23 March 2021: Review Articles
A Systematic Review of Total Thoracic Endovascular Aortic Repair in Treatment of Kommerell Diverticulum Combined with Right-Sided Aortic Arch
Weijian Fan12BCEF, Jinyun Tan3BCD, Weihao Shi3CDE, Jianjie Rong1ABC*, Bo Yu23ABGDOI: 10.12659/MSM.930031
Med Sci Monit 2021; 27:e930031






Abstract
ABSTRACT: Kommerell diverticulum (KD) combined with right-sided aortic arch (RAA) and aberrant left subclavian artery (ALSA) are rare and limited to a few case reports and small series. Thoracic endovascular aortic repair (TEVAR), which is mini-invasive, is widely utilized in complicated aortic disease. We performed a systematic review of the literature to identify all patients who underwent endovascular repair for KD in terms of technical feasibility and procedural outcomes. Published and accepted studies only in English as well as article reference lists were searched and extracted to assess case series reporting solely TEVAR in KD patients. There were 28 patients with KD/RAA identified from 19 studies. All of them underwent endovascular technique for KD exclusion and the median age was 69 years (range 39–83 years). Hypertension (n=17) was the most common comorbidity in this cohort, followed by diabetes mellitus (n=3), hyperlipidemia (n=3), and smoking (n=3). The presenting symptoms were dysphagia (n=8, 29%), intermittent back pain (n=4, 14%), and acute aortic dissection (n=6, 21%), while asymptomatic was found in 9 patients (n=9, 32%). A technical success rate of 100% was reported associated with various managements of ALSA, proximal embolization (n=19, 68%), in-situ revascularization (n=3, 11%), and left carotid-subclavian bypass (n=3, 11%). All patients survived without severe complications and were discharged home within less than 14 days. The mean follow-up time was 9.3 months, patency was found in all patients, thrombosis and distinct shrinkage of KD aneurysm as indicated by CT-scans were noted (n=20, 71%), and type II endoleak was found in only 4 patients (n=4, 14%). TEVAR appears to be safe and offers favorable results, but it still needs substantial evidence to support routine use in KD. TEVAR is an alternative to open repair in selected cases, but it needs further investigation in a large cohort.
Keywords: Aorta, Thoracic, Aortic Aneurysm, Thoracic, Aortic Arch Syndromes, Embolization, Therapeutic, Endoleak, endovascular procedures, Aged, 80 and over, Aneurysm, Dissecting, Aortic Diseases, Blood Vessel Prosthesis, Blood Vessel Prosthesis Implantation, Diverticulum, Stents
Background
Right-sided aortic arch (RAA) is rare and is found in only 0.2–2.5% of autopsy studies; it is genetically associated with 22q11 deletion [1–3]. An extremely rare type of RAA is an aberrant left subclavian artery (ALSA) originating from Kommerell diverticulum (KD), which is a persistent remnant of the fourth primitive dorsal arch, due to the aneurysmal degeneration of the origin of the aberrant subclavian artery (ASA) [4]. Specifically, in patients with KD and RAA, the left dorsal arch diminishes between the subclavian and carotid arteries so that the right subclavian artery eventually originates from the remnant right dorsal arch.
KD was first described by Dr. Friedrich Kommerell in 1936 when he performed a barium swallow examination in a patient with stomach cancer presenting dysphagia lusoria [4]. Specifically, patients with KD are usually asymptomatic, and are discovered incidentally by non-enhanced chest CT scan. When there are symptoms, the most frequent is dysphagia due to compression of the esophagus, followed by asthma and hoarseness due to tracheal compression. Other patients have a long history of intermittent pain in the chest or epigastrium, or sometimes radiating to the back [5].
Given the rarity as well as heterogeneity of RAA combined with KD, there has been no consensus on the treatment. However, Austin et al reported a 19% rate of rupture [6]. Moreover, since the presence of KD mainly predisposes to development of aneurysm and dissection, the highest rate of either rupture or dissection was reported at 53% in a long-term follow-up study [7].
Hence, due to the high rate of rupture and poor prognosis after rupture or dissection, most cardiothoracic surgeons use a surgical approach for both symptomatic and asymptomatic KD patients instead of conservative management [8]. Nonetheless, the treatment of KD varies greatly, and open repair, hybrid repair, and thoracic endovascular aortic repair (TEVAR) were all reported in recent studies [9].
