10 February 2022: Clinical Research
A Single-Center, Randomized, Double-Blind Study of 94 Patients Undergoing Surgery for Cerebral Glioma to Compare Postoperative Thromboprophylaxis with and without Rivaroxaban
Zi-Yan Wang1ABC, You-Dong Wan2CDEF, Xian-Zhi Liu1EFG, Hao Wang1AD, Guang-Yi Jiang1ABF, Bo Yang1ABCDEFG*DOI: 10.12659/MSM.934341
Med Sci Monit 2022; 28:e934341






Abstract
BACKGROUND: Venous thrombosis (VTE) is a common adverse event among inpatients, which can cause pulmonary embolism, and greatly increases mortality. The effects of rivaroxaban in patients undergoing brain glioma surgery have still not been explored. This single-center study of 94 patients undergoing surgery for cerebral glioma aimed to compare postoperative thromboprophylaxis with and without rivaroxaban.
MATERIAL AND METHODS: We designed a randomized, controlled, double-blind study to evaluate the effect of rivaroxaban on 94 patients undergoing brain glioma surgery. These patients were divided into a rivaroxaban group (administered at 10 mg per day from admission to discharge) and a placebo group. The primary study endpoint was incidence of VTE at discharge. The secondary endpoints included safety outcomes of major bleeding, allergy, or VTE-related death.
RESULTS: A total of 94 patients were enrolled in the study: 47 in the rivaroxaban group and 47 in the placebo group. Baseline characteristics of participants were well-matched in both groups. A significant reduction was found in the incidence of VTE in the rivaroxaban treatment group versus the placebo group (1/47 vs 10/47 patients, P=0.008). The rate of major bleeding events was quite low in both group (1/47 vs 1/47 patients). One patient in the placebo group died due to a pulmonary embolism and intractable concomitant underlying diseases.
CONCLUSIONS: Our results indicate that treatment with rivaroxaban is a safe and effective thromboprophylaxis treatment in patients undergoing surgery for malignant cerebral glioma.
Keywords: Neurosurgery, Rivaroxaban, Venous Thrombosis, Glioma, Brain Neoplasms, Double-Blind Method, Factor Xa Inhibitors, Humans, Postoperative Complications, venous thromboembolism
Background
Venous thromboembolism (VTE) is a common adverse event among inpatients, and immobilized patients are more likely to develop VTE [1]. Thrombus formation can cause pulmonary embolism (PE), which greatly increases the mortality of hospitalized patients [1]. Patients with brain tumors are at an even higher risk of VTE because of neurological dysfunction, particularly limb movement disorders, and hypercoagulability [1]. Khaldi et al [2] examined 555 high-risk neurosurgical patients and found that the VTE incidence rate in the first week of hospitalization was 49%; furthermore, even after using mechanical deep-vein thrombosis (DVT) prophylaxis, the incidence rate remained at 16%. Glioma is the most common intracranial tumor, accounting for approximately 80% of all central nervous system malignancies [3]. Patients with malignant glioma with VTE had a 30% increased risk of death within 2 years, making VTE the second leading cause of mortality, second only to death owing to cancer itself [4]. Thus, considering the high incidence of VTE and its associated mortality, thromboprophylaxis, especially for patients confined to bed after glioma surgery, has become an urgent problem.
Mechanical assist devices and anticoagulants are the main prophylactic modalities used [5]. However, because of the inefficiency of mechanical assist devices, drug prevention and VTE treatment are the current standard of care [6]. Unfractionated heparin, low-molecular-weight heparin (LMWH), warfarin, and novel oral anticoagulants such as rivaroxaban are recommended for the initial prevention and treatment of VTE [6]. Rivaroxaban has the following advantages: it can be administered orally without intravenous administration, it does not require frequent laboratory monitoring, and its dose adjustments are rarely necessary [7]. All the aforementioned agents can effectively prevent VTE after orthopedic surgery or atrial fibrillation [8,9]. However, because of limited evidence in the patients with brain glioma, the use of rivaroxaban is limited. Considering the potential benefits of rivaroxaban in preventing VTE, we hypothesized that rivaroxaban can decrease the risk of VTE in patients undergoing brain glioma surgery. Therefore, this study of 94 patients undergoing surgery for cerebral glioma was conducted at a single center and aimed to compare postoperative thromboprophylaxis with and without rivaroxaban.
