24 April 2021: Clinical Research
Anatomy and Correlation of the Coracoid Process and Coracoclavicular Ligament Based on Three-Dimensional Computed Tomography Reconstruction and Magnetic Resonance Imaging
Lan Xin1ABCDEFG, Jin Luo2BF, Mingying Chen3AE, Bing He4AC, Bi Tang1BD, Chunyang Tang1DF, Dongyu Zhang1BC, Lei Zhang5678ABCF*DOI: 10.12659/MSM.930435
Med Sci Monit 2021; 27:e930435






Abstract
BACKGROUND: The anatomy of the coracoid process and coracoclavicular (CC) ligament have been described and the correlation between them has been assessed based on 3-dimensional computed tomography (CT) reconstruction and magnetic resonance imaging (MRI), which provide a guide for coracoclavicular ligament reconstruction.
MATERIAL AND METHODS: Data were collected from 300 patients who underwent both CT and MRI of the shoulder joint from January 2017 to January 2019 at the Jiang’an Hospital of Traditional Chinese Medicine. The coracoid process was observed and classified and parameters of the CC ligament were measured according to different corneal types. All of the statistics were collected and classified by 2 radiologists, and average values were determined. Measurements of segments were taken as follows: ab – In the coronal plane, the length of the CC ligament from the central point of the CC ligament at the clavicular attachment to the CC ligament at the center of the CC attachment); ac – The distance from the center point of the CC ligament at the supraclavicular attachment to the acromioclavicular joint; de – In the sagittal plane, the length of the CC ligament from the center of the clavicular attachment to the coracoid attachment point; fg – The maximum diameter of the CC ligament at the anterior and posterior margins of the clavicle attachment; hi – The largest diameter of the CC ligament at the anterior and posterior edge of the coracoid process attachment; dj – The distance of the coracoclavicular ligament from the center point of the coracoid process attachment to the coracoid process tip; kl – The distance in the supraclavicular plane from the coracoclavicular ligament to the subcoracoid process.
RESULTS: The analysis showed that there are 5 types of coracoid process: gourd (31%), short rod (20%), long rod (22.3%), wedge (10.3%), and water drop (6.3%). There were statistically significant differences between the lengths of the ac and hi segments in the among the wedge and gourd-type and the short rod and water drop-type coracoid processes. There were statistically significant differences between the lengths of the ab, de, and fg segments in the short rod, gourd, and long rod-type coracoid processes. There were statistically significant differences between the lengths of the ac, fg, hi, dj, and kl segments in the water drop, gourd, and long rod-type coracoid processes.
CONCLUSIONS: The present study indicated that measurement of the CC ligament and the different shapes of the coracoid process provide an anatomical basis for the diagnosis and treatment of shoulder diseases and the data can be used to improve the safety of CC ligament reconstruction.
Keywords: Ligaments, Articular, Magnetic Resonance Imaging, Cine, Pathological Conditions, Anatomical, Acromioclavicular Joint, Clavicle, coracoid process, Imaging, Three-Dimensional, Magnetic Resonance Imaging, Shoulder Joint, Tomography, X-Ray Computed
Background
The coracoclavicular (CC) ligament extends from the coracoid process to the lower edge of the outer end of the clavicle and connects the 2 structures. It maintains a constant relationship between the scapula and the clavicle, which is the structure most important to the stability of the acromioclavicular joint [1]. The coracoid process is a hooked bone protruding from the superior side to the lateral side of the articular pelvis of the scapula. It is an important part of the anatomy of the human body and also an attachment point for important muscles in the chest and upper arms. The coracoid process plays an important role in the diagnosis and treatment of shoulder diseases, which is why it is called the “lighthouse” on the shoulder [2].
