14 October 2021: Clinical Research
A Retrospective Study of Postoperative Outcomes in 98 Patients Diagnosed with Gastrointestinal Stromal Tumor (GIST) of the Upper, Middle, and Lower Gastrointestinal Tract Between 2009 and 2019 at a Single Center in Poland
Patryk Zemła1BCDEF*, Anna Stelmach1BEF, Beata Jabłońska2ADE, Dariusz Gołka3E, Sławomir Mrowiec2AEDOI: 10.12659/MSM.932809
Med Sci Monit 2021; 27:e932809






Abstract
BACKGROUND: Gastrointestinal stromal tumors (GISTs) arise in the smooth muscle pacemaker interstitial cells of Cajal, or similar cells. The aim of this retrospective study between 2009 and 2019 from a single center in Poland was to assess the selected prognostic factors (location, tumor size, mitotic index, body mass index (BMI), length of hospital stay, age, sex, and coexistent neoplasm) and to investigate postoperative outcomes in 98 patients with GIST of the upper, middle, and lower gastrointestinal tract.
MATERIAL AND METHODS: Between 2009 and 2019, 98 patients (50 women and 48 men) with an average age of 63.8 years (range from 38 to 90 years) were operated on for GIST in the Department of Gastrointestinal Surgery in Katowice, Poland. Based on the intraoperative and postoperative investigations, the tumor size and mitotic index were determined in each case.
RESULTS: A statistically significant correlation between age and mitotic index (MI) was found (p=0.02). The higher the MI, the younger the age of the patients. However, regardless of sex, younger patients had a tendency to survive longer. A >60-year-old male patient’s probability of survival was around 65% after 40 months. Higher mitotic index was also associated with larger tumor size (p<0.0001). Female patients had a tendency to survive longer than males.
CONCLUSIONS: The findings from this small retrospective study support the importance of preoperative evaluation and frequent postoperative follow-up for patients with GIST of the gastrointestinal tract, particularly in older male patients, and patients with malignant comorbidities, which are associated with increased mortality.
Keywords: Gastrointestinal Neoplasms, gastrointestinal stromal tumors, Medical Oncology, Age Factors, Aged, 80 and over, Disease-Free Survival, Elective Surgical Procedures, Female, Follow-Up Studies, Humans, Poland, Risk Assessment, Risk Factors, Sex Factors, Tumor Burden
Background
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumor located in the gastrointestinal (GI) tract [1]. Most studies have reported the incidence of clinically relevant GISTs at 10–15 per million population per year. GISTs are found most often in the stomach (56%), small bowel (32%), colon and rectum (6%), esophagus (0.7%), and other locations (5.5%) [2,3]. In very rare circumstances, GISTs appear outside of the gastrointestinal tract – they are called extra-gastrointestinal stromal tumors (eGIST) [4]. GISTs occurring outside of the stomach are associated with a higher malignant potential [5]. Gastrointestinal stromal tumors were originally believed to originate from the mesenchymal cells of the gastrointestinal tract [6]. In 1998 it was found that these tumors actually arise from the interstitial cells of Cajal or similar cells [7]. Most GISTs (>95%) stain positively for CD117 (c-KIT) protein [8]. Around 80% carry a mutation in the c-KIT gene or platelet-derived growth factor receptor-alpha (PDGFRA) gene, which code receptor tyrosine kinase mutations that can be targeted by small molecule pharmacological inhibitors [2].
The diagnosis of GIST can be confirmed by mutational analysis to identify known mutations in the PDGFRA and KIT genes, particularly in rare cases that are CD117-negative and DOG1-negative [9]. Mutational analysis has prognostic value and can predict sensitivity to molecular-targeted therapy [9]. For these reasons, current guidelines recommend the inclusion of mutational analysis as standard diagnostic practice for GIST cases [9]. GISTs are usually graded as benign, of uncertain malignant potential, and as malignant [10]. More aggressive GISTs may metastasize to different organs or tissues. They very rarely metastasize to lymph nodes [11]. It is worth noting that the American Joint Cancer Committee/Union for International Cancer Control (AJCC/UICC) grades GISTs separately from other sarcomas, using a two-grade system based on mitotic rate: of low grade (≤5 mitoses per 5 mm2 or per 50 high-power field (HPF)) and high grade (>5 mitoses per 5 mm2 or per 50 HPF) [12]. Current European Society for Medical Oncology (ESMO) guidelines suggest that the standard approach to patients with esophagogastric or duodenal nodules <2 cm is an endoscopic ultrasound assessment and then follow-up, reserving excision for patients whose tumor increases in size or becomes symptomatic [9]. The NCCN guidelines for GISTs recommend that prior to treatment, evaluation and management by a multidisciplinary sarcoma team is performed, including an abdominal/pelvic CT scan with contrast, with or without MRI. Very small gastric GISTs of <2 cm in diameter may be evaluated with endoscopic ultrasound-guided fine-needle aspiration. For GISTs of 2 cm or larger, endoscopy with or without ultrasound may also be indicated [12].
Surgical resection has always been a main treatment because of GISTs resistance to traditional chemotherapy and radiation [9,13,14]. Imatinib has been proven, however, as a very useful drug in selected neoadjuvant settings [9]. It inhibits both c-kit tyrosine kinase mutations and PDGFRA mutations other than D842V [15]. Genetic testing for specific KIT and PDGFRA mutations can predict the patient’s response to imatinib and the possible benefit of a higher imatinib dose. In case of imatinib resistance, sunitinib may be considered as a viable option [9,16]. Some GISTs express or gain resistance to both drugs [9]. In recent years, regorafenib was introduced as a third-line treatment [9,17–19]. The current NCCN treatment recommendations for localized resectable disease include surgical resection for gastric tumors <2 cm with no high-risk features and periodic endoscopic or radiographic surveillance. After complete resection, treatment with adjuvant imatinib is recommended, with follow-up history and physical examination and abdominal/pelvic CT every 3 to 6 months for 5 years, then annually [12].
Conflicting reports about the different clinical and histopathological factors affecting prognosis in patients with GIST have emerged [11,20–24]. Therefore, this retrospective study between 2009 and 2019 from a single center in Poland aimed to investigate postoperative outcomes and selected prognostic factors in 98 patients diagnosed with gastrointestinal stromal tumor (GIST) of the upper, middle, and lower gastrointestinal tract.
Material and Methods
ETHICS STATEMENT:
This was a retrospective study of medical records and all data were fully anonymized before we accessed them. Written informed consent was obtained from all participants. All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Our study is exempted from institutional review board (IRB) approval according to local legislation [25]. Only a medical experiment needs to obtain ethical approval, and a retrospective study including analysis of patients’ medical records does not need IRB approval.
