01 October 2021: Clinical Research
Comparison of the Use of Magnetic Resonance Imaging of Partial Anterior Cruciate Ligament Tears Using Maximum Knee Flexion in the Lateral Decubitus Position with Routine Knee Positioning
Zijun Xu1ABCDEFG, Yichao Chen2ABCDEF, Jianghua Zhu3FG, Lin Zhang1FG, Peng Wu4AG*DOI: 10.12659/MSM.932228
Med Sci Monit 2021; 27:e932228






Abstract
BACKGROUND: This study assessed magnetic resonance imaging (MRI) of acute and chronic partial anterior cruciate ligament (ACL) tears using maximum knee flexion in the lateral decubitus position compared with routine knee positioning in 204 patients at a single center.
MATERIAL AND METHODS: Based on the time interval from injury to MRI examination, the 204 patients in this study were divided into 3 groups: subacute (6 weeks to 3 months), intermediate (3 months to 1 year), and chronic (>1 year). All patients received both routine MRI (MRI R) and maximum knee flexion in the lateral decubitus position MRI (MRI S) examination, followed by knee arthroscopy. Three radiologists blinded to patient groups evaluated the MRI scans and made a diagnosis. Results of knee arthroscopy were referenced as the criterion standard. The sensitivity and specificity of MRI R and MRI S groups were calculated and compared.
RESULTS: The MRI S diagnostic rate was comparable to that of knee arthroscopy. MRI S had significantly higher sensitivity than MRI R for partial ACL tears, especially in the intermediate group (P<0.01).
CONCLUSIONS: MRI of partial ACL tears using maximum knee flexion in the lateral decubitus position improved the diagnostic rate relative to routine MRI examination, particularly in patients in the intermediate group.
Keywords: Anterior Cruciate Ligament Injuries, Arthroscopy, Diagnosis, Magnetic Resonance Imaging, Anterior Cruciate Ligament, Female, Humans, Knee Joint, Patient Positioning, Posture, Reproducibility of Results, Sensitivity and Specificity, Time Factors, young adult
Background
Anterior cruciate ligament (ACL) tears occur most commonly in young and active individuals and can have negative long-term physical and psychological impacts [1].
To accurately diagnose an ACL tear, the clinician has to combine information from the patient’s history, clinical examination, and imaging [2]. As a noninvasive method, magnetic resonance imaging (MRI) is widely used in the diagnosis of bone and joint diseases [3]. For experienced assessors, the combination of patient history and clinical examination is often sufficient to diagnose an ACL tear [4]. However, pain and effusion in the acute stage may hinder detecting the injury during clinical examination [5]. Misdiagnosis is common, and an acute ACL injury is misdiagnosed as an uncomplicated knee sprain in half of the patients with the injury [5]. Repeated clinical examination or MRI in the subacute phase may therefore be necessary to rule out the injury. The diagnostic accuracy of MRI is comparable to that of the Lachman test [5]. For patients with suspected ACL tears, MRI holds value as an adjunct method when the clinical diagnosis is uncertain. Partial ACL tears make up 10%–28% of all ACL tears [4], but considerable controversy remains regarding the role of MRI in their diagnosis [6–9]. While an empty notch sign, a wavy ACL, bone contusion, and posterior horn of lateral meniscus tears suggest a complete ACL tear, a residual straight and tight ACL fiber seen in at least 1 image section is helpful to diagnose a partial ACL tear [10]. However, the ACL may not always be visualized [8,9,11,12], either for technical reasons or because it is ruptured and absent. Complete ACL tears can be easily diagnosed by clinical examination and an MRI [13], while the diagnosis of partial ACL tears is more difficult. In the acute stage of a partial ACL tear, hemorrhage, effusion, and edema from the knee joint or tear site could interfere with the magnetic resonance signals. Therefore, misdiagnosis often occurs [10]. It is even more difficult to diagnose a partial ACL tear at the chronic stage, when the partially ruptured ACL stump can be aggregated or adhered to adjacent normal ACL or bone, which further increases the difficulty of MRI diagnosis [6,7,10,14,15]. In such cases, special methods are needed for accurate diagnosis. Many strategies have been used to improve the visualization of the ACL, including sagittal and coronal oblique sequences and 3-dimensional volume imaging [14–17], but the sensitivity and specificity of MRI are still not high [1–3]. The persistence of an ACL tear can exacerbate the damage to the knee joint and nearby tissue and then affect the function and stability of knee joint [16]. To reduce the interference of tissue signal and improve the visualization of the ligament, optimizing both the patient’s position and the scanning method has attracted considerable attention. According to a previous study [18], MRI with the patient in the prone position allowed a maximum knee flexion that assisted in the diagnosis and treatment of partial ACL ruptures. In our study, we found that maximum knee flexion occurred in the lateral decubitus position. With this position, the joint effusion and hematocele could be squeezed away from the ligament tear site, which reduced the factors interfering with diagnosis. In addition, after knee flexion, the visualization of the ACL attachment end was stronger. We suggest that the advantages of this special position would be effective in diagnosing partial ACL tear. Therefore, we aimed to evaluate the use of MRI of partial ACL tears using maximum knee flexion in the lateral decubitus position compared with routine knee positioning in 204 patients at a single center.
