05 March 2022: Clinical Research
Conversion from Spanning External Fixation to Open Reduction Internal Fixation Contributes to Healing of Soft Tissues and Fractures in Open Distal Humeral Fractures
Kaige Ma1ABCDEFG, Donghua Huang1BC, Chunqing Meng1E, Hong Wang1E, Zengwu Shao1E, Huimin Liu2C*, Dehao Fu13ADOI: 10.12659/MSM.934488
Med Sci Monit 2022; 28:e934488






Abstract
BACKGROUND: Open distal humeral fractures (DHFs) often lead to loss of elbow function, thereby seriously affecting patient quality of life. The aim of this study was to evaluate the treatment outcomes of 2 surgical techniques to determine the better method for repairing open DHFs. Both groups were treated with immediate debridement first, and then group I had only internal fixation (IF), while group II underwent initial external fixation (EF) followed by IF surgery.
MATERIAL AND METHODS: This retrospective study included 32 patients who had open DHFs between 2013 and 2018. Twelve patients underwent thorough debridement and temporary EF treatment and converted to IF as the ultimate treatment. Twenty patients were treated with immediate open reduction and internal fixation (ORIF). Data of final treatment outcomes were analyzed at the latest follow-up. A comparative analysis of radiological results, function observations, and complications was performed for the 2 surgical groups.
RESULTS: All DHFs and osteotomized olecranon united after a mean of 5.2±1.21 months. No significant differences were observed in other preoperative demographic data between the 2 groups. Moreover, there was no significant difference in postoperative complications, elbow range of motion, or fracture healing time between the 2 groups.
CONCLUSIONS: The evidence provided by our study highlights the efficacy of definitive IF in treating open DHFs, which is recommended whenever possible. Furthermore, the combination of EF and ORIF, according to the type of soft tissue damage, may be a promising treatment option with a low revision rate for patients with open DHFs.
Keywords: Elbow Joint, Fracture Fixation, Internal, humeral fractures, Adult, Female, Fracture Healing, Humans, Male, Open Fracture Reduction, Quality of Life, Radiography, Range of Motion, Articular
Background
Distal humeral fractures (DHFs) comprise approximately 2% of all adult fractures and one-third of all humeral fractures [1]. The complex anatomy of elbow articulation, including the distal humerus, proximal ulna, and radial head, leads to complex intra-articular fractures in the distal humerus. The complications accompanying DHFs include elbow stiffness, heterotopic ossification, and loss of elbow function [2,3]. DHFs are frequently the result of high-energy trauma with skin involvement and low-energy trauma in osteoporotic bone [4]. The fundamental goals for the treatment of DHFs are to achieve stable fixation, maintain a viable soft tissue envelope, restore function range of motion, and limit complications [5].
Internal fixation (IF) has shown good outcomes for the complex DHFs with stable fixation and a high rate of union, thus permitting intensive rehabilitation to restore elbow motion [6]. Coblation debridement in treatment with retention of IF is effective for early postoperative infection of extremity fractures, which can avoid second-stage surgery, infectious nonunion, and osteomyelitis [7]. A spanning external fixation (EF) before IF is a safe adjunct providing excellent outcomes by enabling wound care/debridement and soft tissue healing, thus ultimately improving fracture healing [8–10]. A retrospective case study review of 85 humeral fractures, 62 shaft fractures, and 23 extra-articular distal third fractures treated with EF has highlighted EF as a valid treatment method owing to its good outcomes in the stability of reduction, tolerability, healing times, and function recovery [11]. In addition, EF in DHFs in children shows several benefits of avoiding additional injury to the growth plate and enabling careful reduction without interfragmentary compression, with no soft tissue dissection, preserved periosteal blood supply, immediate joint motion, and early weight-bearing; meanwhile, EF ensures primary fracture stability even in the presence of comminution and high adjustment capability [12]. However, the definitive use of EF treatment for fractures is not recommended because this treatment method can also lead to elbow joint stiffness, limit elbow joint activity function, and increase the risk of fracture nonunion or malunion [8,13].
