22 April 2021: Clinical Research
External Screw-Threaded Traction Device Helps Optimize Finger Joint Mobility in Severe Stage III and IV Dupuytren Disease
Raymund E. Horch1ADEFG, Marweh Schmitz1AE, Maria Kreuzer2BCDF, Andreas Arkudas1E, Ingo Ludolph1E, Wibke Müller-Seubert1DEF*DOI: 10.12659/MSM.929814
Med Sci Monit 2021; 27:e929814






Abstract
BACKGROUND: Treating advanced finger joint contractures from Dupuytren disease remains a challenge. We evaluated the effectiveness of a skeletal distraction device versus alternative treatment options.
MATERIAL AND METHODS: We analyzed the surgical treatment of contracted finger joints in stage III and stage IV Dupuytren’s disease over a 10-year period. Data were obtained from inpatient and outpatient medical records, including postoperative clinical examinations and extended Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire scores. Complications of infection, postoperative pain, and wound healing disorders were recorded.
RESULTS: A total of 79 patients (83 hands) were assigned to 2 treatment groups. Patients in group 1 underwent an initial open transection of the main fibrous cord, Z-plasty, distraction with the Erlangen external distraction device, and fasciectomy. The distraction period was 13 to 81 days (mean 31 days). Group 2 underwent a conventional single-stage fasciectomy and arthrolysis. DASH scores and subjective patient satisfaction were lower in group 1 (20.7/33%) than in group 2 (10.3/50%). However, the staged approach of group 1 to treat proximal interphalangeal joint contractures in the long term (improvement >40%) was more effective than the approach of group 2 (>33%). Distraction device pin infections occurred in 20% of hands. Postoperative pain and complex regional pain syndrome type I occurred in 25% of hands in group 1 and 3% in group 2.
CONCLUSIONS: A screw thread driven external fixation device is useful in end-stage Dupuytren’s finger joint contractures. It is indicated when joint contractures are advanced and simple arthrolysis is insufficient.
Keywords: Dupuytren Contracture, External Fixators, Joint Capsule Release, adult, Aged, Aged, 80 and over, Bone Screws, Disease Progression, Equipment and Supplies, Female, Finger Joint, Humans, Male, Middle Aged, Orthopedic Procedures, Postoperative Care, Range of Motion, Articular, Treatment Outcome
Background
Dupuytren disease (DD) is a benign fibroproliferative disorder of the palmar fascia that can result in severe joint contractures and severely impaired hand function. In DD, an excessive accumulation of collagen forms cords and nodules [1,2], while cords mainly comprised of fibroblasts and myofibroblasts have been found to build nodules [3]. It has been suggested that the extracellular matrix secreted by the nodules as an active part of the disease is remodeled and maintained as cords. Finally, the shortening of the cords by the myofibroblasts results in flexion contracture [3–6]. Palmar fasciectomy of any kind – partial, selective, or limited – is currently considered the criterion standard treatment and remains the mainstay in managing DD [7]. Conservative and minimally invasive methods such as collagenase injections and percutaneous needle transection have their specific indications, but are still under debate and are not suitable to treat advanced joint contractures [8–12]. The far-advanced stages of finger joint contractures require surgical arthrolysis, which is frequently followed by severe wound healing problems, and the affected fingers are at risk of amputation. Nevertheless, external distraction devices have been developed as a possible means to regain a certain amount of finger joint and, hence, hand function [13]. Painful cords and flexion deformities in the metacarpophalangeal (MCP) [14] and proximal interphalangeal (PIP) joints reduce hand function significantly, so that any surgical attempt to restore useful hand function can be indicated and worthwhile [15]. The data in the literature show that with an increasing stage of DD finger joint contracture, the results of surgery are less satisfying and are associated with an increase in complications and rate of recurrence [16]. Single-stage treatments in advanced DD with severe stage IV flexion deformities can result in finger amputations. Preoperative distraction aims to avoid the harsh stretching of nerves and vessels that occurs during a single-stage approach, leading to vascular thrombosis and consequent tissue necrosis. Two-staged approaches can help prevent tissue necrosis and potential amputations. It has been shown that 2-staged approaches minimize complication rates [13,17,18]. Messina et al described how previously firm prominent Dupuytren’s bands are reduced to soft fibrous ribbons during the distraction period [19]. However, the exact beneficial mechanisms of the distraction period still remain unclear. The aim of our study was to evaluate the short-term and long-term effectiveness of an Erlangen minimized screw thread external skeletal distraction device in patients with Dupuytren Iselin stage III or IV or recurrent DD.
