24 September 2021: Clinical Research
Comparison of Outcomes Following TiRobot-Assisted Sacroiliac Screw Fixation with Bone Grafting and Traditional Screw Fixation without Bone Grafting for Unstable Osteoporotic Sacral Fracture: A Single-Center Retrospective Study of 33 Patients
Zhaojie Liu1ABE, Ya Gu1CDF, Xin Jin1DF, Wei Tian1BE, Haotian Qi1CD, Yuxi Sun1BF, Gang Li1DF, Hongchuan Wang1BF, Xiang Xiao1DF, Pengfei Li1EF, Yongcheng Hu1AD, Jian Jia1AE*DOI: 10.12659/MSM.932724
Med Sci Monit 2021; 27:e932724






Abstract
BACKGROUND: This retrospective study from a single center aimed to compare patient outcomes following TiRobot-assisted sacroiliac screw fixation and bone grafting with traditional screw fixation without bone grafting in 33 patients with unstable osteoporotic sacral fracture (UOSF).
MATERIAL AND METHODS: Patients with UOSF were included and divided into 2 groups: a TiRobot-assisted surgical group with 18 patients (robot-aided sacroiliac screw fixation and bone grafting) and a standard surgical group with 15 patients (free-hand screw fixation without bone grafting). T values of bone mineral density (BMD) £-2.5 standard deviation (SD) were diagnosed as osteoporosis. Screw positioning and fracture healing time were evaluated. Functional outcomes were investigated at the final follow-up.
RESULTS: There were no statistically significant differences in screw positioning; however, there were satisfactory positioning rates in 94.4% (17/18) of patients in the TiRobot-assisted surgical group and 73.3% (11/15) in the standard surgical group. The advantages with TiRobot on surgical time of screw placement, fluoroscopy frequency, and total drilling times were noted (P=0.000). The nonunion rates were 5.6% (1/18) in the TiRobot-assisted surgical group and 33.3% (5/15) in the standard group (P=0.039). Healing time in the union cases had a significant difference (P=0.031). Functional outcome scores in the TiRobot-assisted surgical group were superior to that in the standard group (P=0.014).
CONCLUSIONS: The findings showed that TiRobot-assisted sacroiliac screw fixation and bone grafting was a safe and effective surgical treatment option that had a reduced radiation dose and improved fracture healing, when compared with standard screw fixation without bone grafting.
Keywords: Fracture Fixation, Internal, Fractures, Bone, Minimally Invasive Surgical Procedures, Osteoporosis, Robotics, Sacrum, Aged, 80 and over, Bone Screws, Bone Transplantation, Female, Humans, Osteoporotic Fractures, Robotic Surgical Procedures
Background
Osteoporotic pelvic fractures, which are related to low bone strength, comprise up to 7% of all osteoporotic fractures and have attracted much attention owing to their increasing frequency [1]. An investigation has demonstrated that approximately two-thirds of all pelvic fractures are osteoporotic fractures, which occur because of an aging population [2].
For elderly people, the decrease of bone mineral density (BMD) in the sacrum follows a unique and consistent pattern. The most obvious decrease of BMD is in the area lateral to the S1 and S2 foramina due to reductions in the trabecula bone, sometimes with significant voids in both sacral alae (Figure 1). Disruption of the weakened bony structures with the ligaments remaining intact is the main characteristic of the fragility fractures of the pelvic ring [3]. In most of these cases with incomplete sacral fractures, conservative treatment can be used. However, complete sacral fractures associated with anterior pelvic ring injuries are considered to be a fracture form with a high degree of instability, and surgical intervention is a valid treatment alternative [4]. If such patients have osteoporosis, management can be more cumbersome, and the fixation methods should be deliberated.
Several options can be used for stabilizing the posterior pelvic ring, such as a transiliac internal fixator, lumbopelvic fixation, and percutaneous sacroiliac screw fixation [5–7]. In recent years, sacroiliac screw fixation has been considered the workhorse of sacral fractures involved in the areas of zone I and II [8]. However, appropriate S1 corridors in 66% of female and 63% of male patients were reported, with appropriate S2 corridors in all female and 87% of male patients included in the investigation [9]. Additionally, the anchorage force of screw fixation in the osteoporotic bone must decrease if the position of the guiding wire is repeatedly adjusted. Consequently, ideal sacroiliac screw placement is challenging, especially in the sacral dysmorphisms with oblique or narrow osseous corridors. Currently, the navigation technique has been demonstrated to be optimal for percutaneous placement of the sacroiliac screw to achieve accurate and efficient results. In addition, internal fixation under robotic guidance can reduce the frequency of intraoperative fluoroscopy use, especially with the TiRobot orthopedic surgery robot, which was made in China [10,11].
Elderly patients with osteoporotic bones have significantly low BMD, which results in a high failure rate of screw fixation [12]. Failure to achieve stable anchorage in sacroiliac screw fixation can lead to screw loosening, unless strict bed rest is undertaken. The cement augmentation technique has been used for years and has been shown to have a higher pull-out strength for screw fixation in the treatment of sacral insufficient fractures with poor healing potentiality [13,14]. However, cement can neither degrade nor organically combine with the host bone to achieve bone ingrowth. The sacral fracture will never heal because of cement interposition [15]. In particular, as a major complication, cement leakage can cause serious consequences. Due to the heat generated in the process of cement solidification, cement leakage has a high risk of causing neurological damage, such as the direct damage of the L5 nerve, where it is exactly over the sacral promontory [16]. In a series of 63 cases with sacral fractures treated by sacroplasty, cement leakage was reported within the fracture gap (27%), veins (6%), neuroforamina (3%), and intervertebral disc space L5/S1 (2%) [17]. For unstable osteoporotic sacral fractures (UOSFs), the sacrum has been found to be completely broken and usually with obvious displacement. Therefore, the application of such materials is controversial.
As a substitute of autogenous bone grafting, artificial bone is mainly composed of calcium sulfate or calcium phosphate. Different from cement, bone substitute does not generate heat during solidification and can be injected along the sacroiliac screw channel to fill in the cavities and defects in the sacrum to increase the fixation strength of the screw. With the gradual degradation and absorption of the bone substitute, bone growth can be easily achieved in the target area [18].