Acromioclavicular joint dislocation accounts for approximately 9% of all shoulder injuries and is a common indication for shoulder surgery. Often a result of an injury during sports, it is common in young athletes [3,4]. Coronal ligament reconstruction is one of the most commonly used clinical treatments for acromioclavicular joint dislocation requiring surgery, with good clinical results [5–7]. In reconstruction of the CC ligament, a clavicular-coracoid process bone tunnel should be established. The location, size, and thickness of the tunnel are vital to the success of surgery [8]. Because the clavicle is visible during the procedure, the location for the opening of the tunnel can be easily determined. Reconstruction has been described in a number of studies [9]. Because of the small size, deep location, and complexity of the anatomy that surrounds the coracoid process, there is no criterion standard for how to accurately create a transverse bone tunnel, and it can be difficult to position accurately, especially during minimally invasive surgery and or when visualization of the structures is limited [10,11]. Coracoid process fracture has become a serious complication of CC ligament reconstruction [12]. A significant amount of literature exists about coracoid ligament reconstruction around the world, but few reports exist about the morphological classification of the coracoid process.
Therefore, the purpose of the present study was to observe the anatomy of the CC ligament, study the correlation between it and the coracoid process, and discuss the indications and contraindications for CC ligament reconstruction based on three-dimensional (3D) computed tomography (CT) reconstruction and magnetic resonance imaging (MRI). The aim was to provide an anatomical basis for CC ligament reconstruction and reduce the risk of surgery and the incidence of postoperative complications.
Material and Methods
Patients
PATIENTS:
A retrospective analysis was performed of imaging data collected between 2017 and 2019 from 300 patients who underwent CT and MRI of the shoulder joint at the same time at the Jiang’an Hospital of Traditional Chinese Medicine. Of the patients, 160 were men and 140 were women, aged 20 to 60 years. Of the reconstructions, 132 were left-sided and 168 were right-sided, and they were in patients with an average age of 42.26±12.40 years old. Because of limited availability of data, information on height and weight was not included.
The present study was approved by the Ethics Committee of Jiang’an traditional Chinese Medicine Hospital in batch number KY2017005.
INCLUSION CRITERIA WERE:
1) age 20 to 60 years old; 2) normal development of the scapula, clavicle, and CC ligaments; 3) no history of fracture of coracoid process or clavicle; and 4) no history of CC ligament injury.
EXCLUSION CRITERIA WERE:
1) developmental deformities of the scapula; 2) other serious scapula diseases or deformity; 3) fractures around the scapula; 4) revision operation; and 5) infectious or chronic wasting disease.
METHODS:
Imaging data were collected from 3D CT reconstructions of the shoulder joints of 300 patients. The data were transmitted to Mimics software to create 3D reconstructions of the joints and 3D models of the coracoid processes.
The coracoid process was observed and classified by 2 radiologists, then the CC ligament was measured, and the final results were averaged. Differences of opinion were resolved by the Director of the Radiology Department. All of the personnel who made the observations had been engaged in professional imaging work for more than 10 years. All of the images collected for the present manuscript, the morphologic classification of the coracoid processes, and all data measurements were reviewed by imaging specialists.
For each patient, data from 3D CT reconstruction of the shoulder joint were collected and then the images themselves were uploaded into the Mimics software to create 3D models of the reconstructed coracoid process. Next, the shape of the coracoid process was observed and classified based on the 3D CT reconstruction. Then, the clearest and most complete layer of the CC ligament in the coronal and sagittal planes was selected on T2-weighted MRI images to measure the CC ligament and its adjacent structures, as shown in Figures 1 and 2.
Measurements of segments were taken as follows: ab - In the coronal plane, the length of the CC ligament from the central point of the CC ligament at the clavicular attachment to the CC ligament at the center of the CC attachment); ac – The distance from the center point of the CC ligament at the supraclavicular attachment to the acromioclavicular joint; de – In the sagittal plane, the length of the CC ligament from the center of the clavicular attachment to the coracoid attachment point; fg – The maximum diameter of the CC ligament at the anterior and posterior margins of the clavicle attachment; hi – The largest diameter of the CC ligament at the anterior and posterior edge of the coracoid process attachment; dj – The distance of the coracoclavicular ligament from the center point of the coracoid process attachment to the coracoid process tip; kl – The distance in the supraclavicular plane from the coracoclavicular ligament to the subcoracoid process.
STATISTICAL ANALYSIS:
Statistical analyses were performed using SPSS software, version 20.0 (IBM Corp.). All of the data from the measurements are shown as means±standard deviations. The data related to the CC ligament that corresponded to the coracoid process types were measured with single-factor analysis of variance (LSD-t), with
Results
There are 5 types of coracoid process, based on shape: gourd, short rod, long rod, wedge, and water drop, as shown in Figure 3.