Material and Methods
The study was approved by our institution’s ethics committee (approval no. 177_20 Bc). Due to the retrospective design of the study, informed consent from the patients was deemed unnecessary. Patients with advanced Dupuytren Iselin stage III or IV disease of 1 or both hands, who underwent surgery in a 10-year period between 2003 and 2012 in our Department of Plastic and Hand Surgery, were included in the study. Data analysis of inpatient and outpatient medical records was performed spanning the preoperative period to the end of treatment. The Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire score was used to perform a standardized evaluation of upper-extremity specific outcomes. The scores for all items in the DASH questionnaire are used to calculate a scale score ranging from 0 (no disability) to 100 (most severe disability) [20,21]. Furthermore, long-term results were studied using the findings of clinical follow-up examinations, during which the range of motion of the treated fingers was recorded. To exclude nerve lesions, finger sensitivity was tested with the 2-point discrimination test. Patients with previous amputation or arthrodesis, or those who underwent surgical treatment or any alternative therapy, such as radiation or injection therapy, elsewhere during the study period were excluded from the study.
According to patient characteristics and the various therapy regimens, patients were assigned to 1 of 2 treatment groups. The therapy regimen was chosen based on the severity of the contraction, the patient’s level of compliance, and the patient’s ability to perform the distraction independently. Patients in group 1 received an initial open transection of the main fibrous cord, Z-plasty, and the continuous skeletal distraction of the PIP joint with the Erlangen external distraction device (Figure 1), followed by a fasciectomy and open joint finger arthrolysis, as a 2-staged approach [13]. The skeletal distraction device acted as an angular and longitudinal distractor of the treated joint, as previously described [13]. Two pins were inserted into the bone proximal and distal to the contracted joint and connected to the distraction device, which transmitted the extension to the contracted joint [19]. Distraction was performed daily by the patients according to the instructions they were given, dependent on pain and perfusion of the finger. The distraction process was stopped when the joint was completely extended.
Group 2 included patients who underwent a conventional single-stage fasciectomy and arthrolysis. Data including sex, age, family history, additional afflictions like Morbus Ledderhose/Morbus Peyronie, nicotine or alcohol abuse, and systemic diseases, such as diabetes mellitus, were recorded for all patients. All intraoperative and postoperative complications, such as injury of vessels and nerves, impaired wound healing, infection, pain, complex regional pain syndrome (CRPS) type I, bleeding, revision surgery, and keloids were recorded. Owing to the retrospective design of this study and incomplete documentation, complications and the absence of a specific complication were recorded when it was reported by the patients. As a result, the total number of patients is different for each complication. Descriptive statistical data analysis was performed using SPSS version 22.0 (IBM, Armonk, NY, USA).
Results
In a 10-year period, 78 patients (83 hands) who underwent surgical treatment of Iselin stage III and IV DD were eligible for this study. The sex ratio was male to female, 8.8: 1 (70 men and 8 women), and patients were an average age of 64 years (range, 35–82 years). Five male patients underwent surgery on both hands. The DASH questionnaire was completed for 46% of the operated hands (n=38) (Figure 2). Follow-up examination was possible for 27% of the operated hands (n=22). In group 1, 20 hands received a 2-staged approach with skeletal distraction followed by a fasciectomy. In group 2, 63 hands underwent a conventional single-stage fasciectomy. Twenty-nine hands (35%) were classified as Iselin stage III and 54 hands (65%) were classified as Iselin stage IV. The subgroup analysis showed that 1 hand (5%) in group 1 was classified as Iselin stage III, compared with 28 hands (44%) in group 2. Nineteen (95%) of the treated hands in group 1 were classified as Iselin stage IV (Figures 3, 4), compared with 35 (56%) of the treated hands in group 2. Potential risk factors, including positive family history, smoking, and alcohol abuse, had a similar incidence of 20% to 30% in both groups (Table 1). The postoperative DASH score was higher in group 1 (mean, 20.7) than in group 2 (mean, 10.3). Thirty-three percent of patients who were successfully followed up in group 1 (4 of 12) were completely satisfied with their treatment, compared with 50% of patients who were followed up in group 2 (17 of 34). The average time to achieve maximum distraction and joint release with the Erlangen distraction device was 31 days (range, 13–81 days). The patient with the distraction period of 81 days presented initially with a 95° flexion contracture and massive arthrosis of the PIP joint. Postoperative follow-up was performed after an average of 39 months in group 1 and after an average of 51 months in group 2.
From the 2-staged treatment of group 1, the average postoperative extension deficit of the MCP joint was 15°, with an improvement of 30° over the preoperative extension deficit. From the single-stage treatment of group 2, the postoperative extension deficit of the MCP joint was 5°, compared with 30° before surgery, with an improvement of 83%. Patients with the 2-staged therapy in group 1 showed long-term outcomes in mobility of the PIP joint, especially with a 35° improvement in extension (Figures 5, 6). In group 2, the mean improvement of PIP joint extension was 20°.