To date, however, there are insufficient reports on the application of a robotic surgery system in injectable bone grafting through the screw channel and simultaneous sacroiliac screw fixation. Therefore, this retrospective study from a single center aimed to compare patient outcomes following TiRobot-assisted sacroiliac screw fixation and bone grafting with traditional screw fixation without bone grafting in 33 patients with UOSF.
Material and Methods
INCLUSIVE AND EXCLUSION CRITERIA:
The inclusive criteria were as follows: 1) patients with Tile [19]. type B or C pelvic fractures combined with sacral complete fractures and T values of BMD ≤-2.5 SD; 2) patients with sacral fractures treated with absorbable injectable bone grafting and percutaneous sacroiliac screw fixation under robotic navigation guidance; 3) patients with sacral fractures treated with percutaneous sacroiliac screws using the free-hand technique as control; 4) evaluation with imaging and function outcomes described by Mears [20]. and Majeed [21]; and 5) patient data was collected retrospectively.
The exclusion criteria were as follows: 1) the time from injury to surgery that was more than 3 weeks; 2) the S1 osseous corridor was unable to accommodate a ϕ7.3-mm screw; and 3) the follow-up period was less than 12 months.
PATIENTS:
We retrospectively analyzed 78 patients with osteoporotic sacral fractures who were admitted to our department from April 2012 to February 2020. A total of 33 patients (9 men, 24 women) who met the inclusion and exclusion criteria were divided into 2 groups based on different methods of sacroiliac screw placement with or without bone grafting: the TiRobot-assisted surgical group included patients who underwent robot-aided screw fixation combined with injectable bone substitute through the screw channel and the standard surgical group included patients who underwent free-hand screw fixation without bone grafting.
In total, there were 5 men and 13 women in the TiRobot-assisted surgical group, aged from 53 to 80 years. The injuries occurred after falls from a standing position or some height in 16 patients and from traffic accidents in 2 patients. According to the classification by Denis on sacral fractures [22], 12 sacral fractures were classified as type I and 6 as type II. Anterior pelvic ring injuries occurred in all patients in the TiRobot-assisted surgical group, including pubic rami fractures in 15 patients and pubic symphysis diastasis in 3 patients. According to the classification of the pelvic fractures described by Tile [19], there were type B pelvic fractures in 5 patients and type C in 13 patients. Sacral nerve damage occurred with grade II and grade I in each of 2 patients based upon Gibbons’ classification [23] of neurologic deficits. There were 4 men and 11 women in the standard surgical group, aged from 51 to 81 years. The injuries were caused by falling from a standing position or some height in 14 patients and from a traffic accident in 1 patient. Ten sacral fractures were classified with Denis type I and 5 were classified with type II. Anterior pelvic ring injuries also occurred in all patients of the standard surgical group, including pubic rami fractures in 13 patients and pubic symphysis diastasis in 2 patients. There were Tile type B pelvic fractures in 4 patients and type C in 11 patients. Sacral nerve injury was classified with Gibbons’ grade I in 1 patient and grade II in 1 patient.
PREOPERATIVE PREPARATION:
After admission, patients were monitored for vital signs. Venous access was established, and blood volume expansion therapy, including rehydration and blood transfusion, were undertaken for the patients with unstable hemodynamics. Once they passed the resuscitation phase, definitive surgical treatment was planned. BMD was routinely examined in our institution for patients over 50 years of age and was evaluated with dual X-ray absorptiometry (DXA). The reference of SD was used with T scores based on the examination of DXA, and osteoporosis was defined as a T score of less than or equal to −2.5 SD, according to the criteria of the World Health Organization. According to the inclusion criteria, T scores of BMD ≤-2.5 SD were included in this study [24].
All patients with pelvic fractures were examined with computed tomography (CT) scans. According to the injury mechanism of the sacral fracture, supracondylar bone traction was performed to correct the displacement if there was vertical instability. The iliac cortical density and S1 and S2 corridors were measured with CT data to verify if S1 and S2 screws could be placed. Visual analog scale (VAS) scores were investigated for all patients after surgery.
TIROBOT ORTHOPEDIC SURGERY ROBOT AND THE C-ARM MACHINE:
The TiRobot orthopedic surgery robot, the third generation TianJi robot (TINAVI Medical Technologies, Beijing, China), consists of a main console with a surgical planning system and a navigation-controlled workstation, an infrared optical tracking system, and a robotic 6-axis-arm (Figure 2).
The fluoroscopy equipment that connected with the TiRobot orthopedic surgery robot was the mobile C-arm machine (Siemens, Germany).
ABSORBABLE INJECTABLE BONE SUBSTITUTE:
The absorbable injectable bone substitute ALLOMATRIX® (Wright, Memphis, TN, USA) that was used was composed of 13% calcium sulfate and 87% demineralized bone matrix and bone morphogenetic proteins.
SURGICAL PROCEDURES:
All surgical procedures were carried out by the same surgeons, who had sufficient experience. After general anesthesia, the patient was placed on the radiolucent orthopedic operating table. Percutaneous sacroiliac screw fixation was first performed for non-displaced sacral fractures to avoid the radiographic disturbance of the anterior ring implant. For displaced anterior and posterior pelvic ring fractures, anatomical reduction and internal fixation of anterior pelvic ring helped to reduce sacral fractures.
Open reduction and lumbopelvic fixation were performed immediately, with patients in the prone position for those whose sacral fractures were still associated with residual vertical displacement after indirect reduction. Unilateral sacral fractures were treated with triangle osteosynthesis using a lumbosacral posterior paramedian incision, whereas bilateral fractures had a middle incision. After exposure of the posterior superior iliac spine and L5 superior articular process, a 6-mm implant system (Kanghui, China) consisting of polyaxial pedicle screws and polyaxial iliac screws and rods was used to reduce and fix the vertical displaced sacral fractures.
