01 September 2021: Lab/In Vitro Research
A Pilot Investigation Generating an Alternative Therapeutic Strategy Combining Deproteinized Bovine Bone and Gelatin Sponge for a Novel Implant Material in Sinus Floor Elevation Operation
Xiaofeng Chang12BCDEF, Miao Wang1BCDEF, Liangzhi Du12BCDF, Lifan Liao12BCDF, Lixing He1BCF, Huixia Zhou1BC, Longlong He12ABDG*DOI: 10.12659/MSM.930785
Med Sci Monit 2021; 27:e930785






Abstract
BACKGROUND: Implant placement in the posterior maxilla is typically complicated by a shortage of bone. Gelatin sponge could be combined with an appropriate material to enhance mechanical strength and maintain stability of an implant. This study aimed to evaluate the clinical application of bone grafting with bovine bone mixed with gelatin sponge.
MATERIAL AND METHODS: Fifty-four patients were divided into a control group (deproteinized bovine bone, n=26) and a test group (deproteinized bovine bone combined with gelatin sponge, n=28). Implants were placed in patients simultaneously after surgery (operation). Cone-beam computed tomography examination was carried out immediately and 6 months after surgery. Space with grafting materials was measured with Mimics software (version 16.0).
RESULTS: No remarkable differences were found for simultaneous placement, height of residual bone, delayed placement, width of residual bone, graft volume immediately after surgery (V₁), graft volume 6 months after surgery (V₂), or volumetric change rate between the test group and the control group (P>0.05). Graft volume V₂ was remarkably decreased compared with V1 in the control and test groups (P=0.01). There were no significant differences for bone height immediately after surgery (H₁) and bone height at 6 months after surgery (H₂) between the 2 groups. Bone height H₂ was markedly decreased compared with H1 (P<0.05). At 1 year after implantation, there was 1 implant loss in the control group and 2 in the test group. The implant survival rate in the control group was 97.62% and 95.24% in the test group.
CONCLUSIONS: Absorbable gelatin sponge combined with bovine bone particles was an effective and economical material for use in routine sinus floor elevation surgery.
Keywords: alveolar bone grafting, Arrhythmia, Sinus, Dental Implantation, Maxillary Sinus, Absorbable Implants, Bone Substitutes, Bone Transplantation, Cone-Beam Computed Tomography, Female, Gelatin Sponge, Absorbable, Humans, Materials Testing, Maxilla, Pilot Projects, Sinus floor augmentation
Background
Replacement of an implant in the posterior maxilla can commonly cause bone shortage, and bone resorption and/or sinus pneumatization can caused height shortage [1]. The maxillary sinus floor elevation approach is an effective and safe strategy demonstrating higher implant survival rate, and it has been commonly applied for resolving the limitations of implant replacement [2–4]. Tan et al [3] reported that implants inserted in combination with sinus floor elevation had a lower incidence of complications during and after surgery. Pjetursson et al [4] also found that insertion of the dental implant combined with maxillary sinus floor elevation was associated with higher implant survival rates and a lower incidence of surgical complications. Therefore, the maxillary sinus floor elevation approach is a promising method for efficient placement of an implant. Bovine bone grafts are currently extensively used for grafting implants (or material) [5,6], although some research has suggested that its low absorption rate has a negative impact on new bone formation [7,8].
Gelatin is characterized by biocompatibility, biodegradability, noncarcinogenicity, and nontoxicity, and it is extensively applied in medical fields for engineering scaffolds and as drug carriers [9]. As a scaffold with a porous 3-dimensional (3D) structure, gelatin sponge could provide ample area for cell adhesion, but it demonstrates poor mechanical strength [9]. However, fortifying the gelatin sponge scaffold with an appropriate material can enhance its mechanical strength and maintain the stability during the implantation [10]. A few studies have reported the use of gelatin sponge as a suitable material for generating 3D bovine chondrocyte cultures [11,12]. Moreover, a sinus lift without grafting material is not a widely accepted concept and is controversial [13,14]; however, the sinus demonstrates potentially high self-healing capability. We speculated that a mixture combining deproteinized bovine bone (DBB) with gelatin sponge would serve as a novel grafting implant material in patients.
In this study, we hypothesized that the clinical outcomes of patients after routine sinus floor elevation surgery using DBB combined with gelatin sponge would be satisfactory. Therefore, the present clinical research was designed and conducted to provide evidence supporting the application of a novel grafting strategy in the sinus.
Material and Methods
ETHICS AND CONSENT:
This study was approved by the Ethics Committee of the College of Stomatology of Xi’an Jiaotong University (No. xjkq11[2017] No.14). The project complies with the regulations contained in the National Statement on Ethical Conduct in Research involving humans and complies with the regulations governing experimentation on humans. All patients provided informed consent prior to enrolling in the study.
