30 September 2021: Clinical Research
Prospective Study on the Postoperative Use of Levosimendan After Conventional Heart Valve Replacement
Wei Sheng1ABCDEF*, Hui Qiao1ABCDEF, Zhaozhuo Niu1BCE, Tianyi Wang1BCE, Haoyou Li1CDE, Wenfeng Zhang1CDE, Jiantao Wu1CDE, Xiao Lv1ADEFDOI: 10.12659/MSM.932001
Med Sci Monit 2021; 27:e932001






Abstract
BACKGROUND: The aim of this study was to explore the effect of levosimendan in patients after heart valve replacement and its influence on postoperative recovery.
MATERIAL AND METHODS: This prospective study included 185 patients with valvular diseases undergoing conventional valve replacement. Patients were divided into 2 groups using a random number table before surgery. Patients in the levosimendan group were administrated levosimendan intravenous infusion immediately after entering the Intensive Care Unit (ICU). The left ventricular ejection fraction (LVEF), cardiac output, and heart failure-related index, such as B-type natriuretic peptide (BNP) level, were recorded at 1, 3, and 7 days after surgery. The dosage and administration time of dopamine and epinephrine, mechanical ventilation time, ICU length of stay, and postoperative adverse events were recorded.
RESULTS: Cardiac output and LVEF of patients in the levosimendan group were significantly higher than those in the control group at different time points (P<0.05), and BNP level was lower than that of the control group (P<0.0001). Dosage and administration time of dopamine and epinephrine in the levosimendan group were lower than those of the control group (P<0.0001, P<0.0001, respectively). ICU length of stay and total incidence of postoperative adverse events were lower than those of the control group (P<0.0001, P=0.002, respectively).
CONCLUSIONS: Levosimendan administration immediately after heart valve replacement effectively improved the heart function of patients, reduced administration of vasoactive drugs, shortened length of ICU stay, reduced incidence of postoperative adverse events, and promoted recovery of patients after surgery.
Keywords: Cardiac Output, Heart Valve Diseases, Simendan, Cardiotonic Agents, Female, Heart Valve Prosthesis Implantation, Heart Valves, Humans, Length of Stay, Postoperative Care, Postoperative Complications, Prospective Studies
Background
Despite great advances in cardioprotective strategies, surgical techniques and skills, cardiopulmonary bypass techniques, and postoperative management, myocardial injury is still a common complication following cardiopulmonary bypass surgery, inducing myocardial dysfunction and circulatory impairment [1], arrhythmia, myocardial energy metabolism disturbance, microcirculation disorder, and low cardiac output syndrome (LCOS) [2,3], thus severely threatening the postoperative recovery of patients. The therapeutic management of LCOS includes hemodynamic support with inotropic agents, vasopressors, and circulatory assist devices. Catecholamine vasoactive drugs are the most commonly used drugs after cardiac surgery, which can effectively enhance myocardial contractility of patients; however, at the same time, they lead to increased myocardial oxygen consumption, which results in an increase in associated complications. Levosimendan, as a new calcium sensitizer, can significantly improve cardiac function by increasing myocardial contractility and dilating blood vessels, and this effect of improving cardiac contractility does not lead to increased myocardial oxygen consumption and arrhythmia. It has recently been suggested that levosimendan can effectively improve cardiac function and long-term prognosis in patients with severe heart diseases during the perioperative period [4,5]. In this study, we prospectively observed the effect of the immediate administration of levosimendan on postoperative cardiac function and postoperative echocardiographic and hemodynamic indexes in patients undergoing conventional valve replacement.
