on COVID-19, but despite the development of better understanding of the disease, the pandemic has become more serious. Many countries are still struggling to contain COVID-19, particularly the United States, where the cumulative COVID-19 cases and resulting deaths are over 18.82 million and 329 000, respectively [2]. In contrast, China, as the most seriously affected country in the early stage of the COVID-19 epidemic, has brought the disease under control successfully, which might be attributed to aggressive containment measures [6]. China was the first country to report COVID-19 and to recognize the seriousness of the new emerging disease. To slow the spread of the disease during the first stage of this global pandemic, with little knowledge and no effective vaccine or specific drug treatment for COVID-19, a range of nonpharmaceutical interventions were adopted, including prohibiting all travel, locking down cities, wearing masks, and social distancing; these measures were verified to be effective [7–10]. After paying a huge price, China has become the first country in the world to successfully contain the domestic spread of COVID-19. On September 7, the World Health Organization stated that China has brought the disease to a very low level [11] because all cases in the previous 20 days were imported and the people were quarantined right away. Up to February 8, 2021, the confirmed cases and deaths in China were 101 316 and 4 831, respectively [2].
Therefore, the experiences and practices of fighting against COVID-19 could serve as an invaluable reference for other countries or regions to contain the further development of COVID-19. Here, we report a cluster of SARS-CoV-2 infections in the early stage of the epidemic that occurred in Xi’an, Shaanxi Province, which was joint with Hubei Province, to provide more practical evidence for the prevention and control of COVID-19 and to highlight the importance of a swift response to the disease.
Material and Methods
STUDY DESIGN:
On January 27, 2020, a suspected case of COVID-19 in a person with a long history of residence in Xiaogan City (the secondary focus of COVID-19 in Hubei Province) was reported by hospital A in Xi’an City. The hospital immediately collected nasopharyngeal swab samples, which were sent to the local Center for Disease Control and Prevention (CDC) for nucleic acid testing. On January 28, the CDC reported that the case (index patient) was positive for SARS-CoV-2 nucleic acid. Then, 9 other cases were successively identified in the next 16 days, including 4 second-generation patients, 2 third-generation patients, 1 fourth-generation patient, and 2 fifth-generation patients.
DATA COLLECTION AND ANALYSIS:
The data of patients were obtained from the epidemiological investigation during the COVID-19 outbreak in Xi’an City. A confirmed case was defined as an individual with positive respiratory swabs and clinical symptoms [12]. The date of onset of asymptomatic cases was defined as the date of collection of positive swab specimens, while the date of diagnosis was determined as the date of a positive test [13]. Using a unified questionnaire from the Third Edition of Novel Coronavirus Prevention and Control Protocol [14], the investigators had face-to-face interviews with the people with confirmed COVID-19 or had face-to-face or telephone interviews with their families and other informed persons (including medical staff) to obtain details on demographic characteristics, clinical symptoms, treatment history, and activity patterns (including history of travel, residence, exposure, and close contacts for 14 days prior to quarantine). Two investigators (HZ and ZJC) cross-checked the acquired data to make sure the information was correct. The demographic, epidemiological, clinical, and cluster characteristics of the 10 patients were described and analyzed.
LABORATORY TESTING:
The nasopharyngeal swabs obtained from the patients were tested by real-time reverse-transcription polymerase chain reaction (RT-PCR) assay for SARS-CoV-2 or a genetic sequence that matches SARS-CoV-2, using from detection reagents from Shanghai Bojie Medical Technology Co., Ltd. and Shanghai Jienuo Biotechnology Co., Ltd.
ETHICS STATEMENT:
This study was approved by the Institutional Review Board of the Xi’an City Center for Disease Control and Prevention (XA20200504). We obtained written consent from all the patients, and all the description and analysis were anonymized to protect the individuals’ privacy.