INCLUSION CRITERIA:
Eligibility for the study was based on the following inclusion criteria: (1) patients were 18 years or older at the time of surgery; (2) the height of the residual alveolar bone for the edentulous maxilla below the sinus floor was less than 5 mm and more than 1 mm, while the width of the residual alveolar bone was more than 6 mm, based on measurement by cone-beam computed tomography (CBCT); (3) results were available for repeat CBCT examinations (prior to the surgery, immediately after surgery, and 6 months after the maxillary sinus floor elevation); (4) patients were free of chronic or acute infection of the sinus and other disorders of the maxillary sinus; and (5) patients were generally healthy, did not experience complications after local anesthesia, and had no systemic disorders that could influence wound healing.
EXCLUSION CRITERIA:
Patients were considered ineligible if any of the following criteria were met: (1) they received any therapeutic treatment that could interfere with surgery or the operation or influence wound healing after the maxillary sinus floor elevation; (2) current pregnancy; (3) presence of psychiatric problems or physical disability that could interfere with proper oral hygiene; (4) a history of chronic drug administration or abuse of alcohol, or smoking more than 10 cigarettes daily; (5) use of medications that interfere with bone formation; (6) the presence of mucosal diseases such as erosive lichen planus or uncontrolled periodontal disease; (7) previous radiotherapy and/or chemotherapy; (8) severe bruxism or jaw-clenching habits; (9) signs or symptoms of acute sinus infections or the presence of benign/malignant tumors of the maxillary sinus; and (10) the presence of large sinus membrane perforations that could not be repaired/healed during the sinus floor elevation process.
SAMPLE SIZE ESTIMATE:
To minimize the overall sample size of the pilot and the main trial together, we used Kieser and Wassmer’s method to set the pilot trial sample size, as described by Whitehead et al [15]. They applied the 80% upper confidence limit approach to the sample size calculation and found that a pilot trial sample size between 20 and 40 would minimize the overall sample size for a main study sample size of 80–250, corresponding to standardized effect sizes of 0.4 and 0.7 (for 90% power based on a standard sample size calculation).
PARTICIPANT RECRUITMENT AND STUDY DESIGN:
This study complied with CONSORT guidelines [16]. A controlled clinical trial was designed to compare the clinical results of a modified grafting technique with the traditional method. According to the inclusion and exclusion criteria, a total of 60 patients were recruited in the Hospital of Stomatology of Xi’an Jiaotong University, between October 2014 and October 2016. CBCT was done for all participants before surgery, immediately after surgery, and 6 months after surgery. The opposite dentition of all the patients enrolled in this study was their natural dentition. Written informed consent was obtained from all subjects for use of their clinical and radiological data for research purposes. The randomization approach was used to allocate the patients to the control group (n=30) or the test group (n=30). The 2 surgeons (Dr. Du and Dr. He) were trained, and all participants (n=60) were randomly assigned to the control group (Dr. Du) or the test group (Dr. He) by a nurse (Mrs. Liu). Large-diameter particles (1–2 mm) of Bio-Oss® only (Geistlich Pharma AG, Switzerland) were used in the control group (n=30). In the test group (n=30), large-diameter particles (1–2 mm) of Bio-Oss® and gelatin sponge (Jingling Pharm, Nanjing, China) were used, with 1 package of 0.5 g (or 0.5 cm3) Bio-Oss® bone paired with 1 sheet of gelatin sponge (0.6 cm3).
The height of residual alveolar bone and the stability for dental implant materials were assessed during the operation, and the patients received transplants with dental implant materials simultaneously after the operation. Patients could also receive transplants with a dental implant at 6 months after the maxillary sinus floor elevation, but if the height of the residual alveolar bone was more than 3 mm, the patients had to receive the dental implant material simultaneously.
A total of 60 patients received maxillary sinus elevation, but 6 were excluded from the analysis owing to indistinct CBCT images that prevented accurate 3D reconstruction. The remaining 54 patients were divided into the control group (n=26) and the test group (n=28).