However, open surgery remains a challenging procedure, with extensive incision, considerably higher need for technical dexterity, and relatively higher mortality rate (8% to 26%) [10]. Therefore, with the dramatic advent of minimally invasive procedures, TEVAR has become an attractive option for selected patients, with minimal incision and favorable results. The optimal treatment strategies of endovascular repair applied for KD patients in the present era have not been established, mainly differing in whether the ALSA is reconstructed and the application scenarios (or indications) for it [11]. In-situ fenestration by needle and radio frequency, chimney stenting, and total occlusion of ALSA via coils or plug have emerged but still remain controversial [12,13].
The aim of this study was to evaluate the early and long-term outcomes of different TEVAR strategies in treatment for KD combined with RAA through reviewing the literature, so as to provide better evidence of the efficacy of endovascular repair in treatment and enrollment of KD patients.
Material and Methods
The aim of this review was to assess all relevant studies on KD treatment by TEVAR technique. Papers published between 1990 and May 2020 were included. Searches were performed in PubMed, EMBASE, and Web of Science using the terms “Kommerell diverticulum”, “Kommerell diverticulum”, “Kommerell diverticula”, “Kommerell diverticula”, “Right-Sided Arch” in combination with “TEVAR”, “endovascular” and “endovascular repair”. Additional papers were cross-checked from reference lists of included papers.
Studies that solely reported open surgery on thoracic aorta were excluded. Studies reporting hybrid repair or two-staged operation involving ascending aortic replacement were also excluded. Studies were excluded when reporting conservative therapy or best medical treatment (BMT) without endovascular repair. Studies in which data for endovascular repair were not distinguished from data for patients undergoing total arch replacement or hybrid repair without endovascular part were excluded. Data published repeatedly by the same group were excluded; however, papers from the same authors were not excluded when