DIAGNOSIS OF GIST:
Patients were diagnosed, treated, and monitored after the surgery according to current ESMO guidelines [9]. Multidisciplinary treatment planning was conducted, involving participation of a surgeon, gastroenterologist, radiologist, and oncologist. Prior to surgical treatment, radiological and endoscopic examinations (ultrasonography of the abdominal cavity, computed tomography and endoscopic investigations of the upper and lower gastrointestinal tract with tumor biopsy) were performed to check staging of the tumors in TNM classification according to the American Joint Committee on Cancer (AJCC) Staging Manual (7th and 8th edition) [26]. If necessary, positron emission tomography (PET) was also conducted. Immunohistochemical investigations of CD117, CD34, smooth muscle actin (SMA), and S-100 protein were carried out to differentiate between GISTs and other mesenchymal neoplasms. They were completed in the Department of Pathology, Medical University of Silesia, Katowice, Poland. Moreover, each patient with confirmed GIST in the above-mentioned examinations was consulted by an anesthesiologist to assess general health and risk of surgery, and to qualify for general anesthesia (taking into account all comorbidities).
PATIENTS’ CHARACTERISTICS:
Between 2009 and 2019, 98 consecutive patients (50 women and 48 men) with an average age of 63.8 years (range from 38 to 90 years) were operated on for GIST in the Department of Gastrointestinal Surgery Medical University of Silesia, Katowice, Poland.
MANAGEMENT OF GIST:
Patients with a locally advanced, resectable tumor (without distant metastases) with an acceptable perioperative risk were qualified for elective surgery. In case of tumor hemorrhage or rapture, patients were qualified for urgent surgery due to vital indications. Some tumors were found intraoperatively during surgery performed for a different reason. The aim of the surgical treatment was to obtain R0 resection (macroscopic and microscopic margins without tumor). The type of surgery depended on the location and diameter of the tumor. Based on the intraoperative and postoperative investigations, the tumor size and mitotic index were determined in each patient. GISTs were divided into 3 groups according to location within the gastrointestinal tract: (1) upper gastrointestinal tract (UGIT) – esophagus, stomach, duodenum; (2) middle gastrointestinal tract (MGIT) – jejunum and ileum; and (3) lower gastrointestinal tract (LGIT) – colon, rectum, and others. The tumor size cut-off point was decided to be 50 mm [11]. The mitotic index (MI), defined as the number of mitotic figures in 50 high-power fields (HPF), was assessed. We decided to divide it into 3 groups: A (0–1), B (2–9), and C (≥10). The patients were split into 2 age groups (≤60 years old or >60 years old). The duration of postoperative hospitalization ranged from 5 to 72 days (mean 14 days).
FOLLOW-UP:
Follow-up of patients was conducted by regular hospital visits and then at 3, 6, and 12 months, and yearly thereafter. Each assignment consisted of a physical examination, and selected imaging procedures were carried out (endoscopy, computed tomography, and laboratory investigations) based on the location, diameter, mitotic index, and the type of resection (R0/R1). In the case of GIST with high risk of recurrence, rectal location, or applied adjuvant chemotherapy (imatinib), additional chest X-ray every year was conducted. Thirty-three patients are lost to follow-up and were excluded from several analyses.
EVALUATION OF PATIENT OUTCOME:
The malignant potential of GISTs was categorized according to the Appelman and Helwig classification [27]. In addition, we stratified patients based on National Institute of Health (NIH) consensus criteria for GIST risk according to Fletcher et al [28,29].
STATISTICAL ANALYSIS:
Detailed descriptive analysis was performed. Correlation between sex, age, tumor location, mitotic index, tumor size, body mass index (BMI), length of hospitalization, coexistent neoplasm, imatinib treatment and survival of patients was assessed. Results were subjected to statistical analysis, where p<0.05 was considered to be significant. Univariate and multivariate survival analysis was performed. Survival curves were calculated applying the Kaplan-Meier method. Breslow hazard functions were applied and its use is shown in figures in order to handle patients lost to follow-up. The Breslow estimator was used to determine the cumulative baseline hazard function, which allowed the application of simple statistical transformations [30]. Confidence intervals (CI) were determined at the 95% level. We also calculated the risk of GIST recurrence based on GIST Risk Calculator, which is formed by research from Dr. Heikki Joensuu, Professor of Oncology at the University of Helsinki and the Research Director at the Helsinki Comprehensive Cancer Center, and his colleagues [31]. The study encompassed an international sample of 2000 diagnosed GIST patients, and analyzed them using a mathematical model designed by Professor Aki Vehtari of Aalto University. It takes into account tumor size, mitotic count, tumor site, and rupture. It is also worth noting that the data are solely comprised of patients that were treated via surgery alone. All calculations and statistical analysis were performed in IBM SPSS Statistics 26.
Results
SURGICAL TREATMENT:
There were numerous surgical procedures used in the study (Table 1). Surgical approach depended on the tumor location, size, and the prospect of complete resection. A wedge gastric excision was the most frequent surgical procedure (42.86%).
PATIENT CHARACTERISTICS:
The study group consisted of 50 (51.02%) men and 48 (48.98%) women, with a mean age of 63.8 (±10.6) years (range 38–90) (Table 2). Sixty-two patients (63.3%) were aged >60 years.
TUMOR LOCATION: Tumor characteristics are presented in Table 3. Eighty-two patients (83.7%) had tumors located in the UGIT, while only 2 (2%) were in the LGIT. Eight cases were detected in MGIT (Table 3). The stomach was the most prevalent location (71.4%) (Table 1). Thirty UGITs were found in the ≤60-year-old group, while 52 UGITs were in the >60 years group (Table 3). Significantly more MGITs were found in the >60 years population (6 vs 2).
TUMOR SIZE: The mean tumor size was 57 (±49) mm (3–240), and a neoplasm diameter ≥5 cm was discovered in 45 patients (45.9%) (Table 2). Mean tumor diameter in UGITs were found to be 56.2 (±47.6) mm, while in MGIT was 48.1 (±48.1) mm and LGIT was 57.5 (±17.7) mm (Table 3). Sixty percent of patients had ≤50 mean neoplasm size, whereas 40% of patients had >50 mean tumor size in the UGIT category.
TUMOR MITOTIC INDEX:
The mean MI was 5.19 (±7.95) HPF (0–44) and a MI ≥10/50 HPF was noted in 9 patients (9.2%). Twenty-seven patients (27.6%) had MI from 0 to 1. The largest group consisted of 61 patients (62.2%), and their MI ranged between 2 and 9 (Table 2). Low-risk GISTs, according to NIH classification, were the most common (34.02%), followed by high- (24.74%), intermediate- (23.71%), and very low-risk (17.53%) (Table 4). Fifteen (15.3%) patients had coexisting additional malignant neoplasms. Five of them had adenocarcinomas, while the others had different types of gastric or pancreas tumors.
CORRELATIONS BETWEEN CLINICAL AND PATHOLOGICAL PARAMETERS:
Data analysis (Table 5) showed a statistically significant correlation between age and mitotic index (p=0.02). Higher mitotic index was correlated with younger age of the patients. Higher MI was also tied with larger tumors (p<0.001) (Figure 1). Other correlations worth noting exist between length of hospitalization, mitotic index, and tumor diameter (the higher index and larger tumor, the longer the hospital stay (p=0.148 and p=0.277, respectively), as well as age and tumor size (the bigger the size, the younger the age (p=0.233) although they were not statistically significant (p<0.05 was considered to be significant).