Of the 3D reconstructions of adult scapulas, 94 (31%) were gourd, 60 (20%) were short rod, 67 (22.3%) were long rod, 31 (10.3%) were wedge, and 48 (16.3%) were water drop-type. The measurements of morphological parameters from the coracoid ligament that corresponded to each type of coracoid process are shown in Table 1. There were significant differences in measurements for segments ab (
Between the gourd and short rod-type scapulas, there were significant differences in morphological parameters of the CC ligament. In measurements for segments ac (
Discussion
The shoulder is the most flexible joint in the human body, with the largest range of movement and it plays a very important role in the movement of the upper arm. It is also the most unstable of the large joints in the body. Development of society and improvements in living standards have resulted in an increasing incidence of shoulder dislocation, which is particularly common in children, youth, and individuals who possess strong athletic ability [4]. Reconstruction of the CC ligament can help restore vertical stability of the shoulder joint in patients with acromioclavicular joint dislocation [1,3,13]. Endobutton CC ligament reconstruction has been widely used in clinic practice since it was first proposed by Struhl in 2007 [14,15]. Clinical results with CC ligament reconstruction are better than with a clavicular hook plate, screw internal fixation, and distal clavicle resection [16,17]. The key to a successful Endobutton reconstruction lies in the diameter and location of the bone tunnel. Improper pore size, positioning, or drilling position can easily lead to improper fixation of postoperative implants, resulting in surgical failure, another dislocation, and fractures of the clavicle and coracoid process; the bone fracture rate reportedly is as high as 5.3% [13]. During the procedure, the clavicle is perforated under arthroscopic guidance, but the coracoid process is not exposed. Therefore, the choice of location into which to drill is based solely on the experience of the surgeon, which greatly increases the risk of coracoid process fracture intraoperatively and postoperatively. At present, there are few clinical studies of the indications and contraindications for CC ligament reconstruction based on different shapes of the coracoid process, which is another reason for the high rates of surgical failure and postoperative complications. Therefore, there is an urgent need to study the anatomical morphology of the coracoid process and anatomical parameters related to CC ligament reconstruction.
The purpose of the present study was to explore the morphological correlation between the coracoid process and the CC ligament, and to provide an anatomical basis and predictive value for treatment of shoulder dislocation and guidance for surgical correction of it. In our study, we identified 5 types of coracoid processes, with the gourd-type being the most common. The anatomical parameters of most coracoid ligaments and their attachment points differ in keeping with the diverse coracoid processes. Therefore, the treatment of acromioclavicular dislocation should be individualized for patients with different coracoid processes, so as to improve the success rate for coracoid ligament reconstruction and reduce the occurrence of postoperative complications, especially coracoid fractures. Some researchers have conducted cadaver specimen studies on the attachment points of the CC ligament [18]. The present study, however, was based on 3D CT reconstruction and MRI. For clinical practice, it offers more intuitive guidance on diagnosing and treating patients and the data are more valuable than those from the cadaveric specimen study. Cheng Xue used 3D printing technology to study the feasibility of CC ligament reconstruction but did not include an in-depth discussion of the attachment point of the CC ligament [19]. The present research compensated for that deficiency by incorporating study of the attachment of the CC ligament as a way to guide clinicians on choosing the location for bone tunnel drilling.