demonstrating further information on different cases, measurements, and consequences. Given the rarity of KD, one-case reports and review articles were all enrolled. Data were assessed for quality independently by 2 researchers. Data were specifically collected on endovascular technique, intraoperative details, postoperative outcomes, and prognosis. Our search strategy conformed to the guidelines in the Preferred Reporting Items for Systematic Reviews (PRISMA) statement standards [14].
Results
IDENTIFIED STUDIES AND POPULATION CHARACTERISTICS:
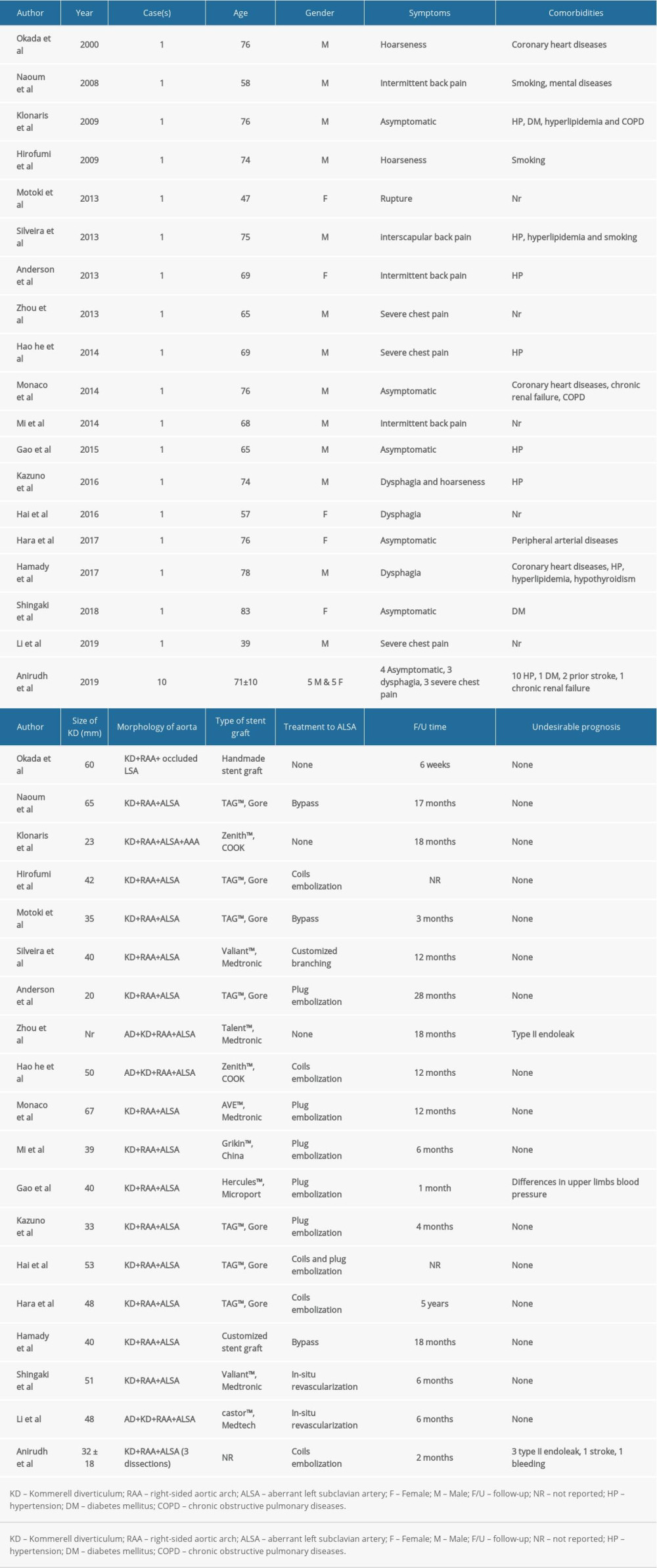
According to PRISMA protocol, 19 articles were identified from 415 articles that involved “Kommerell diverticulum” or “Kommerell diverticulum”. Studies were excluded if they did not contain any information on endovascular therapies. Also, studies were excluded when only comparing endovascular techniques or reporting hybrid repair. In terms of endovascular therapy, articles in which the classification was not KD with coexistent RAA and ALSA were excluded. Among them, mostly were case reports reporting 1 or 2 patients and 1 case cohort containing 10 patients. We analyzed data from 28 patients who were diagnosed with RAA combined with ALSA that originated from KD, and we also assessed data on demographics, details of each patient’s clinical presentation, comorbidities, pathologies, management, and follow-up [12,13,15–30].
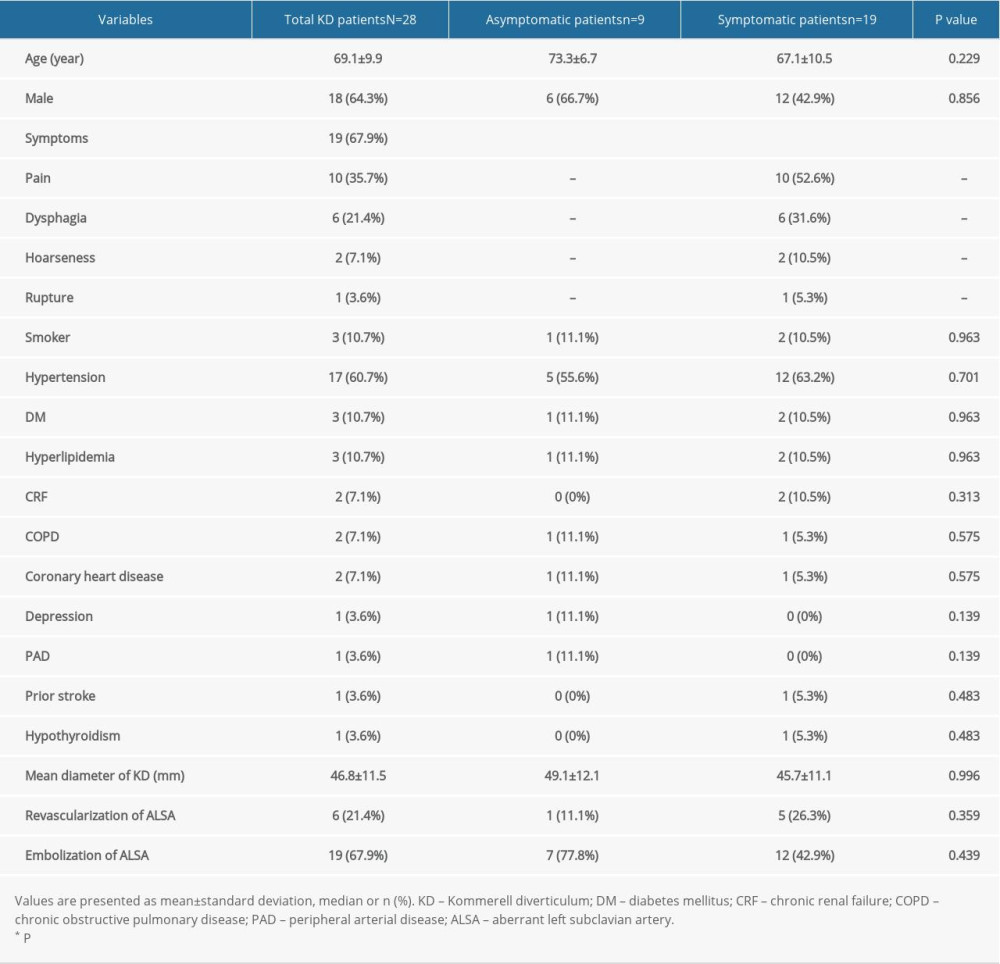
In this review, 10 patients were female and 18 were male. The median age at presentation was 69 years (range 39–83 years). We analyzed data on comorbidities. We found that the illness frequently coexists with other chronic diseases. According to our research, the majority of patients showed more than 1 comorbidity, with hypertension being most common (n=17). Other comorbidities included diabetes mellitus (n=3), hyperlipidemia (n=3), and smoking (n=3), which are known risk factors for arterial diseases. Chronic renal failure, chronic obstructive pulmonary diseases, and coronary heart diseases were found in 2 patients each. Depression, peripheral arterial diseases, prior stroke, and hypothyroidism were each present in 1 patient.