Material and Methods
STATISTICAL ANALYSIS:
Statistical analysis was carried out using SPSS version 19.0. Measurement data with a normal distribution were presented as mean±standard deviation, and data with non-normal distribution were presented as median and interquartile range. Enumeration data were presented as percentages. The
Results
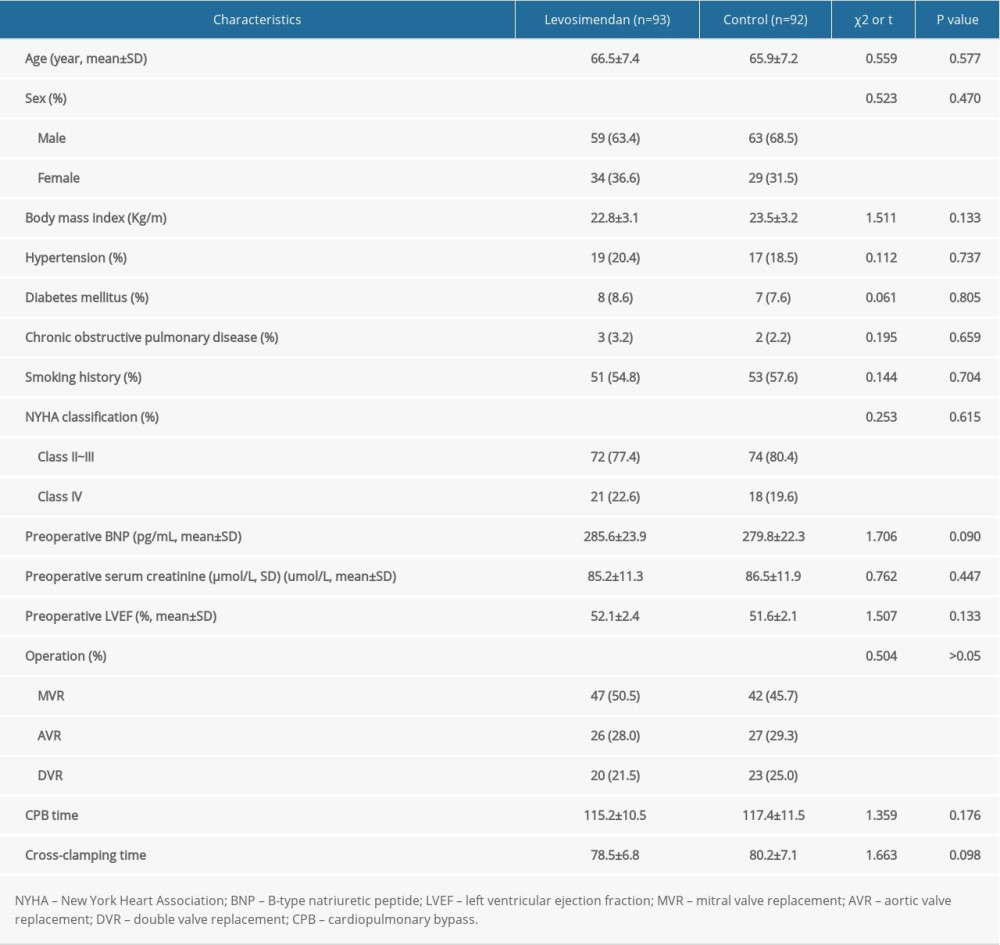
COMPARISON OF PREOPERATIVE AND INTRAOPERATIVE CLINICAL CHARACTERISTICS BETWEEN THE 2 GROUPS:
A total of 200 patients were initially enrolled, of which 9 patients did not meet the inclusion criteria, 5 patients refused to participate in the trial, and 1 patient withdrew for other reasons. Finally, 185 patients were enrolled. There were no statistically significant differences in age, sex, body mass index, smoking history, diabetes mellitus, hypertension, chronic obstructive pulmonary disease, serum creatinine, preoperative NYHA classification, preoperative BNP level, LVEF, types of surgical procedure, cardiopulmonary bypass time, and aortic cross-clamping time between the 2 groups (Table 1).
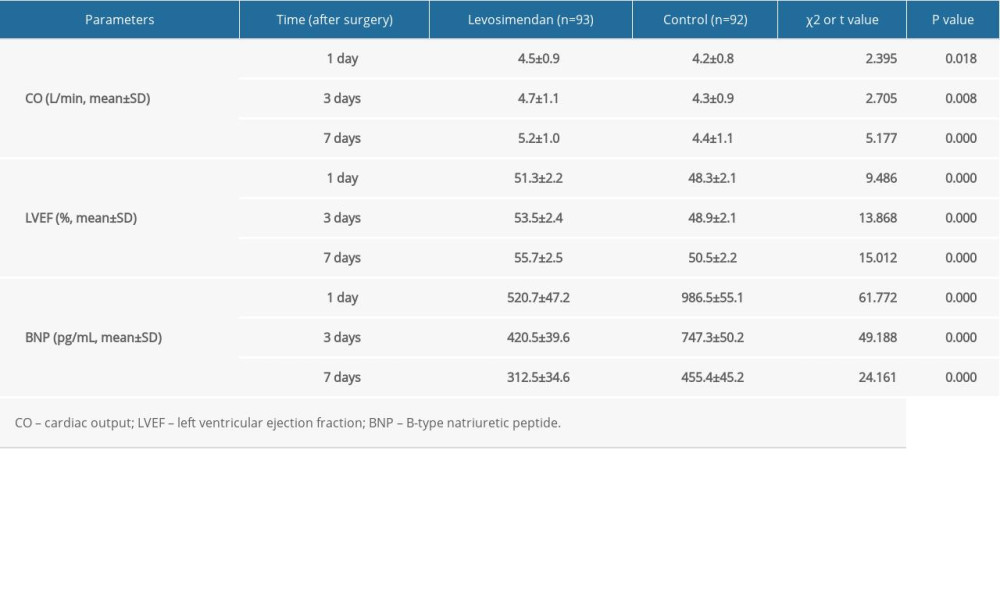
COMPARISON OF CARDIAC FUNCTION AFTER SURGERY BETWEEN THE 2 GROUPS:
The cardiac output and LVEF of the levosimendan group at 1, 3, and 7 days after surgery were significantly higher than those of the control group (P<0.05). The levels of BNP in the levosimendan group were significantly lower than that of the control group at 1, 3, and 7 days after surgery (P<0.05) (Table 2).