Of the 5 forms of coracoid processes, the wedge-type had the shortest distances for segments ab, ac, hi, and de. Therefore, the coracoid process corresponding to the wedge-type may be shorter and thinner, which should be less prone to coracoid ligament rupture caused by excessive exercise and other factors. With a wedge-spaced coracoid process, there is less coracoid base and in principle, the punch position should be far away from the base. However, of the 5 types, it is associated with the shortest distance for segment dj, so punching into the coracoid base could cause a beak lock fracture after ligament reconstruction. Therefore, a coracoid process that is wedge-type is unfavorable and beak lock ligament revascularization of the tunnel should be considered so as not to push the coracoid upward like a thimble. Because of its shape, a wedge-type coracoid process is not easy to remove. Good long-term clinical and imaging results also have been achieved in practice with sleeve ring surgery, which can greatly reduce the risk of coracoid process fracture [20,21]. Of the segments dj was the shortest in the CC process, but de and fg also were short. The ligaments in the CC and the wedge-type coracoid processes are both short, thin, and easily broken. Individuals with this anatomy should take protective measures to avoid rupture of the CC ligament caused by strenuous exercise of the shoulder. A short rod-type coracoid process also has less bone mass, which increases the risk that it will fracture during drilling. It is also short, making it easy for the sheath ring to slip. Therefore, CC ligament reconstruction should not be used for patients with acromioclavicular joint dislocation and CC ligament rupture; internal fixation with a clavicular hook plate is a more appropriate alternative. With a water drop-type coracoid process, the tip of the coracoid process may be smaller and more prone to fall off when the annulus is performed. Therefore, in patients with that type of anatomy, a bone tunnel and annulus should not be used during ligament reconstruction. CC ligament reconstruction can be recommended for treatment of patients with acromioclavicular dislocation who have a long rod or gourd-type coracoid process because their coracoid process bone is long and their anatomical structure is suitable. During CC ligament reconstruction, the tunnel positions for the long rod and gourd-type coracoid processes were roughly the same: long rod-type ac 2.62±0.29 cm and dj 1.02±0.12 cm; gourd-type ac 2.78±0.15 cm and dj 1.00±0.16 cm. The length of the kl segment corresponding to the gourd-type coracoid process was 3.71±0.19 cm, and for the long rod-type coracoid process, it was 3.63±0.35 cm. These distances can guide selection of the length of the clinical loop. Methods of treatment of dislocation of the acromioclavicular joint should be dictated by the different coracoid processes.
The present study had some limitations. Data were collected only from patients in southwest China, most of whom were from rural areas, and the sample size was small. Further biomechanical studies should be performed to investigate whether a CC ligament corresponding to a wedge- or short rod-shaped coracoid process is shorter, thinner, or easier to break than the ligaments associated with the other coracoid process types.
Conclusions
In 300 patients, 5 types of CC ligaments were defined according to the shape of the coracoid process. Of them, the gourd-type was the most common in a Chinese population. Endobutton CC ligament reconstruction requires the creation of bone tunnels and their stability is the key to the success of the procedure. At present, however, there is no accurate way to determine the best anatomical location in which to drill for the tunnel entry. The present study showed that measurements and relevant parameters for the CC ligament and its attachment can be obtained with use of 3D reconstruction and MRI technology. Data from these images can guide successful clinical reconstruction of the CC ligament and provide an anatomical basis for the procedure.
Figures
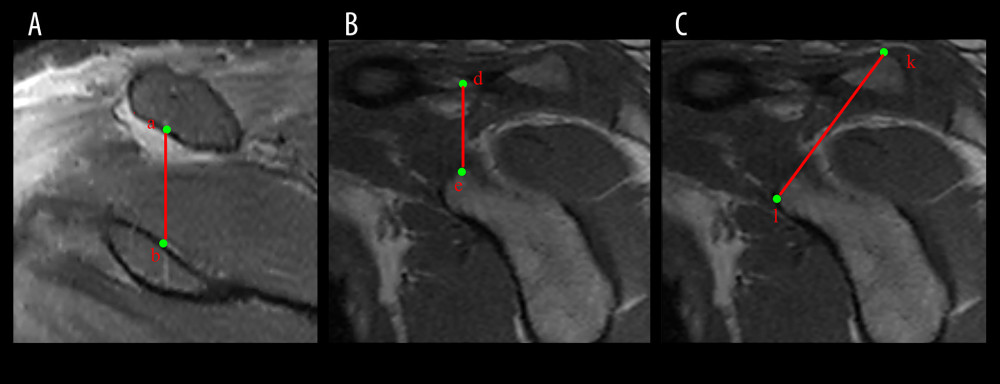 Figure 1. T2-weighted image correlation data for coracoclavicular (CC) ligament magnetic resonance imaging (MRI). (A) Measurement of the length of the CC ligament on T2-weighted MRI. (B) Sagittal coracoclavicular ligament length measurement on T2-weighted MRI. (C) Measurement of the distance from the supraclavicular plane to the subcoracoid plane on T2-weighted MRI. Point a: The central point of the CC ligament at the clavicular attachment. Point b: The CC ligament at the center of the CC attachment. Point d: The CC ligament at the center of the clavicular attachment. Point e: The CC ligament at the coracoid attachment point. Point k: The point of the supraclavicular plane through the CC ligament. Point l: The point of the subcoracoid plane through the CC ligament the length of the CC ligament. ab: The length of the CC ligament in the coronal plane. de: The length of the CC ligament in the sagittal plane. kl: The distance between the supraclavicular plane of the CC ligament and the subcoracoid process plane.