In terms of symptoms, 9 patients (32%) were asymptomatic and most of the other patients were mildly symptomatic. Specifically, the combination of dysphagia, hoarseness, and cough was a common ‘typical’ symptom due to aneurysmal compression of adjacent structures (29%). Severe chest pain was found in 6 patients who underwent acute aortic dissection (AD) as a destructive consequence of KD (21%). Furthermore, 4 patients had intermittent back pain and mild chest pain and 1 patient had a rupture, which is the most severe emergency complication of KD. Patients were classified into 2 groups depending on their symptoms. Preoperative baseline characteristics are shown in Table 1.
PATHOLOGICAL DETAILS:
The mean diameter of KD was 46.8±11.5 mm. The mean diameter of that in asymptomatic patients was 49.1±12.1 mm, while it was 41.2±10.1 mm in 6 patients who had acute AD or rupture. One patient was not measured due to extensive intramural hemorrhage and hematoma. Acute AD was recorded in 6 patients, all categorized as Stanford type B. Chronic AD and abdominal aortic aneurysm were each found in 1 patient.
ENDOVASCULAR STRATEGIES:
Endovascular repair, which is a minimally invasive and effective treatment, was utilized in all 28 patients and selected for reconstructing KD and RAA. Percutaneous puncture of the common femoral artery (CFA) was normally performed before TEVAR, while CFA exposure was only performed for patients with severe atherosclerosis and calcification. Moreover, various management methods for ALSA were noted. First, TEVAR only without further intervention to ALSA were reported in 3 articles. Moreover, further occlusion of proximal ALSA via left brachial artery was noted in 19 patients and coils were utilized in 14 patients, while plugs were used for 5 patients. Left carotid-subclavian bypass by woven Dacron graft was found in 3 patients and in-situ revascularization through thoracic branched or customized stent grafts were noted in 2 patients. Finally, a new in-situ fenestration technique by radiofrequency and subsequent stenting were reported in 1 article. In terms of device selection, Gore TAG™ and Medtronic Valiant™ were widely utilized for endovascular repair. Grikin and Medtech from China and COOK from the USA were also noted to be used in some individual cases.
PERIOPERATIVE FINDINGS:
General anesthesia was normally performed in most articles while local anesthesia was also noted in some case with full hemodynamic monitoring. Type I endoleak mostly occurred after exclusion and was found in 5 patients. Hoarseness was noticed in 1 patient after left carotid- subclavian bypass probably due to left vocal cord paralysis and recovered after thyroplasty. Mild differences in upper-limb blood pressure were instantly noticed in most of patients after ALSA occlusion. There was no intraoperative stroke or hemorrhage, and intensive care was reported in KD patients with acute dissection. All patients were discharged within 14 days.
MEAN FOLLOW-UP TIME AND PROGNOSIS:
The mean follow-up time was 9.3 months, ranging from 6 weeks to 5 years, and 2 patients were lost to follow-up. In this review, we found that patency was reported in all patients verified by CT-scans at last follow-up. However, type II endoleak was found in 4 patients, while none of them underwent further embolization. Thrombosis and distinct shrinkage of KD aneurysm shown by CT-scans were noted in 20 patients. The symptoms of dysphagia and hoarseness disappeared in 7 patients and were alleviated in 1. There were no migration and fracture of stent grafts in follow-up, and posterior cerebral ischemia was only found in 1 patient. No arm claudication, upper-limb dysfunction and mortality were reported. The specific details for each article are presented in Table 2.