For patients in the TiRobot-assisted surgical group, it was optimal to put them in the supine position to avoid the impact on the accuracy of the robot-aided sacroiliac screw placement caused by breathing movement. A navigation tracker was fixed on the contralateral anterior superior iliac spine percutaneously. Next, the calibrator was connected to the end of the robotic arm, and the 10 target points on it were confirmed within the range of the infrared optical tracking system. After standard pelvic inlet, outlet, and lateral views for the affected sacrum had been achieved with fluoroscopies, the images were transmitted to the main console for planning the sacroiliac screws for S1 and/or S2, according to the morphology of the affected sacrum. After establishing the navigation planning, the robotic arm moved to the screw entry point outside the body, following guidance. The protective sleeve was then placed onto the lateral lamina of the iliac wing through a 1-cm skin incision. After recalibration in the surgical planning system, a guiding wire was drilled along the preplanned trajectory of the sacroiliac screw. The guiding wire was placed into the sacral body, or even across the contralateral sacroiliac joint if the screw channel measured from the CT scans was introduced with sufficient depth. After the length had been measured, the entry point in the cortex was reamed with a corresponding cannulated drill, the diameter of which was smaller than the sacroiliac screw. After insertion of a metal cannula, the guiding wire was removed. Next, the calcium sulfate material, ALLOMATRIX® bone substitute (Wright, USA), was prepared in a semi-liquid state for injection under C-arm fluoroscopy. Owing to the limited solidification time, the bone substitute was injected successfully along the wire path. To ensure the effective bone graft into the target area, including the fracture site and sacral alae, the surgeon moved the conduit back and forth while injecting. Next, the guiding wire needed to be reinserted, and the cannulated screw with a diameter of 7.3 mm (Synthes, Switzerland) was fully placed. In the standard surgical group, bone grafting was not performed, and sacroiliac screws were inserted free-hand, with C-arm monitoring pelvic inlet and outlet views repeatedly conducted. Next, the position of the screws and the reduction of sacral fractures were confirmed with pelvic inlet, outlet, and lateral view by the C-arm machine.
For the patients in the standard surgical group, percutaneous sacroiliac screw fixation without bone grafting was performed with the traditional free-hand technique, following frequent pelvic inlet and outlet views with the C-arm machine.
Open reduction and the pre-contoured 3.5-mm reconstruction locking plate (Zimmer, USA) fixation were performed via the Pfannenstiel approach for pubic symphysis diastasis. With the displaced pubic superior rami fractures, open reduction was performed using the Stoppa approach and/or an iliac fossa incision, and the pre-contoured reconstruction locking plates were inserted subperiosteally. For the pubic superior rami fractures without obvious displacement, if the fracture line was located internally to the obturator, the fractures were still fixed with the pre-contoured 3.5-mm reconstruction locking plates, and if the fracture line was located laterally to the obturator, antegrade or retrograde cannulated screws were used.
POSTOPERATIVE MANAGEMENT:
Second generation cephalosporin was administered intravenously 30 min before surgery and continued for 24 h after surgery. Patients were encouraged to mobilize their lower extremities without weight bearing from 2 weeks after surgery. Partial weight bearing was initiated 4 weeks after surgery, and full weight bearing was permitted only when fracture lines were indistinctive from a series of pelvic radiographies at the follow-up visits. As long as patients had no absolute contraindications with medications, bisphosphonate anti-osteoporosis treatment, according to osteoporosis guidelines, was used for 6 months.
FOLLOW-UP:
Clinical and radiographic follow-up was conducted for at least 12 months after surgery. Healing was defined as relative comfort in the pelvic area with activities and obliteration of fracture lines on pelvic anteroposterior, inlet, and outlet X-ray radiographs. Patient questionnaires about daily activities, including pain, gait, and whether walking aids were needed or not, were completed at each follow-up.
According to the evaluation criteria of pelvic images described by Mears [20], the reduction of pelvic fractures in 3 planes was measured and classified as follows: extremely satisfactory reduction (anatomical reduction), satisfactory reduction (rotation <15° and horizontal displacement <1 cm and vertical displacement <1 cm), and unsatisfactory reduction (rotation >15° and/or horizontal displacement >1 cm and/or vertical displacement >1 cm). The positioning of the sacroiliac screw was evaluated by the modified Gras classification, which consists of 3 grades: grade I, satisfactory, in the sacral corridor; grade II, secure, contacting the cortex; and grade III, misplaced, penetrating the cortex [25]. The function outcomes were assessed according to the Majeed scoring system [21]. Clinical outcomes were graded as excellent (>84), good (70–84), fair (55–69), or poor (<55).
STATISTICAL ANALYSIS:
Relevant data were processed by SPSS (version 20.0; IBM Corp, Armonk, NY, USA), and a value of
Results
The demographic data of the 2 groups in the study demonstrated no statistically significant differences (Table 1).
The mean surgical time of sacroiliac screw placement was 17.0±3.0 min in the TiRobot-assisted surgical group and 34.5±10.6 min in the standard surgical group (
Postoperative CT scanning indicated that there was no incidence of screw perforation. Based upon the modified Gras classification [25], there were 17 patients with grade I and 1 patient with grade II in the TiRobot-assisted surgical group, and 11 patients with grade I and 4 patients with grade II in the standard surgical group (
Excluding the 6 patients with nonunion, the mean healing time was 4.1±1.2 months in the TiRobot-assisted surgical group and 5.2±1.3 months in the standard surgical group (
Typical cases are exhibited in Figures 3 and 4.
Discussion
The main findings of this study were that the ideal position of sacroiliac screws, including the entry point and angulation in a safe osseous corridor, was planned and positioned by the robot navigation system and absorbable bone substitute was accurately injected into the osteoporotic area simultaneously. This technique demonstrated a reasonable treatment option for UOSF, achieving satisfactory results.