Material and Methods
INCLUSION AND EXCLUSION CRITERIA:
Adults admitted to the hospital for brain glioma surgery were eligible for enrollment. Patients aged ≥18 years signed a dated informed consent form. They also needed to have an intended treatment duration of at least 7 days and no signs of VTE at the time of hospitalization. Patients with contraindications to rivaroxaban, mainly including those with clinically significant active bleeding, those with liver cirrhosis reaching Child Pugh grades B and C, those with severe renal insufficiency, or pregnant and lactating women, were excluded. Patients with recent intracranial hemorrhages, intracranial arteriovenous malformations, and vascular aneurysms were also excluded. Patients considered by surgeons to have complex intracranial conditions during surgery, resulting in high risk of postoperative intracranial hemorrhage, were also excluded. Additionally, patients taking antiplatelet or anticoagulant drugs, including aspirin, clopidogrel, or warfarin, were excluded.
DATA COLLECTION:
We collected the clinical data of patients after they signed the informed consent and authorization form. We collected basic medical data such as sex, age, body mass index (BMI), platelets, hemoglobin, brain glioma histological findings, medical history, World Health Organization (WHO) glioma grade, and therapeutic and diagnostic outcomes such as incidence of VTE, bleeding events, and mortality. All the measurements were made by the same doctor and then checked by another researcher.
OUTCOME:
The primary endpoint was the incidence of VTE at discharge. VTE was confirmed using compression ultrasonography for DVT; PE was confirmed using computed tomographic pulmonary angiography, ventilation-perfusion lung scanning, or pulmonary angiography [12]. All patients were examined for VTE on the last day of hospital stay. The secondary outcome was the presence or absence of major bleeding. The severity of major bleeding events was graded on a 3-point scale: heavy, moderate, and light were considered fatal, critical, and clinically overt bleeding, respectively. Fatal bleeding events were defined as bleeding directly leading to a patient’s death. Critical bleeding events included non-surgery-related intracranial, intraocular, intraspinal, pericardial, and retroperitoneal bleeding. Clinically, overt bleeding decreased hemoglobin levels by >2 g/dL. The secondary outcomes were rivaroxaban-related mild bleeding and thrombocytopenia, rivaroxaban allergy, and VTE-related death. The patients were monitored for 30 days to determine mortality. All outcomes were prespecified according to the protocol. Thrombocytopenia was defined as a platelet count <100 giga/L or a decrease of ≥50% compared with the count before surgery [13].
SAMPLE SIZE ESTIMATION:
The sample size estimation used data from similar studies published previously [2,14], according to which the incidence of venous thromboembolism in the control group was about 40%, with the usage of rivaroxaban, and we estimated that the risk of venous thromboembolism would decrease by about 25%. We set the significance level (alpha) as 0.05, with power of test (1-β) 0.80, and the Pearson chi-square test was used to calculate the sample size [15]. The results showed that we needed 94 patients, with 47 in each group.
STATISTICAL ANALYSIS:
To assess whether continuous variable data such as age and BMI were normally distributed, we used the Kolmogorov-Smirnov test (
Results
PARTICIPANT CHARACTERISTICS:
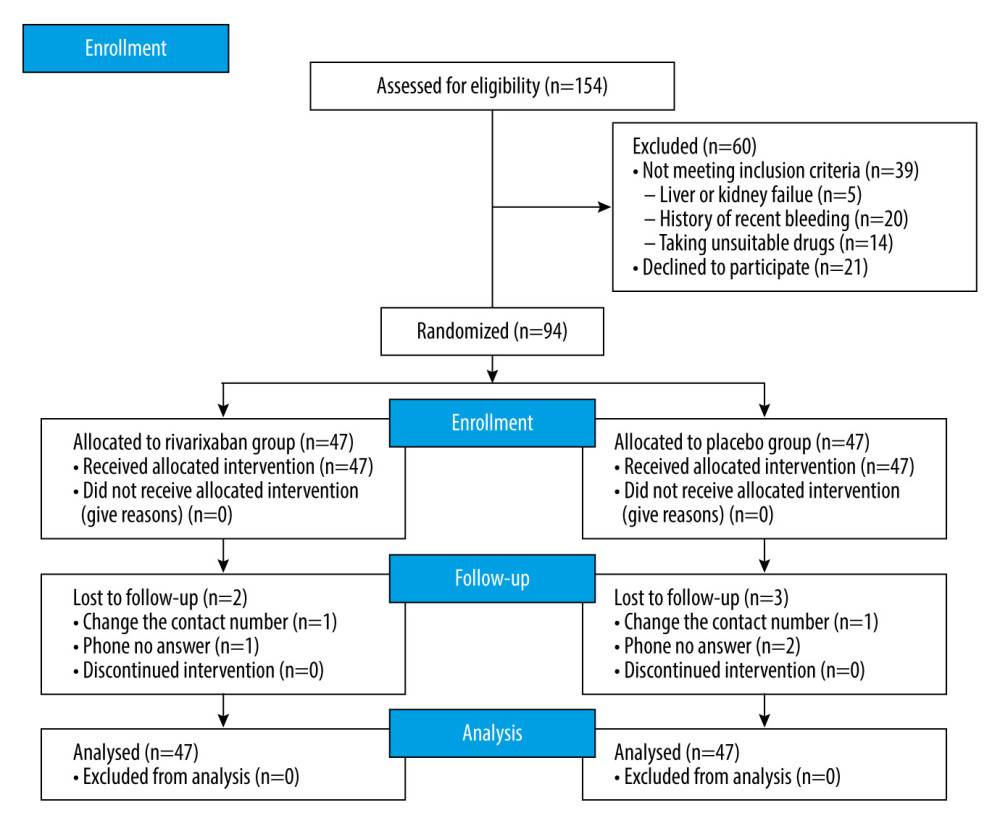
At the patient enrollment stage, 154 patients considered suitable for randomization were selected, among whom 60 were excluded. Twenty-one patients refused to sign the informed consent form, mainly because of concerns regarding adverse drug reactions, the risk of bleeding outweighing potential benefits, and other unpredictable drug-related risks. Thirty-nine patients were excluded because of their recent physical condition such as recent active bleeding of various organs, including gastrointestinal ulcer bleeding and intracranial bleeding, and because they received antiplatelet or anticoagulant drugs before surgery. Finally, we enrolled 94 randomized patients, with 47 patients in the rivaroxaban and placebo groups each. The enrollment process with the CONSORT standardized flow diagram is shown in Figure 1. The 30-day mortality rate was determined by telephone follow-up, and 5 patients were lost to follow-up because their contact number changed or they did not respond to the calls. All data of 94 patients were analyzed based on the intention-to-treat principle.
The baseline characteristics of patients in the rivaroxaban and placebo groups were well matched (Table 1). There were no significant differences between the 2 groups with respect to age, sex, BMI, laboratory test results, medical history, and WHO glioma grade. The average age of patients at brain glioma surgery was approximately 54 years, and women accounted for a slightly higher percentage of patients. Platelet counts and hemoglobin levels of patients were normal before surgery. Approximately 16% of patients had common chronic diseases such as hypertension and diabetes. A relatively high proportion of patients with the WHO classifications of III and IV suggested that most patients had malignant gliomas. The final pathology revealed oligodendrogliomas (grade II), astrocytes (grade II), mixed glioma (grade II), anaplastic glioma (grade III), glioblastoma (grade IV), and other malignant gliomas (grade IV). Postoperative results showed that all patients received total resection.