Material and Methods
CONSENT TO PUBLISH:
Informed consent was obtained from all participants included in the study regarding publication. All procedures in this study were approved by the Ethics Review Board of the hospital before the study began.
GROUPING OF PATIENTS:
A total of 398 patients from October 2016 to November 2018 were selected to participate in this study based on the following inclusion criteria: (1) clinical physical examination suggested a partial ACL tear, and (2) arthroscopy was indicated for reasons such as suspected meniscus injury or loose body. Exclusion criteria were (1) knee deformity or deformity caused by previous trauma; (2) an acute ACL tear (less than 6 weeks); (3) difficulty achieving the specific position needed for MRI examination; (4) refusal of arthroscopic surgery or MRI examination; and (5) complete ACL tear. A total of 194 patients were excluded from the study, and 204 knees of 204 patients (112 males and 92 females) were included. Our primary focus in this study was the diagnostic value of routine MRI and special posture MRI for partial ACL injury, so the associated meniscus injury, loose body, and collateral ligaments are not discussed here.
Of the 204 cases, 125 involved the right knee and 79 involved the left knee. The age of the patients ranged from 17 to 65 years, with an average of 42.1±9.6 years. Based on previous studies [14,15] and the time that had elapsed between the injury and the MRI examination, the patients were divided into 3 groups: 72 cases in the subacute group (6 weeks to 3 months after injury), 58 cases in the intermediate group (3 months to 1 year after injury), and 74 cases in the chronic group (more than 1 year after injury). Routine MRI (MRI R) and maximum knee flexion in the lateral decubitus position MRI (MRI S) were performed for each patient, and these images were evaluated by 3 senior diagnostic physicians blinded to the group allocation. Diagnoses made by at least 2 physicians were chosen as the final results. Arthroscopy examination results (criterion standard) were compared with MRI R and MRI S results to evaluate the sensitivity (the probability of positive detection in the criterion standard positive patients) and specificity (the probability of negative detection in the criterion standard negative patients) of different MRI examinations [10]. Auxiliary equipment included 3.0T postprocessing workstation, joint-specific flexible coil (commonly used for shoulder joint examination), a sandbag, and an angle ruler.
SCANNING METHODS OF THE KNEE:
For MRI R, the patient was placed in the supine position with the knee joint naturally straightened. The lower edge of the patella was located in the center of the knee coil, and the sandbag was pressed to fix the knee joint. For MRI S, the patient moved the joint properly before examination and then lay on their side with the knee joint at the maximum flexion angle under the guidance of doctors (Figure 1A). A wide cloth strip was placed on the dorsum of the foot and the other end of the cloth strip was pulled with both hands (Figure 2A). The upper and lower ends of the affected knee joint were wrapped with special flexible coils and fixed with sandbags.
SCANNING SEQUENCE:
For MRI R, all patients were scanned using a Magnetom Verio 3.0 T MRI imager. Imaging parameters included axial T1WI (TR 586 ms, TE 17 ms, slice thickness 5 mm, slice spacing 0.5 mm, FOV 180×180 mm), coronal PDWI/FS (TR 3000 ms, TE 33.0 ms, thickness 3 mm, spacing 0.3 mm), sagittal PDWI (TR 3000 ms, TE 33.0 ms, thickness 3 mm, spacing 0.3 mm), T2WI/FS (TR 3500 ms, TE 98 ms, thickness 3 mm, spacing 0.3 mm; FOV 180×180 mm).
For MRI S, the parameters were sagittal PDWI (TR 3000 ms, TE 33.0 ms, slice thickness 3 mm, slice distance 0.3 mm). The oblique coronal position was parallel to the ACL, T2WI/FS (TR 3500 ms, TE 98 ms, thickness 3 mm, spacing 0.3 mm).
STATISTICAL METHODS:
SPSS 19.0 statistical software was used. Chi-square test and nonparametric Wilcoxon rank sum test were used for analysis. With the results of arthroscopy as the criterion standard, the sensitivity and specificity of the 2 examination methods for the diagnosis of partial ACL tear (MRI R and MRI S) were compared (Tables 1–4). Statistically significant differences were defined by P<0.05.