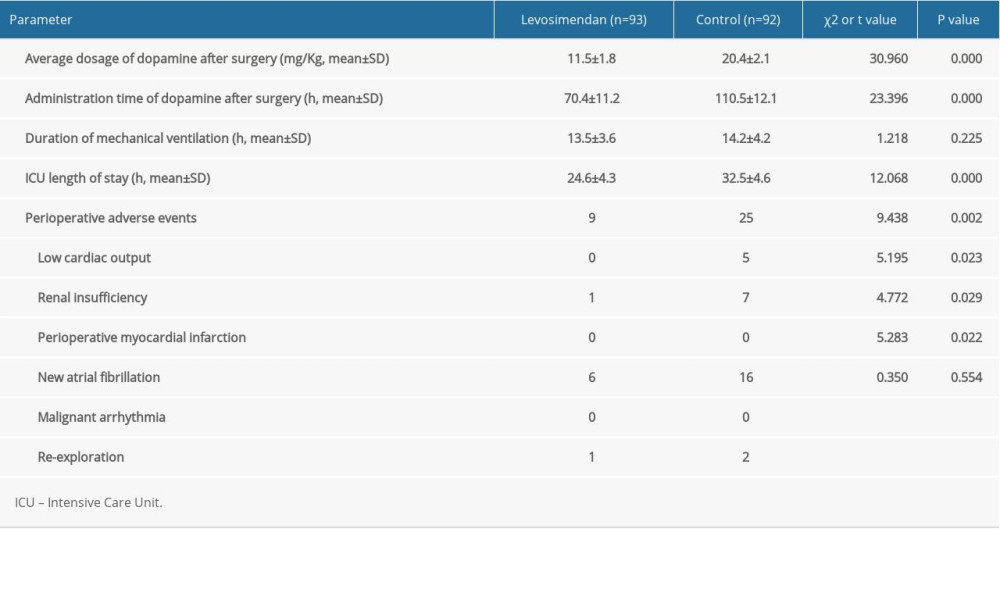
COMPARISON OF OTHER PERIOPERATIVE PARAMETERS BETWEEN THE 2 GROUPS:
The dosage and administration time of dopamine in the levosimendan group were significantly lower than those in the control group (P<0.05). The hemodynamics were stable in the levosimendan group after surgery, and without epinephrine infusion. In the control group, some patients needed intravenous infusion of epinephrine, and the dosage of epinephrine (non-normal distribution data) was 31.8 (0, 48.5) g/kg. The ICU length of stay in the levosimendan group was shorter than that of the control group (P<0.05). There was no significant difference in mechanical ventilation time between the 2 groups, as shown in Table 3. The incidences of LCOS, renal insufficiency, new atrial fibrillation, and total adverse events in the levosimendan group were significantly lower than those in the control group (P<0.05).