PRIMARY EFFICACY ENDPOINT:
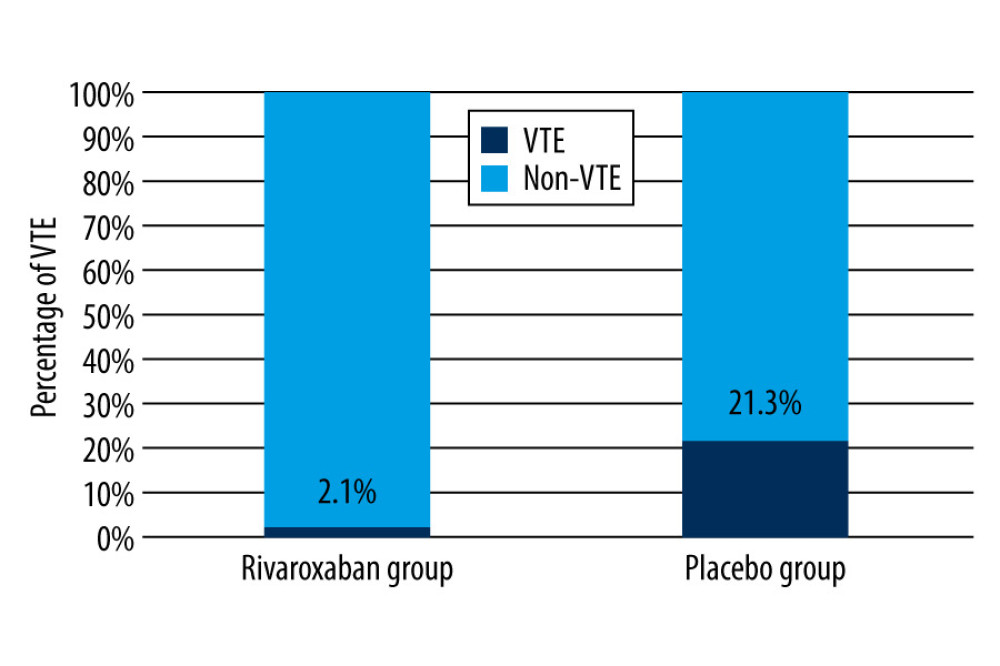
The primary composite outcome occurred in 1 (2.1%) of 47 patients and in 10 (21.3%) of 47 patients in the rivaroxaban and placebo groups, respectively. The results are shown in Figure 2 and Table 2. In the rivaroxaban group, the only patient with VTE had distal DVT, as detected on ultrasound, and was asymptomatic. In the placebo group, a high percentage of patients had VTE, but most patients were asymptomatic, only 1 patient had PE, and there were 6 distal DVTs and 3 proximal DVTs. However, because of the combination of severe diabetes and complex multivessel coronary artery disease, the patient with PE could not be surgically treated and eventually died owing to PE-related heart failure. Two patents were symptomatic, with symptoms of lower-limb edema or ache, but no PE was found in these 2 patients. In brief, patients in the rivaroxaban group had a significantly lower VTE incidence rate than those in the placebo group (P=0.008). No significant results were obtained with respect to the effect of rivaroxaban on PE because of its low incidence.
SAFETY OUTCOMES:
The study safety endpoints in the rivaroxaban and placebo groups are shown in Table 3. Major bleeding events were noted in 1 patient each in the rivaroxaban and placebo groups, with no significant difference between groups. No fatal bleeding or critical bleeding was observed in our study. Patients in the rivaroxaban group had hematuria, and after discontinuing the drug, urine and hemoglobin levels returned to normal. Similarly, patients in the placebo group also had hematuria, and after further examination, they were confirmed to have bladder tumors. No thrombocytopenia or allergy was noted in either group. One patient in the placebo group died because of PE and complex and intractable concomitant underlying diseases. Two patients in the rivaroxaban group had mild bleeding, including nosebleeds and bloody sputum; however, the symptoms were mild and transient.
Discussion
This is the first study to explore the effectiveness and safety of rivaroxaban in patients undergoing brain glioma surgery. Vein thrombosis occurred in 1 out of 47 patients (2.1%) in the rivaroxaban group, and in the placebo group it occurred in 10 out of 47 patients (21.3%). The incidence decreased by approximately 20%. The safety of rivaroxaban in preventing VTE was also assessed, but no significant difference was found because of the limited sample size.