SURGICAL PROCEDURE:
All patients received antibiotic prophylaxis therapy 30 min prior to surgery. A 0.2% chlorhexidine mouth rinse was utilized 3 times, 3 min each time, prior to surgery. All patients underwent the same surgery for sinus floor elevation using a lateral wall method under local anesthesia. Middle/crestal incisions and vertical incisions were made along the residual alveolar bone to enhance the muco-periosteal flap and expose the wall of the buccal sinus. In the lateral wall of the maxilla, a piezoelectric osteotome was used to create a rectangular access window following the treatment plan and the patient’s anatomy. Bone surrounding the access window was gently fractured using the osteotome and conserved in normal saline, while intact sinus membranes were enhanced superiorly. Bio-Oss® was used to fill the lifted space in the control group, while the mixture combining Bio-Oss® plus gelatin sponge was used in the test group (Figure 1). Based on the residual alveolar bone height (≥3 mm) and the primary stability (≥10 N·cm) of the dental implant, most patients received the dental implant placement simultaneously. The bone preserved in saline was replaced in the buccal window and the collagen membrane was covered on top. The flap was sutured for primary closure.
CBCT was used to observe the result of the graft surgery. All patients underwent the same surgical protocol. Antibiotic prophylaxis therapy (0.5 g amoxicillin, 3 times daily, and metronidazole 0.4 g, twice daily) was administered for 7 days postoperatively, and patients were instructed to use a 0.2% chlorhexidine mouth rinse for 10–14 days and pain killer as needed. Follow-up occurred at 10–14 days after surgery, 2 months after surgery, and 6 months after surgery. Patients without a simultaneous implant placement received implant placement at 6 months.
CLINICAL FOLLOW-UP:
All patients received cement-retained or screw-retained fixed prosthetic restorations. Evaluation of the implant condition 1 year after loading included clinical examination of implant loosening and X-ray of the implant without continuous shadow. After 1 year of functional loading of the implant, the bone absorption in the vertical direction was less than 1.5 mm. In addition, patients had no signs or symptoms of persistent or irreversible subjective pain, such as foreign body sensation and so forth [17].
RADIOGRAPHIC ANALYSIS:
Personnel were trained to calculate the volume of every CBCT and were blind to whether patients were in the control or test group. To evaluate the volumetric bone graft changes, CBCT was conducted at 3 time points, including prior to surgery, immediately after surgery, and 6 months after surgery. The CBCT images were obtained with a CBCT scanner (DCTPro, Vatech. Co, Korea) at 120 kVp and 18.54 mA, with a voxel size of 0.2 mm and a field of view of 12×8 cm.
The data derived from CBCT were captured as files in digital images and communications of medicine (DICOM) format. Volumetric changes for implant were evaluated and analyzed with professional Mimics software (version 16.0; Materialise Europe, Leuven, Belgium). Three-dimensional reconstruction was used for the sinus bone grafting area to assess volume changes for the implants in the test and control groups. The 3D reconstruction analysis was carried out using the area-sum method, which is an approach for calculating the volume from sequential computed tomography images [18]. The linear method for the measurements and the dimensional variation analyses were carried out as previously described [19]. For each section, the software calculates the volume in cubic centimeters within the delineated region of interest, according to the thickness of the slice. The individual volume of each slice was added to the volume of the preceding sections, until the complete delineation was reached. At this point, the volumetric function of the software was added, and the result was automatically obtained (Figure 2). The reduction rate of the grafting volume was (V1–V2)/V1×100%, where V1 was the volume immediately after surgery and V2 was the volume at 6 months after surgery. The height was defined as the measurement from the implant tip to the bone end above the implant tip. The height change above the implant was calculated as (H1–H2)/H× 100%.
STATISTICAL ANALYSIS:
The primary measured outcomes included reductions in grafted bone volume and in bone height between the top of the implants and the sinus membrane after 6 months. Data were statistically analyzed with
Results
CHARACTERISTICS OF PATIENTS:
A total of 84 implants (n=78 for BEGO implant systems (Bremen, Germany), n=6 for OSSTEM implant systems (Seoul, Korea)) were placed successfully. Age and sex distribution between the test group (mean: 51.18±9.70 years; 17 men, 11 women) and the control group (mean: 52.27±7.69 years; 14 men, 12 women) had no significant differences (
IMPLANT DISTRIBUTION BETWEEN TEST AND CONTROL GROUPS:
Table 1 presents the ratio of implants simultaneously inserted, the residual alveolar bone height and width, and their respective P values for the test and control groups. Our findings showed no marked differences for height of residual bone, simultaneous placement, width of residual bone, and delayed placement between the test group and the control group (Table 1, P>0.05).
GRAFT VOLUMES AND VOLUMETRIC CHANGE RATES BETWEEN TEST AND CONTROL GROUPS:
There were no remarkable differences for the graft volume immediately after surgery (V1) (1.82±0.78 cm3 vs 1.77±0.81 cm3, P=0.793), graft volume at 6 months after surgery (V2) (1.62±0.72 cm3 vs 1.61±0.76 cm3, P=0.956), and volumetric change rates (12.76±5.45% vs 10.22±4.37%, P=0.069) between the control and test groups (Table 2, P>0.05). However, graft volume was remarkably decreased at 6 months after surgery (V2) compared with immediately after surgery (V1) in both the control and test groups (Table 2, both P=0.01).