SURVIVAL ANALYSIS:
Among the 98 operated patients, long-term postoperative follow-up was performed in 60 of them (61.22%). The mean overall survival (OS) was 57.03 (±36.29) months (3–123). Seven patients died during the follow-up period due to various causes (disease progression, cardiovascular disorders, cerebral stroke). Another 2 deaths occurred shortly after surgery due to postoperative complications. We found a correlation between survival and coexistence of additional neoplasm (n=15). In patients with coexisting tumors, the chance for survival after 39 months was 58%, while in the absence of additional neoplasm it was 88% (Figure 2). Furthermore, as these Breslow hazard functions show (Figure 3) (p<0.05), there is a strong relationship between sex in different age groups and their survival time. Female patients under the age of 60 had a 97.5% chance for survival after 39 months, while those at the age of 60 or above had 86% chance. However, male patients under the age of 60 had a 93% chance to be alive while those 60 years and older had only a 63% chance for survival.
Discussion
The most common site of GIST in our study was the stomach. There was no correlation between tumor site and mitotic index (p=0.572) or size (p=0.778). A larger tumor was associated with a higher mitotic index (p<0.0001). We also found a correlation between mitotic index and age of the patients. The younger patient’s age was correlated with the higher tumor mitotic index. The age was correlated only with mitotic index (p=0.02), while a relationship between age and tumor primary location (p=0.495) or size (p=0.233) was not found. Male sex was the strongest poor prognostic factor in patients with GISTs. There was no statistically significant correlation between patient’s sex and tumor primary location (p=0.512), mitotic index (p=0.786), or size (p=0.951). Body mass index (BMI) did not influence OS or disease-free survival (DSF), and its correlation with tumor primary location (p=0.615), mitotic index (p=0.674), and size (p=0.873) was not significant (Table 5). In our study, length of hospital stay did not correlate with OS, DFS. There was no correlation between length of hospital stay and tumor primary location (p=0.944), mitotic index (p=0.148), or size (p=0.277). There was a very significant correlation between coexistence of the other malignant neoplasm and probability of survival in our patients (p<0.001).
The most common site of GIST in our study was the stomach, which is in keeping with most clinical reports [3,20,32–34]. The question still remains, is tumor location of any significance as a prognostic factor? Some studies insist that it does [1,20,21,32–42], while others say it does not hold any statistical relevance [43–47]. Our data correspond more to the latter one. In addition, there is some evidence in the literature that supports gastric location as a positive prognostic factor [32]. Our analysis shows that there is no strong indication that would suggest a correlation between tumor site and its mitotic index (p=0.572) or size (p=0.778).
There are numerous studies trying to define a threshold of tumor diameter for its recurrence and/or malignant behavior. For example, some analyses give 10 cm as a cut-off point [47], while others use 5 cm [11,33] and there are some that go as low as 3 cm [48]. In 2002 [28], Fletcher and his colleagues collaborated to create the NIH (National Institute of Health) classification, the first GIST grading system taking into account tumor diameter and its mitotic activity, thus determining the risk of recurrence. The Appelman and Helwig [27] categorization system reported that the odds of malignant probability increase in tumors of diameter over 60 mm. Our analysis did not find this correlation, however; it pointed out that the larger the tumor, the higher its mitotic index (p<0.0001), which indirectly means higher malignant potential (Figure 1). Many studies indicated tumor size as an adverse factor in patients with GISTs [2,8,21,28,32,36,38–40,43,45–47,49,50]. Some studies point out mitotic index as one of the main determinants [2,8,11,20,21,28,32,36, 38,39,41–44,46,47,49]. We found a correlation between mitotic index and age of the patients. The younger the patient, the higher tumor’s mitotic index (Table 5, Figure 4).
The association between the most frequent poor prognostic factors and survival in patients with GISTs in the recent literature is shown in Table 6.
Elderly people tend to have higher incidence rates of the tumor [28]. Age is one of the more controversial topics concerning GISTs survival rates and as its prognostic factor. Some studies indicate that it does not affect it in any way [20,50], while others consider it as a possible prognostic aspect [1,21,32,33,38,42]. Among those, a few state that younger age tends to be more problematic [42], while others claim the exact opposite [33]. We decided to divide our patients into 2 groups based on their age, with a 60-year-old threshold. Thirty-three of them were 60 years old or younger, while 59 were over 60 years old. Our analysis points out that younger patients have longer OS (Figure 3) and mitotic index is also higher. It is, however, an outlier in comparison to other studies (Figure 4). It may suggest more aggressive behavior of tumors in younger patients. Potential risk factors such as primary location, tumor diameter, and mitotic index varied significantly between the different age groups. However, age itself (without subdividing into different age groups) correlated only with mitotic index (p=0.02), while no relationship between age and tumor primary location (p=0.495) or size (p=0.233) was found (Table 5).
In our study, male sex was the strongest poor prognostic factor in patients with GISTs. Their survival rate was at a significantly lower level than in females, regardless of age. However, the difference is most striking in the group over 60 years old (Figure 3). This is in line with some previous studies [20,42]. It is worth mentioning that there is one paper that suggests that it does not matter [36] and one that suggests that male sex increases survival rates [33]. It is, however, an outlier, and Cox proportional hazards model does not support univariate analysis in this case. There was no statistically significant correlation between sex and tumor primary location (p=0.512), mitotic index (p=0.786), or its size (p=0.951) (Table 5).
Body mass index (BMI) is one of the basic clinical parameters that is being included in clinical studies. With the general population getting more and more obese [58,59], an analysis regarding its significance as a prognostic factor needed to be done. It has not been reported in the literature. Our research shows that it does not influence OS or disease-free survival (DSF) and its correlation with tumor primary location (p=0.615), mitotic index (p=0.674), and size (p=0.873) is not significant (Table 5).
Length of hospital stay as a prognostic factor is another important topic that is not discussed in the literature. Our study shows that it does not correlate with overall survival or disease-free survival, and it is not significantly correlated with tumor primary location (p=0.944), mitotic index (p=0.148), or size (p=0.277) (Table 5).
Coexisting neoplasms in patients with GISTs are fairly common [60], and occur in 2.95–33.33% of cases. It occurred in 15 (15.31%) of our patients. Analysis reveals that there is a very significant correlation between coexistence of the other malignant neoplasm and probability of survival (Figure 2) (p<0.001). In patients with coexisting tumors, the probability of survival beyond 39 months was 58%, while in the absence of additional neoplasm it was 88%. Additional tumors are most frequently found in the stomach [61]. Our data confirm these findings, although it is worth noting there were several tumors located in the pancreas. There is little evidence of the coexistence of the other neoplasm as a prognostic factor in patients with GISTs [20,62]. Some studies have assessed the occurrence, clinicopathology, epidemiology, immunohistochemical analysis, and treatment of GISTs coexisting with other malignant neoplasms [61,62]. Sometimes GISTs appear in groups [63].