The most frequent postoperative complication was infection, which occurred in 20% of the treated hands in each group (4 of 20 in group 1; 6 of 30 in group 2), and wound healing problems in 17% (2 of 12) treated hands in group 1 and in 26% (7 of 27) treated hands in group 2 (Figure 7). Complaints of postoperative pain after the procedures and CRPS type I were present in 3 of 12 (25%) treated hands in group 1 and in 1 of 29 (3%) treated hands in group 2. These patients received several treatment modalities such as pharmacological treatments, physical therapy, and patient education, which relieved the symptoms considerably. Hypertrophic scars appeared most frequently in group 1, in 9 of 13 hands (69%), compared with 12 of 39 hands (31%) in group 2. Reduction of sensitivity was described in 1 of 12 (8%) treated hands in group 1 and in 1 of 31 (23%) treated hands in group 2. The overall rate of relapse was less than 15% in both groups. Pin infections of the distraction device occurred in 4 of 20 hands (20%). Four patients in group 1 developed fractures of the distracted fingers. Two fractures were treated conservatively and 1 fracture of the middle phalanx required longer treatment with the distraction device. Another fracture of the middle phalanx was treated with additional Kirschner wire osteosynthesis. Arterial repair during fasciectomy was necessary in 1 hand in group 1 (5%) and in 3 hands in group 2 (5%). Surgery for recurrent disease was necessary in 2 hands each in group 1 (10%) and group 2 (3%)
Discussion
Treatment of advanced flexion deformities of the fingers or recurrent DD remains challenging. We analyzed our standard therapy methods in advanced or relapsing DD with or without the use of external fixation distraction because the literature on the optimal therapy in these advanced cases remains scarce. Among various technical devices available for use, the external fixation device proposed by Messina and Messina has been used to pretreat the contracture by stretching the contracted skin and potentially stretching the contracted joint structures [18]. This apparatus, however, is hampered by its bulkiness. Therefore, we previously developed a smaller device [13] as an alternative to pneumatic pre-expansion [22]. Nevertheless, even when such a pretreatment seems technically more feasible with a smaller device, the surgical therapy of joint contractures still remains tedious, and a considerable level of compliance from the patient is required. End-stage DD with far-advanced joint flexion contractures requires frequent arthrodesis, or can even require finger amputation, when standard surgical release is attempted. A possible insufficient perfusion of the surgically treated finger might be recorded using indocyanine angiography [23,24]. Methods of tissue engineering and regenerative medicine [25–28] have been applied to study the behavior of Dupuytren cells in culture and to modify their proliferation, but these methods are not yet available for routine clinical treatment [6]. The cord transection method was initially performed by Baron Guillaume Dupuytren in Paris in 1831, and was widely used until the 1960s. Since then, a localized fasciectomy with resection of macroscopically affected connective tissue has become the criterion standard of surgical treatment. It has been widely discussed in the literature that a simple checkrein ligament release alone does not sufficiently address the shortened arteries or deficient skin required to treat PIP flexion contractures [29]. To overcome that problem, various devices, such as the Messina continuous extension technique (TEC) device and the Digit Widget system [17], have been used to distract the soft tissue and relieve the joint contracture. Studies comparing checkrein ligament release alone with fasciectomy versus preliminary soft-tissue distraction followed by a surgical release to treat PIP contractures have shown that a staged procedure has beneficial outcomes [17]. The present retrospective analysis corroborates these findings.
When dealing with advanced joint contractures, an optimized treatment strategy with partial fasciectomy as the central step appears to be useful. With a partial fasciectomy alone, Donaldson et al reached an improvement in MCP extension of 38% [30], whereas the patients in our present study showed a postoperative improvement in joint function of up to 83%. Our results are higher than those reported in the literature, where in general the outcome of improved PIP joint function after contracture ranges between 30% and 63% [15,16,30–32]. These improvement figures are similar to our results in group 2, which yielded a 33% improvement in PIP joint mobility. Our overall complications are similar to those reported in other studies, namely a rate of vessel and nerve injuries of 2% to 3% [33] and wound healing disorders of 2% to 57% [31,34]. The development of CRPS type I has been reported in other studies as ranging from 2% to 4%. [30,31]. A reason for our higher 25% rate of pain or CRPS I in group 1 might be that a clear distinction between pain and CRPS 1 was not possible because of the retrospective character of this study. Citron et al described CRPS type I of up to 38% [35]. Subjective patient satisfaction data, as validated with the DASH score, corroborates the findings of other researchers, who reported scores between 7 and 30 points [36,37].
When Messina treated finger joint contractures solely with his above-mentioned TEC device, he noted that more than 50% of his patients showed a relapse as early as 10 days after the removal of the distraction device. Therefore, he developed a 2-step approach with partial fasciectomy following the distraction to treat advanced Dupuytren contractures [18]. Although Messina reported a complete joint extension in his patients within 14 days, our patients needed an average of 31 days to achieve satisfactory results. After the addition of a partial fasciectomy in the second step, 90% of Messina’s patients were reported to have good to excellent results. Unfortunately, he did not further specify the range of motion the patients regained or the length of the follow-up period. In another study, Citron and Messina reported an improvement in PIP extension of 63% in 13 patients after a mean follow-up of 18 months [35]. Other studies reported on a distraction device treatment for 28 days that ended with a partial fasciectomy. They achieved an improvement of 50% in PIP extension within 6 to 48 months [38]. The authors’ experiences with patient compliance were similar to ours.