Compared with iliac screws and locking compression plates, sacroiliac screws have been shown to have biomechanical advantages on the fixation of the posterior pelvic ring and have been shown to be less invasive [26]. The main challenges and risks of sacroiliac screw fixation are individual variations in the 3-dimensional space of the sacrum, owing to the sacral dysmorphism, and important neurovascular structures in close proximity to the osseous boundary. According to our experience in this study, the advantages of robot-aided percutaneous sacroiliac screw fixation can be summarized as follows. Conventionally, the accurate entry point and trajectory of sacroiliac screws possibly need to be attempted frequently with a C-arm machine, which is the principal factor to decrease the pull-out force of screws, especially in patients with osteoporosis; whereas, following the surgical planning with the robot system, the protective sleeve can be directly placed onto the accurate entry point by the 6-axis arm. In contrast to sacroiliac screw fixation with the free-hand method, radiation exposure for patients and operating room personnel under robotic guidance were significantly reduced in this study (
For patients with osteoporosis with thin cortical bone and decreasing trabecula in the cancellous bone, cement augmentation combined with sacroiliac screw fixation can play an important role in stabilizing fractures when the sacral fractures are treated surgically. However, the injectable bone substitute that has calcium sulfate as the main component, which we used in this study, can effectively enhance bone strength and promote bone healing [32]. In the TiRobot-assisted surgical group, bone substitute leakage into sacral foramina occurred in only 1 patient, with no related symptoms of neurologic damage. The outcome in our study showed that TiRobot-assisted bone grafting was more accurate than grafting with the free-hand technique used in previous studies [16,17]. In particular, compared with medical cement, this sort of injectable bone substitute did not produce heat during solidification, thereby effectively avoiding some serious complications.
Some of the other advantages of the bone substitute are as follows. First, as a bone conduction scaffold, the solidified bone substitute is poriferous and can effectively occupy and prevent the soft tissue, except the blood vessels, from growing into the filling area. Experiments have shown that osteoblasts can adhere on the surface of calcium sulfate and form absorption lacunae, just as in normal bone [33]. Second, the solidified bone substitute can provide structural support with a certain strength and perform the role of augmentation to enhance the fixation of a sacroiliac screw in the target area. Third, owing to the presence of bone morphogenetic proteins, this bone substitute can induce bone growth of sacral fractures in patients with osteoporosis with poor osteogenic ability. In addition, the absorption of calcium sulfate can form a local acidic environment, leading to the decalcification of the surrounding cancellous bone and stimulating the activities of osteoinductive factors for the formation of new bone. One study showed that the absorption time of calcium sulfate in vivo is about 30 to 60 days, whereas calcium phosphate bone substitute is so stable that it takes 1 to 2 years to be absorbed completely, which would delay normal bone healing [34]. Finally, with the creation of an accurate sacroiliac screw channel under robotic guidance, it is important that the bone substitute can be injected into the target area for the minimally invasive treatment of UOSF. In consecutive follow-ups of our patients, the mean healing time was 4.1±1.2 months in the TiRobot-assisted surgical group and 5.2±1.3 months in the standard surgical group, except for 6 cases of nonunion. The nonunion rates of sacral fractures were 5.6% (1/18) in the TiRobot-assisted surgical group and 33.3% (5/15) in the standard surgical group; the difference was statistically significant (
There are some surgical precautions and technical key points that need to be carefully considered during the manipulative process. First, to ensure the accuracy of the sacroiliac screw, the relative position between the tracker and fracture ends should be maintained during the procedure, from navigation planning to the guiding wire insertion. The operation should be performed gently, otherwise the spatial corridor of the sacroiliac screw can cause changes, resulting in inaccurate screw positioning or even failure. Second, the accuracy of the described technique is very sensitive to the relative position of the robotic arm and patient. The thoracic movement with respiration can have a slight impact on the relative position of the patient’s body and the drilling sleeve in the prone position. Therefore, the supine position should be taken instead of the prone position. If the prone position is necessary because of lumbopelvic fixation, the patient’s respiration should be paused for a few seconds in order to insert the guiding wire accurately under robotic guidance. Third, a cannulated drill with the diameter smaller than that of sacroiliac screw is used to enlarge the context to insert a metal cannula along the guiding wire, which is a crucial step for the injection of the semi-liquid bone substitute to fill the screw channel and even the fracture gaps. Additionally, the amount of bone substitute injected into the target area should be reasonably planned, generally 10 mL, to reduce the risk of leakage and avoid insufficient bone grafting. Even so, the leakage of bone graft into sacral foramina occurred in 1 patient, with no related symptoms. Therefore, the injection process of bone grafting should be monitored with a C-arm machine. Finally, for the osteoporotic patients with unstable sacral fractures, it is important that S1 and S2 screws are used simultaneously to increase the fixation effect, unless the anatomic corridor is limited according to the biomechanical study of sacroiliac screw fixation [35].
This study has some limitations. This technology is associated with higher costs owing to the TiRobot orthopedic surgery robot and, consequently, it cannot be carried out in all medical institutions. To increase the persuasiveness of this study, a multi-center study is recommended that could span a longer period to recruit a larger sample size and further validate the practicability of this method.
Conclusions
The findings from this retrospective review of patients with UOSF at a single center showed that TiRobot-assisted sacroiliac screw fixation and bone grafting was a safe and effective surgical treatment option that had a reduced radiation dose and improved fracture healing, compared with traditional screw fixation without bone grafting.