Discussion
Right-sided aortic arch, normally known as RAA, with an incidence of 0.1%, is reported in case reports and reviews with a small cohort. Kommerell diverticulum originating from aneurysmal degeneration of ASA has a prevalence of 0.04% to 0.4% based on autopsy studies, with a relatively high tendency toward rupture and dissection [4,30]. According to previous studies, KD can be categorized into 5 distinct types. The ALSA originating from RAA, left-sided aortic arch (LAA) or aorto-ductal junction were defined as 3 types. The origin of ALSA arising at the junction of RAA and the descending aorta with mirror image branching was determined as another type, while the extremely rare one involved a diverticulum at the origin of an aberrant right vertebral artery arising distal to the left subclavian artery [31].
KD has been treated by open repair for decades. Total arch replacement of RAA and aberrant left subclavian aneurysm with various exposure ways under deep hypothermic circulatory arrest (DHCA) has been widely accepted [32]. The threshold of surgical option for KD is controversial. Similar to abdominal aortic aneurysm (AAA), the maximum diameter of aneurysm determines the time for operation. Some experts advised intervening when the diameter is greater than 3 cm, while others recommended 5 cm as the point for intervention [33]. Recent research has focused on the ratio of KD diameter and its concomitant ALSA, showing that the KD did not need resection until it was 1.5 times the size of the ALSA [34]. However, KD is an embryological remnant due to failed regression and the tissue is vulnerable. Given that long-term hypertension as well as wall shear stress, KD with its abnormal morphology and angulation ruptures easily and eventually becomes AD [35]. Clearly, for symptomatic patients, troublesome symptoms caused by the compression of mediastinal structures are an indication to intervene. However, owing to a high rate of rupture and dissection, surgical repair was recommended in all KD by some groups [7].
Moreover, surgical indication is feasible when patients experience symptoms from gradual organ compression [36]. Specifically, patients might have a long history of difficulty swallowing and regurgitation due to moderate compression of the esophagus. Chest pain, chest pressure, and retrosternal burning pain in the middle of the night were also illustrated in case reports [37]. Although most patients with KD are asymptomatic, symptoms present in different ways, even in symptomatic patients, due to the correlation of ALSA and adjacent structures. Provided that the ALSA is located behind the esophagus, approximately 80% of patients present with dysphagia to solid food. In the other 2 situations, between the esophagus and trachea (15%) or anterior to the trachea (5%), the symptoms may present as dysphagia, dyspnea, or stridor [38].
Open repair (OR) has been widely used and advocated in the treatment of KD in order to not only prevent sudden rupture or dissection, but also to ameliorate the symptoms arising from moderate compression [39]. OR ordinarily involves diverticulum resection/subclavian arterial reconstruction as well as total arch replacement, using DHCA [40]. However, there still remain some limitations of OR in KD treatments. In treatment of KD using OR, thoracotomy, sternotomy, ligation, aorta cross-clamping, and DHCA are required. The whole procedure remains challenging and it requires high technical dexterity and comprehensive perioperative experience. Therefore, OR carries substantial surgical risks and complications, such as left vocal cord paralysis and right vocal cord edema, as reported by Rosu [41]. Nonetheless, the mortality was 11–25% in different reviews, while the main factors associated with death were massive pulmonary embolism, mediastinitis, hematemesis, and fistula between KD and the esophagus, respectively [4]. Subsequently, increasing experience with TEVAR has paved the way for less invasive hybrid approaches. However, even hybrid repair (HR) still needs thoracotomy or sternotomy and replacement of the ascending aorta, which may still lead to multiple complications due to vast exposure and strict operative conditions during the long surgery [42].
Furthermore, Erben et al reported that 92% of patients with KD were found incidentally and Yu et al indicated that in asymptomatic patients with KD, the morbidity and mortality associated with conventional open intervention outweighed the potential benefit of rupture prevention [5,43]. The mortality and morbidity rates of open repair in KD were not acceptable even though KD with RAA is rare, and treatment is risky and controversial. Compared with postoperative complications like bleeding, nerve injuries, and respiratory failures in OR or HR, the TEVAR technique had illustrated favorable outcomes in aorta reinstitution.