We also calculated risk of GIST recurrence based on GIST Risk Calculator, which was formed by research from Dr. Heikki Joensuu, Professor of Oncology at the University of Helsinki and the Research Director at the Helsinki Comprehensive Cancer Center, and his colleagues [31]. The study encompassed an international sample of 2000 diagnosed GIST patients, and analyzed them using a mathematical model designed by Professor Aki Vehtari of Aalto University. It takes into account tumor size, mitotic count, tumor site, and rupture. It is also worth noting that the data are solely comprised of patients that were treated via surgery alone. In our study the chance of recurrence after 5 and 10 years was 22.32% and 28.49%, respectively, without taking into account so-called “low risk” tumors. Low-risk tumors, according to the calculator, are those with a chance of recurrence lower than 1%. If we take them into account as well (counting them as a 0.5% chance of recurrence on average), median risk drops to 18.19% and 24.13%, respectively.
Results of imatinib use show that this drug is highly effective, especially with non-resectable or high-risk GISTs [2,8,32,36–39,45]. In intermediate-risk GISTs, however, some studies indicate that imatinib adjuvant therapy does not add any significant benefits for the patients [64] while others claim that it does [65,66]. A study suggested neo-adjuvant therapy should be used before surgery in advanced GISTs [67].
In our study, 9 patients were treated with imatinib (Gleevec), and the sample size was not large enough to determine any statistical significance.
There are some limitations to our research. It was a single-center retrospective study and it was restricted to 98 patients. There may be some bias that could have been introduced by the long duration of the study. Some data were not available, as in another retrospective studies. Some of the material was insufficient for proper statistical analysis (for example, the imatinib use).
Conclusions
INSTITUTIONAL REVIEW BOARD STATEMENT:
This was a retrospective study of medical records and all data were fully anonymized before we accessed them. Written informed consent was obtained from all participants. All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
DATA AVAILABILITY STATEMENT:
The data that support the findings of this study are openly available in Kaggle at
Figures
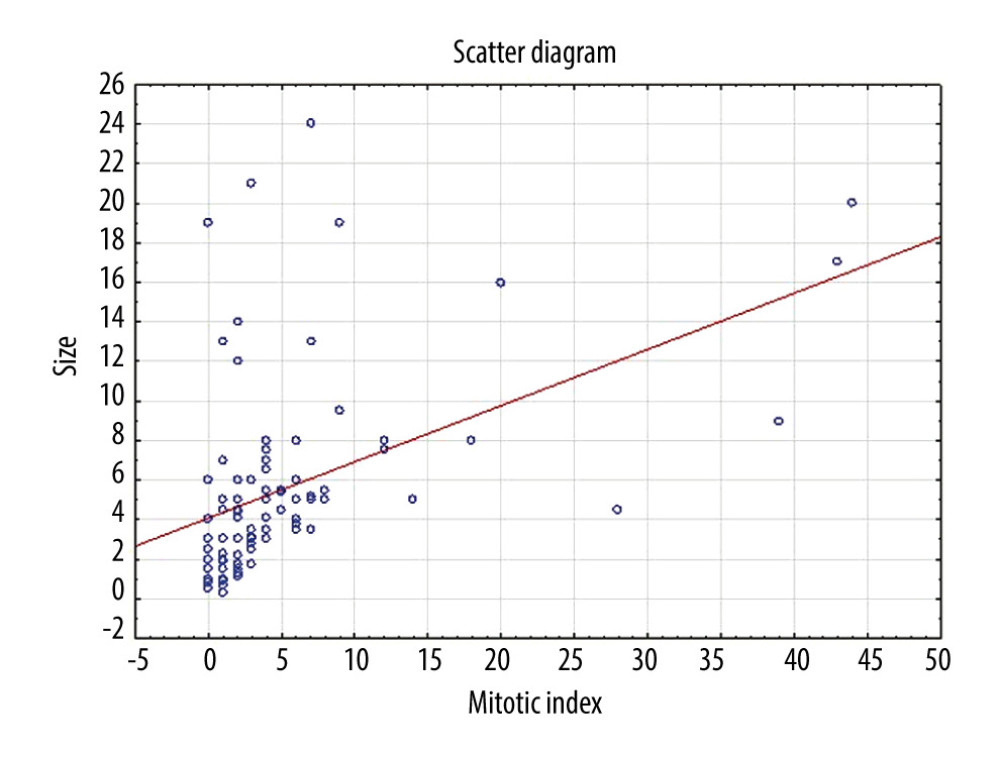 Figure 1. Scatter diagram shows correlation between Mitotic Index and size of the tumors.
Figure 1. Scatter diagram shows correlation between Mitotic Index and size of the tumors. 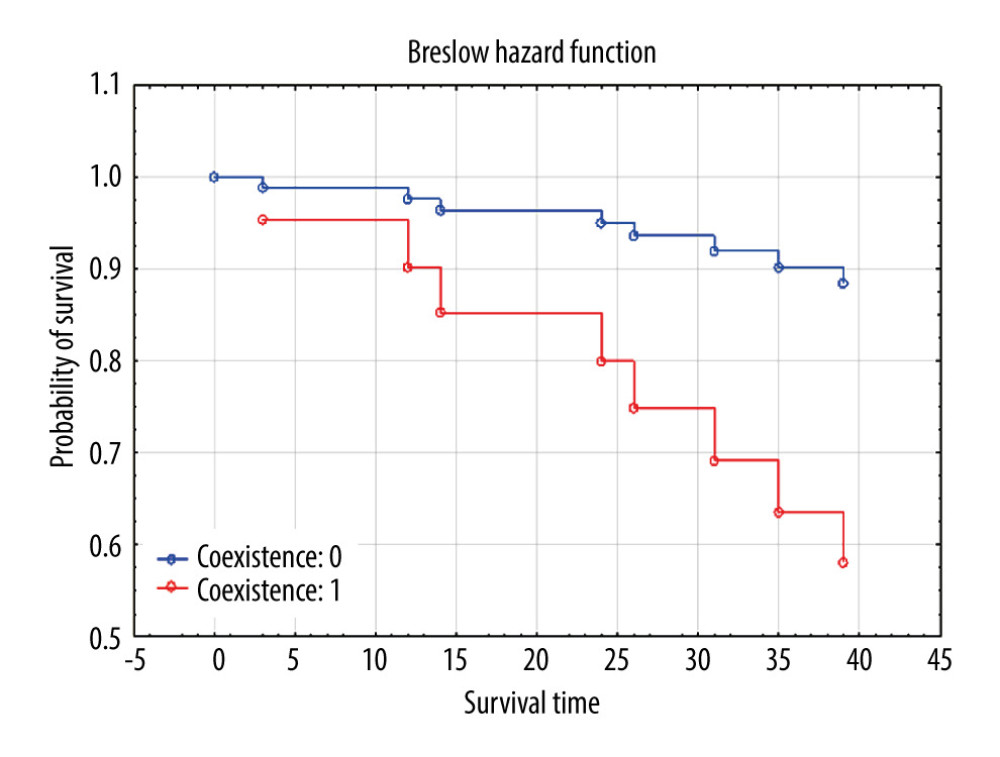 Figure 2. Breslow hazard function demonstrates the difference in probability of survival between patients with and without coexisting neoplasm after certain time.