Figures
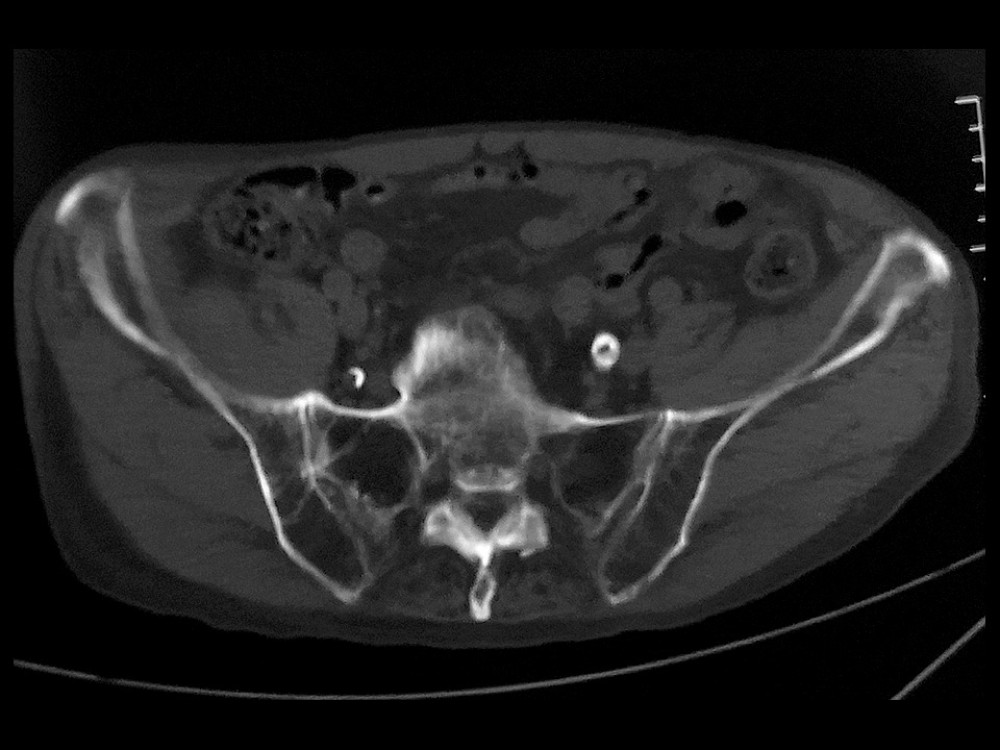 Figure 1. Transverse computed tomography (CT) scan of an 80-year-old woman with osteoporosis. There are obvious alar voids in both sacral alae, corresponding with a significant resorption of trabecular bone.
Figure 1. Transverse computed tomography (CT) scan of an 80-year-old woman with osteoporosis. There are obvious alar voids in both sacral alae, corresponding with a significant resorption of trabecular bone.  Figure 2. Overall view of the TiRobot navigation system. It consists of a main console, tracking system, and robotic arm.
Figure 2. Overall view of the TiRobot navigation system. It consists of a main console, tracking system, and robotic arm. 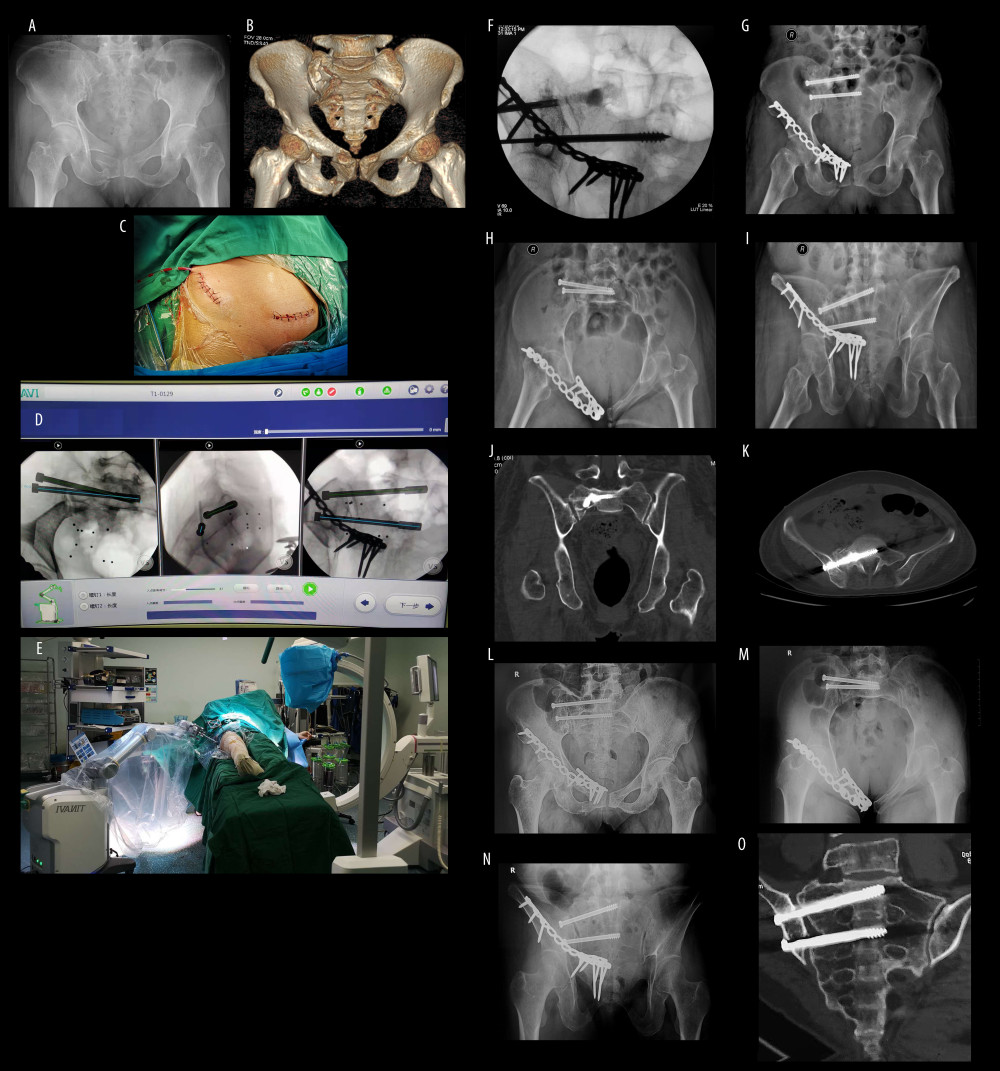 Figure 3. A 67-year-old woman with injury from falling from a height. (A) The anteroposterior pelvic view reveals displaced superior and inferior pubic rami fractures on the right side, close to pubic symphysis. (B) Computed tomography (CT) construction scan of the pelvic ring demonstrates the overlapping superior and inferior pubic rami fracture and the compression sacral fracture due to the internal rotation of the pelvis. It concerns a type B1 lesion according to Tile classification on pelvic fracture. (C) The medial and lateral incisions of anterior pelvis ring. (D) Path planning of sacroiliac screw placement in S1 and S2. (E) Overall view of robot-aided sacroiliac screw manipulation. (F) Bone grafting via sacroiliac screw channel under C-arm fluoroscopy. There is a dense shadow in sacral ala, showing the injectable bone substitute. (G–I) Postoperative anteroposterior, inlet and outlet views. (J, K) Coronal and transverse CT views showing the positioning of the sacroiliac screw and the bone grafting. (L–O) Anteroposterior, inlet and outlet views and CT scan at 6 months after surgery showing the union of sacrum.