Results
The results of the MRI S and MRI R compared with arthroscopy are presented in Tables 1 and 2. Among the 204 patients, a partial ACL tear was detected by arthroscopy in 86 cases (42.2%), MRI R in 55 cases (27.0%), and MRI S in 74 cases (36.3%). The positive detection rate was significantly higher with MRI S than MRI R (chi-square test,
A comparison of the sensitivity and specificity of different MRI examination methods is presented in Table 3. The sensitivity and specificity of MRI R were 48.84% and 88.98%, respectively, and the sensitivity and specificity of MRI S were 80.29% and 95.76%, respectively. MRI S had a significantly higher sensitivity (chi-square test,
In the intermediate group, MRI S had a significantly higher sensitivity than MRI R (chi-square test,
Discussion
Our study showed that the sensitivity of routine MRI in diagnosing partial ACL tears was 48.84% (Table 3). According to previous studies, the diagnostic rate of partial ACL tears is rather low, with the sensitivity being about 40% [9,12,17]. Our study showed similar results. Possible explanations include (1) difficulty in observing the full length of the ACL in the same or several layers by routine examination; (2) lack of obvious direct signs of changes in ligament morphology and MRI signal; and (3) interference due to hemorrhage and effusion from joint or tear site. Direct signs of ligament morphological changes and indirect signs such as knee edema, posterior cruciate ligament flexion changes, and bone contusion are often used as the basis for the diagnosis of an ACL tear [16]. However, in our study, 12 patients had no twisting of the posterior cruciate ligament, 24 patients had minor edema of the joint, and 7 patients had no edema, suggesting that indirect signs were insufficient for the diagnosis of a partial ACL tear. To improve the visualization of the morphological changes of the ACL, some researchers display the full length of the ACL on oblique coronal images in parallel with ACL scanning and achieve a good display effect [9,13,19]. However, in our study, we found that joint effusion or hemorrhage near the ligament tear site interfered with the diagnosis of the tear site in 62 of the 204 cases (30.4%). Therefore, we designed a special position for patients to obtain maximum flexion of the knee in the lateral decubitus position (Figures 1, 2). In this case, the joint effusion or hemorrhage could be squeezed away from the ligament tear site, thereby reducing the factors that interfered with the diagnosis. In our study, disruptive factors were eliminated in 60 of 62 patients (96.8%) after additional special postural examinations (Figure 2B, 2C). There was no statistical difference in the diagnostic rate of a partial ACL tear between arthroscopic examination and MRI S. The sensitivity in the MRI S group was 80.29%, which was significantly higher than that of the MRI R group, which was 48.84% (
The optimization of both the body position and the scanning method is a precondition of obtaining high-quality images [20]. There are many MRI methods for ACL internationally. Arfanakis et al [21] used diffusion sequence to evaluate the value of ligament tear. Breitenseher and Mayerhoefer [22] used volume scans to reconstruct images to observe the morphological changes of ACL tears. Most of their methods were based on optimizing the scanning technology because the applicable data for scanning based on changes in body position are rare. Currently, the study of posture optimization is mostly focused on investigating knee joint function. However, MRI with the knee flexed at a certain angle has been reported to permit better visualization of the ACL. These studies examined MRI while the knee was positioned at a 30° angle and compared the results with imaging done during full extension of the knee joint, and the results indicated a better diagnostic rate of the ACL tear when the flexed position was used [23,24].
Burak et al [18] and Muhle et al [25] described why MRI with knee flexion enabled better visualization of ACL lesions. They found that as knee flexion increased, the femoral adhesion site of the ACL had a more horizontal position and the anteromedial bundle was also tightened. With the increased flexion angle, the ACL moved away from the intercondylar roof at the femoral adhesion site, thus the tear could be better visualized, especially in sagittal MRI scans [18,25]. In addition, with knee flexion, the ACL shape was cylindrical and tears could be better detected [18,25]. Total ACL tears were detected with a sensitivity of 83% at full extension of the knee, 83% at 30° knee flexion, and 93% at 55° knee flexion; however, in partial ACL tears, sensitivity was 50% with full extension of the knee, 63% with 30° knee flexion, and 63% with 55° knee flexion [18,25]. These findings led to the question of whether an increase in the flexion angle would improve the visualization of a partial ACL tear. Thus, we decided to maximize the flexion angle to get better visualization of the ACL. In our study, we found the sensitivity of MRI S was 80.2% at 30° knee flexion (Table 3), which was an excellent result for detecting partial ACL injury.