Figure 2. Breslow hazard function demonstrates the difference in probability of survival between patients with and without coexisting neoplasm after certain time. 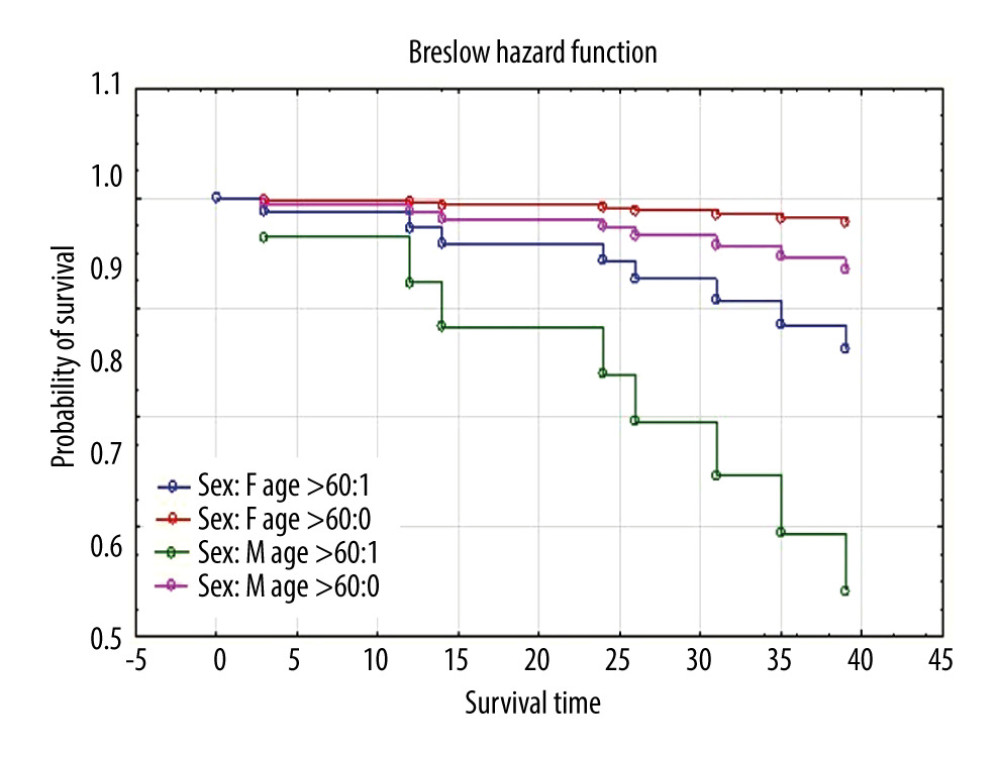 Figure 3. Breslow hazard function shows the difference in probability of survival between different age groups and sexes in time.
Figure 3. Breslow hazard function shows the difference in probability of survival between different age groups and sexes in time. 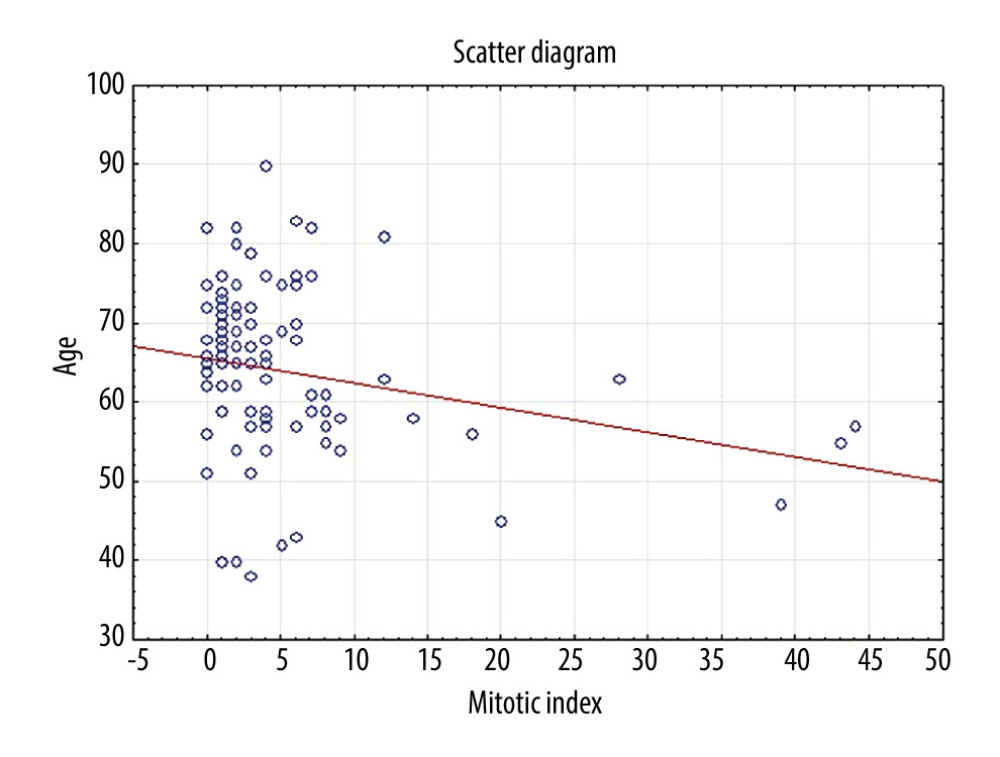 Figure 4. Scatter diagram displays correlation between mitotic index and age of the patients.
Figure 4. Scatter diagram displays correlation between mitotic index and age of the patients. Tables
Table 1. Surgical procedures and tumor location (n=98*).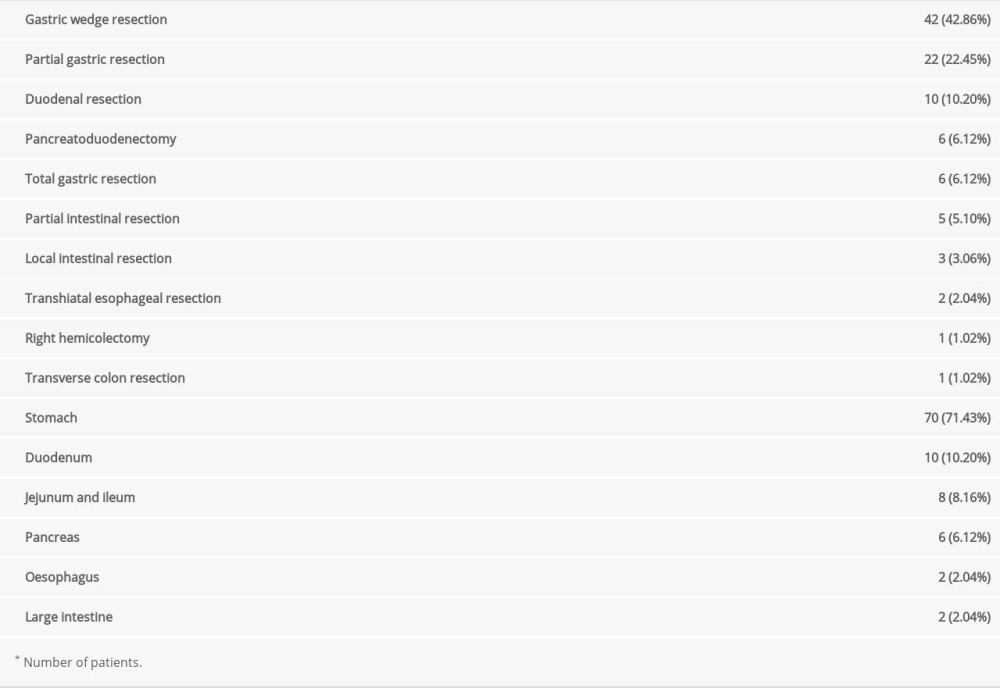 Table 2. Patient and tumor characteristics (n=98*).