Figure 3. A 67-year-old woman with injury from falling from a height. (A) The anteroposterior pelvic view reveals displaced superior and inferior pubic rami fractures on the right side, close to pubic symphysis. (B) Computed tomography (CT) construction scan of the pelvic ring demonstrates the overlapping superior and inferior pubic rami fracture and the compression sacral fracture due to the internal rotation of the pelvis. It concerns a type B1 lesion according to Tile classification on pelvic fracture. (C) The medial and lateral incisions of anterior pelvis ring. (D) Path planning of sacroiliac screw placement in S1 and S2. (E) Overall view of robot-aided sacroiliac screw manipulation. (F) Bone grafting via sacroiliac screw channel under C-arm fluoroscopy. There is a dense shadow in sacral ala, showing the injectable bone substitute. (G–I) Postoperative anteroposterior, inlet and outlet views. (J, K) Coronal and transverse CT views showing the positioning of the sacroiliac screw and the bone grafting. (L–O) Anteroposterior, inlet and outlet views and CT scan at 6 months after surgery showing the union of sacrum. 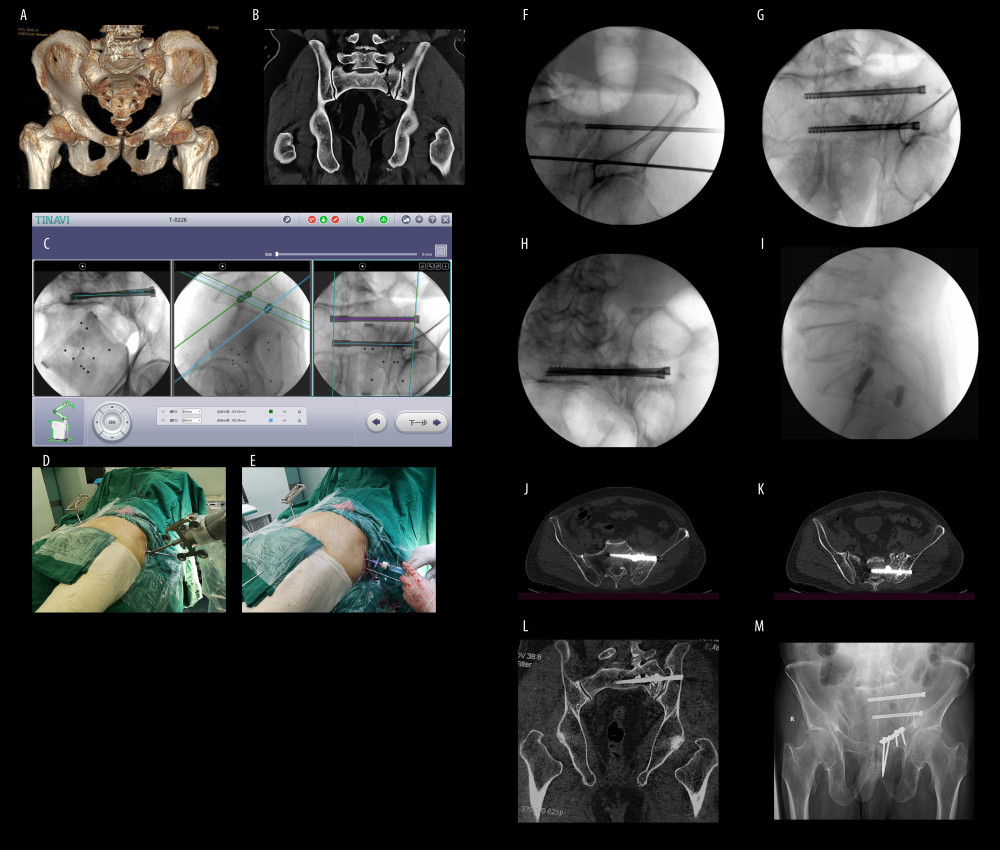 Figure 4. A 75-year-old man with an injury from a car accident. (A) Computed tomography (CT) construction scan of the pelvic ring reveals the displaced pubic body and inferior pubic rami fracture associated with the ipsilateral sacral fracture. (B) Coronal CT scan showing the complete sacral fracture. (C) Intraoperative planning of sacroiliac screws after collection and transmission of the radiographs. (D) The view of robotic arm positioning at the entry point of sacroiliac screw. (E) The intraoperative picture demonstrating bone grafting injected along the channel of the sacroiliac screw. (F) Bone grafting along sacroiliac screw channel under C-arm fluoroscopy. (G–I) Intraoperative anteroposterior, inlet, and outlet views. (J–L) Postoperative coronal and transverse CT views revealing the satisfactory positioning of sacroiliac screws and the bone grafting. (M) The pelvic outlet view at 6 months after surgery showing that the fracture healed.