BONE HEIGHT BETWEEN TEST AND CONTROL GROUPS:
Our data showed no remarkable differences for the bone height immediately after surgery (H1) (4.04±1.57 mm vs 3.95±1.76 mm, P=0.803) and bone height at 6 months after surgery (H2) (3.35±1.54 mm vs 3.30±1.62 mm, P=0.882) between the control and test groups (Table 3). Meanwhile, there was no significant difference for the mean height reduction rate between the control and test groups (Table 3, P>0.05). For both the control and test groups, bone height was markedly decreased at 6 months after surgery (H2) compared with immediately after surgery (H1) (Table 3, both P<0.05).
IMPLANT LOSS AMONG PATIENTS:
At 1 year post implantation, there was one implant loss in the control group and 2 implant losses in the test group. Furthermore, the implant survival rate was 95.24% in the test group and 97.62% in the control group, and these rates were not significantly different (
Discussion
Whether grafting material is a necessity in sinus floor elevation is controversial. Some studies showed clinical success with rigid synthetic resorbable barriers used for space maintenance without bone grafts after maxillary sinus floor elevation [20,21]. Other studies showed clinical success without grafting material [13,14,22]. However, the usage of bone particles in the sinus is generally deemed necessary, but few attempts have been made to apply new materials or mixtures [23,24].
We have some experience in osteotome sinus elevation without grafting material, and some research supports that approach [25,26]. However, the clinical situation of sinus floor elevation using the lateral wall method is different. This method requires more space and would permit more implants.
Lundgren et al [14] showed that sinus lift could be successful without grafting materials, which Palma et al [13] previously proved in a primate model. Meanwhile, a study conducted by Ahn et al [27] indicated that no new bone formed in 6 out of 8 patients. Due to such findings, not using grafting material in patients undergoing sinus elevation does not appear to be a wise choice.
Gelatin sponge was previously used as a hemostatic material after tooth extraction, and the white or yellow soft and porous sponge made from special gelatin could degrade and be absorbed. Owing to its porous nature, the gelatin can absorb blood, promote platelet rupture, make fibrinogen turn into fibrin, and allow blood to coagulate. Gelatin is also an excellent scaffold in terms of biocompatibility and biodegradability in tissue engineering [28,29].
Step-by-step attempts were made to use gelatin sponge as part of grafting material. At first, it was only used in the posterior area of the sinus where no implant could be inserted. Later, gelatin sponge was placed between the implant’s end and the sinus membrane, and then small chunks of gelatin sponge were mixed with bone particles at a ratio of almost 1: 1. Finally, a pilot study was carried out to obtain more information on the absorption of the graft materials and the clinical results. CBCT was more accurate and reliable than 2-dimensional X-ray imaging techniques [30–32] and was used to measure bone graft volumetric contraction in the current study.
The reduced volume following the procedures of augmentation was primarily affected by the characteristics of the bone implant material. Because gelatin sponge is readily absorptive and will certainly be absorbed when grafted within a short time, the expected contraction of the graft area should be greater than with the traditional method. As it has limited or no resorption, DBB has been widely used in recent years. According to previous studies [33,34], the resorption rate for DBB ranged from 6% to 20% following surgery for sinus floor elevation. In the current study, the volume reduction rate was 12.76±5.45% in the control group, which was close to previous literatures. Interestingly, the study results showed that the contraction between the 2 groups was not significantly different (
There are several possible reasons why the test group had better results. First, when gelatin sponge was grafted into the sinus, it was compressed and there may have been some expansion in the hours after the surgery; after contraction, the result was then close to the control group. Second, DBB particles in the sinus would absorb blood and become stable. When gelatin sponge was cut into small chunks, the gelatin sponge chunks would also absorb blood and became stable blood clots surrounding stable DBB particles after grafting. The osteogenic speed within DBB particles was slower than in natural blood clot, and this phenomenon (grafted DDB after 6 months was still soft, but new bone was always much harder in the extraction socket site after 6 months) could easily be seen in patients. The blood clot with gelatin sponge would act like small chamber within stable grafted bone materials, DBB was osteo-inductive, the sinus membrane had features such as periosteum, the blood supply in sinus was good, the space of sinus was stable, and the small chamber could turn into cancellous bone with very limited contraction. Meanwhile, Yanfeng et al [35] reported that bovine basic fibroblast growth factor/human bone morphogenetic protein combined with gelatin sponge could accelerate and improve fracture healing compared with the combination without gelatin sponge involvement. Additionally, sinus lift without grafting material is not a widely accepted concept and is controversial [13,14]. Therefore, in our study, we added the gelatin sponge to the DBB materials. However, the best ratio of bone particles and small gelatin sponge chunks needs further study; the volume ratio used in the current study was 1: 1.2 (0.5 cm3 bone particles: 0.6 cm3 gelatin sponge).