Table 2. Patient and tumor characteristics (n=98*). Table 3. Tumor characteristics (division into groups) (n=92*).
Table 3. Tumor characteristics (division into groups) (n=92*). Table 4. Tumor characteristics: National Institute of Health classification and tumor location within the gastrointestinal tract (n=92*).
Table 4. Tumor characteristics: National Institute of Health classification and tumor location within the gastrointestinal tract (n=92*).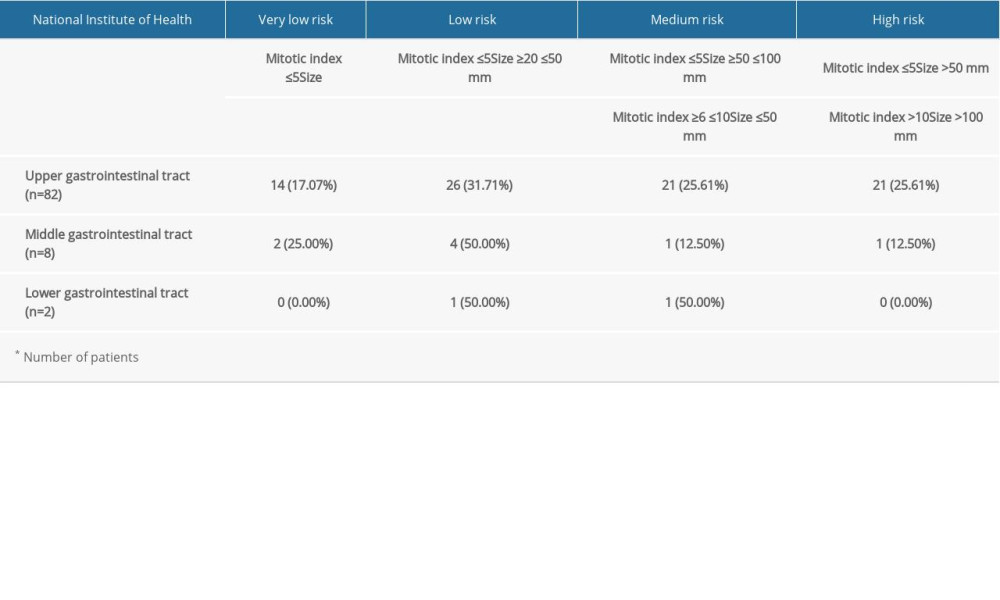 Table 5. Correlations between clinical and pathological parameters (n=98*).
Table 5. Correlations between clinical and pathological parameters (n=98*). Table 6. Association between the most common poor prognostic factors and survival in patients with Gastrointestinal stromal tumors (GISTs) in the recent literature (2009–2018).
Table 6. Association between the most common poor prognostic factors and survival in patients with Gastrointestinal stromal tumors (GISTs) in the recent literature (2009–2018).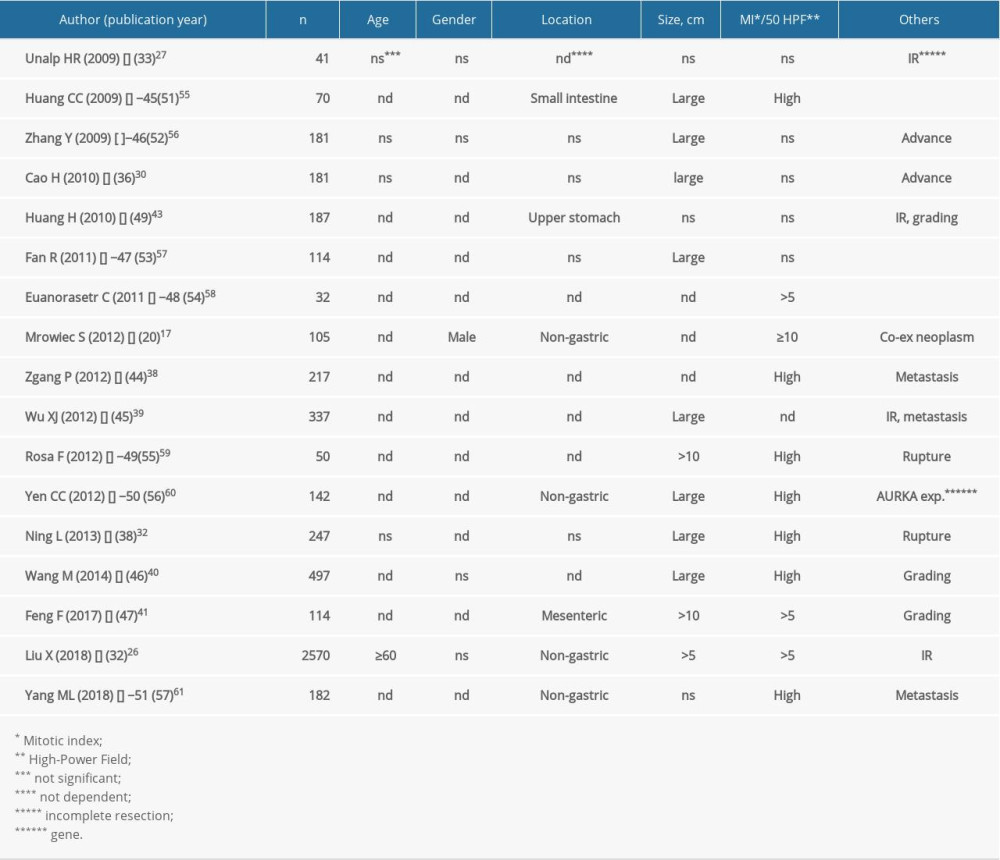
References
1. Rabin I, Chikman B, Lavy R, Gastrointestinal stromal tumors: A 19-year experience: Isr Med Assoc J, 2009; 11(2); 98-102
2. Sanchez-Hidalgo JM, Duran-Martinez M, Molero-Payan R, Gastrointestinal stromal tumors: A multidisciplinary challenge: World J Gastroenterol, 2018; 24(18); 1925-41
3. Søreide K, Sandvik OM, Søreide JA, Global epidemiology of gastrointestinal stromal tumours (GIST): A systematic review of population-based cohort studies: Cancer Epidemiol, 2016; 40; 39-46
4. Miettinen M, Sobin LH, Lasota J, Gastrointestinal stromal tumors presenting as omental masses – a clinicopathologic analysis of 95 cases: Am J Surg Pathol, 2009; 33; 1267-75
5. Miettinen M, Lasota J, Gastrointestinal stromal tumors: Review on morphology, molecular pathology, prognosis, and differential diagnosis: Arch Pathol Lab Med, 2006; 130(10); 1466-78
6. Mazur MT, Clark HB, Gastric stromal tumors. Reappraisal of histogenesis: Am J Surg Pathol, 1983; 7(6); 507-19
7. Kindblom LG, Remotti HE, Aldenborg F, Meis-Kindblom JM, Gastrointestinal pacemaker cell tumor (GIPACT): Gastrointestinal stromal tumors show phenotypic characteristics of the interstitial cells of Cajal: Am J Pathol, 1998; 152(5); 1259-69
8. Parab TM, DeRogatis MJ, Boaz AM, Gastrointestinal stromal tumors: A comprehensive review: J Gastrointest Oncol, 2019; 10(1); 144-54
9. Casali PG, Abecassis N, Aro HTESMO Guidelines Committee and EURACAN, Gastrointestinal stromal tumours: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up: Ann Oncol, 2018; 29(Suppl 4); iv68-78
10. Fletcher CDM, Bridge JA, Hogendoorn P, Mertens F: World Health Organization Classification of Tumours of Soft Tissue and Bone, 2013, Lyon, France, IARC
11. DeMatteo RP, Lewis JJ, Leung D, Two hundred gastrointestinal stromal tumors: Recurrence patterns and prognostic factors for survival: Ann Surg, 2000; 231; 51-58
12. National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Gastrointestinal Stromal Tumors (GISTs). Version 1.2021 October 30, 2020 https://www.nccn.org/professionals/physician_gls/pdf/gist.pdf
13. Corbin KS, Kindler HL, Liauw SL, Considering the role of radiation therapy for gastrointestinal stromal tumor: Onco Targets Ther, 2014; 7; 713-18
14. Kantarjian HM, Wolff RA, Koller CA: The MD Anderson Manual of Medical Oncology, 2011; 1122, McGraw-Hill
15. : NCCN Clinical Practice Guidelines in Oncology Soft Tissue Sarcomas, version 3, 2012; 23, National Comprehensive Cancer Network
16. Okuno S, The Use of tyrosine kinase inhibitors for gastrointestinal stromal tumors (GIST): Contemporary Oncology Sep 14, 2011
17. Nilsson B, Nilsson O, Ahlman H, Treatment of gastrointestinal stromal tumours: Imatinib, sunitinib – and then?: Expert Opin Investig Drugs, 2009; 18(4); 457-68
18. Overton LC, Heinrich MC, Regorafenib for treatment of advanced gastrointestinal stromal tumors: Expert Opin Pharmacother, 2014; 15(4); 549-58
19. Khoshnood A, Gastrointestinal stromal tumor – A review of clinical studies: J Oncol Pharm Pract, 2019; 25(6); 1473-85
20. Mrowiec S, Jabłońska B, Liszka L, Prognostic factors for survival post surgery for patients with gastrointestinal stromal tumors: Eur Surg Res, 2012; 48(1); 3-9
21. Ge XY, Lei LW, Ge F, Jiang X, Analysis of risk factors of gastrointestinal stromal tumors in different age groups based on SEER database: Scand J Gastroenterol, 2019; 54(4); 480-84
22. Yang Z, Feng X, Zhang PChina Gastrointestinal Stromal Tumor Study Group (CN-GIST), Clinicopathological features and prognosis of 276 cases of primary small (≤2 cm) gastric gastrointestinal stromal tumors: A multicenter data review: Surg Endosc, 2019; 33(9); 2982-90