Open reduction and internal fixation (ORIF) is the criterion standard management of DHFs in middle-aged and elderly patients [4,7,14]. The method of fixation depends on the type of fracture, the degree of comminution, and the restoration of columns and articular surface [15]. ORIF treatment for DHFs with an extensor mechanism-on approach can achieve favorable healing, a mean elbow flexion-extension exceeding 100°, and maintenance of 90% of elbow extension strength, relative to that of the contralateral, normal elbow [4]. Spanning the elbow temporarily with a plate as an adjunct to the ORIF method has been demonstrated to be simple and effective in achieving fracture stability and union and can minimize failure rates after fixation of DHFs [16]. However, a recent systematic review and meta-analysis revealed that complications and reoperations of DHFs after ORIF may be more frequent than previously understood [17].
The aim of this study was to identify a specific approach in treating open DHFs, which offered optimal care to prevent infection and additional soft tissue injury while achieving good elbow movement outcomes.
Material and Methods
PATIENTS:
Between 2013 and 2018, 100 patients with DHFs were treated at our institution, of which 40 patients were included in this study as they presented with open DHFs. All fractures were caused by high-energy trauma, including motor vehicle accidents (n=30), falls (n=8), and crush injuries (n=2). We selected the surgical methods based on the general condition of the patients, the degree of wound injury, and the willingness of the patients and their family members. Fifteen patients underwent EF treatment (group I) and 25 patients were treated with ORIF (group II). Sixty patients with open fractures were excluded owing to Gustilo-Anderson grade III type IIIb and IIIc open DHFs, life-threatening complications, or open fractures in adolescents. A total of 3 and 5 patients from each group, respectively, were lost to follow-up before the minimum follow-up period. Twelve patients in group I and 20 patients in group II were available at the latest follow-up, and their data were analyzed for final outcomes. Patient demographic characteristics are shown in Table 1.
This study was approved by the local Ethics Committee and followed the ethical standards established in the Declaration of Helsinki. Informed and written consent was provided by the patients or their family members.
DAMAGE CONTROL ORTHOPEDICS:
The patients were initially evaluated in the Emergency Department (ED) by a senior trauma doctor for open fractures and systemic injuries assessments. Imaging, including computed tomography (CT) of the skull/spine/abdomen/thorax and local fracture imaging by X-ray and CT scan were performed as advised. Primary treatment consisted of fluids, resuscitation, and airway and circulation checks. Limb assessment was performed for distal neuro-vascular deficits. Wounds were rinsed with saline lavage in the ED. Antibiotic prophylaxis was conducted in the ED for contaminated open wounds.
OPEN WOUND GRADING AND FRACTURES:
The wounds of all included patients were classified according to the Gustilo-Anderson system [18]. Group I included 10 patients with open Gustillo grade I or II and 2 patients with open Gustillo grade IIIa distal humerus articular metaphyseal multi-fragmentary fractures. In group II, all 20 patients had open Gustillo grade I or II distal humerus articular metaphyseal multi-fragmentary fractures. Patients with Gustilo-Anderson grades IIIb and IIIc were excluded from the analysis owing to huge variations related to the degree and prognosis of the fractures. The fractures were classified by the Arbeitsgemeinschaft für Osteosynthesefragen (AO) pattern for DHFs [19]. In group I, there were 3 patients with AO type C1, 8 patients with AO type C2, and 1 patient with AO type C3 fractures. In group II, there were 4 patients with AO type C1, 14 patients with AO type C2, and 2 patients with AO type C3 fractures.