Figure 1. T2-weighted image correlation data for coracoclavicular (CC) ligament magnetic resonance imaging (MRI). (A) Measurement of the length of the CC ligament on T2-weighted MRI. (B) Sagittal coracoclavicular ligament length measurement on T2-weighted MRI. (C) Measurement of the distance from the supraclavicular plane to the subcoracoid plane on T2-weighted MRI. Point a: The central point of the CC ligament at the clavicular attachment. Point b: The CC ligament at the center of the CC attachment. Point d: The CC ligament at the center of the clavicular attachment. Point e: The CC ligament at the coracoid attachment point. Point k: The point of the supraclavicular plane through the CC ligament. Point l: The point of the subcoracoid plane through the CC ligament the length of the CC ligament. ab: The length of the CC ligament in the coronal plane. de: The length of the CC ligament in the sagittal plane. kl: The distance between the supraclavicular plane of the CC ligament and the subcoracoid process plane. 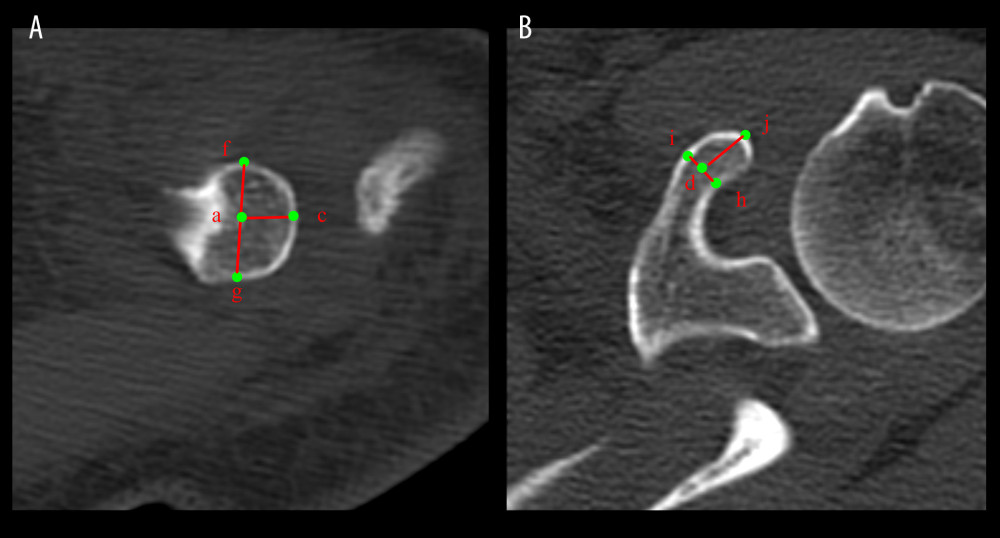 Figure 2. Image correlation data for computed tomography of the coracoclavicular (CC) ligament. (A) Subclavian observation. (B) superior coracoid process observation. Point a: The center of the CC ligament at the clavicular attachment. Point c: The farthest point at the acromion end of the clavicle. Point d: The point of the CC ligament at the center of the clavicular attachment. Point f: The point of the CC ligament at the anterior edge of the clavicular attachment. Point g: The posterior margin of the CC ligament at the clavicle attachment. Point h: The anterior edge of the CC ligament attached to the coracoid process. Point i: The posterior margin of the CC ligament attached to the coracoid process. Point j: Apical apex of the coracoid process. ac: Distance from the center point of the CC ligament at the supraclavicular attachment to the acromioclavicular joint. fg: The maximum diameter of the CC ligament at the anterior and posterior margin of the clavicle attachment. hi: The largest diameter of the CC ligament at the anterior and posterior edge of the coracoid process attachment. dj: The length of the CC ligament from the center point of the coracoid process attachment to the coracoid process tip.