Discussion
Ischemia-reperfusion injury, additional heparin-induced thrombocytopenia of cardiopulmonary bypass, direct surgical injuries such as myocardial incision, and perioperative myocardial infarction in patients undergoing cardiac surgery inevitably induce different degrees of myocardial injury, and even heart failure [6,7]. Positive inotropic drugs are the most important drugs to improve cardiac function in patients after cardiac surgery. However, most positive inotropic drugs often give rise to adverse effects, such as increasing myocardial contractility and myocardial oxygen consumption, leading to local myocardial ischemia and subsequent myocardial damage and the incidence of arrhythmia increases [8,9]. As a new type of positive inotropic drug, levosimendan induces calcium to bond with cardiac troponin C and increases the sensitivity of myofilament to calcium ions to increase myocardial contraction. Its binding is calcium-dependent but it does not increase the concentration of calcium ions in the cytoplasm, so it does not increase myocardial oxygen consumption [10,11]. The mechanism of action of levosimendan also includes the activation of adenosine triphosphate-sensitive potassium channels, which results in improved myocardial contractility, vasodilation, and cardioprotection. Results of recent clinical trials have shown that the administration of the calcium sensitizer levosimendan after cardiac surgery can improve cardiac and renal functions of patients [12–14]. However, these benefits were greatest for the cardiac surgery patients with severe valvular disease or patients with severe coronary heart disease with diminished LVEF. A number of meta-analyses have shown that levosimendan can significantly improve general and pulmonary hemodynamics in patients with perioperative heart failure [15–17]. Zangrillo et al [18] demonstrated that levosimendan can improve kidney function in patients with mitral valve surgery and chronic kidney disease who develop perioperative myocardial dysfunction. Khaled et al [19] showed that levosimendan significantly improved hemodynamic parameters and had no effect on mortality in patients with left ventricular dysfunction undergoing cardiac surgery, compared with conventional inotropic agents. Weber et al [20] reported a meta-analysis of the beneficial effects of prophylactic levosimendan administration in patients with severe impairment of left ventricular function undergoing heart surgery. However, there have been few studies of the benefits of levosimendan in patients without perioperative heart failure. In the present prospective study, we explored the effect of levosimendan on patients undergoing conventional heart valve replacement. In our study, levosimendan was administrated immediately when patients returned to the ICU after heart valve replacement. We confirmed that the heart function indexes at 1, 3, and 7 days after surgery in the levosimendan group were better than those of the control group. We showed that levosimendan significantly improved heart function in patients undergoing conventional cardiac valve replacement. Our results also demonstrated that the duration of ICU stay was significantly shortened in the levosimendan group, indicating that the administration of levosimendan enhanced the recovery of patients undergoing conventional cardiac valve replacement.
Catecholamine vasoactive drugs can enhance myocardial contraction by increasing myocardial oxygen consumption and can simultaneously increase heart rate and increase the incidence of arrhythmia [21,22]. Therefore, they will inevitably lead to an increase in morbidity and mortality [23]. Zatloukalová et al [24] showed that 100 mg/kg of isoprenaline by subcutaneous injection in a catecholamine model of acute myocardial infarction increased mortality, myocardial calcium overload, histological impairment, and peripheral hemodynamic disturbances 24 h after administration and could lead to late myocardial impairment and ventricular fibrillation due to myocardial calcium overload. In the present study, we showed that levosimendan administration significantly decreased the dosage and duration of catecholamine dopamine infusion, compared with the control group, and no epinephrine was administrated in the levosimendan group. The results also demonstrated that the incidence of postoperative atrial fibrillation was significantly lower in the levosimendan group, and no malignant arrhythmias occurred in those patients, which showed that levosimendan administration reduced the incidence of arrhythmias and did not increase the incidence of malignant arrhythmias, while improving the cardiac function of patients after routine heart valve replacement. Reduction in the administration of other positive inotropic drugs, such as dopamine and epinephrine, also reduced the occurrence of related adverse events. This finding is similar to that of Abacilar et al [25] who found that the occurrence of atrial fibrillation was significantly lower in the levosimendan group (12% vs 36%), and the duration of atrial fibrillation in the levosimendan group was significantly shorter compared with that of the control group in patients with poor left ventricle function after coronary artery bypass graft surgery. In our study, the results also demonstrated that the incidence of renal insufficiency was significantly lower in the levosimendan group, which was consistent with the results of many studies that showed levosimendan can improve kidney function in cardiac surgery. Guerrero Orriach et al [26] demonstrated that the incidence of kidney failure was lower with the postoperative administration of levosimendan than with the administration of beta-agonists in patients undergoing cardiac surgery with LCOS. However, some studies have drawn different conclusions. For instance, van Diepen et al [27] demonstrated that levosimendan was associated with lower 90-day mortality and LCOS in patients undergoing isolated coronary artery bypass graft surgery but not in patients undergoing isolated valve or combined coronary artery bypass graft surgery/valve procedures. Furthermore, Mehta et al [28] demonstrated that prophylactic levosimendan did not affect the rate of the short-term composite endpoint of death, renal replacement therapy, perioperative myocardial infarction, or use of a mechanical cardiac assist device, and was lower than the rate with placebo among patients with a reduced LVEF who were undergoing cardiac surgery with cardiopulmonary bypass. Landoni et al [29] demonstrated that, compared with placebo, low-dose levosimendan in addition to standard care did not result in lower 30-day mortality in patients who required perioperative hemodynamic support after cardiac surgery. Different trials had heterogeneous results, which may be related to the administration dose and timing of levosimendan, different causes of cardiac dysfunction, and different choice of endpoint; therefore, to confirm the efficacy of levosimendan in cardiac surgery, more detailed and adequately powered clinical trials are needed.