23. Liu Q, Wang Y, Kong L, Kan Y, Study on clinicopathological features of gastrointestinal stromal tumor and relevant prognostic factors: Cell Biochem Biophys, 2015; 73(3); 743-47
24. Mrowiec S, Jabłońska B, Leidgens M, Influence of location and mitotic index on prognosis in patients with gastrointestinal stromal tumors: Pol Przegl Chir, 2008; 80(6); 569-45
25. http://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU19990470480/T/D19990480L.pdf
26. Edge SB, Compton CCThe American Joint Committee on Cancer
27. Appelman HD, Helwig EB, Sarcomas of the stomach: Am J Clin Pathol, 1977; 67; 2-10
28. Fletcher CD, Berman JJ, Corless C, Diagnosis of gastrointestinal stromal tumors: A consensus approach: Hum Pathol, 2002; 33(5); 459-65
29. Zhao B, Zhang J, Mei D, The assessment of different risk classification systems for gastrointestinal stromal tumors (GISTs): The analytic results from the SEER database: Scand J Gastroenterol, 2018; 53(10–11); 1319-27
30. Lin DY, On the Breslow estimator: Lifetime Data Anal, 2007; 13; 471-80
31. Joensuu Heikki: GIST Risk Calculator http://www.gistrisk.com
32. Liu X, Qiu H, Zhang PChina Gastrointestinal Stromal Tumor Study Group (CN-GIST), Prognostic factors of primary gastrointestinal stromal tumors: A cohort study based on high-volume centers: Chin J Cancer Res, 2018; 30(1); 61-71
33. Unalp HR, Derici H, Kamer E, Gastrointestinal stromal tumours: Outcomes of surgical management and analysis of prognostic variables: Can J Surg, 2009; 52(1); 31-38
34. Sakin A, Can O, Arici S, Factors affecting disease-free survival in operated nonmetastatic gastrointestinal stromal tumors: J Surg Res, 2019; 241; 170-77
35. Li Y, Tan B, Wu H, The risk factors about prognosis of 142 GIST patients with recurrence or metastasis: A retrospective study of single centre in Northern China: J Buon, 2018; 23(6); 1855-61
36. Cao H, Zhang Y, Wang M, Prognostic analysis of patients with gastrointestinal stromal tumors: A single unit experience with surgical treatment of primary disease: Chin Med J (Engl), 2010; 123(2); 131-36
37. Yang HX, Chen HN, Zhang BPrognostic analysis of 349 cases with gastrointestinal stromal tumor: Sichuan Da Xue Xue Bao Yi Xue Ban, 2013; 44(1); 155-58 [in Chinese]
38. Ning L, Zhang DF, Zhou YBPrognosis analysis of 247 cases of gastrointestinal stromal tumor: Zhonghua Wei Chang Wai Ke Za Zhi, 2013; 16(3); 247-50 [in Chinese]
39. Cavnar MJ, Seier K, Curtin C, Outcome of 1000 patients with gastrointestinal stromal tumor (GIST) treated by surgery in the pre and post-imatinib eras: Ann Surg, 2019; 273(1); 128-38
40. Zhu L, Khan S, Hui Y, Treatment recommendations for small gastric gastrointestinal stromal tumors: Positive endoscopic resection: Scand J Gastroenterol, 2019; 54(3); 297-302
41. Rutkowski P, Nowecki ZI, Michej W, Risk criteria and prognostic factors for predicting recurrences after resection of primary gastrointestinal stromal tumor: Ann Surg Oncol, 2007; 14; 2018-27
42. Rutkowski P, Debiec-Rychter M, Nowecki ZI, Different prognostic factors are responsible for predicting relapses after primary tumors resection and for imatinib treatment outcomes in gastrointestinal stromal tumors: Med Sci Monit, 2007; 13; 515-22
43. Krajinovic K, Germer CT, Agaimy A, Outcome after resection of one hundred gastrointestinal stromal tumors: Dig Surg, 2010; 27(4); 313-19
44. Zhang P, Zheng WQ, Tao KXClinical analysis of 217 patients with gastrointestinal stromal tumor: Zhonghua Wei Chang Wai Ke Za Zhi, 2012; 15(3); 251-54 [in Chinese]
45. Wu XJ, Zhang RX, Chen G, Prognostic factors in surgically managed gastrointestinal stromal tumours: J Int Med Res, 2012; 40(5); 1904-11
46. Wang M, Xu J, Zhang Y, Gastrointestinal stromal tumor: 15-years’ experience in a single center: BMC Surg, 2014; 14; 93
47. Feng F, Feng B, Liu S, Clinicopathological features and prognosis of mesenteric gastrointestinal stromal tumor: Evaluation of a pooled case series: Oncotarget, 2017; 8(28); 46514-22
48. Zhong YX, Zhou ZX, Pei WRisk factors and surgical treatment of recurrent gastrointestinal stromal tumor in the rectum: Zhonghua Wei Chang Wai Ke Za Zhi, 2008; 11(6); 545-57
49. Huang H, Liu YX, Zhan ZL, Liang H, Different sites and prognoses of gastrointestinal stromal tumors of the stomach: Report of 187 cases: World J Surg, 2010; 34(7); 1523-33
50. Bülbül Doğusoy GTurkish GIST Working Group, Gastrointestinal stromal tumors: A multicenter study of 1160 Turkish cases: Turk J Gastroenterol, 2012; 23(3); 203-11