TREATMENT:
All patients underwent surgical debridement for primary wound care of the open fractures. After the debridement surgery, the fractures were treated by closed reduction, and 12 patients with high-grade and contaminated injuries had their fractures temporarily fixed by EF. After the overall physiological examination and wound care, IF was selected as the ultimate treatment (Figures 1, 2). We used the olecranon osteotomy approach for DHFs [20,21]. Twenty patients with low-grade injuries were treated with thorough debridement and immediate ORIF. Antibiotics were used in preoperative and postoperative wound care as per our institutional protocols or recommendations. The grade I and II open fractures required coverage by a first-generation cephalosporin for 24 h after wound closure. Grade III open fractures required coverage by a first-generation cephalosporin and an aminoglycoside for 48 to 72 h after initial injury but no longer than 24 h after wound closure [22,23]. The patients undergoing conversion to ORIF were intravenously administered a first-generation cephalosporin (cefazolin, 1 g) within 1 h before skin incision and did not receive additional postoperative antibiotics. C-reactive protein (CRP) levels were measured regularly 2 to 3 days after EF surgery, and the gradually decreased levels of CRP or levels lower than 30 were used as a reference for the conversion surgery [24,25]. Postoperative infection, heterotopic ossification, and other complications were prevented by using preventive medicine (non-steroidal anti-inflammatory drugs [NSAIDs]) and strengthening the elbow joint function through exercises. The postoperative rehabilitation began with early active-assisted range of motion exercises on the second day after surgery, with the only restrictions being lifting weights or resistance training. Otherwise, there was no limitation to the range of motion. An NSAID (etoricoxib, 90 mg daily) was prescribed for 9 days to prevent heterotopic ossification [26].
FOLLOW-UP AND OUTCOMES:
All patients were followed up for a minimum period of 18 months from the date of final ORIF. Radiographs were used after a mean follow-up of 28.8 months to evaluate fracture healing. A thorough physical examination including range of motion was used to evaluate the recovery effects according to the presence of narrowed joint space or early signs of arthritis or heterotopic ossification. When the fractures had healed at approximately 2 years after surgery, the IF devices were removed after a mean of 18 months (12–30 months). Function outcomes were recorded based on assessment by the Mayo Elbow Performance Score (MEPS) and Disabilities of Arm and Shoulder and Hand (DASH) scores.
STATISTICAL ANALYSIS:
Data were analyzed and compared between the 2 groups. We developed a spreadsheet for data entry, including demographic data, surgical treatment, patient outcomes, complications, and other patient-specific information. Descriptive statistics were presented as frequencies and percentages (categorical variables) or as mean±standard deviation (continuous variables). The categorical data were analyzed using the chi-squared test, and the continuous data were analyzed using
Results
A retrospective review was performed on 32 patients (20 men and 12 women; mean age: 35.41±11.67 years) with open DHFs at our institution. Of these patients, 12 (7 men and 5 women, mean age: 37.6±10.4) underwent procedure 1, and 20 (13 men and 7 women, mean age: 34±11.9) underwent procedure 2 (Table 2). All patients were available at the latest follow-up for radiological and function assessment. Most of the injuries were associated with high-energy trauma, with road traffic accidents accounting for 75% of injuries in the 32 patients. There were 3 patients with fall injuries in group I and 5 patients with fall injuries in group II, both accounting for 25% of the patients in these groups. Associated systemic or multi-organ injuries were noted in 5 patients. Mean CRP levels before IF were 4±5.92 mg/dL in group I.