The 2-stage method is not free of unexpected complications. In 4 patients in group 1, we noted fractures of the distracted fingers, necessitating prolonged fixation therapy, Kirschner wire osteosynthesis, or immobilization until the bone was healed. One patient with a fracture fell on the distraction device, and the origin of the fractures of the other 3 patients is unknown. One reason for fracture might be the tension on the contracted joint. Another issue we found in our study was the development of unexpected pain during the distraction period. This naturally influenced the compliance of patients to complete the distraction treatment. Interestingly, other researchers either did not report or did not observe any pain in their patients [18,35]. We suggest that a fast distraction and neglecting the occurrence of unusual pain may be possible reasons for this inconsistency. Given the number of unwanted adverse effects, it is understandable that the subjective rating score of patients with an external fixation distraction was found to be worse than that of patients without distraction.
There were some potential study limitations. Owing to the retrospective study design, the DASH score was recorded only after surgery, so comparison with the score before surgery was not possible. The Tubiana classification of DD was not possible in all patients because of incomplete documentation. Even though both groups included severe joint contractures classified as Iselin stage III or IV, 95% of the treated hands in group 1 were classified as Iselin stage IV, compared with 56% in group 2. This difference might explain why group 1 had worse DASH scores than did group 2. The number of patients in group 1 was much smaller than in group 2. One reason might be that a distraction period requires a patient who is compliant with the instructions and is able to do the distraction independently. Furthermore, a staged approach including previous distraction is indicated in extremely severe joint contractures and most patients presented more moderate stages of DD.
The Erlangen external screw thread distractor is demanding and requires frequent outpatient visits, even though it was shown to be effective in our study. Therefore, it should be indicated only in patients with a high level of compliance, but may be kept in mind as another tool to treat isolated joint contractures.
Conclusions
Sufficient treatment and the achievement of long-term positive outcomes of advanced end-stage Dupuytren’s finger joint contractures remain challenging. The careful assessment of hand and joint function and choice of the appropriate surgical approach with staged procedures seem to be important to effectively treat advanced Dupuytren’s finger contractures. External skeletal traction devices are helpful in treating severe, long-lasting PIP joint flexion contractures. Our results emphasize the effectiveness of a 2-staged approach to obtain results that are superior to those of a single-stage surgery in advanced Dupuytren’s finger joint contractures.
Figures
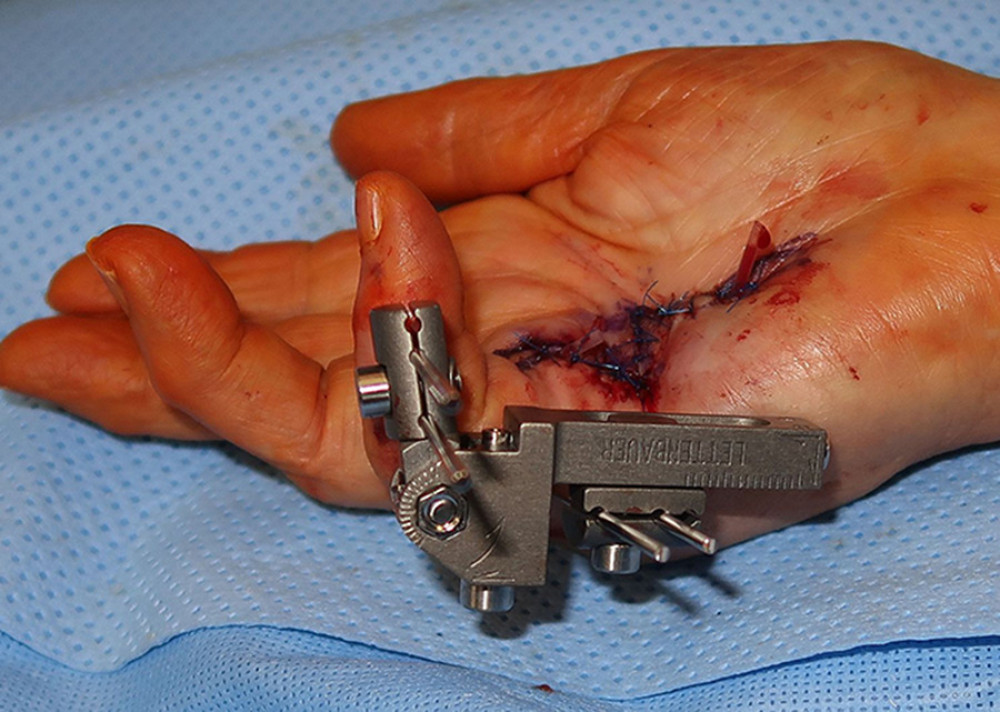 Figure 1. The Erlangen skeletal distraction device.