There are some limitations in our study that should be emphasized. First, the patient population enrolled in this study was in a single institution and relatively small; therefore, the conclusions might not be applicable to other centers. Second, additional hemodynamic parameters, such as central venous pressure, mean arterial pressure, systemic vascular resistance, and pulmonary arterial wedge pressure, were not analyzed in this study. Finally, our study presented only short-term outcomes, and median and long-term follow-up might be needed to further assess the effect of levosimendan.
Conclusions
In conclusion, levosimendan administration immediately after surgery effectively improved heart function and protected renal function of patients after heart valve replacement. It reduced the postoperative administration of catecholamines, such as dopamine and epinephrine, reduced the occurrence of postoperative adverse events, shortened the duration of ICU stay, and enhanced the recovery of patients after cardiac valve replacement. The curative effect of levosimendan was better than that of traditional positive inotropic drug treatment with dopamine and epinephrine infusion. Levosimendan was safe and effective to administer for 24 h of continuous infusion after surgery for patients undergoing cardiac valve replacement.
References
1. Zhou RH, Yu H, Yin XR, Effect of intralipid postconditioning on myocardial injury in patients undergoing valve replacement surgery: A randomised controlled trial: Heart, 2017; 103(14); 1122-27
2. Sunny , Yunus M, Karim HM, Comparison of levosimendan, milrinone and dobutamine in treating low cardiac output syndrome following valve replacement surgeries with cardiopulmonary bypass: J Clin Diagn Res, 2016; 10(12); UC05-8
3. Mubashir T, Balogh J, Chaudhry R, Transcatheter and surgical aortic valve replacement outcomes for patients with chronic heart failure: J Cardiothorac Vasc Anesth, 2021; 35(3); 888-95
4. Desai PM, Sarkar MS, Umbarkar SR, Prophylactic preoperative levosimendan for off-pump coronary artery bypass grafting in patients with left ventricular dysfunction: Single-centered randomized prospective study: Ann Card Anaesth, 2018; 21(2); 123-28
5. Jiménez-Rivera JJ, Álvarez-Castillo A, Ferrer-Rodríguez J, Preconditioning with levosimendan reduces postoperative low cardiac output in moderate-severe systolic dysfunction patients who will undergo elective coronary artery bypass graft surgery: A cost-effective strategy: J Cardiothorac Surg, 2020; 15(1); 108
6. Cao Z, Shen R, Zhang X, Effects of remote ischemic preconditioning on acute myocardial injury in patients undergoing valve replacement: Ir J Med Sci, 2017; 186(4); 889-93
7. De Hert S, Moerman A, Myocardial injury and protection related to cardiopulmonary bypass: Best Pract Res Clin Anaesthesiol, 2015; 29(2); 137-49
8. Yamazaki Y, Oba K, Matsui Y, Vasoactive-inotropic score as a predictor of morbidity and mortality in adults after cardiac surgery with cardiopulmonary bypass: J Anesth, 2018; 32(2); 167-73
9. Garcia RU, Walters HL, Delius RE, Vasoactive inotropic score (VIS) as biomarker of short-term outcomes in adolescents after cardiothoracic surgery: Pediatr Cardiol, 2016; 37(2); 271-77
10. Kandasamy A, Simon HA, Murthy P, Comparison of levosimendan versus dobutamine in patients with moderate to severe left ventricular dysfunction undergoing off-pump coronary artery bypass grafting: A randomized prospective study: Ann Card Anaesth, 2017; 20(2); 200-6
11. Putzu A, Clivio S, Belletti A, Perioperative levosimendan in cardiac surgery: A systematic review with meta-analysis and trial sequential analysis: Int J Cardiol, 2018; 251; 22-31