Okada et al first reported endovascular repair in a RAA patient combined with aneurysm. The procedure showed successful isolation of KD and occlusion of ALSA without instant complications and undesirable prognosis [25]. However, TEVAR is not suitable for all KD patients and accurate preoperative clinical and anatomical evaluation is extremely critical for enrollment [15]. The optimal timing for performing TEVAR on KD involves 3 main aspects: (1) the suitability of access vessels for insertion; (2) feasible tortuosity and angulation of the aorta arch; and (3) the availability of a proximal landing zone (PLZ) [44]. The limited landing area for a graft will always lead to type I endoleak as a consequence, along with the possibility of esophagus compression by stents [37]. Therefore, a sufficient PLZ is essential for the success of TEVAR in KD treatment. PLZ was proposed and classified to 3 types according to the modified Hishimaru aortic arch classification. Tinelli et al suggested that a standard thoracic stent graft was feasible for implantation when the PLZ comprised at least 2 cm of healthy aorta [44].
According to the results reported above, we found that there were no differences in the mean diameter of KD in asymptomatic and symptomatic patients and no significant difference in mild symptomatic and acute dissection or rupture. Current treatment guidelines for KD are based on a small case series of patients with no clear consensus on the surgical indications. One of the most consistent indications emphasize size, claiming that the KD aneurysm and aortic diameter need to be larger than 3 cm and 5 cm, respectively [33]. However, we found that the size of the KD was not the threshold for intervention because it would lead to disastrous consequences regardless of diameter.
There has been considerable controversy in the literature regarding the feasibility for TEVAR in KD patients. Ota et al argued that there is no volume reduction of the diverticulum after complete exclusion by stent graft, and compression symptoms cannot be attenuated [39]. However, thrombosis and shrinkage of a saccular aneurysm were widely found in this review, so that the compression by KD and corresponding symptoms would be largely alleviated [23]. Also, El Batti et al found that there was ample room between the KD and the esophagus during hybrid repair, which means that the most important aim for KD treatment was preventing rupture, although we assume that a very large KD compression may be a problem [45]. Moreover, Ota et al claimed that a “sharp angle” between the distal arch and descending aorta was an anatomical challenge for transition [39]. It may be taken into consideration in early stage of TEVAR, yet we believe that it is no longer a contraindication due to materials innovation. The introducer sheath of the new stent graft produced by Cordis (USA) is 14-F, with more flexibility compared to the normal 18-F and 24-F sheaths.
Furthermore, no matter which devices are used to treat ALSA, there remain 2 basic techniques: proximal exclusion with/without blood flow reconstruction. Percutaneous coil embolization of the proximal segment of the ALSA was performed by coils or plugs after deployment of the device in some cases [16,21]. However, some researchers were concerned that intentional coverage of the ALSA during TEVAR would increase the risk of upper-extremity subclavian steal syndrome, or possibly of spinal cord ischemia. Rizvi et al reported the need for revascularization need in investigations of cerebral and vertebrobasilar circulation [46]. To avoid arm claudication and vertebrobasilar ischemia, in-situ revascularization and bypass were performed for fear of subclavian steal syndrome [23,24]. However, based on limited cases of KD, more research and observations are needed before reaching a consensus.
Conclusions
KD, usually combined with right-sided aortic arch, is extremely rare and associated with ASA degeneration. Symptoms can be atypical for aneurysms due to persistent compression to adjacent tissues in the mediastinum. Several types of therapies were utilized and reported in the last 50 years, including best medication only, which was not recommended recently, and total arch replacement and debranching of the aortic arch followed with endovascular procedures and total TEVAR. Total arch replacement and debranching for KD under deep hypothermic circulatory arrest are not always required except for severe symptoms or lesions involving the ascending aorta. However, given the increased complexity of and limited experience with conventional surgery in such rare anatomic configurations, with the availability of PLZ, TEVAR is more feasible for KD patients who are asymptomatic or mildly symptomatic. Even in patients who also have acute dissection or rupture, TEVAR still has an acceptable safety profile, and there have been reports of encouraging postoperative outcomes. As the technology continues to improve, TEVAR may become the ideal interventional approach for KD under conditions of preoperative planning, careful delineation of anatomy, and strict patient enrollment.