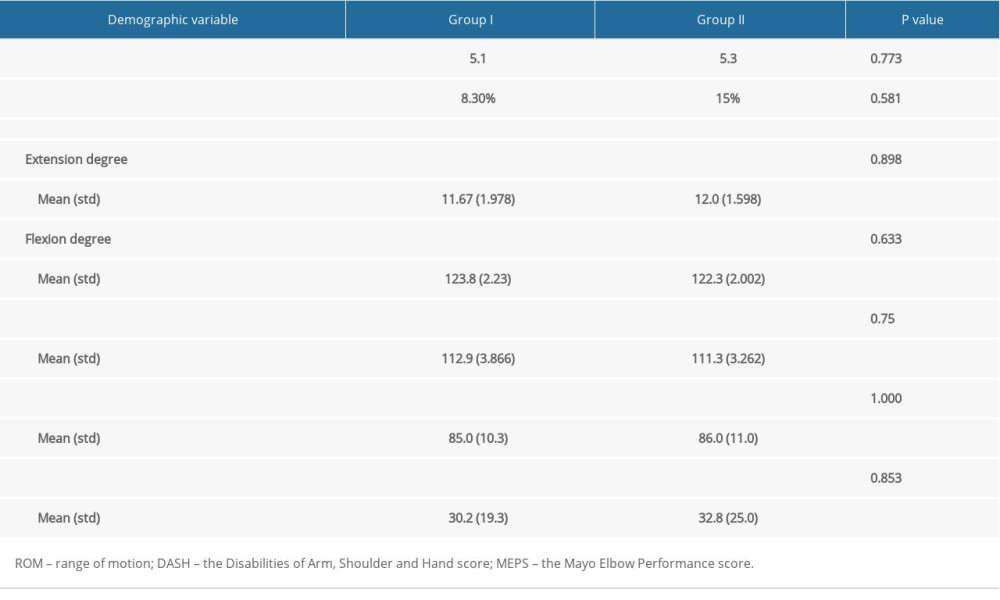
In function evaluation at 12 months following surgery, patients in group I achieved greater elbow range of movement for flexion-extension (111.3±3.262 degrees vs 112.9±3.866 degrees for group II;
Duration of hospital stay in group I was 13 (10–15) days vs 12 (8–18) days in group II (
All DHFs and osteotomized olecranon united after a mean of 5.2±1.21 months. Only 1 case of heterotopic ossification occurred in group I. Three patients developed postoperative complications, including heterotopic ossification (2 patients) and elbow stiffness (1 patient) in group II, and 1 patient’s elbow motion was still seriously affected 1 year after the elbow injury, thus requiring arthroscopy to remove an abnormal bone mass and release the joint.
Discussion
The best choice of surgical methods for the treatment of severe open humeral fractures has been controversial for several decades. Previous case reports of open DHFs have demonstrated favorable outcomes using definitive ORIF to achieve good elbow function [27–29]. In the present study, we clarified the importance of EF as a primary procedure for the stabilization and prevention of further soft tissue injury and as a spanning fixator for wound management until it was appropriate to convert to ORIF [24].
The results obtained in the present investigation revealed that, at function evaluation at 12 months following surgery, patients treated with EF exhibited greater elbow range of movement for flexion-extension than did patients treated with ORIF. The most common complications of open fractures are wound infection and nonunion [28]. A previous study showed that patients with distal radius fractures in an EF group exhibited better grip strength than did those in the volar locking plate group, with a mean difference of 12.48 (
The present study also found that only 1 case of heterotopic ossification occurred in patients treated with EF, while 3 patients reported postoperative complications, including heterotopic ossification (2 patients) and stiff elbow (1 patient) in response to ORIF treatment. Recent findings suggest that EF is safe and effective for the definitive treatment of the anterior ring in unstable pelvic fractures and has a high proportion of excellent outcomes, regardless of the type of fracture, and a low complication rate [33]. A previous report on the function outcomes and complications after ORIF for acute DHF AO/OTA type 13 C2 and C3 with a minimum 2-year follow-up showed that the median flexion/extension and supination/pronation arcs were 120 degrees and 160 degrees, respectively; 8 complications were found in 7 patients, and 4 of them required reoperation owing to fracture pseudoarthrosis or elbow stiffness [14]. A prior prospective clinical evaluation showed that 7 cases with displaced both-column fractures of the acetabulum developed postoperative complications, including subcutaneous hematoma in 2, wound infection in 2, and heterotopic ossification in 3, when treated by ORIF with cerclage wiring; none of these complications had an adverse effect on the clinical outcome, and all the cases had excellent final outcomes [34].