The clinical results were successful, most implants were restored on time. The 2 failed implants in the test group occurred in 1 patient, mostly because of soft bone and poor osseo-integration and loosening after loading. The failed implant in the control group became loose after 2 months because of poor osseo-integration. The wounds healed later, and the sinus floor grafts were stable afterward.
This study had a few limitations. First, it did not include histological analysis at 6 months after healing. Second, no conclusions could be made on the relationship between volumetric reduction and histo-morphometric measurement. Most patients received implant insertion right after the grafting surgery, specimen harvest would have caused additional trauma, and most patient refused to do the surgery. Third, the allocation treatments were not disclosed after the sinus mucosa elevation at the time of placing the filler; however, the methods in this study did not allow this. Fourth, this study did not apply the same protocol for the delayed implant insertion and the simultaneous implant insertion. The material could be harvested easily at the time of the second surgery to conduct a histological analysis. Fifth, the patients’ selection as distal bilateral edentulism could have permitted performing a split mouth evaluation with removal of interindividual differences for the test procedure and the control procedure; however, this was not done in this study. Sixth, this study only included follow-up time of 6 months after surgery, which was too short for meaningful clinical findings on the implant survival rates.
In a future study, we would like to conduct a histological analysis at 6 months after healing and clarify the relationship between the volumetric reduction and histo-morphometric measurement. In addition, the allocation treatments would also be disclosed after the sinus mucosa elevation at the time of placing filler, and a longer follow-up after the surgery would be conducted. The application of gelatin sponge combined with bovine bone particles in routine sinus floor elevation surgery should be assessed in a larger sample of patients.
Conclusions
The gelatin sponge combined with bovine bone particles in routine sinus floor elevation surgery demonstrated improved simultaneous placement, height of residual bone, delayed placement, width of residual bone, graft volume immediately after surgery (V1), graft volume 6 months after surgery (V2), and volumetric change rate. No implant loss occurred and higher implant survival rates were demonstrated in the patients undergoing the above treatment. Therefore, the absorbable gelatin sponge combined with bovine bone particles was an effective and economical material used in routine sinus floor elevation surgery.
Figures
 Figure 1. The gelatin sponge was cut into small chunks and mixed with bovine bone, and then mixed with saline or local blood. Around the window area, only bovine bone particles were used.
Figure 1. The gelatin sponge was cut into small chunks and mixed with bovine bone, and then mixed with saline or local blood. Around the window area, only bovine bone particles were used. 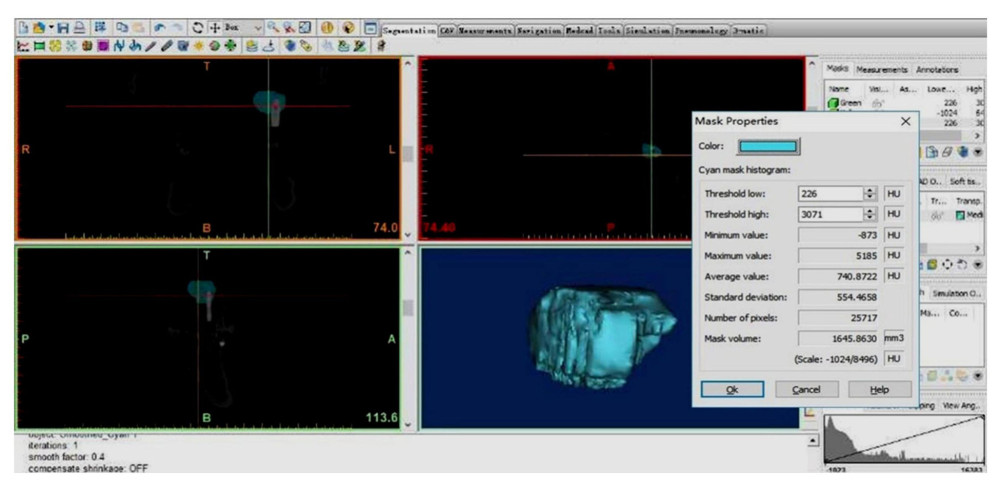 Figure 2. Digital (3-dimensional) reconstruction technique was carried out through selecting the grafting volume, while the artificial reconstruction was also calculated according to the threshold values. In this study, the threshold values were selected based on gray values for the native bone, grafting bone, sinus cavity, and soft tissue, with analysis by Mimics software (version 16.0, Leuven, Belgium). This representative image is from a patient at 6 months after surgery.