Results
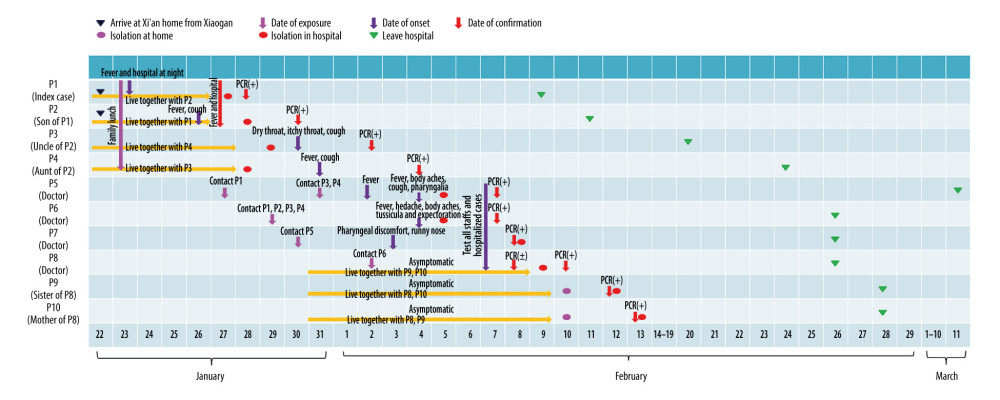
Ten individuals were confirmed as having SARS-CoV-2 infection, affecting 2 families and a public general hospital. We numbered the cases from 1 to 10 according to the order of illness onset (Figure 1).
Patient 1, the index case, was a 45-year-old woman living in Xiaogan City, Hubei Province. On January 22, she drove from Xiaogan to Xi’an with her husband and son. The next day, she developed a fever of 38.5°C and went to hospital A. She underwent a computed tomography (CT) examination, and the result was normal. From January 24 to 26, she had no fever during the day but had fevers up to 38.4°C at night. On January 27, she went to hospital A for re-examination, and she was questioned by the traffic police because the car license showed that the car was from Hubei Province. She was sent to hospital A and SARS-COV-2 infection was confirmed by a positive nucleic acid detection result on January 28. There were 6 close contacts related with her. Patient 2 was thought to be the second generation of this outbreak, along with patients 3, 4, and 5; patients 3 and 4 were family members of the index case and patient 5 was a doctor. Patients 6 and 7 were infected by the family member and the doctor, respectively. Patient 6 transmitted the disease to patient 8, who then spread it to family members, patients 9 and 10. Other detail information is shown in Table 1.
In the cluster, only 2 cases (patients 1 and 2) had an exposure history from traveling in an epidemic area of Hubei Province, while other cases had no exposure history in Hubei and no history of contacting other suspected sources (Table 1). Six cases were familial transmission, and 4 cases were nosocomial infection. The median times from onset to diagnosis and to discharge were 3.5 days (range, 1.0–5.0 days) and 19.5 days (range, 16.0–38.0 days), respectively. The median incubation period of COVID-19 was 4.0 days (range, 1.0–8.0 days), according to the shortest exposure time of patients 1 to 10. The day when patients 3 and 4 had a meal with patients 1 and 2 was 1 and 3 days earlier than the onset of the later 2, respectively, the day patient 7 contacted patient 5 was 3 days earlier than the onset for patient 5, and the exposure day of patient 8 was 2 days earlier than the onset for patient 6. The exposure time of the next generation was 3 days earlier than the onset of previous generation (Figure 1). At the time of admission, mycoplasma pneumoniae, chlamydia infection, and influenza A and B virus infection were excluded for all cases.
Of the 10 confirmed cases, 7 cases had varying degrees of clinical symptoms (Table 2) and 3 cases were asymptomatic. Fever and cough were the most common symptoms, reported in 5 (71%) and 5 (71%) individuals, respectively, and 1 adult was diagnosed as having severe pneumonia. The results of chest CT presented varying degrees of ground-glass pulmonary lesions upon admission for all patients, except patient 2, a teenager.
Discussion
There were 10 patients confirmed in the cluster transmission of COVID-19 in the early stage of the epidemic from January 27 to February 13, 2020. The median incubation period was 4.0 days, which was consistent with previous studies [15–17]. The median time from onset to confirmation was 3.5 days, which was much shorter than in a previous study [18] and could be attributable to the definition of exposure time in this study.