In our study, patients flexed their knees only to the extent that they could to avoid unnecessary harm and to improve the success rate of the examination. After knee flexion, the visualization of the ACL attachment end was stronger (Figures 1, 2). Although the flexion angle in the subacute ACL tear group was less than that of the intermediate and chronic groups, the maximum knee flexion in the lateral decubitus position MRI scans of the patients in the modified groups could be used for diagnosis. However, the diagnostic sensitivity of subacute and chronic groups was 34.28%, lower than that of the intermediate group (94.44%) and the chronic group (44.68%). This may be related to the slight flexion angle that patients could achieve. Among acute-stage patients, severe joint edema and pain made it difficult to attain the appropriate position, so these patients were not included in this study.
Interestingly, we found no significant difference between methods with regard to diagnosing a complete ACL tear (Table 5), suggesting that routine MRI examination is sufficient for the diagnosis of a complete ACL tear.
The limitation of our study is that although we tried to divide the patients into 4 groups according to the course of disease, 32 patients in the acute group could not achieve knee flexion due to severe joint edema and pain. Thus, we assumed that overbending the injured knee would worsen the medical experience of acute-stage patients and could aggravate their injury. For acute ACL tears, we recommend that patients receive routine MRI examination. Also, due to the small sample size and the use of a single center, some study bias may have occurred. We hope to build upon current results in a future study.
Conclusions
This study showed that MRI of partial ACL tears at different stages using maximum knee flexion in the lateral decubitus position improved the diagnostic rate compared with routine MRI examination, particularly for partial ACL tears at the intermediate stage.
Figures
 Figure 1. (A) The sketch of maximum flexion of knee joint with maximum flexibility of 150°. (B) Image from a 37-year-old man, 13 months after injury. Only routine position magnetic resonance imaging (MRI) scans were provided. The display angle of anterior cruciate ligament attachment points was poor. Sagittal and coronal scanning images both had effusion disturbing the diagnosis. (C) Image from a 45-year-old man. Only routine position MRI scans were provided. The joint effusion or hemorrhage near the ligament tear site interfered with the diagnosis.
Figure 1. (A) The sketch of maximum flexion of knee joint with maximum flexibility of 150°. (B) Image from a 37-year-old man, 13 months after injury. Only routine position magnetic resonance imaging (MRI) scans were provided. The display angle of anterior cruciate ligament attachment points was poor. Sagittal and coronal scanning images both had effusion disturbing the diagnosis. (C) Image from a 45-year-old man. Only routine position MRI scans were provided. The joint effusion or hemorrhage near the ligament tear site interfered with the diagnosis. 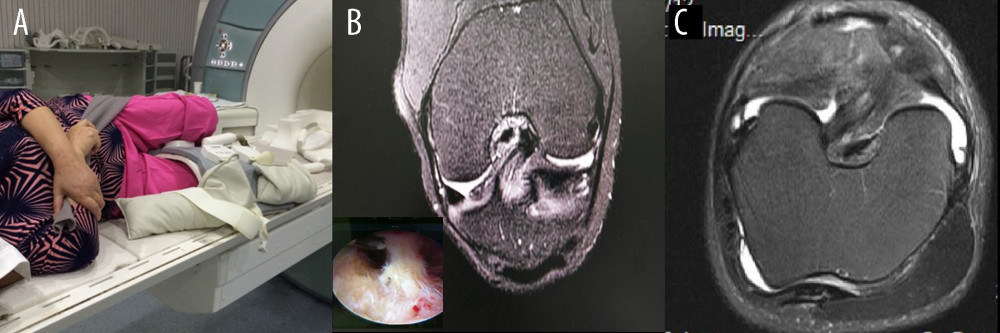 Figure 2. (A) Maximum knee flexion in lateral decubitus position magnetic resonance imaging examination of knee joint: the knee joint of the affected side in side position with maximum flexion with the coil tightly wrapped around the knee joint. (B) After additional special position scanning, the tear site showed high signal, which was diagnosed as a chronic partial tear of anterior cruciate ligament. It was confirmed by arthroscopy. (C) After additional special position scanning, the joint effusion or hemorrhage was squeezed away from the ligament tear site.