Figure 1. The Erlangen skeletal distraction device. 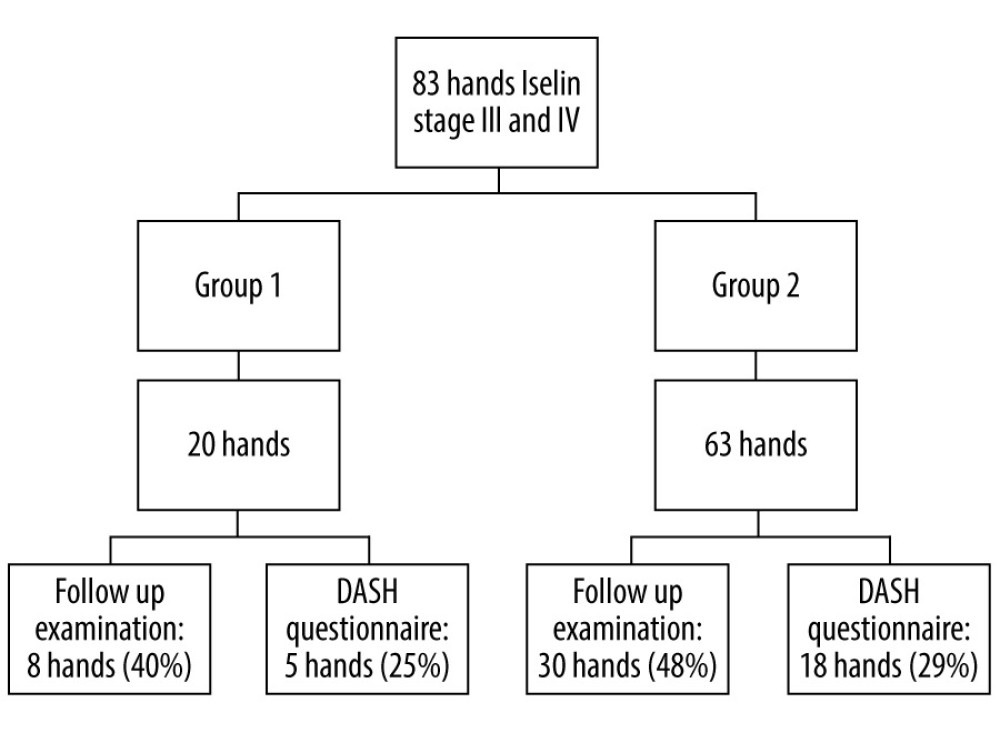 Figure 2. Flow chart of study participation.
Figure 2. Flow chart of study participation.  Figure 3. Patient with recurrent stage IV Dupuytren‘s contracture.
Figure 3. Patient with recurrent stage IV Dupuytren‘s contracture.  Figure 4. X-ray of the contracted proximal interphalangeal joint.
Figure 4. X-ray of the contracted proximal interphalangeal joint. 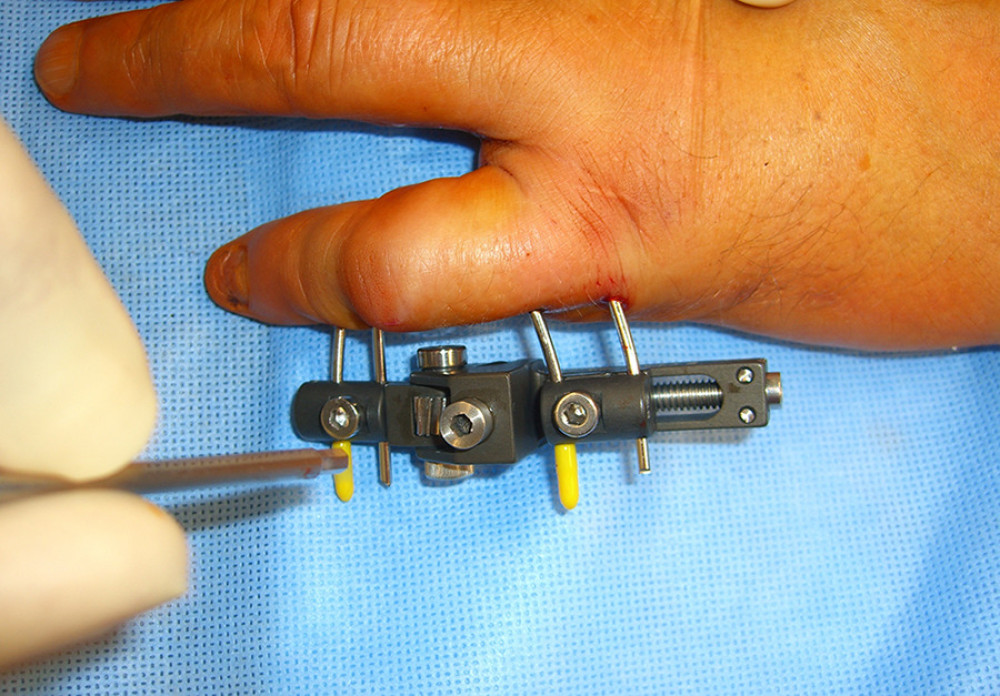 Figure 5. Intraoperative image of the applied distraction device.