Several studies have reported the effect of pharmacological thromboprophylaxis in adult patients undergoing neurosurgical interventions for preventing VTE. A cohort study [16] including 2638 neurosurgical patients found that most DVTs occurred within the first week after a neurosurgical procedure. The use of early subcutaneous heparin (at either 24 or 48 h) was associated with a 43% reduction in DVT development, without an increase in surgical site hemorrhage. Constantini et al [17] conducted a randomized study to evaluate the safety of mini-dose heparin (5000 U of heparin per day) in patients undergoing surgery for supratentorial brain tumors and found that the perioperative administration of heparin was safe and did not significantly alter bleeding risk. Hamidi et al [18] examined 89 patients who received either LMWH or no prophylaxis before elective instrumental spinal surgery and found that preoperative prophylactic LMWH was not associated with major bleeding complications that altered the postoperative course. Our study included 94 patients undergoing brain glioma surgery and found that the novel oral anticoagulant rivaroxaban was associated with a 20% reduction in DVT development, without an increase in major bleeding events. A recent systematic review [19] including 7 randomized controlled trials and 3 non-randomized controlled studies suggested that pharmacologic thromboprophylaxis can decrease the risk of asymptomatic proximal DVT by approximately 50%. However, no study has yet reported the effect of rivaroxaban in neurosurgical procedures, which has limited its usage. Rivaroxaban is a highly selective direct oral inhibitor of factor Xa. Inhibitor Xa can interrupt the endogenous and exogenous pathways of coagulation waterfall-cascade and inhibit the production of thrombin and thrombosis [20]. Compared with other oral anticoagulants such as warfarin, rivaroxaban does not require laboratory monitoring or frequent dose adjustments [21]. We found that rivaroxaban has been studied in patients with peripheral artery disease [7], nonmajor orthopedic surgery [8], nonvalvular atrial fibrillation [9], acute ischemic stroke [22], and stable cardiovascular disease [23]. Patients with cancers, particularly those with malignant tumors, have changes in the homeostatic mechanism of coagulation and fibrinolysis, predisposing them to hypercoagulation [24]. The incidence of VTE can be as high as 20% in patients with brain metastases and primary central nervous system lymphoma and as high as 30% in patients with high-grade glioma [25,26]. Our study showed that VTE occurred in 21.3% of patients undergoing brain glioma surgery; however, most patients were asymptomatic and only 20% were symptomatic. Heidrich et al [27] examined the incidence of venous thrombosis in tumor patients and found that 31.3% of patients with venous thromboses were symptomatic and 68.7% were asymptomatic, and they mostly occurred during chemotherapy, surgery, or radiation therapy. If asymptomatic VTE is untreated, it can lead to PE; therefore, asymptomatic VTE should be treated as symptomatic venous thrombosis.
This study had some limitations. First, the conclusions may not be appropriate for all patients undergoing neurosurgery procedures because the study strictly limited enrollment to patients who underwent brain glioma surgery. Although we showed that rivaroxaban can be beneficial for patients undergoing brain glioma surgery, clinicians should alert for adverse reactions to rivaroxaban. Moreover, we strictly limited the scope of inclusion to patients with gliomas, and we did our best to exclude patients at risk for bleeding, based on preoperative or intraoperative evaluation results. Therefore, rivaroxaban should not be administered to patients who are determined by clinicians to be at risk for bleeding. Second, our results cannot be generalized to the use of all new oral anticoagulants. Currently, there are several kinds of anticoagulants corresponding to different treatment outcomes and adverse reactions that may differ from those reported in our study. Therefore, caution should be exercised when considering our results. In addition, our study is limited by its small sample size and single-center design, which may have biased our results. Surgical impairment of brain function areas resulting in limb dyskinesia was not considered when patients were enrolled. The accuracy of ultrasonography and patient compliance could also have biased the results. Subsequent studies should have a larger sample size and use different doses of rivaroxaban to better understand the effect of rivaroxaban in patients undergoing brain glioma surgery or other neurosurgical procedures.
Conclusions
The administration of rivaroxaban is safe and is associated with a lower VTE incidence rate in patients undergoing brain glioma surgery. This preventive application with evidently lower incidence should be regularly used perioperatively in glioma cerebral surgery.