Figure 2. Image correlation data for computed tomography of the coracoclavicular (CC) ligament. (A) Subclavian observation. (B) superior coracoid process observation. Point a: The center of the CC ligament at the clavicular attachment. Point c: The farthest point at the acromion end of the clavicle. Point d: The point of the CC ligament at the center of the clavicular attachment. Point f: The point of the CC ligament at the anterior edge of the clavicular attachment. Point g: The posterior margin of the CC ligament at the clavicle attachment. Point h: The anterior edge of the CC ligament attached to the coracoid process. Point i: The posterior margin of the CC ligament attached to the coracoid process. Point j: Apical apex of the coracoid process. ac: Distance from the center point of the CC ligament at the supraclavicular attachment to the acromioclavicular joint. fg: The maximum diameter of the CC ligament at the anterior and posterior margin of the clavicle attachment. hi: The largest diameter of the CC ligament at the anterior and posterior edge of the coracoid process attachment. dj: The length of the CC ligament from the center point of the coracoid process attachment to the coracoid process tip.  Figure 3. Reconstruction on three-dimensional computed tomography of the morphology of 5 types of coracoid processes. (A) Gourd. (B) Short rod. (C) Long rod. (D) Wedge. (E) Water drop.
Figure 3. Reconstruction on three-dimensional computed tomography of the morphology of 5 types of coracoid processes. (A) Gourd. (B) Short rod. (C) Long rod. (D) Wedge. (E) Water drop. References
1. Zhu NF, Rui BY, Anatomic study of coracoclavicular ligaments for reconstruction of acromioclavicular joint dislocations: J Orthop Sci, 2016; 216; 749-52
2. Mohammed H, Skalski MR, Patel DB, Coracoid process: The lighthouse of the shoulder: Radiographics, 2016; 36; 2084-101
3. Gibbs DB, Lynch TS, Nuber ED, Common shoulder injuries in American football athletes: Curr Sports Med Rep, 2015; 14; 413-19
4. Campbell ST, Heckmann ND, Shin SJ, Biomechanical evaluation of coracoid tunnel size and location for coracoclavicular ligament reconstruction: Arthroscopy, 2015; 31; 825-30
5. Hashiguchi H, Iwashita S, Abe K, Arthroscopic coracoclavicular ligament reconstruction for acromioclavicular joint dislocation: J Nippon Med School, 2018; 85; 166-71
6. Mori D, Yamashita F, Kizaki K, Anatomic coracoclavicular ligament reconstruction for the treatment of acute acromioclavicular joint dislocation: Minimum 10-year follow-up: JB JS Open Access, 2017; 2; e0007
7. Teodoro RL, Nishimi AY, Pascarelli L, Surgical treatment of acromioclavicular dislocation using the Endobutton: Acta Ortopedica Brasileira, 2017; 25; 81-84
8. Wylie JD, Johson JD, DiVence J, Shoulder acromioclavicular and coracoclavicular ligament injuries: Common problems and solutions: Clin Sports Med, 2018; 37; 197-207