Patient 1 had a long history of living in the focus of COVID-19 and was regarded as the index case of this outbreak. Patient 2 also lived in Xiaogan, but he was a student at a middle school, where he spent much of his time and had relatively smaller chance of contact with other sources of infection. No cases were found in the school. It was difficult to define the infectious source for patient 2, and the first apparent indication of human-to-human transmission in this cluster was detected with confirmed infection of patient 3. Upon patient 1 having a clinically diagnosed suspected case on the evening of 27 January, Xi’an CDC immediately conducted medical observation and nucleic acid testing for all close contacts, then confirmed patients 2–4. Due to the lack of emergency experience and inadequate protection in the early stage, 2 doctors working in hospital A (patients 5 and 6) were infected, most likely through contact with patients 1, 3, or 4. Patient 5 was regarded as the second-generation because she had been in close contact with patient 1 for up to an hour, while patient 6 had not. Furthermore, with the swift response in contact tracing and quarantine of close contacts, patients 7–10 were detected, ensuring no further onward transmission.
Many studies have shown that COVID-19 cases were highly contagious at the pre-incubation period [19–21]; however, the above results suggest that the exposure time of the next generation was earlier than 1–3 days after the onset of disease in the previous generation of patients (Table 1). This finding could indicate that COVID-19 cases had high infectivity for at least 3 days at the end of the incubation period [22,23]. The sixth edition of COVID-19 Prevention and Control Plan suggested that a person is infectious in the last 2 days of incubation of COVID-19 [24] and the current guideline, namely the seventh edition does not mention relevant information [25]. Our findings demonstrate that it might be earlier than we know.
Although patients 5 and 6 wore surgical masks when they were in contact with outpatients in the hospital, they were infected as well, indicating that only adopting primary protections such as surgical masks cannot prevent the transmission of COVID-19. Thus, wearing adequately protective equipment, such as N95 respirators, medical masks, eye protection, gowns, and gloves at the same time, should be strengthened in high-risk areas such as hospitals. Patient 8 was infected in the hospital and then transmitted the virus to family members during the incubation period, strengthening the evidence that asymptomatic cases play important roles in the transmission of COVID-19. Zou et al [26] found that the viral load of symptomatic and asymptomatic patients was similar. It has been reported that asymptomatic infected persons might represent a key node for epidemic prevention and control, and close contacts should be restricted as confirmed cases [27]. Du et al [28] suggested that 12.6% of transmission was presymptomatic. High infectivity and a high proportion of asymptomatic individuals (30%) among cases exacerbated the difficulty of preventing the dissemination of the disease, highlighting that more rigorous measures should be taken to control and prevent the transmission of COVID-19 [29].
To identify all suspected cases and control the transmission of COVID-19 in hospital A and other communities, medical officers adopted rigorous strategies and measures to block the further spread of COVID-19. The effective measures included the following. First, the Fever Clinic and Emergency Department of hospital A were shut down immediately, and terminal disinfection of the hospital was conducted. Medical service of the whole hospital was suspended, with patients with mild disease being transferred out of the hospital for home isolation and patients with severe disease remaining isolated in the hospital. Second, the nucleic acid screening was immediately conducted for all hospital staff and inpatients. People with positive results were hospitalized for isolation and treatment, while those with negative results were quarantined at home. Third, the CDC conducted comprehensive free nucleic acid screening for patients and their escort personnel who visited the hospital since January 23 and warned them to stay at home for 14 days of isolation. Meanwhile, the close contacts of the cases whose screening results were positive underwent nucleic acid screening and quarantined for 14 days. Fourth, at the expiration of the isolation period, the Xi’an CDC conducted nucleic acid screening for all the above-mentioned people again to ensure that there were no new infections. As of March 12, all close contacts associated with the outbreak had exceeded twice the longest incubation periods and the last case was discharged from the hospital. No new infections occurred, and the outbreak was considered to have subsided. Recent reports suggested that SARS-CoV-2 has mutated to increase its infectivity and a patient who had recovered was re-infected [30,31], which indicates that the effectiveness of the vaccine is questionable and strict control measures remain the effective means of preventing further development of the disease. Our study can serve as a valuable reference for controlling the transmission of COVID-19.