References
1. Stein PD, Matta F, Hughes MJ, Hospitalizations for high-risk pulmonary embolism: Am J Med, 2021; 134(5); 621-25
2. Khaldi A, Helo N, Schneck MJ, Venous thromboembolism: Deep venous thrombosis and pulmonary embolism in a neurosurgical population: J Neurosurg, 2011; 114(1); 40-46
3. Sepulveda-Sanchez JM, Munoz LJ, Arraez MA, SEOM clinical guideline of diagnosis and management of low-grade glioma (2017): Clin Transl Oncol, 2018; 20(1); 3-15
4. Semrad TJ, O’Donnell R, Wun T, Epidemiology of venous thromboembolism in 9489 patients with malignant glioma: J Neurosurg, 2007; 106(4); 601-8
5. Pavon JM, Adam SS, Razouki ZA, Effectiveness of intermittent pneumatic compression devices for venous thromboembolism prophylaxis in high-risk surgical patients: A systematic review: J Arthroplasty, 2016; 31(2); 524-32
6. Streiff MB, Agnelli G, Connors JM, Guidance for the treatment of deep vein thrombosis and pulmonary embolism: J Thromb Thrombolysis, 2016; 41(1); 32-67
7. Bonaca MP, Bauersachs RM, Anand SS, Rivaroxaban in peripheral artery disease after revascularization: N Engl J Med, 2020; 382(21); 1994-2004
8. Samama CM, Laporte S, Rosencher N, Rivaroxaban or enoxaparin in nonmajor orthopedic surgery: N Engl J Med, 2020; 382(20); 1916-25
9. Patel MR, Mahaffey KW, Garg J, Rivaroxaban versus warfarin in nonvalvular atrial fibrillation: N Engl J Med, 2011; 365(10); 883-91
10. Key NS, Khorana AA, Kuderer NM, Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update: J Clin Oncol, 2020; 38(5); 496-520
11. Kirschner M, do Ó Hartmann N, Parmentier S, Primary thromboprophylaxis in patients with malignancies: Daily practice recommendations by the hemostasis working party of the German Society of Hematology and Medical Oncology (DGHO), the Society of Thrombosis and Hemostasis Research (GTH), and the Austrian Society of Hematology and Oncology (ÖGHO): Cancers (Basel), 2021; 13(12); 2905
12. Pedraza GJ, Valle AJ, Ceballos GP, Comparison of the accuracy of emergency department-performed point-of-care-ultrasound (POCUS) in the diagnosis of lower-extremity deep vein thrombosis: J Emerg Med, 2018; 54(5); 656-64
13. Lo GK, Juhl D, Warkentin TE, Evaluation of pretest clinical score (4 T’s) for the diagnosis of heparin-induced thrombocytopenia in two clinical settings: J Thromb Haemost, 2006; 4(4); 759-65