9. Rios CG, Arciero RA, Mazzocca AD, Anatomy of the clavicle and coracoid process for reconstruction of the coracoclavicular ligaments: Am J Sports Med, 2017; 35; 811-17
10. Sella GDV, Miyazaki AN, Nico MAC, Study on the anatomic relationship between the clavicle and the coracoid process using computed tomography scans of the shoulder: J Shoulder Elbow Surgery, 2017; 26; 1740-47
11. Koh KH, Shon MS, Choi NH, Anatomic tunnel placement is not feasible by transclavicular-transcoracoid drilling technique for coracoclavicular reconstruction: A cadaveric study: Arthroscopy, 2018; 34; 2012-17
12. Xue C, Song L, Li X, Coracoclavicular ligaments anatomical reconstruction: A feasibility study: Int J Med Robot, 2015; 11; 181-87
13. Woodmass JM, Esposito JG, Ono Y, Complications following arthroscopic fixation of acromioclavicular separations: A systematic review of the literature: Open Access J Sports Med, 2015; 6; 97-107
14. Struhl S, Double endobutton technique for repair of complete acromioclavicular joint dislocations: Techniq Shoulder Elbow Surgery, 2007; 8; 175-79
15. North AS, Wilkinson T, Surgical reconstruction of the acromioclavicular joint: Can we identify the optimal approach: Arthroscopy, 2018; 13; 69-74
16. Mouhsine E, Garofalo R, Crevoisier X, Grade III acromioclavicular dislocations: Results of conservative treatment: J Shoulder Elbow Surg, 2003; 12; 599-602
17. Monica J, Vredenburgh Z, Korsh J, Acute shoulder injuries in adults: Am Family Phys, 2016; 94; 119-27
18. Chahla J, Marchetti DC, Moatshe G, Quantitative assessment of the coracoacromial and the coracoclavicular ligaments with 3-dimensional mapping of the coracoid process anatomy: A cadaveric study of surgically relevant structures: Arthroscopy, 2018; 34; 1403-11
19. Xue C, Song LJ, Li X, Coracoclavicular ligaments anatomical reconstruction: a feasibility study: Int J Med Robot, 2015; 11(2); 181-87
20. Parnes N, Blevins M, Caery P, Arthroscopic reconstruction of the coracoclavicular ligaments using a cerclage technique: Arthroscopy Techniq, 2016; 5; 241-46
21. Paenes N, Friedman D, Phillips C, Outcome after arthroscopic reconstruction of the coracoclavicular ligament using a double-bundle coracoid cerclage technique: Arthroscopy, 2015; 31; 1933-40
Figures
Figure 1. T2-weighted image correlation data for coracoclavicular (CC) ligament magnetic resonance imaging (MRI). (A) Measurement of the length of the CC ligament on T2-weighted MRI. (B) Sagittal coracoclavicular ligament length measurement on T2-weighted MRI. (C) Measurement of the distance from the supraclavicular plane to the subcoracoid plane on T2-weighted MRI. Point a: The central point of the CC ligament at the clavicular attachment. Point b: The CC ligament at the center of the CC attachment. Point d: The CC ligament at the center of the clavicular attachment. Point e: The CC ligament at the coracoid attachment point. Point