Skeletal stabilization is conducted by the temporary EF at the first debridement. After the conversion operation from EF to ORIF, the fractures are firmly fixed, and patients can perform early function exercises. The temporary EF can reduce the initial surgical trauma compared with definitive IF, since trauma and surgeries lead to an inflammatory response [24]. Meanwhile, EF is recommended for fractures with serious injuries in the soft tissues to avoid intramedullary infection [35]. These data were consistent with our study, in which EF allowed for debridement and wound care, while the health of the patients as well as the soft tissues were stabilized for ORIF surgery. In addition, previously published literature has indicated that, compared with individual EF treatment, combined fixation of EF with limited IF is an effective and safe alternative for the management of open tibial diaphyseal fractures, as it can provide superior initial reduction and better stability as well as decrease the risk of inferior alignment and delayed union without increasing the risk of infection [36,37]. The present study provided evidence suggesting that EF in combination of ORIF, according to the type of soft tissue damage, can be an effective treatment for patients with open DHFs, with a low revision rate.
One limitation of this pilot retrospective study was selection bias, whereby patients with lower Gustilo-Anderson grades of open injuries were advised to receive ORIF as the primary treatment. These patients carried a lower risk for local or systemic complications after primary ORIF surgery, and hence this approach was appropriate without increasing the risk of soft tissue damage or extensive surgery. Owing to the retrospective design, this study was restricted to assess objective range of