12. Atalay H, Temizturk Z, Altinsoy HB, Levosimendan use increases cardiac performance after coronary artery bypass grafting in end-stage renal disease patients: Heart Surg Forum, 2016; 19(5); E230-36
13. Anastasiadis K, Antonitsis P, Vranis K, Effectiveness of prophylactic levosimendan in patients with impaired left ventricular function undergoing coronary artery bypass grafting: A randomized pilot study: Interact Cardiovasc Thorac Surg, 2016; 23(5); 740-47
14. Zhou C, Gong J, Chen D, Levosimendan for prevention of acute kidney injury after cardiac surgery: A meta-analysis of randomized controlled trials: Am J Kidney Dis, 2016; 67(3); 408-16
15. Qiang H, Luo X, Huo JH, Perioperative use of levosimendan improves clinical outcomes in patients after cardiac surgery: A systematic review and meta-analysis: J Cardiovasc Pharmacol, 2018; 72(1); 11-18
16. Lee CT, Lin YC, Yeh YC, Effects of levosimendan for perioperative cardiovascular dysfunction in patients receiving cardiac surgery: A meta-analysis with trial sequential analysis: Intensive Care Med, 2017; 43(12); 1929-30
17. Chen QH, Zheng RQ, Lin H, Effect of levosimendan on prognosis in adult patients undergoing cardiac surgery: A meta-analysis of randomized controlled trials: Crit Care, 2017; 21(1); 253
18. Zangrillo A, Alvaro G, Belletti A, Effect of levosimendan on renal outcome in cardiac surgery patients with chronic kidney disease and perioperative cardiovascular dysfunction: A substudy of a multicenter randomized trial: J Cardiothorac Vasc Anesth, 2018; 32(5); 2152-59
19. Khaled M, Almogy AN, Shehata M, Effect of levosimendan compared to conventional inotropic agents on hemodynamics and outcome in patient with poor LV function undergoing cardiac surgery: Open Access Maced J Med Sci, 2019; 7(19); 3205-10
20. Weber C, Esser M, Eghbalzadeh K, Levosimendan reduces mortality and low cardiac output syndrome in cardiac surgery: Thorac Cardiovasc Surg, 2020; 68(5); 401-9
21. Abacilar AF, Dogan OF, Levosimendan use decreases atrial fibrillation in patients after coronary artery bypass grafting: A pilot study: Heart Surg Forum, 2013; 16(5); E287-94
22. Suita K, Fujita T, Cai W, Vidarabine, an anti-herpesvirus agent, prevents catecholamine-induced arrhythmias without adverse effect on heart function in mice: Pflugers Arch, 2018; 470(6); 923-35
23. Cholley B, Caruba T, Grosjean S, Effect of levosimendan on low cardiac output syndrome in patients with low ejection fraction undergoing coronary artery bypass grafting with cardiopulmonary bypass: the LICORN Randomized Clinical Trial: JAMA, 2017; 318(6); 548-56
24. Zatloukalová L, Filipský T, Mladěnka P, Dexrazoxane provided moderate protection in a catecholamine model of severe cardiotoxicity: Can J Physiol Pharmacol, 2012; 90(4); 473-484
25. Abacilar AF, Dogan OF, Levosimendan use decreases atrial fibrillation in patients after coronary artery bypass grafting: A pilot study: Heart Surg Forum, 2013; 16(5); E287-94
26. Guerrero Orriach JL, Navarro Arce I, Hernandez Rodriguez P, Preservation of renal function in cardiac surgery patients with low cardiac output syndrome: Levosimendan vs beta agonists: BMC Anesthesiol, 2019; 19(1); 212
27. van Diepen S, Mehta RH, Leimberger JD, Levosimendan in patients with reduced left ventricular function undergoing isolated coronary or valve surgery: J Thorac Cardiovasc Surg, 2020; 159(6); 2302-9.e6
28. Mehta RH, Leimberger JD, van Diepen S, Levosimendan in patients with left ventricular dysfunction undergoing cardiac surgery: N Engl J Med, 2017; 376(21); 2032-42
29. Landoni G, Lomivorotov VV, Alvaro G, Levosimendan for hemodynamic support after cardiac surgery: N Engl J Med, 2017; 376(21); 2021-31
In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387