Figure 5. Intraoperative image of the applied distraction device. 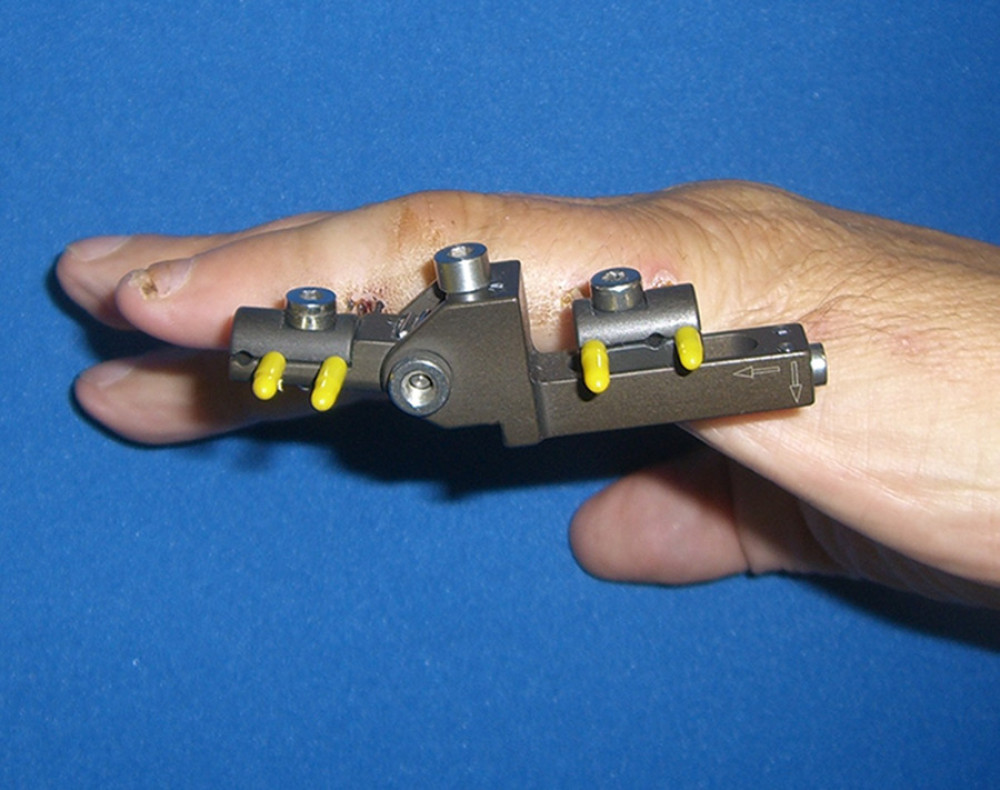 Figure 6. Fully extended proximal interphalangeal joint after a distraction period of 19 days.
Figure 6. Fully extended proximal interphalangeal joint after a distraction period of 19 days. 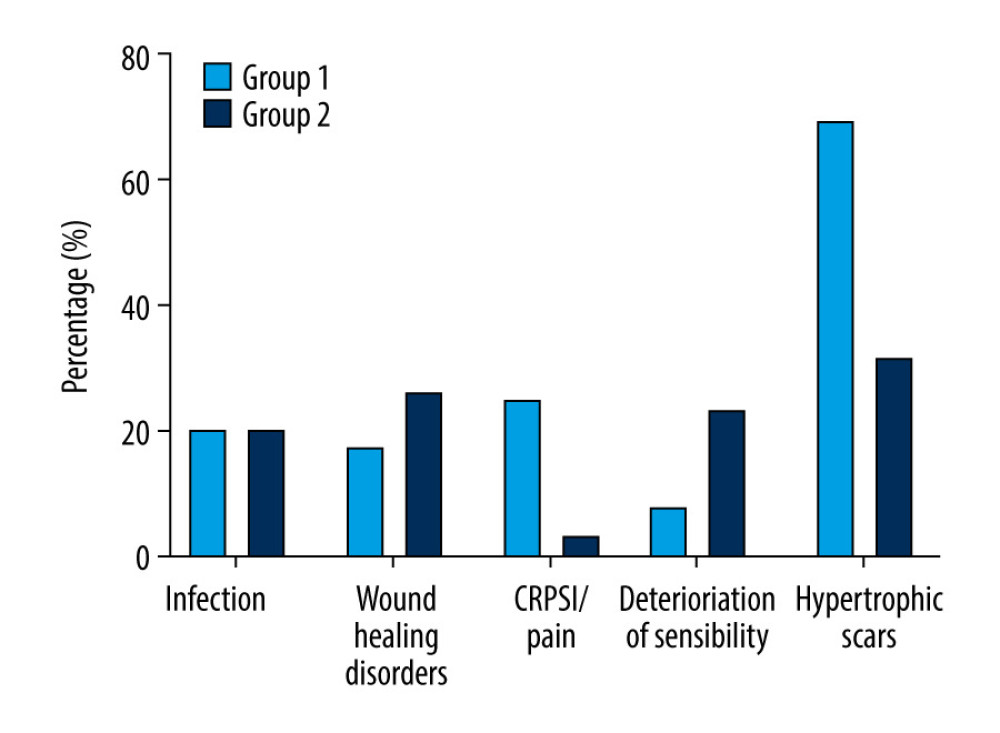 Figure 7. Complications after treatment.