motion and function scores reported by patients during follow-up. Future prospective studies with larger sample sizes are required to validate the early benefits of EF in offering immediate stabilization, pain relief, and ease of surgical conversion from EF to ORIF. This is a no-difference study according to the statistical results. A possibility of difference might be present; however, this difference did not reach statistical significance owing to the small sample size.
Conclusions
The evidence provided by our study highlights the potential of EF as a primary treatment for all open fractures around the elbow, despite an insignificant statistical difference. The EF treatment prior to conversion to ORIF led to fewer complications, easier wound care, and improved patient health. Undoubtedly, ORIF is the definitive treatment option to restore elbow function as evidenced by the findings from this study and the published literature review. Meanwhile, we advocate primary EF in selected patients to achieve optimal fracture healing and wound repair.
Figures
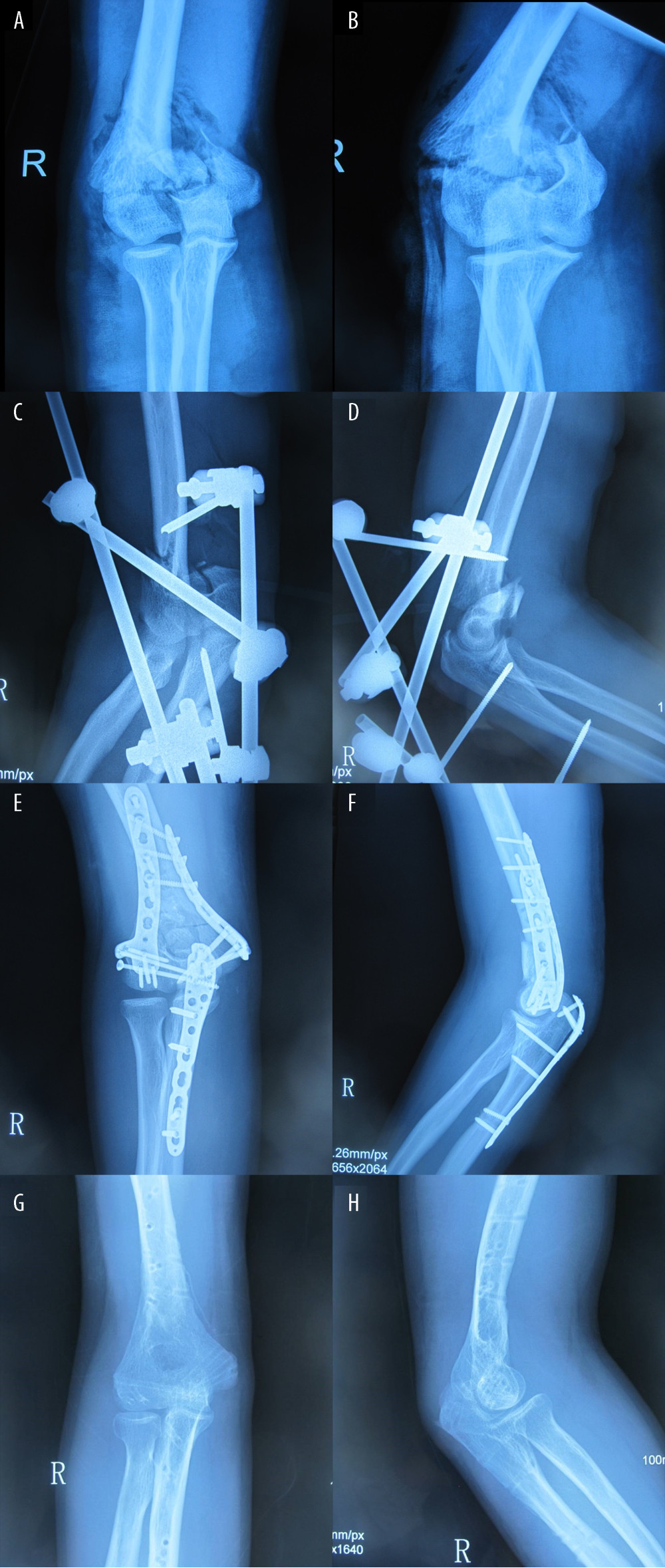 Figure 1. Radiographs from a 35-year-old man who had a grade II open distal humeral fracture in a motor vehicle accident. (A) Anteroposterior and (B) lateral radiographs of AO/OTA type 13-C2 intra-articular fracture of distal humerus on admission. (C) Postoperative anteroposterior and (D) lateral radiographs showing fractures of the distal humeral stabilized by uniplanar external fixation (EF) following debridement. (E) Anteroposterior and (F) lateral radiographs of plate fixation immediately after surgery. EF had been converted to a plate on day 10 after injury. (G) Anteroposterior and (H) lateral radiographs (the internal fixation plates were removed 1 year after plate fixation) showing excellent bony union.