Conclusions
The cluster transmission of COVID-19 in the current study showed that COVID-19 can be easily transmitted within families and in hospitals, due to close contact and the lack of efficient protections. At the end of the incubation period (at least 3 days before onset), a patient can be highly contagious, and asymptomatic patients can also be a source of infection within clusters. It is recommended that people with confirmed cases should be quarantined and treated as quickly as possible, and that all their close contacts should be subjected to medical quarantined observation and nucleic acid screening to prevent the risk of further spread.
References
1. World Health Organization: WHO Director-General’s opening remarks at the media briefing on COVID-19 March 11, 2020 https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020
2. World Health Organization: WHO coronavirus (COVID-19) dashboard https://covid19.who.int/
3. Li Q, Guan X, Wu P, Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia: N Engl J Med, 2020; 382; 1199-207
4. Yang HY, Duan GCAnalysis on the epidemic factors for COVID-19: Zhonghua Yu Fang Yi Xue Za Zhi, 2020; 54(6); 608-13 [in Chinese]
5. Li R, Pei S, Chen B, Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2): Science, 2020; 368(6490); 489-93
6. Tian H, Liu Y, Li Y, An investigation of transmission control measures during the first 50 days of the COVID-19 epidemic in China: Science, 2020; 368(6491); 638-42
7. Lai S, Ruktanonchai NW, Zhou L, Effect of non-pharmaceutical interventions to contain COVID-19 in China: Nature, 2020; 585(7825); 410-13
8. Hsiang S, Allen D, Annan-Phan S, The effect of large-scale anti-contagion policies on the COVID-19 pandemic: Nature, 2020; 584(7820); 262-67
9. Ng V, Fazil A, Waddell LA, Projected effects of nonpharmaceutical public health interventions to prevent resurgence of SARS-CoV-2 transmission in Canada: CMAJ, 2020; 192(37); E1053-64
10. Chinazzi M, Davis JT, Ajelli M, The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak: Science, 2020; 368(6489); 395-400
11. World Health Organization: Virtual press conference September 7, 2020 https://www.who.int/docs/default-source/coronaviruse/transcripts/covid-19-virtual-press-conference---7-september-corrects-name.pdf
12. National Health Commission, PRC: COVID-19 Diagnosis and Treatment Protocol (Trial version 4) [EB/OL] January 27, 2020 http://www.nhc.gov.cn/xcs/zhengcwj/202001/4294563ed35b43209b31739bd0785e67.shtml
13. National Health Commission, PRC: Notice of the General Office of the National Health Commission on Issuing the New Coronavirus Pneumonia Prevention and Control Plan February 21, 2020 http://www.nhc.gov.cn/jkj/s3577/202002/a5d6f7b8c48c451c87dba14889b30147.shtml
14. National Health Commission, PRC: Notice of the General Office of the National Health Commission on Printing and Distributing the Pneumonia Prevention and Control Plan for Novel Coronavirus Infection January 28, 2020 [cited 2020 April 6[. http://www.nhc.gov.cn/xcs/zhengcwj/202001/470b128513fe46f086d79667db9f76a5.shtml