Figure 2. (A) Maximum knee flexion in lateral decubitus position magnetic resonance imaging examination of knee joint: the knee joint of the affected side in side position with maximum flexion with the coil tightly wrapped around the knee joint. (B) After additional special position scanning, the tear site showed high signal, which was diagnosed as a chronic partial tear of anterior cruciate ligament. It was confirmed by arthroscopy. (C) After additional special position scanning, the joint effusion or hemorrhage was squeezed away from the ligament tear site. Tables
Table 1. Results of the maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) compared with arthroscopy (number of patients).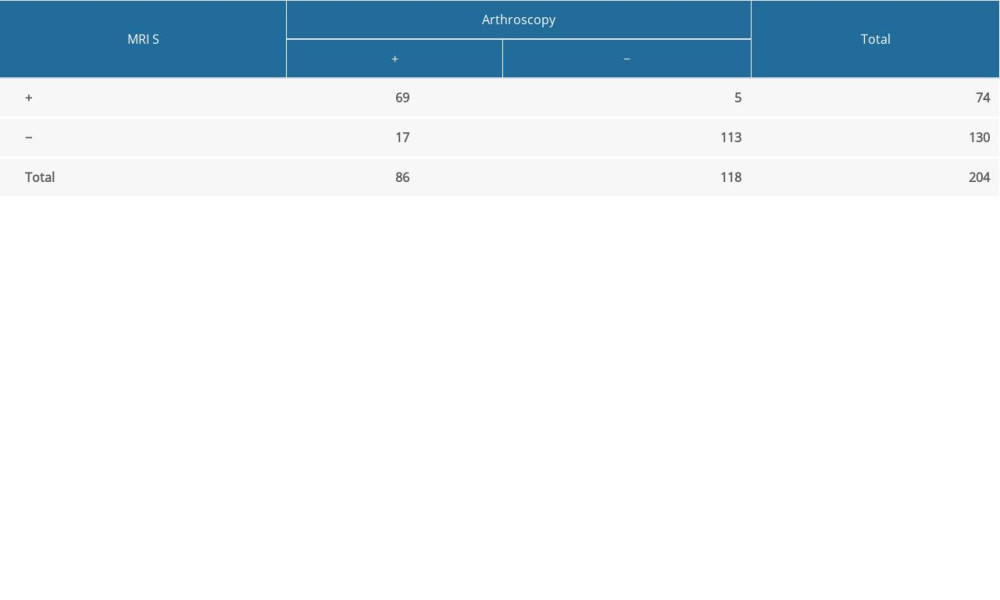 Table 2. Results of the routine magnetic resonance imaging (MRI R) compared with arthroscopy (number of patients).
Table 2. Results of the routine magnetic resonance imaging (MRI R) compared with arthroscopy (number of patients).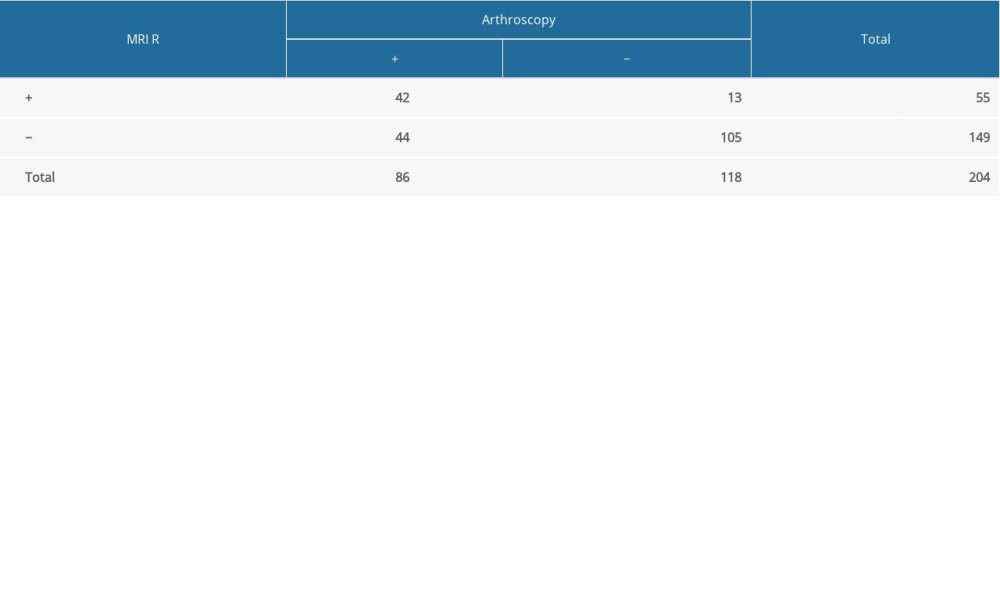 Table 3. Sensitivity and specificity of routine magnetic resonance imaging (MRI R) and special posture magnetic resonance imaging (MRI S) for diagnosing partial anterior cruciate ligament (ACL) tear.