14. Cerrato D, Ariano C, Fiacchino F, Deep vein thrombosis and low-dose heparin prophylaxis in neurosurgical patients: J Neurosurg, 1978; 49(3); 378-81
15. Chow S-C, Shao J, Wang H, Lokhnygina Y: Sample size calculations in clinical research, 2018; 77(4.7), Boca Raton, FL, Taylor & Francis Group
16. Khaldi A, Helo N, Schneck MJ, Venous thromboembolism: Deep venous thrombosis and pulmonary embolism in a neurosurgical population: J Neurosurg, 2011; 114(1); 40-46
17. Constantini S, Kanner A, Friedman A, Safety of perioperative minidose heparin in patients undergoing brain tumor surgery: A prospective, randomized, double-blind study: J Neurosurg, 2001; 94(6); 918-21
18. Hamidi S, Riazi M, Incidence of venous thromboembolic complications in instrumental spinal surgeries with preoperative chemoprophylaxis: J Korean Neurosurg Soc, 2015; 57(2); 114-18
19. Yepes-Nunez JJ, Rajasekhar A, Rahman M, Pharmacologic thromboprophylaxis in adult patients undergoing neurosurgical interventions for preventing venous thromboembolism: Blood Adv, 2020; 4(12); 2798-809
20. Kvasnicka T, Malikova I, Zenahlikova Z, Rivaroxaban – metabolism, pharmacologic properties and drug interactions: Curr Drug Metab, 2017; 18(7); 636-42
21. Bott-Kitslaar DM, Mcbane RD, Casanegra AI, Apixaban and rivaroxaban in patients with acute venous thromboembolism: Mayo Clin Proc, 2019; 94(7); 1242-52
22. Yasaka M, Minematsu K, Toyoda K, Rivaroxaban administration after acute ischemic stroke: The RELAXED study: PLoS One, 2019; 14(2); e212354
23. Eikelboom JW, Connolly SJ, Bosch J, Rivaroxaban with or without aspirin in stable cardiovascular disease: N Engl J Med, 2017; 377(14); 1319-30
24. Falanga A, Schieppati F, Russo D, Cancer tissue procoagulant mechanisms and the hypercoagulable state of patients with cancer: Semin Thromb Hemost, 2015; 41(7); 756-64
25. Jenkins EO, Schiff D, Mackman N, Venous thromboembolism in malignant gliomas: J Thromb Haemost, 2010; 8(2); 221-27
26. Lacy J, Saadati H, Yu JB, Complications of brain tumors and their treatment: Hematol Oncol Clin North Am, 2012; 26(4); 779-96
27. Heidrich H, Konau E, Hesse P, Asymptomatic venous thrombosis in cancer patients – a problem often overlooked. Results of a retrospective and prospective study: Vasa, 2009; 38(2); 160-66
Figures
Tables
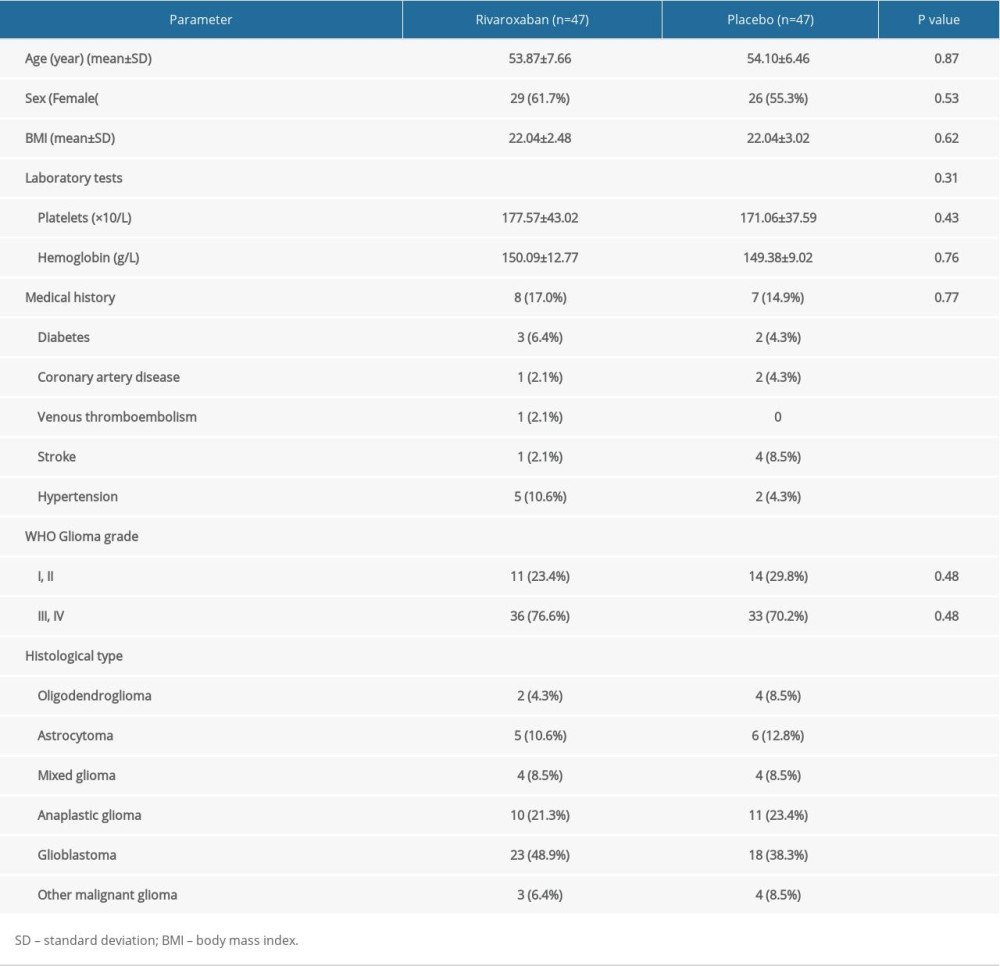 Table 1. Baseline characteristics of participants with rivaroxaban and placebo.