15. Pung R, Chiew CJ, Young BE, Investigation of three clusters of COVID-19 in Singapore: Implications for surveillance and response measures: Lancet, 2020; 395(10229); 1039-46
16. Lauer SA, Grantz KH, Bi Q, The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application: Ann Intern Med, 2020; 172(9); 577-82
17. Jin X, Lian JS, Hu JH, Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms: Gut, 2020; 69(6); 1002-9
18. Tian S, Hu N, Lou J, Characteristics of COVID-19 infection in Beijing: J Infect, 2020; 80(4); 401-6
19. Gao Y, Shi C, Chen Y, A cluster of the Corona Virus Disease 2019 caused by incubation period transmission in Wuxi, China: J Infect, 2020; 80(6); 666-70
20. Huang L, Zhang X, Zhang X, Rapid asymptomatic transmission of COVID-19 during the incubation period demonstrating strong infectivity in a cluster of youngsters aged 16–23 years outside Wuhan and characteristics of young patients with COVID-19: A prospective contact-tracing study: J Infect, 2020; 80(6); e1-e13
21. Li P, Fu JB, Li KF, Transmission of COVID-19 in the terminal stage of incubation period: A familial cluster: Int J Infect Dis, 2020; 96; 452-53
22. Qian G, Yang N, Ma AHY, A COVID-19 Transmission within a family cluster by presymptomatic infectors in China: Clin Infect Dis, 2020; 71(15); 861-62
23. Wei WE, Li Z, Chiew CJ, Presymptomatic transmission of SARS-CoV-2 – Singapore, January 23–March 16, 2020: MMWR Morb Mortal Wkly Rep, 2020; 69(14); 411-15
24. : National Health Commission, Notice of the General Office of the National Health Commission on Issuing the New Coronavirus Pneumonia Prevention and Control Plan March 7, 2020 http://www.nhc.gov.cn/xcs/zhengcwj/202003/4856d5b0458141fa9f376853224d41d7.shtml
25. National Health Commission, PRC: Notice on Issuing the New Coronavirus Pneumonia Prevention and Control Plan September 15, 2020 http://www.nhc.gov.cn/cms-search/xxgk/getManuscriptXxgk.htm?id=318683cbfaee4191aee29cd774b19d8d
26. Zou L, Ruan F, Huang M, SARS-CoV-2 viral load in upper respiratory specimens of infected patients: N Engl J Med, 2020; 382(12); 1177-79
27. Wölfel R, Corman VM, Guggemos W, Virological assessment of hospitalized patients with COVID-2019: Nature, 2020; 581(7809); 465-69
28. Du Z, Xu X, Wu Y, Serial interval of COVID-19 among publicly reported confirmed cases: Emerg Infect Dis, 2020; 26(6); 1341-43
29. Lu S, Lin J, Zhang Z, Alert for non-respiratory symptoms of Coronavirus Disease 2019 (COVID-19) patients in epidemic period: A case report of familial cluster with three asymptomatic COVID-19 patients: J Med Virol, 2021; 93(1); 518-21
30. Korber B, Fischer WM, Gnanakaran S, Tracking changes in SARS-CoV-2 spike: Evidence that D614G increases infectivity of the COVID-19 virus: Cell, 2020; 182(4); 812-27.e19
31. To KK, Hung IF, Ip JD, COVID-19 re-infection by a phylogenetically distinct SARS-coronavirus-2 strain confirmed by whole genome sequencing: Clin Infect Dis, 2020 [Online ahead of print]
Figures
Tables
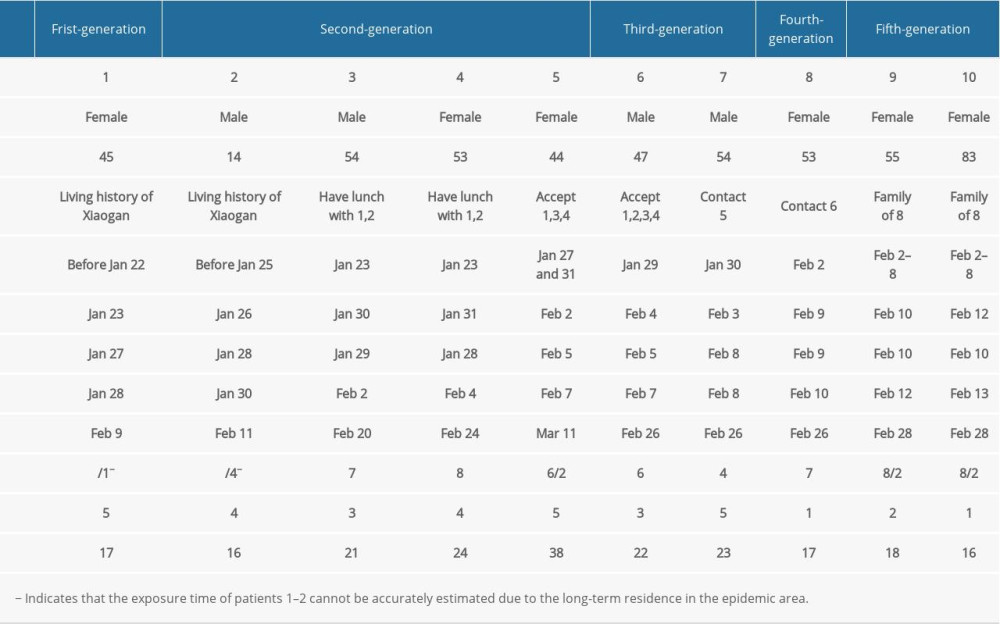 Table 1. Information of the confirmed cases of COVID-19 in the cluster.