Table 3. Sensitivity and specificity of routine magnetic resonance imaging (MRI R) and special posture magnetic resonance imaging (MRI S) for diagnosing partial anterior cruciate ligament (ACL) tear.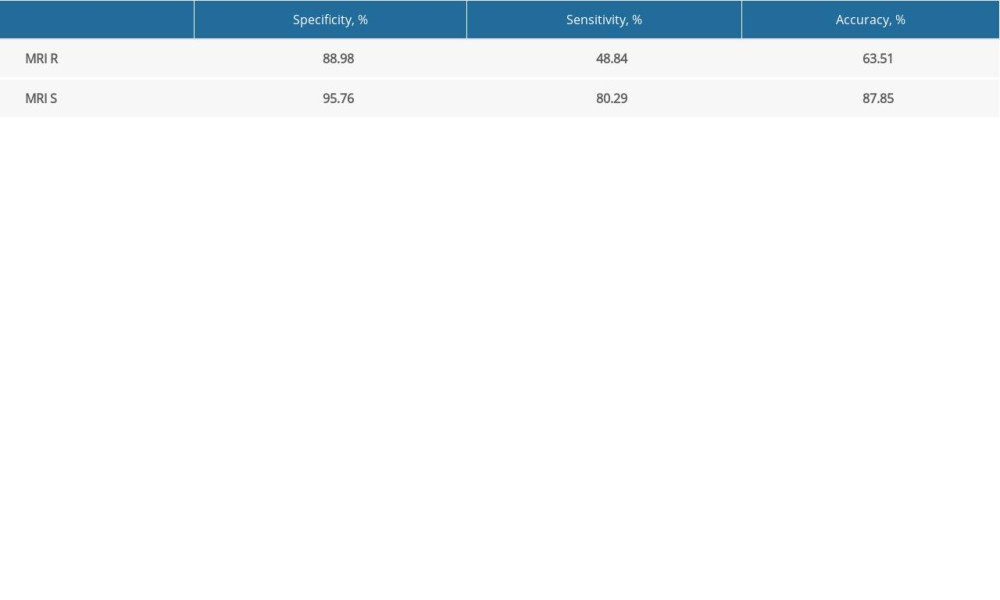 Table 4. Sensitivity and specificity of routine magnetic resonance imaging (MRI R) and maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) for diagnosing partial anterior cruciate ligament tear at different stages (time from injury to examination).
Table 4. Sensitivity and specificity of routine magnetic resonance imaging (MRI R) and maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) for diagnosing partial anterior cruciate ligament tear at different stages (time from injury to examination).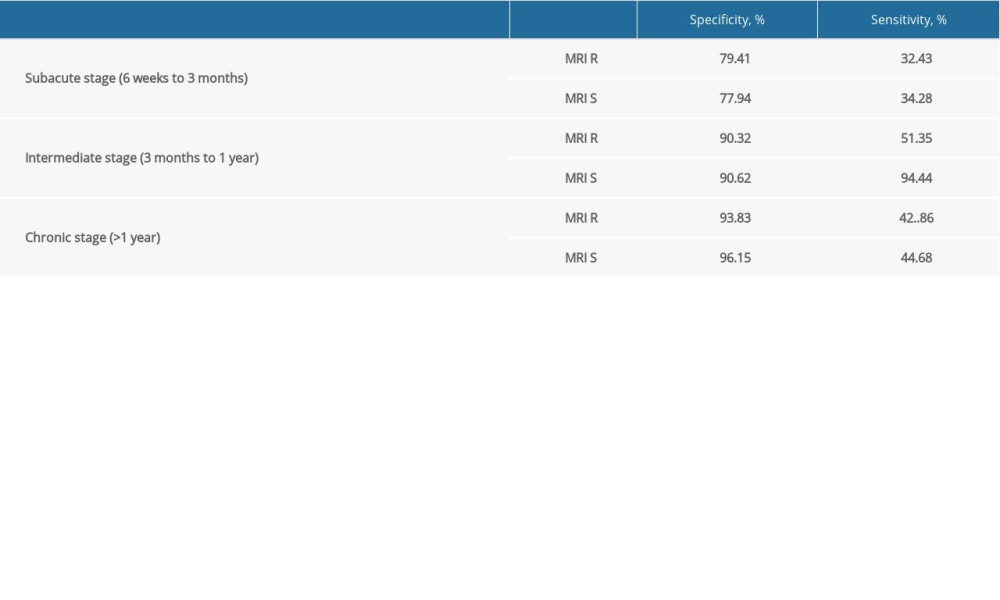 Table 5. Results of complete anterior cruciate ligament tear by routine magnetic resonance imaging (MRI R) and maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) examination.