Figure 2. Digital (3-dimensional) reconstruction technique was carried out through selecting the grafting volume, while the artificial reconstruction was also calculated according to the threshold values. In this study, the threshold values were selected based on gray values for the native bone, grafting bone, sinus cavity, and soft tissue, with analysis by Mimics software (version 16.0, Leuven, Belgium). This representative image is from a patient at 6 months after surgery. References
1. Mumcu E, Dayan SC, Effect of smoking and locations of dental implants on peri-implant parameters: 3-years follow-up: Med Sci Monit, 2019; 25; 6104-9
2. Bornstein MM, Chappuis V, von Arx T, Buser D, Performance of dental implants after staged sinus floor elevation procedures: 5-year results of a prospective study in partially edentulous patients: Clin Oral Implants Res, 2008; 19; 1034-43
3. Tan WC, Lang NP, Zwahlen M, Pjetursson BE, A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. Part II: Transalveolar technique: J Clin Periodontol, 2008; 35; 241-54
4. Pjetursson BE, Tan WC, Zwahlen M, Lang NP, A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation: J Clin Periodontol, 2008; 35; 216-40
5. Stumbras A, Krukis MM, Januzis G, Juodzbalys G, Regenerative bone potential after sinus floor elevation using various bone graft materials: A systematic review: Quintessence Int, 2019; 50; 548-58
6. Musson DS, Gao R, Watson M, Bovine bone particulates containing bone anabolic factors as a potential xenogenic bone graft substitute: J Orthop Surg Res, 2019; 14; 60
7. Lutz R, Berger-Fink S, Stockmann P, Sinus floor augmentation with autogenous bone vs. a bovine-derived xenograft – a 5-year retrospective study: Clin Oral Implants Res, 2015; 26; 644-48
8. Aludden HC, Mordenfeld A, Hallman M, Lateral ridge augmentation with Bio-Oss alone or Bio-Oss mixed with particulate autogenous bone graft: A systematic review: Int J Oral Maxillofac Surg, 2017; 46; 1030-38
9. Yang G, Xiao Z, Long H, Assessment of the characteristics and biocompatibility of gelatin sponge scaffolds prepared by various crosslinking methods: Sci Rep, 2018; 8; 1616
10. Ratanavaraporn J, Rangkupan R, Jeeratawatchai H, Influences of physical and chemical crosslinking techniques on elecrospun type A and B gelatin fiber mats: Int J Biol Macromol, 2010; 47; 431-38
11. Klangjorhor J, Nimkingratana P, Settakorn J, Hyaluronan production and chondrogenic properties of primary human chondrocyte on gelatin based hematostatic spongostan scaffold: J Orthop Surg Res, 2012; 7; 40
12. Anders JO, Mellenhauer J, Beberhold A, A gelatin-based haemostyptic spongostan as a possible three-dimensional scaffold for a chondrocyte matrix? An experimental study with bovine chondrocytes: J Bone Joint Surg Br, 2009; 91; 409-16
13. Palma VC, Magro-Filho O, de Oliveria JA, Bone reformation and implant integration following maxillary sinus membrane elevation: An experimental study in primates: Clin Implant Dent Relat Res, 2006; 8; 11-24
14. Lundgren S, Andersson S, Gualini F, Sennerby L, Bone reformation with sinus membrane elevation: A new surgical technique for maxillary sinus floor augmentation: Clin Implant Dent Relat Res, 2004; 6; 165-73
15. Whitehead AL, Julious SA, Cooper CL, Campbell MJ, Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable: Stat Methods Med Res, 2016; 25; 1057-73
16. Moher D, Schulz KF, Altman DG, The CONSORT statement: Revised recommendations for improving the quality of reports of parallel-group randomised trials: Lancet, 2001; 357; 1191-94
17. Albrektsson T, Zarb G, Worthington P, Eriksson AR, The long-term efficacy of currently used dental implants: A review and proposed criteria of success: Int J Oral Maxillofac Implants, 1986; 1; 11-25
18. Gorla LF, Spin-Neto R, Boos FB, Use of autogenous bone and beta-tricalcium phosphate in maxillary sinus lifting: A prospective, randomized, volumetric computed tomography study: Int J Oral Maxillofac Surg, 2015; 44; 1486-91
19. Kawakami S, Lang NP, Ferri M, Influence of the height of the antrostomy in sinus floor elevation assessment by cone-beam computed tomography – a randomized clinical trial: Int J Oral Maxillofac Implants, 2019; 34; 223-32