References
1. Barr JG, Sepehripour AH, Jarral OA, A review of the surgical management of right-sided aortic arch aneurysms: Interact Cardiovasc Thorac Surg, 2016; 23; 156-62
2. Villaescusa JM, Sarralde JA, Nistal JF, Kommerell diverticulum and aberrant right subclavian artery: Rev Esp Cardiol (Engl Ed), 2016; 69(7); 696
3. Verkroost MW, Hamerlijnck RP, Vermeulen FE, Surgical management of aneurysms at the origin of an aberrant right subclavian artery: J Thorac Cardiovasc Surg, 1994; 107; 1469-71
4. Tanaka A, Milner R, Ota T, Kommerell’s diverticulum in the current era: A comprehensive review: Gen Thorac Cardiovasc Surg, 2015; 63; 245-59
5. Erben Y, Brownstein AJ, Velasquez CA, Natural history and management of Kommerell’s diverticulum in a single tertiary referral center: J Vasc Surg, 2020; 71; 2004-11
6. Austin EH, Wolfe WG, Aneurysm of aberrant subclavian artery with a review of the literature: J Vasc Surg, 1985; 2; 571-77
7. Cinà CS, Althani H, Pasenau J, Abouzahr L, Kommerell’s diverticulum and right-sided aortic arch: A cohort study and review of the literature: J Vasc Surg, 2004; 39; 131-39
8. Kim JB, Yang DH, Kang JW, Right aortic arch and an aberrant left subclavian artery arising from a Kommerell diverticulum complicated by acute aortic dissection: J Thorac Cardiovasc Surg, 2012; 144; 978-79
9. Tsukui H, Aomi S, Yamazaki K, Surgical strategy for Kommerell’s diverticulum: Total arch replacement: J Thorac Cardiovasc Surg, 2014; 148; 1423-27
10. Vendramin I, Lechiancole A, Frigatti P, Aortic arch aneurysm and Kommerell’s diverticulum: Repair with a single-stage hybrid approach: J Card Surg, 2019; 34; 641-44
11. Domínguez-Massa C, Berbel-Bonillo A, Pérez-Guillen M, Montero-Argudo JA, Dissected aberrant right subclavian artery with Kommerell diverticulum: Rev Port Cardiol, 2019; 38; 737.e1-e4
12. Shingaki M, Kurimoto Y, Morishita K, Anatomical repair for Kommerell diverticulum with deep site in-situ fenestration: Asian Cardiovasc Thorac Ann, 2018; 26; 467-69
13. Hara M, Fujii T, Kawasaki M, Endovascular treatment for Kommerell’s diverticulum with a right-sided aortic arch: Ann Vasc Dis, 2017; 10; 74-76
14. Tam W, Tang A, Woo B, Goh S, Perception of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement of authors publishing reviews in nursing journals: A cross-sectional online survey: BMJ Open, 2019; 9; e026271
15. He H, Yao K, Nie WP, Endovascular treatment for acute type B aortic dissection involving a right-sided aortic arch and Kommerell’s diverticulum. A case report and review of the literature: Ann Vasc Surg, 2015; 29; 841.e5-12
16. Kazuno K, Murata S, Endovascular repair for Kommerell’s diverticulum and right-sided aortic arch: Ann Vasc Dis, 2017; 10; 48-50
17. Li Z, Wu R, Liu C, Endovascular repair for Kommerell diverticulum with type A aortic dissection: Ann Thorac Surg, 2020; 110; e217-19
18. Hamady M, Sharma PM, Patel R, Hybrid endovascular repair of aneurysmal right-sided aortic arch and Kommerell’s diverticulum using a two-vessel branched stent graft: Case report and review of literature: SAGE Open Med Case Rep, 2017; 5; 2050313X17749082
19. Monaco M, Lillo S, La Marca Giordano A, Endovascular repair of a right-sided thoracic aortic aneurysm with Kommerell diverticulum and aberrant left subclavian artery: Ann Vasc Surg, 2014; 28; 1323.e1-5
20. Klonaris C, Avgerinos ED, Katsargyris A, Endovascular repair of a right-sided descending thoracic aortic aneurysm associated with a right aortic arch and a left subclavian artery arising from a Kommerell’s diverticulum: Cardiovasc Intervent Radiol, 2009; 32; 758-61
21. Midorikawa H, Kannno M, Ishikawa K, Endovascular repair of a Kommerell’s diverticulum and aneurysmal right-sided aortic arch: A case report: Ann Vasc Dis, 2009; 2; 54-57
22. Gao P, Wang M, Dong D, Endovascular repair of a Kommerell diverticulum anomaly: Ann Thorac Surg, 2015; 99; 1801-3
23. Motoki M, Hattori K, Kato Y, Endovascular repair of ruptured aberrant left subclavian artery with right aortic arch: Ann Thorac Surg, 2013; 95; 699-701