Table 1. Information of the confirmed cases of COVID-19 in the cluster.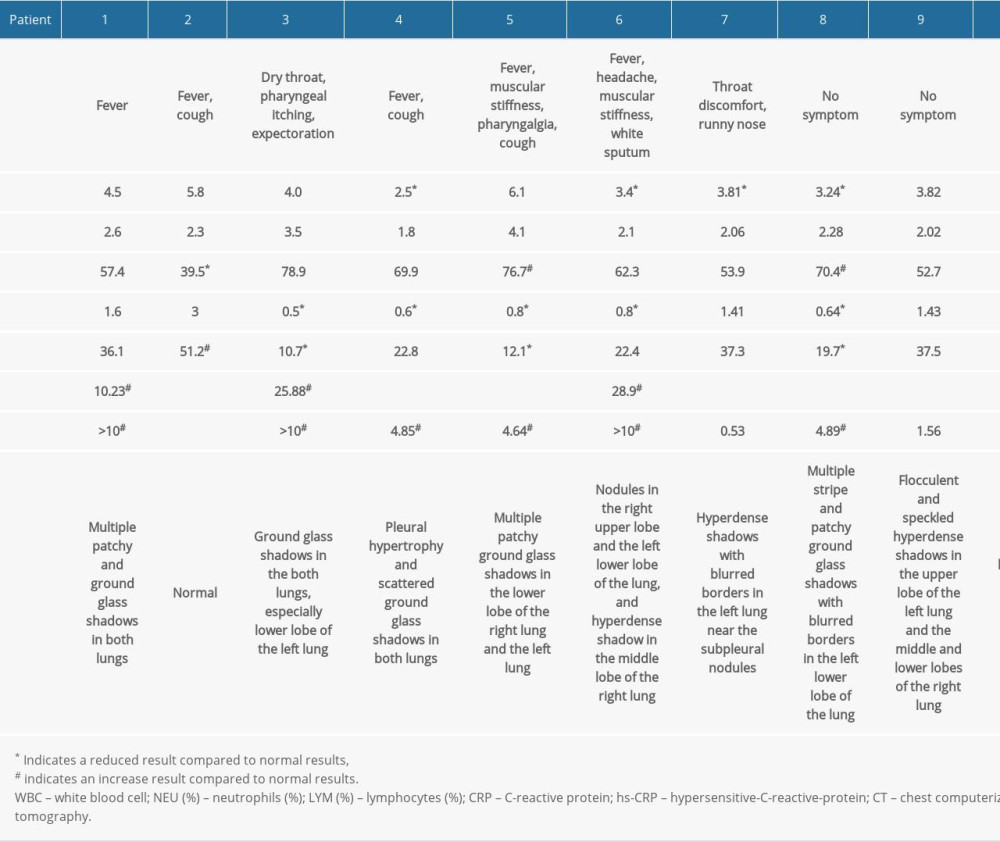 Table 2. Clinical findings and laboratory test results of COVID-19 confirmed cases upon admission.Table 1. Information of the confirmed cases of COVID-19 in the cluster.Table 2. Clinical findings and laboratory test results of COVID-19 confirmed cases upon admission.
Table 2. Clinical findings and laboratory test results of COVID-19 confirmed cases upon admission.Table 1. Information of the confirmed cases of COVID-19 in the cluster.Table 2. Clinical findings and laboratory test results of COVID-19 confirmed cases upon admission. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387