20. Stefanski S, Svensson B, Thor A, Implant survival following sinus membrane elevation without grafting and immediate implant installation with a one-stage technique: An up-to-40-month evaluation: Clin Oral Implants Res, 2017; 28; 1354-59
21. Felice P, Scarano A, Pistilli R, A comparison of two techniques to augment maxillary sinuses using the lateral window approach: Rigid synthetic resorbable barriers versus anorganic bovine bone. Five-month post-loading clinical and histological results of a pilot randomised controlled clinical trial: Eur J Oral Implantol, 2009; 2; 293-306
22. Moraschini V, Uzeda MG, Sartoretto SC, Calasans-Maia MD, Maxillary sinus floor elevation with simultaneous implant placement without grafting materials: A systematic review and meta-analysis: Int J Oral Maxillofac Surg, 2017; 46; 636-47
23. Meloni SM, Jovanovic SA, Pisano M, Sinus lift grafting with anorganic bovine bone vs 50% autologous bone mixed with 50% anorganic bovine bone: 2 years after loading results from a randomised controlled trial: Eur J Oral Implantol, 2017; 10; 425-32
24. Ocak H, Kutuk N, Demetoglu U, Comparison of bovine bone-autogenic bone mixture versus platelet-rich fibrin for maxillary sinus grafting: Histologic and histomorphologic study: J Oral Implantol, 2017; 43; 194-201
25. He L, Chang X, Liu Y, Sinus floor elevation using osteotome technique without grafting materials: A 2-year retrospective study: Clin Oral Implants Res, 2013; 24(Suppl A100); 63-67
26. Pérez-Martínez S, Martorell-Calatayud L, Peñarrocha-Oltra D, Indirect sinus lift without bone graft material: Systematic review and meta-analysis: J Clin Exp Dent, 2015; 7; e316-19
27. Ahn JJ, Cho SA, Byrne G, New bone formation following sinus membrane elevation without bone grafting: Histologic findings in humans: Int J Oral Maxillofac Implants, 2011; 26; 83-90
28. Tabata Y, Biomaterial technology for tissue engineering applications: J R Soc Interface, 2009; 6; S311-24
29. Ponticiello MS, Schinagl RM, Kadiyala S, Barry FP, Gelatin-based resorbable sponge as a carrier matrix for human mesenchymal stem cells in cartilage regeneration therapy: J Biomed Mater Res, 2000; 52; 246-55
30. Umanjec-Korac S, Wu G, Hassan B, A retrospective analysis of the resorption rate of deproteinized bovine bone as maxillary sinus graft material on cone beam computed tomography: Clin Oral Implants Res, 2014; 25; 781-85
31. Fornell J, Johansson LÅ, Bolin A, Flapless, CBCT-guided osteotome sinus floor elevation with simultaneous implant installation I: Radiographic examination and surgical technique. A prospective 1-year follow-up: Clin Oral Implants Res, 2012; 23; 28-34
32. Baciut M, Hedesiu M, Bran S, Pre- and postoperative assessment of sinus grafting procedures using cone-beam computed tomography compared with panoramic radiographs: Clin Oral Implants Res, 2013; 24; 512-16
33. Mazzocco F, Lops D, Gobbato L, Three-dimensional volume change of grafted bone in the maxillary sinus: Int J Oral Maxillofac Implants, 2014; 29; 178-84
34. Jensen T, Schou S, Svendsen PA, Volumetric changes of the graft after maxillary sinus floor augmentation with Bio-Oss and autogenous bone in different ratios: A radiographic study in minipigs: Clin Oral Implants Res, 2012; 23; 902-10
35. Yanfeng T, Jianlin C, Yunbiao ZExperimental study on accelerated healing of jaw fracture using gelatin sponge compound growth factor: Hua Xi Kou Qiang Yi Xue Za Zhi, 2017; 35; 506-9 [in Chinese]
Figures
Figure 1. The gelatin sponge was cut into small chunks and mixed with bovine bone, and then mixed with saline or local blood. Around the window area, only bovine bone particles were used.Figure 2. Digital (3-dimensional) reconstruction technique was carried out through selecting the grafting volume, while the artificial reconstruction was also calculated according to the threshold values. In this study, the threshold values were selected based on gray values for the native bone, grafting bone, sinus cavity, and soft tissue, with analysis by Mimics software (version 16.0, Leuven, Belgium). This representative image is from a patient at 6 months after surgery. Tables
 Table 1. Patients and implants distribution in groups.