Figure 4. A 75-year-old man with an injury from a car accident. (A) Computed tomography (CT) construction scan of the pelvic ring reveals the displaced pubic body and inferior pubic rami fracture associated with the ipsilateral sacral fracture. (B) Coronal CT scan showing the complete sacral fracture. (C) Intraoperative planning of sacroiliac screws after collection and transmission of the radiographs. (D) The view of robotic arm positioning at the entry point of sacroiliac screw. (E) The intraoperative picture demonstrating bone grafting injected along the channel of the sacroiliac screw. (F) Bone grafting along sacroiliac screw channel under C-arm fluoroscopy. (G–I) Intraoperative anteroposterior, inlet, and outlet views. (J–L) Postoperative coronal and transverse CT views revealing the satisfactory positioning of sacroiliac screws and the bone grafting. (M) The pelvic outlet view at 6 months after surgery showing that the fracture healed. References
1. Burge R, Dawson-Hughes B, Solomon DH, Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025: J Bone Miner Res, 2007; 22(3); 465-75
2. Kannus P, Palvanen M, Niemi S, Epidemiology of osteoporotic pelvic fractures in elderly people in Finland: sharp increase in 1970–1997 and alarming projections for the new millennium: Osteoporos Int, 2000; 11(5); 443-48
3. Rommens PM, Hofmann A, Comprehensive classification of fragility fractures of the pelvic ring: recommendations for surgical treatment: Injury, 2013; 44; 1733-44
4. Bruce B, Reilly M, Sims S, OTA highlight paper predicting future displacement of nonoperatively managed lateral compression sacral fractures: Can it be done?: J Orthop Trauma, 2011; 25; 523-27
5. Füchtmeier B, Maghsudi M, Neumann C, The minimally invasive stabilization of the dorsal pelvic ring with the transiliacal internal fixator (TIFI) – surgical technique and first clinical findings: Unfallchirurg, 2004; 107(12); 1142-51
6. Piltz S, Rubenbauer B, Böcker W, Trentzsch H, Reduction and fixation of displaced U-shaped sacral fractures using lumbopelvic fixation: Technical recommendations: Eur Spine J, 2018; 27(12); 3025-33
7. Iorio JA, Jakoi AM, Rehman S, Percutaneous sacroiliac screw fixation of the posterior pelvic ring: Orthop Clin North Am, 2015; 46(4); 511-21
8. Tidwell J, Cho R, Reid JS, Percutaneous sacroiliac screw technique: J Orthop Trauma, 2016; 30(Suppl 2); S19-20
9. König MA, Sundaram RO, Saville P, Anatomical considerations for percutaneous trans ilio-sacroiliac S1 and S2 screw placement: Eur Spine J, 2016; 25; 1800-5
10. Liu HS, Duan SJ, Xin FZ, Robot-assisted minimally-invasive internal fixation of pelvic ring injuries: A single-center experience: Orthopaedic Surgery, 2019; 11(1); 42-51
11. Long T, Li KN, Gao JH, Comparative study of percutaneous sacroiliac screw with or without TiRobot assistance for treating pelvic posterior ring fractures: Orthop Surg, 2019; 11(3); 386-96
12. Mears SC, Sutter EG, Wall SJ, Biomechanical comparison of three methods of sacral fracture fixation in osteoporotic bone: Spine (Phila Pa 1976), 2010; 35(10); E392-95
13. Grechenig S, Gansslen A, Gueorguiev B, PMMA-augmented SI screw: A biomechanical analysis of stiffness and pull-out force in a matched paired human cadaveric model: Injury, 2015; 46(Suppl 4); S125-28
14. Kortman K, Oetiz O, Miller T, Multicenter study to assess the efficacy and safety of sacroplasty in patients with osteoporotic sacral insufficiency fractures or pathologic sacral lesions: J Neurointerv Surg, 2013; 5(5); 461-66
15. Rommens PM, Ossendorf C, Pairon P, Clinical pathways for fragility fractures of the pelvic ring: Personal experience and review of the literature: J Orthop Sci, 2015; 20(1); 1-11
16. Bayley E, Srinivas S, Boszczyk BM, Clinical outcomes of sacroplasty in sacral insufficiency fractures: A review of the literature: Eur Spine J, 2009; 18(9); 1266-71
17. Bastian JD, Keel MJ, Heini PF, Complications related to cement leakage in sacroplasty: Acta Orthop Belg, 2012; 78(1); 100-5
18. Grüneweller N, Wähnert D, Raschke MJ, Fuchs T, Implant augmentation in pelvic surgery. Options and technique: Unfallchirurg, 2015; 118(10); 831-37
19. Tile M: Fractures of the pelvis and acetabulum, 1995, Baltimore, Williams & Wilkins
20. Mears DC, Velyvis J, Surgical reconstruction of late pelvic post-traumatic nonunion and malalignment: J Bone Joint Surg Br, 2003; 85; 21-30
21. Majeed SA, Grading the outcome of pelvic fractures: J Bone Joint Surg Br, 1989; 71(2); 304-6
22. Denis F, Davis S, Comfort T, Sacral fractures: An important problem. Retrospective analysis of 236 cases: Clin Orthop Relat Res, 1988; 227; 67-81
23. Gibbons KJ, Soloniuk DS, Razack N, Neurological injury and patterns of sacral fractures: J Neurosurg, 1990; 72; 889-93
24. World Health Organization, Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO study group: World Health Organ Tech Rep Ser, 1994; 843; 1-129
25. Gras F, Marintschev I, Wilharm A, 2D-fluoroscopic navigated percutaneous screw fixation of pelvic ring injuries – a case series: BMC Musculoskelet Disord, 2010; 11; 153