k: The point of the supraclavicular plane through the CC ligament. Point l: The point of the subcoracoid plane through the CC ligament the length of the CC ligament. ab: The length of the CC ligament in the coronal plane. de: The length of the CC ligament in the sagittal plane. kl: The distance between the supraclavicular plane of the CC ligament and the subcoracoid process plane.Figure 2. Image correlation data for computed tomography of the coracoclavicular (CC) ligament. (A) Subclavian observation. (B) superior coracoid process observation. Point a: The center of the CC ligament at the clavicular attachment. Point c: The farthest point at the acromion end of the clavicle. Point d: The point of the CC ligament at the center of the clavicular attachment. Point f: The point of the CC ligament at the anterior edge of the clavicular attachment. Point g: The posterior margin of the CC ligament at the clavicle attachment. Point h: The anterior edge of the CC ligament attached to the coracoid process. Point i: The posterior margin of the CC ligament attached to the coracoid process. Point j: Apical apex of the coracoid process. ac: Distance from the center point of the CC ligament at the supraclavicular attachment to the acromioclavicular joint. fg: The maximum diameter of the CC ligament at the anterior and posterior margin of the clavicle attachment. hi: The largest diameter of the CC ligament at the anterior and posterior edge of the coracoid process attachment. dj: The length of the CC ligament from the center point of the coracoid process attachment to the coracoid process tip.Figure 3. Reconstruction on three-dimensional computed tomography of the morphology of 5 types of coracoid processes. (A) Gourd. (B) Short rod. (C) Long rod. (D) Wedge. (E) Water drop. Tables
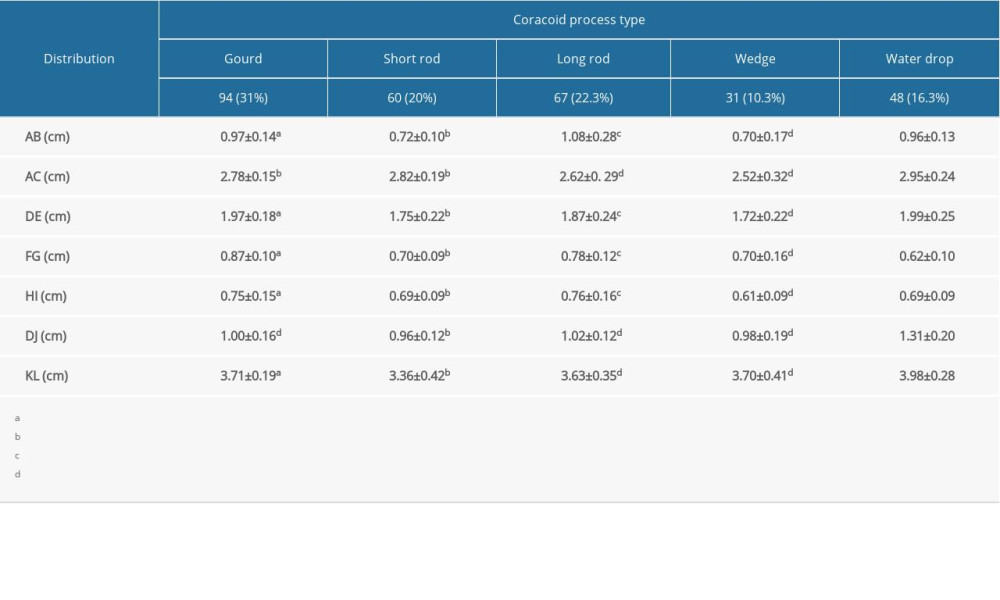 Table 1. Anatomical morphological measurements of the coracoid process and coracoclavicular ligament (χ̄±s).
Table 1. Anatomical morphological measurements of the coracoid process and coracoclavicular ligament (χ̄±s).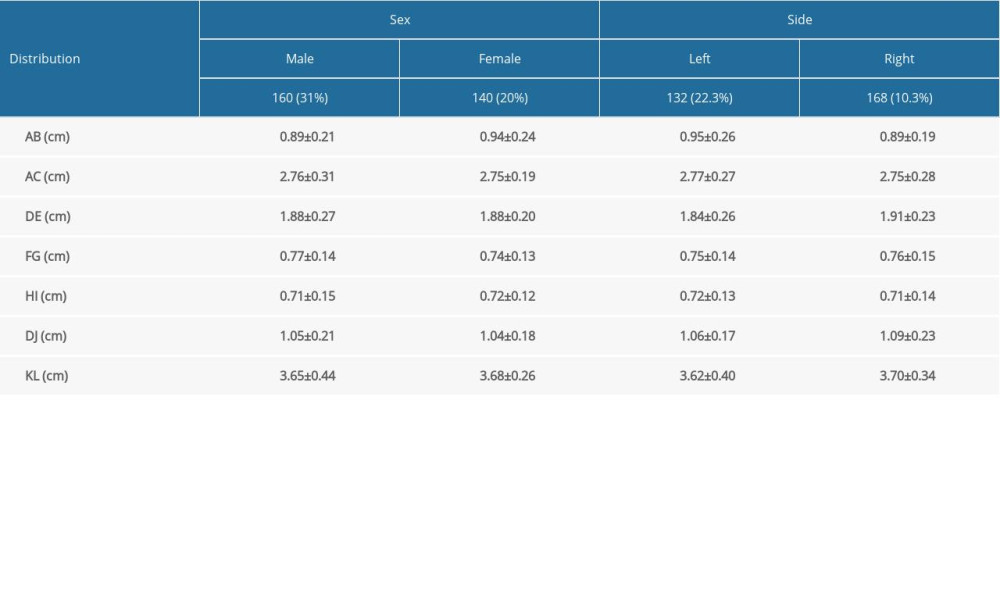 Table 2. Comparisons of anatomic morphological measurements of coronal and coracoclavicular ligaments based on sex and side (χ̄±s).Table 1. Anatomical morphological measurements of the coracoid process and coracoclavicular ligament (χ̄±s).Table 2. Comparisons of anatomic morphological measurements of coronal and coracoclavicular ligaments based on sex and side (χ̄±s).
Table 2. Comparisons of anatomic morphological measurements of coronal and coracoclavicular ligaments based on sex and side (χ̄±s).Table 1. Anatomical morphological measurements of the coracoid process and coracoclavicular ligament (χ̄±s).Table 2. Comparisons of anatomic morphological measurements of coronal and coracoclavicular ligaments based on sex and side (χ̄±s). In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387