Figure 7. Complications after treatment. 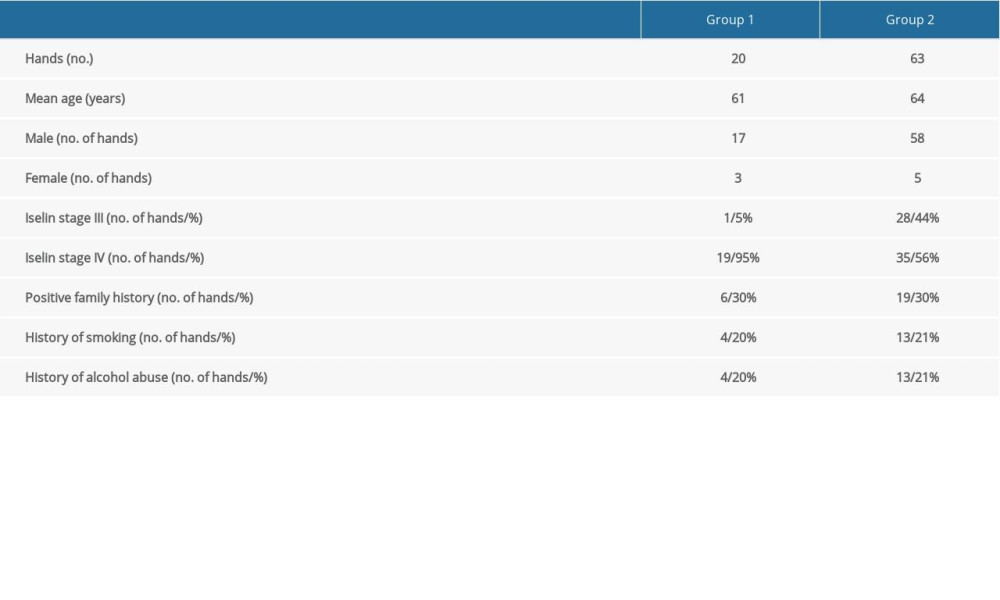
References
1. Kopp J, Seyhan H, Müller B, N-acetyl-L-cysteine abrogates fibrogenic properties of fibroblasts isolated from Dupuytren’s disease by blunting TGF-beta signalling: J Cell Mol Med, 2006; 101; 157-65
2. Bazin S, Le Lous M, Duance VC, Biochemistry and histology of the connective tissue of Dupuytren’s disease lesions: Eur J Clin Invest, 1980; 101; 9-16
3. Layton T, Nanchahal J, Recent advances in the understanding of Dupuytren’s disease: F1000Res, 2019; 8; F1000
4. Verjee LS, Midwood K, Davidson D, Myofibroblast distribution in Dupuytren’s cords: Correlation with digital contracture: J Hand Surg, 2009; 3410; 1785-94
5. van Beuge MM, Ten Dam EJ, Werker PM, Bank RA, Matrix and cell phenotype differences in Dupuytren’s disease: Fibrogenesis Tissue Repair, 2016; 9; 9
6. Seyhan H, Kopp J, Schultze-Mosgau S, Horch RE, Increased metabolic activity of fibroblasts derived from cords compared with nodule fibroblasts sampling from patients with Dupuytren’s contracture: Plast Reconstr Surg, 2006; 1174; 1248-52
7. Crean SM, Gerber RA, Le Graverand MP, The efficacy and safety of fasciectomy and fasciotomy for Dupuytren’s contracture in European patients: A structured review of published studies: J Hand Surg European Volume, 2011; 365; 396-407
8. Peimer CA, Blazar P, Coleman S: J Hand Surg, 2015; 40; 1597-605
9. Zhao JZ, Hadley S, Floyd E, The Impact of collagenase clostridium histolyticum introduction on Dupuytren treatment patterns in the United States: J Hand Surg, 2016; 41; 963-68
10. Leafblad ND, Wagner E, Wanderman NR, Outcomes and direct costs of needle aponeurotomy, collagenase injection, and fasciectomy in the treatment of Dupuytren contracture: J Hand Surg, 2019; 44; 919-27
11. De Vitis R, Passiatore M, Perna A, Seven-year clinical outcomes after collagenase injection in patients with Dupuytren’s disease: A prospective study: J Orthop, 2020; 21; 218-22
12. Ferrari M, Lellouche H, Roulot E, Iterative percutaneous needle aponeurotomy for Dupuytren’s disease: Functional outcome at 5-year follow-up: Joint Bone Spine, 2019; 87; 273-74
13. Loos B, Horch RE, Skeletal traction treatment of severe finger contracture: A new innovative skeletal distraction device: Plast Reconstr Surg, 2008; 122; 99e-100e
14. Spies CK, Langer MF, Low SMetacarpophalangeal joint replacement: Der Orthopade, 2019; 48; 386-93 [in German]
15. Karabeg R, Jakirlic M, Arslanagic S, Results of surgery treatment of Dupuytren’s contracture in 115 patients: Med Arch (Sarajevo, Bosnia and Herzegovina), 2012; 66; 329-31
16. Misra A, Jain A, Ghazanfar R, Predicting the outcome of surgery for the proximal interphalangeal joint in Dupuytren’s disease: J Hand Surg, 2007; 32; 240-45
17. Craft RO, Smith AA, Coakley B, Preliminary soft-tissue distraction versus checkrein ligament release after fasciectomy in the treatment of dupuytren proximal interphalangeal joint contractures: Plast Reconstr Surg, 2011; 128; 1107-13
18. Messina A, Messina J, The continuous elongation treatment by the TEC device for severe Dupuytren’s contracture of the fingers: Plast Reconstr Surg, 1993; 92; 84-90
19. Messina A, Messina J, The TEC treatment (continuous extension technique) for severe Dupuytren’s contracture of the fingers: Ann Chir Main Memb Super, 1991; 10; 247-50
20. Gummesson C, Atroshi I, Ekdahl C, The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: Longitudinal construct validity and measuring self-rated health change after surgery: BMC Musculoskelet Disord, 2003; 4; 11
21. Germann G, Wind G, Harth AThe DASH (Disability of Arm-Shoulder-Hand) Questionnaire – a new instrument for evaluating upper extremity treatment outcome: Handchir Mikrochir Plast Chir, 1999; 31; 149-52 [in German]