26. Lee CH, Hsu CC, Huang PY, Biomechanical study of different fixation techniques for the treatment of sacroiliac joint injuries using finite element analyses and biomechanical tests: Comput Biol Med, 2017; 87; 250-57
27. Hou ZY, Zhang Q, Chen W, The application of the axial view projection of the S1 pedicel for sacroiliac screw: J Trauma, 2010; 69(1); 122-27
28. Zwingmann J, Konrad G, Mehlhorn AT, Percutaneous iliosacral screw insertion: Malpositioning and revision rate of screws with regards to application technique (navigated vs. Conventional): J Trauma, 2010; 69(6); 1501-6
29. Hinsche AF, Giannoudis PV, Smith RM, Fluoroscopy-based multiplanar image guidance for insertion of sacroiliac screws: Clin Orthop Relat Res, 2002; 395; 135-44
30. van den Bosch EW, van Zwienen CM, van Vugt AB, Fluoroscopic positioning of sacroiliac screws in 88 patients: J Trauma, 2002; 53(1); 44-48
31. Zwingmann J, Hauschild O, Bode G, Malposition and revision rates of different imaging modalities for percutaneous iliosaeral screw fixation following pelvic fractures: A systematic review and meta-analysis: Arch Orthop Trauma Surg, 2013; 133(9); 1257-65
32. Yashavantha KC, Nalini KB, Jagdish M, Calcium sulfate as bone graft substitute in the treatment of osseous bone defects, a prospective study: J Clin Diagn Res, 2013; 7(12); 2926-28
33. Winn SR, Hollinger JO, An osteogenic cell culture system to evaluate the cytocompatibility of Osteoset, a calcium sulfate bone void filler: Biomaterials, 2000; 21(23); 2413-25
34. Fulmer MT, Ison IC, Hankermayer CR, Measurements of the solubilities and dissolution rates of several hydroxyapatites: Biomaterials, 2002; 23(3); 751-55
35. Zhang LH, Peng Y, Du CF, Tang PF, Biomechanical study of four kinds of percutaneous screw fixation in in two types of unilateral sacroiliac joint dislocation: A finite element analysis: Injury, 2014; 45(12); 2055-59
Figures
Figure 1. Transverse computed tomography (CT) scan of an 80-year-old woman with osteoporosis. There are obvious alar voids in both sacral alae, corresponding with a significant resorption of trabecular bone.Figure 2. Overall view of the TiRobot navigation system. It consists of a main console, tracking system, and robotic arm.Figure 3. A 67-year-old woman with injury from falling from a height. (A) The anteroposterior pelvic view reveals displaced superior and inferior pubic rami fractures on the right side, close to pubic symphysis. (B) Computed tomography (CT) construction scan of the pelvic ring demonstrates the overlapping superior and inferior pubic rami fracture and the compression sacral fracture due to the internal rotation of the pelvis. It concerns a type B1 lesion according to Tile classification on pelvic fracture. (C) The medial and lateral incisions of anterior pelvis ring. (D) Path planning of sacroiliac screw placement in S1 and S2. (E) Overall view of robot-aided sacroiliac screw manipulation. (F) Bone grafting via sacroiliac screw channel under C-arm fluoroscopy. There is a dense shadow in sacral ala, showing the injectable bone substitute. (G–I) Postoperative anteroposterior, inlet and outlet views. (J, K) Coronal and transverse CT views showing the positioning of the sacroiliac screw and the bone grafting. (L–O) Anteroposterior, inlet and outlet views and CT scan at 6 months after surgery showing the union of sacrum.Figure 4. A 75-year-old man with an injury from a car accident. (A) Computed tomography (CT) construction scan of the pelvic ring reveals the displaced pubic body and inferior pubic rami fracture associated with the ipsilateral sacral fracture. (B) Coronal CT scan showing the complete sacral fracture. (C) Intraoperative planning of sacroiliac screws after collection and transmission of the radiographs. (D) The view of robotic arm positioning at the entry point of sacroiliac screw. (E) The intraoperative picture demonstrating bone grafting injected along the channel of the sacroiliac screw. (F) Bone grafting along sacroiliac screw channel under C-arm fluoroscopy. (G–I) Intraoperative anteroposterior, inlet, and outlet views. (J–L) Postoperative coronal and transverse CT views revealing the satisfactory positioning of sacroiliac screws and the bone grafting. (M) The pelvic outlet view at 6 months after surgery showing that the fracture healed. Tables
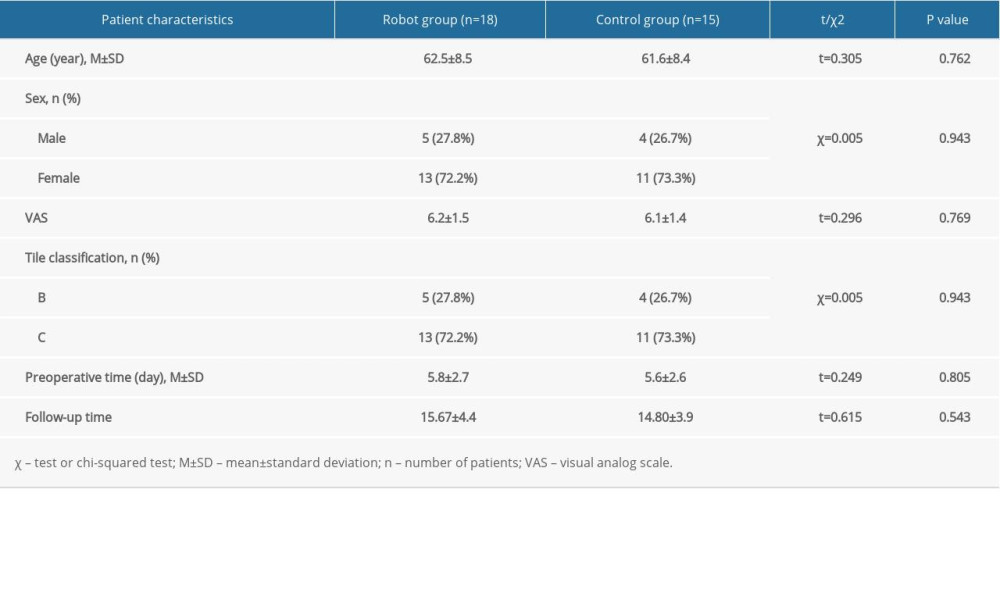 Table 1. The demographic data of the 2 groups.
Table 1. The demographic data of the 2 groups. Table 2. Perioperative clinical indicators of the 2 groups.
Table 2. Perioperative clinical indicators of the 2 groups. Table 3. Perioperative union rates of the 2 groups.Table 1. The demographic data of the 2 groups.Table 2. Perioperative clinical indicators of the 2 groups.Table 3. Perioperative union rates of the 2 groups.
Table 3. Perioperative union rates of the 2 groups.Table 1. The demographic data of the 2 groups.Table 2. Perioperative clinical indicators of the 2 groups.Table 3. Perioperative union rates of the 2 groups. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387