Table 1. Baseline characteristics of participants with rivaroxaban and placebo.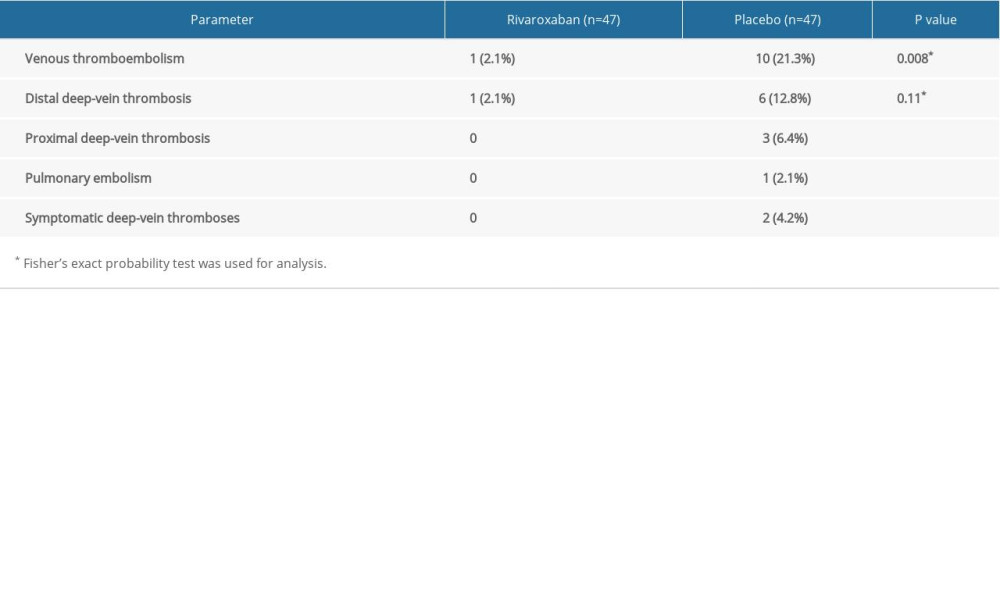 Table 2. Comparison of primary endpoint between rivaroxaban and placebo groups.
Table 2. Comparison of primary endpoint between rivaroxaban and placebo groups.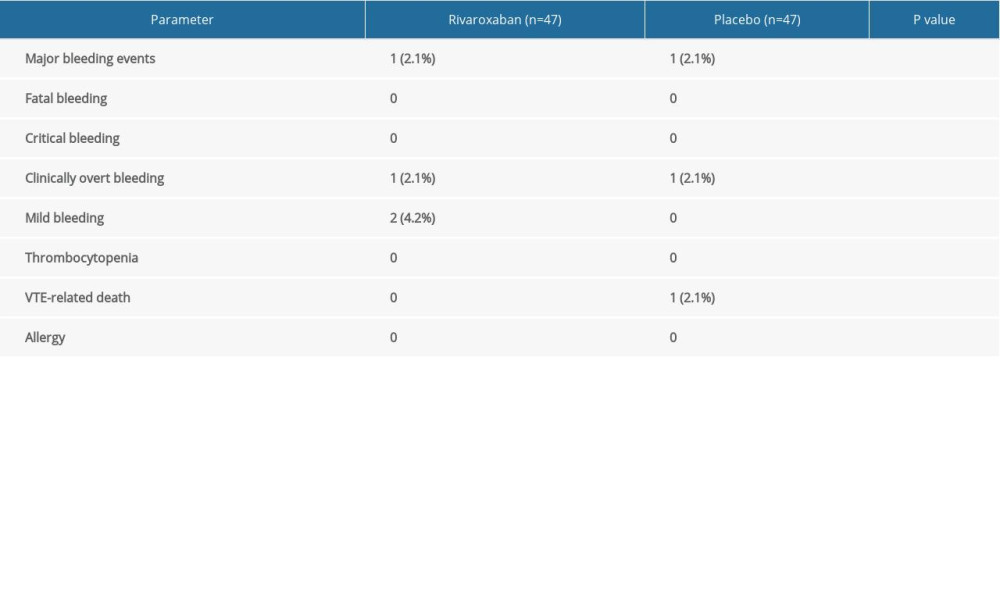 Table 3. Comparison of safety outcomes between rivaroxaban and placebo groups.Table 1. Baseline characteristics of participants with rivaroxaban and placebo.Table 2. Comparison of primary endpoint between rivaroxaban and placebo groups.Table 3. Comparison of safety outcomes between rivaroxaban and placebo groups.
Table 3. Comparison of safety outcomes between rivaroxaban and placebo groups.Table 1. Baseline characteristics of participants with rivaroxaban and placebo.Table 2. Comparison of primary endpoint between rivaroxaban and placebo groups.Table 3. Comparison of safety outcomes between rivaroxaban and placebo groups. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387