51. Huang CC, Yang CY, Lai IR, Gastrointestinal stromal tumor of the small intestine: A clinicopathologic study of 70 cases in the postimatinib era: World J Surg, 2009; 33(4); 828-34
52. Zhang Y, Cao H, Wang MAnalysis of clinicopathology and prognosis in 181 patients with gastrointestinal stromal tumors: Zhonghua Wei Chang Wai Ke Za Zhi, 2009; 12(2); 150-54
53. Fan R, Zhong J, Wang ZT, Prognostic factors and outcome of resected patients with gastrointestinal stromal tumors of small intestine: Med Oncol, 2011; 28(Suppl 1); S185-88
54. Euanorasetr C, Outcomes and prognostic factors of primary gastric GIST following complete surgical resection: A single surgeon experience: J Med Assoc Thai, 2011; 94(1); 55-64
55. Rosa F, Alfieri S, Tortorelli AP, Gastrointestinal stromal tumors: Prognostic factors and therapeutic implications: Tumori, 2012; 98(3); 351-56
56. Yen CC, Yeh CN, Cheng CT, Integrating bioinformatics and clinicopathological research of gastrointestinal stromal tumors: Identification of aurora kinase A as a poor risk marker: Ann Surg Oncol, 2012; 19(11); 3491-99
57. Yang ML, Wang JC, Zou WB, Yao DK, Clinicopathological characteristics and prognostic factors of gastrointestinal stromal tumors in Chinese patients: Oncol Lett, 2018; 16(4); 4905-14
58. Wright SM, Aronne LJ, Causes of obesity: Abdom Imaging, 2012; 37(5); 730-32
59. Zdrojowy-Wełna A, Zatońska K, Bednarek-Tupikowska G, Determinants of obesity in population of PURE study from Lower Silesia: Endokrynol Pol, 2018; 69(6); 644-52
60. Murphy JD, Ma GL, Baumgartner JM, Increased risk of additional cancers among patients with gastrointestinal stromal tumors: A population-based study: Cancer, 2015; 121(17); 2960-67
61. Liszka Ł, Zielińska-Pająk E, Pająk J, Coexistence of gastrointestinal stromal tumors with other neoplasms: J Gastroenterol, 2007; 42; 641-49
62. Liu Z, Liu S, Zheng G, Clinicopathological features and prognosis of coexistence of gastric gastrointestinal stromal tumor and gastric cancer: Medicine (Baltimore), 2016; 95(45); e5373
63. Li K, Tjhoi W, Shou C, Multiple gastrointestinal stromal tumors: Analysis of clinicopathologic characteristics and prognosis of 20 patients: Cancer Manag Res, 2019; 11; 7031-38
64. Fu Y, Hao H, Guo L, Retrospective analysis of 85 cases of intermediate-risk gastrointestinal stromal tumor: Oncotarget, 2017; 8(6); 10136-44
65. Li J, Gong JF, Wu AW, Shen L, Post-operative imatinib in patients with intermediate or high risk gastrointestinal stromal tumor: Eur J Surg Oncol, 2011; 37(4); 319-24
66. Wu X, Li J, Xu W, Postoperative imatinib in patients with intermediate risk gastrointestinal stromal tumor: Future Oncol, 2018; 14(17); 1721-29
67. Doyon C, Sidéris L, Leblanc G, Prolonged therapy with imatinib mesylate before surgery for advanced gastrointestinal stromal tumor results of a phase II trial: Int J Surg Oncol, 2012; 2012; 761576
Figures
Figure 1. Scatter diagram shows correlation between Mitotic Index and size of the tumors.Figure 2. Breslow hazard function demonstrates the difference in probability of survival between patients with and without coexisting neoplasm after certain time.Figure 3. Breslow hazard function shows the difference in probability of survival between different age groups and sexes in time.Figure 4. Scatter diagram displays correlation between mitotic index and age of the patients. Tables
Table 1. Surgical procedures and tumor location (n=98*).Table 2. Patient and tumor characteristics (n=98*).Table 3. Tumor characteristics (division into groups) (n=92*).Table 4. Tumor characteristics: National Institute of Health classification and tumor location within the gastrointestinal tract (n=92*).Table 5. Correlations between clinical and pathological parameters (n=98*).Table 6. Association between the most common poor prognostic factors and survival in patients with Gastrointestinal stromal tumors (GISTs) in the recent literature (2009–2018).Table 1. Surgical procedures and tumor location (n=98*).Table 2. Patient and tumor characteristics (n=98*).Table 3. Tumor characteristics (division into groups) (n=92*).Table 4. Tumor characteristics: National Institute of Health classification and tumor location within the gastrointestinal tract (n=92*).Table 5. Correlations between clinical and pathological parameters (n=98*).Table 6. Association between the most common poor prognostic factors and survival in patients with Gastrointestinal stromal tumors (GISTs) in the recent literature (2009–2018). In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387