Table 5. Results of complete anterior cruciate ligament tear by routine magnetic resonance imaging (MRI R) and maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) examination.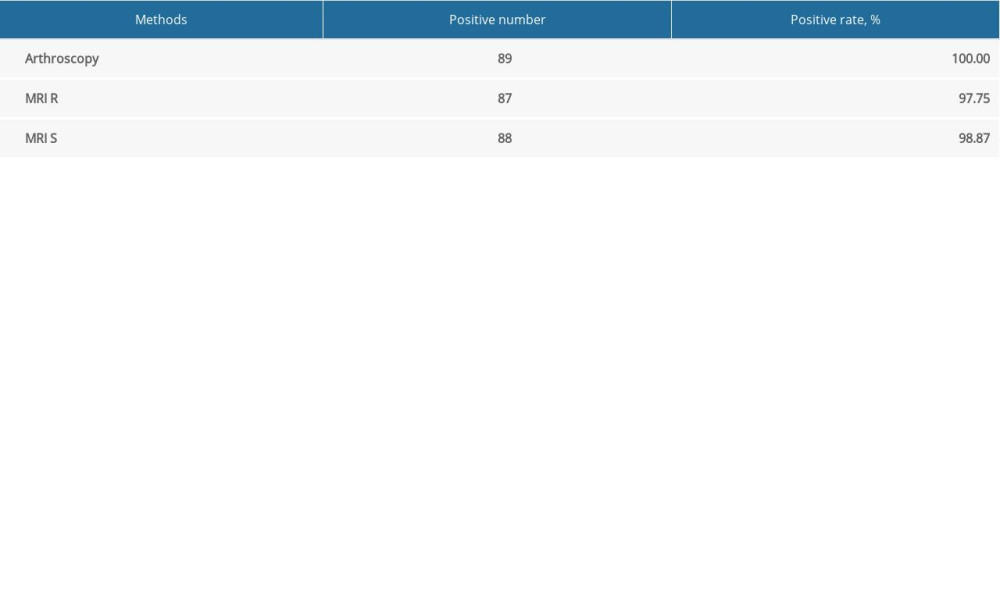
References
1. Cotten A, Delfaut E, Demondlon X, Lapegue F, MR imaging of the knee at 0.2 and 1.5 T: correlation with surgery: Am J Roentgenol, 2000; 174; 1093-97
2. Klass D, Toms AP, Greenwood R, Hopgood P, MR imaging of acute anterior cruciate ligament injuries: Knee, 2007; 14; 339-47
3. Tsai KJ, Chiang H, Jiang CC, Magnetic resonance imaging of anterior cruciate ligament rupture: BMC Musculoskelet Disord, 2004; 5; 21
4. McCauley TR, Moses M, Kier R, MR diagnosis of tears of anterior cruciate ligament of the knee: Importance of ancillary findings: Am J Roentgenol, 1994; 162; 115-19
5. Filbay SR, Grindem H, Evidence-based recommendations for the management of anterior cruciate ligament (ACL) rupture: Best Pract Res Clin Rheumatol, 2019; 33(1); 33-47
6. McNally EG, Nasser KN, Dawson S, Goh LA, Role of magnetic resonance imaging in the clinical management of the acutely locked knee: Skeletal Radiol, 2002; 31; 570-73
7. Roychowdhury S, Fitzgerald SW, Sonin AH, Using MR imaging to diagnose partial tears of the anterior cruciate ligament: Value of axial images: Am J Roentgenol, 1997; 168; 1487-91
8. Bretlau T, Tuxoe J, Larsen L, Bone bruise in the acutely injured knee: Knee Surg Sports Traumatol Arthrosc, 2002; 10; 96-101
9. Katahira K, Yamashita Y, Takahashi M, MR imaging of the anterior cruciate ligament: Value of thin slice direct oblique coronal technique: Radiat Med, 2001; 19; 1-7
10. Chen WT, Shih TT, Tu HY, Partial and complete tear of the anterior cruciate ligament: Acta Radiol, 2002; 43(5); 511-16
11. Borbon CA, Mouzopoulos G, Siebold R, Why perform an ACL augmentation?: Knee Surg Sports Traumatol Arthrosc, 2012; 20; 245-51
12. Shen H, Jiang T, Zhao JDiagnosis of old anterior cruciate ligament injury: Chinese Journal of Orthopedics, 2002; 22(3); 150-53 [in Chinese]
13. Amis AA, Dawkins GP, Functional anatomy of the anterior cruciate ligament. Fibre bundle actions related to ligament replacements and injuries: J Bone Joint Surg Br, 1991; 73(2); 260-67
14. Hofbauer M, Muller B, Murawski CD, The concept of individualized anatomic anterior cruciate ligament (ACL) reconstruction: Knee Surg Sports Traumatol Arthrosc, 2014; 22(5); 979-86
15. Ng AW, Lee RK, Ho EP, Anterior cruciate ligament bundle measurement by MRI: Skeletal Radiol, 2013; 42(11); 1549-54
16. Liu C, Zhao J, Chen LA comparative study of anterior cruciate ligament reconstruction with double bundles of autologous carmine tendon and allogenic semitendinosus tendon: Chinese Journal of Orthopedics, 2010; 30(3); 255-59 [in Chinese]
17. Davies NH, Niall D, King LJ, Magnetic resonance imaging of bone bruising in the acutely injured knee – short-term outcome: Clin Radiol, 2004; 59; 439-45
18. Burak G, Gulcan G, Abdulkadir S, A new method for diagnosis of anterior cruciate ligament tear: MRI with maximum flexion of knee in the prone position: A case control study: Int J Surg, 2019; 68; 142-47
19. Hong SH, Choi JY, Lee GK, Grading of ACL injury: Diagnostic efficacy of oblique coronal MRI of the knee: J Comput Assist Tomogr, 2003; 27(5); 814-19
20. Padulo J, Oliva F, Frizziero A, Maffulli N, Muscles, Ligaments and Tendons Journal – basic principles and recommendations in clinical and field science research: 2016 update: Muscles Ligaments Tendons J, 2016; 6(1); 1-5
21. Arfanakis K, Hermann BP, Rogers BP, Diffusion tensor MRI intemporal lobe epilepsy: Magn Reson Imaging, 2002; 20(1); 511-19