24. Naoum JJ, Parenti JL, LeMaire SA, Coselli JS, Endovascular repair of a right-sided descending thoracic aortic aneurysm with a right-sided aortic arch and aberrant left subclavian artery: Ann Thorac Surg, 2008; 85; 1074-76
25. Okada K, Sueda T, Orihashi K, Endovascular stent-graft repair for thoracic aortic aneurysm associated with right-sided aortic arch: J Thorac Cardiovasc Surg, 2001; 122; 185-86
26. Silveira PG, Franklin RN, Cunha JR, Total endovascular repair of aberrant left subclavian artery with Kommerell’s diverticulum using a customized branched device: J Vasc Surg, 2013; 57; 1123-25
27. Hai Z, Maohua W, Guangrui S, Successful endovascular repair of symptomatic aberrant left subclavian artery arising from Kommerell diverticulum with the chimney technique: J Thorac Cardiovasc Surg, 2017; 153; 806-8
28. Vinnakota A, Idrees JJ, Rosinski BF, Outcomes of repair of Kommerell diverticulum: Ann Thorac Surg, 2019; 108; 1745-50
29. Andersen ND, Barfield ME, Hanna JM, Intrathoracic subclavian artery aneurysm repair in the thoracic endovascular aortic repair era: J Vasc Surg, 2013; 57; 915-25
30. Zhou W, Endovascular repair of a type B aortic dissection with a right-sided aortic arch: Case report: J Cardiothorac Surg, 2013; 8; 18
31. Balani A, Marda SS, Kumar AD, Alwala S, Kommerell’s diverticulum: Unusual case expanding the horizon: Can Assoc Radiol J, 2015; 66; 298-99
32. Hashimoto M, Fukui T, Takanashi S, Surgical treatment for chronic type B aortic dissection originating from a Kommerell diverticulum with right-sided aortic arch: Eur J Cardiothorac Surg, 2014; 46; 753
33. Kouchoukos NT, Masetti P, Aberrant subclavian artery and Kommerell aneurysm: Surgical treatment with a standard approach: J Thorac Cardiovasc Surg, 2007; 133; 888-92
34. Bhandary SP, Papadimos TJ, Svensson LG, Sale S, Anesthetic management of the resection of a Kommerell’s diverticulum: J Cardiothorac Vasc Anesth, 2015; 29; 142-45
35. Boyd AJ, Kuhn DC, Lozowy RJ, Kulbisky GP, Low wall shear stress predominates at sites of abdominal aortic aneurysm rupture: J Vasc Surg, 2016; 63; 1613-19
36. Kim KM, Cambria RP, Isselbacher EM, Contemporary surgical approaches and outcomes in adults with Kommerell diverticulum: Ann Thorac Surg, 2014; 98; 1347-54
37. Yang C, Shu C, Li M, Aberrant subclavian artery pathologies and Kommerell’s diverticulum: A review and analysis of published endovascular/hybrid treatment options: J Endovasc Ther, 2012; 19; 373-82
38. Gomes MM, Bernatz PE, Forth RJ, Arteriosclerotic aneurysm of an aberrant right subclavian artery: Dis Chest, 1968; 54; 549-52
39. Ota T, Okada K, Takanashi S, Surgical treatment for Kommerell’s diverticulum: J Thorac Cardiovasc Surg, 2006; 131; 574-78
40. Gupta P, Harky A, Jahangeer S, Varying evidence on deep hypothermic circulatory arrest in thoracic aortic aneurysm surgery: Tex Heart Inst J, 2018; 45; 70-75
41. Rosu C, Dorval JF, Abraham CZ, Single-stage hybrid repair of right aortic arch with Kommerell’s diverticulum: Ann Thorac Surg, 2017; 103; e381-84
42. Kozlov BN, Panfilov DS, Saushkin VV, Shipulin VM, Hybrid treatment of aortic dissection associated with Kommerell’s diverticulum: Interact Cardiovasc Thorac Surg, 2016; 22; 854-55
43. Yu PS, Yu SC, Ng CT, Coil embolization of diverticulum of Kommerell: A targeted hybrid endovascular technique: Ann Thorac Surg, 2016; 101; e139-41
44. Tinelli G, Ferrer C, Giudice RKommerell Diverticulum Study Group, Long-term results of hybrid repair techniques for Kommerell’s diverticulum: J Vasc Surg, 2020; 72; 1213-21
45. El Batti S, Ben Abdallah I, Alsac JM, Vouhé P, Hybrid repair of Kommerell diverticulum in right aortic arch: Anatomic considerations: Ann Thorac Surg, 2018; 105; 1279
46. Rizvi AZ, Murad MH, Fairman RM, The effect of left subclavian artery coverage on morbidity and mortality in patients undergoing endovascular thoracic aortic interventions: A systematic review and meta-analysis: J Vasc Surg, 2009; 50; 1159-69
In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387