22. Piza-Katzer H, Herczeg E, Aspek RPreoperative intermittent pneumatic extension treatment stage III and IV Dupuytren contracture: Handchir Mikrochir Plast Chir, 2000; 32; 33-37 [in German]
23. Ludolph I, Cai A, Arkudas A, Indocyanine green angiography and the old question of vascular autonomy – long term changes of microcirculation in microsurgically transplanted free flaps: Clin Hemorheol Microcirc, 2019; 72; 421-30
24. Ludolph I, Horch RE, Arkudas A, Schmitz M, Enhancing safety in reconstructive microsurgery using intraoperative indocyanine green angiography: Front Surg, 2019; 6; 39
25. Horch RE, Beier JP, Kneser U, Arkudas A, Successful human long-term application of in situ bone tissue engineering: J Cell Mol Med, 2014; 18; 1478-85
26. Buehrer G, Balzer A, Arnold I, Combination of BMP2 and MSCs significantly increases bone formation in the rat arterio-venous loop model: Tissue Eng Part A, 2015; 21; 96-105
27. Leibig N, Wietbrock JO, Bigdeli AK, Flow-induced axial vascularization: the arteriovenous loop in angiogenesis and tissue engineering: Plast Reconstr Surg, 2016; 138; 825-35
28. Horch RE, Weigand A, Wajant HBiofabrication: New approaches for tissue regeneration: Handchir Mikrochir Plast Chir, 2018; 50; 93-100 [in German]
29. Hohendorff B, Spies CK, Unglaub FAnatomy of the metacarpophalangeal and proximal interphalangeal finger joint with respect to arthroplasty: Der Orthopade, 2019; 48; 368-77 [in German]
30. Donaldson OW, Pearson D, Reynolds R, Bhatia RK, The association between intraoperative correction of Dupuytren’s disease and residual postoperative contracture: J Hand Surg European Volume, 2010; 35; 220-23
31. Weinzweig N, Culver JE, Fleegler EJ, Severe contractures of the proximal interphalangeal joint in Dupuytren’s disease: Combined fasciectomy with capsuloligamentous release versus fasciectomy alone: Plast Reconstr Surg, 1996; 97; 560-66
32. Abe Y, Rokkaku T, Ofuchi S, Surgery for Dupuytren’s disease in Japanese patients and a new preoperative classification: J Hand Surg (Edinburgh, Scotland), 2004; 29; 235-39
33. Bulstrode NW, Jemec B, Smith PJ, The complications of Dupuytren’s contracture surgery: J Hand Surg Am, 2005; 30; 1021-25
34. Chen NC, Srinivasan RC, Shauver MJ, Chung KC, A systematic review of outcomes of fasciotomy, aponeurotomy, and collagenase treatments for Dupuytren’s contracture: Hand (New York, NY), 2011; 6; 250-55
35. Citron N, Messina JC, The use of skeletal traction in the treatment of severe primary Dupuytren’s disease: J Bone Joint Surg Br, 1998; 80; 126-29
36. Ball C, Pratt AL, Nanchahal J, Optimal functional outcome measures for assessing treatment for Dupuytren’s disease: A systematic review and recommendations for future practice: BMC Musculoskelet Disord, 2013; 14; 131
37. Skoff HD, The surgical treatment of Dupuytren’s contracture: A synthesis of techniques: Plast Reconstr Surg, 2004; 113; 540-44
38. White JW, Kang SN, Nancoo T, Management of severe Dupuytren’s contracture of the proximal interphalangeal joint with use of a central slip facilitation device: J Hand Surg European Volume, 2012; 37; 728-32
Figures
Figure 1. The Erlangen skeletal distraction device.Figure 2. Flow chart of study participation.Figure 3. Patient with recurrent stage IV Dupuytren‘s contracture.Figure 4. X-ray of the contracted proximal interphalangeal joint.Figure 5. Intraoperative image of the applied distraction device.Figure 6. Fully extended proximal interphalangeal joint after a distraction period of 19 days.Figure 7. Complications after treatment. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387