22. Breitenseher MJ, Mayerhoefer ME, Oblique MR imaging of the anterior cruciate ligament based on three-dimensional orientation: J Magnetic Res Imaging, 2007; 26; 794-98
23. Niitsu M, Ikeda K, Fukubayashi T, Knee extension and flexion: MR delineation of normal and torn anterior cruciate ligaments: J Comput Assist Tomogr, 1996; 20; 322-27
24. Pereira ER, Ryu KN, Ahn JM, Evaluation of the anterior cruciate ligament of the knee: Comparison between partial flexion true sagittal and extension sagittal oblique positions during MR imaging: Clin Radiol, 1998; 53; 574-78
25. Muhle C, Brossmann J, Heller M, Kinematic MRI of the knee using a specially designed positioning device: J Comput Assist Tomogr, 1996; 20; 522-25
Figures
Figure 1. (A) The sketch of maximum flexion of knee joint with maximum flexibility of 150°. (B) Image from a 37-year-old man, 13 months after injury. Only routine position magnetic resonance imaging (MRI) scans were provided. The display angle of anterior cruciate ligament attachment points was poor. Sagittal and coronal scanning images both had effusion disturbing the diagnosis. (C) Image from a 45-year-old man. Only routine position MRI scans were provided. The joint effusion or hemorrhage near the ligament tear site interfered with the diagnosis.Figure 2. (A) Maximum knee flexion in lateral decubitus position magnetic resonance imaging examination of knee joint: the knee joint of the affected side in side position with maximum flexion with the coil tightly wrapped around the knee joint. (B) After additional special position scanning, the tear site showed high signal, which was diagnosed as a chronic partial tear of anterior cruciate ligament. It was confirmed by arthroscopy. (C) After additional special position scanning, the joint effusion or hemorrhage was squeezed away from the ligament tear site. Tables
Table 1. Results of the maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) compared with arthroscopy (number of patients).Table 2. Results of the routine magnetic resonance imaging (MRI R) compared with arthroscopy (number of patients).Table 3. Sensitivity and specificity of routine magnetic resonance imaging (MRI R) and special posture magnetic resonance imaging (MRI S) for diagnosing partial anterior cruciate ligament (ACL) tear.Table 4. Sensitivity and specificity of routine magnetic resonance imaging (MRI R) and maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) for diagnosing partial anterior cruciate ligament tear at different stages (time from injury to examination).Table 5. Results of complete anterior cruciate ligament tear by routine magnetic resonance imaging (MRI R) and maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) examination.Table 1. Results of the maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) compared with arthroscopy (number of patients).Table 2. Results of the routine magnetic resonance imaging (MRI R) compared with arthroscopy (number of patients).Table 3. Sensitivity and specificity of routine magnetic resonance imaging (MRI R) and special posture magnetic resonance imaging (MRI S) for diagnosing partial anterior cruciate ligament (ACL) tear.Table 4. Sensitivity and specificity of routine magnetic resonance imaging (MRI R) and maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) for diagnosing partial anterior cruciate ligament tear at different stages (time from injury to examination).Table 5. Results of complete anterior cruciate ligament tear by routine magnetic resonance imaging (MRI R) and maximum knee flexion in lateral decubitus position magnetic resonance imaging (MRI S) examination. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387