Table 1. Patients and implants distribution in groups.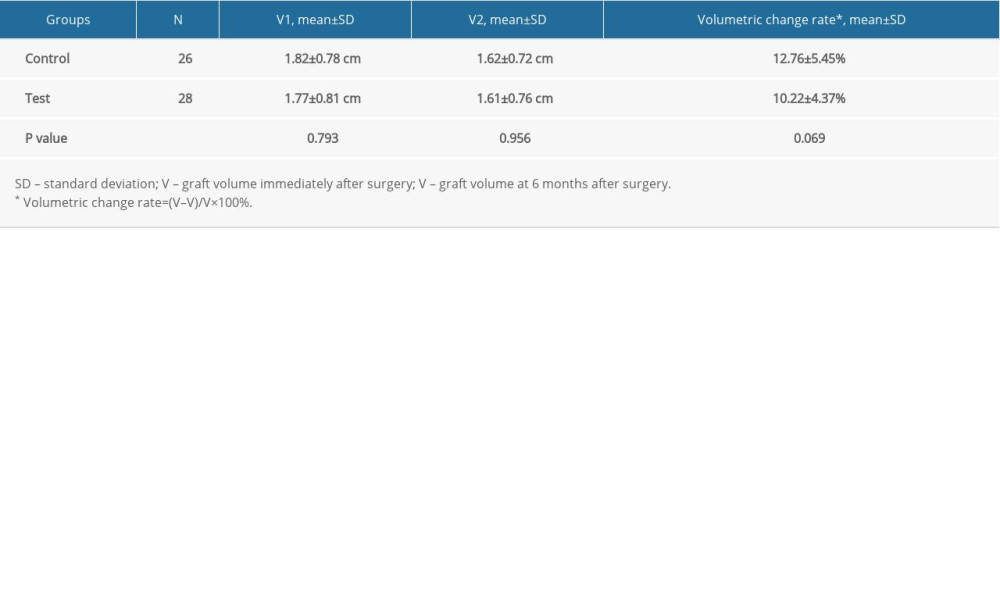 Table 2. Graft volumes and volumetric change rates for both groups.
Table 2. Graft volumes and volumetric change rates for both groups.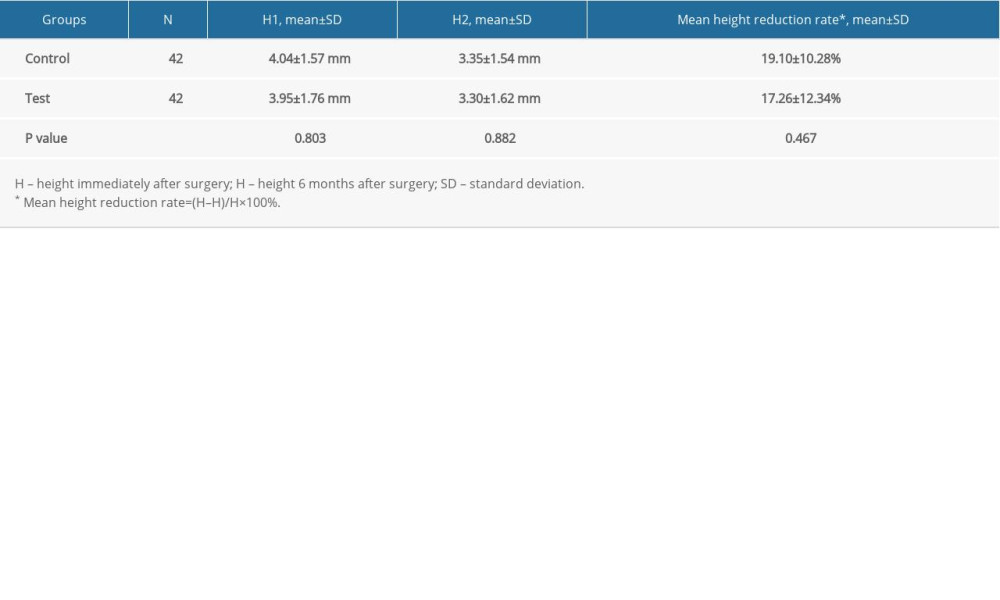 Table 3. Bone height reduction rate between the tip of implant and sinus membrane.Table 1. Patients and implants distribution in groups.Table 2. Graft volumes and volumetric change rates for both groups.Table 3. Bone height reduction rate between the tip of implant and sinus membrane.
Table 3. Bone height reduction rate between the tip of implant and sinus membrane.Table 1. Patients and implants distribution in groups.Table 2. Graft volumes and volumetric change rates for both groups.Table 3. Bone height reduction rate between the tip of implant and sinus membrane. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387