Figure 1. Radiographs from a 35-year-old man who had a grade II open distal humeral fracture in a motor vehicle accident. (A) Anteroposterior and (B) lateral radiographs of AO/OTA type 13-C2 intra-articular fracture of distal humerus on admission. (C) Postoperative anteroposterior and (D) lateral radiographs showing fractures of the distal humeral stabilized by uniplanar external fixation (EF) following debridement. (E) Anteroposterior and (F) lateral radiographs of plate fixation immediately after surgery. EF had been converted to a plate on day 10 after injury. (G) Anteroposterior and (H) lateral radiographs (the internal fixation plates were removed 1 year after plate fixation) showing excellent bony union. 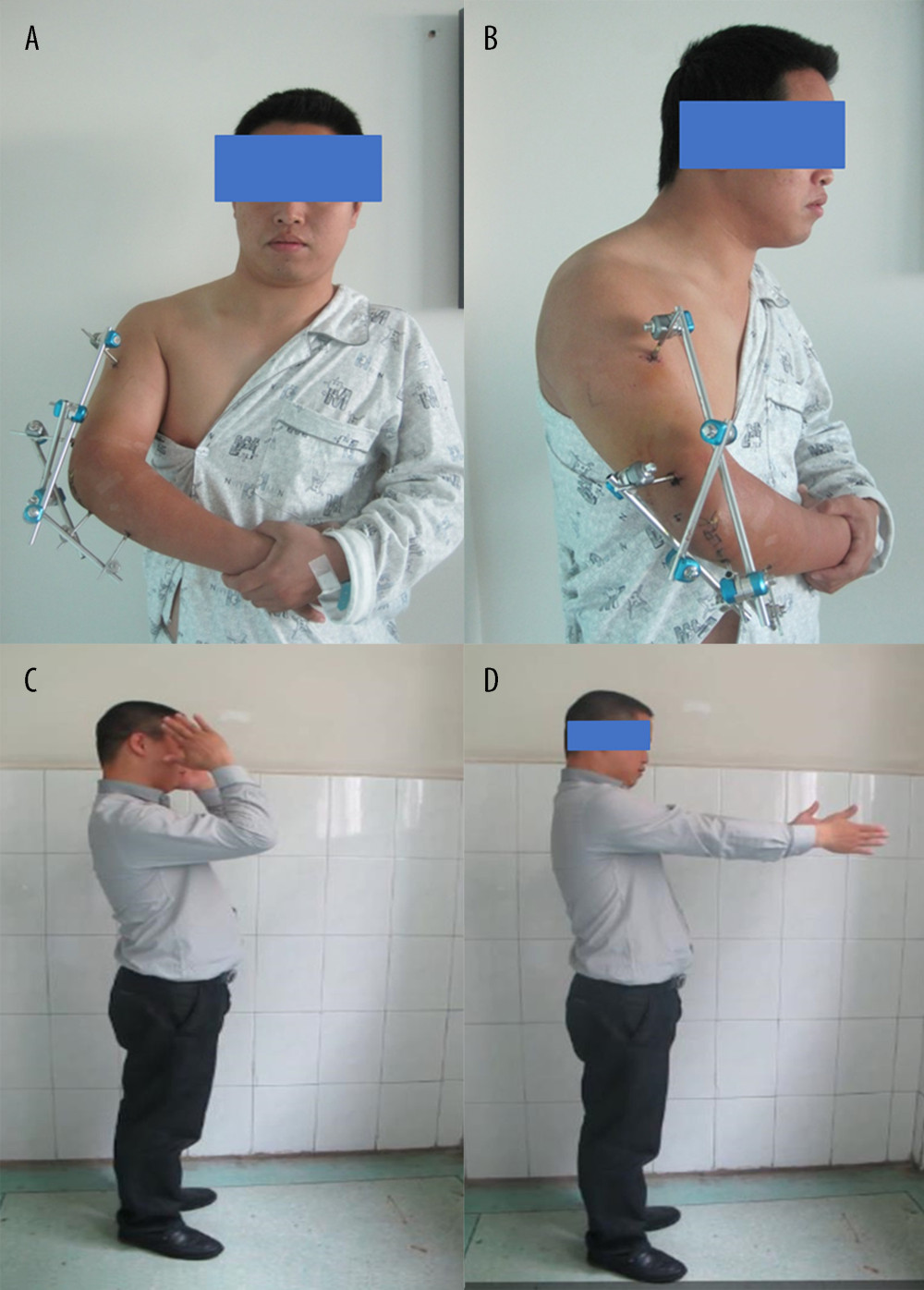 Figure 2. (A) Anteroposterior and (B) lateral images of the injured right elbow showing the well-healed elbow wound when the distal humeral fractures were stabilized by uniplanar external fixation following debridement on day 10 after injury. The red arrow indicates the wound from the motor vehicle accident. Postoperative elbow function. One year after internal fixation, the patient’s (C) elbow flexion and (D) extension function images were presented when the elbow joint internal fixation plates were removed.
Figure 2. (A) Anteroposterior and (B) lateral images of the injured right elbow showing the well-healed elbow wound when the distal humeral fractures were stabilized by uniplanar external fixation following debridement on day 10 after injury. The red arrow indicates the wound from the motor vehicle accident. Postoperative elbow function. One year after internal fixation, the patient’s (C) elbow flexion and (D) extension function images were presented when the elbow joint internal fixation plates were removed. 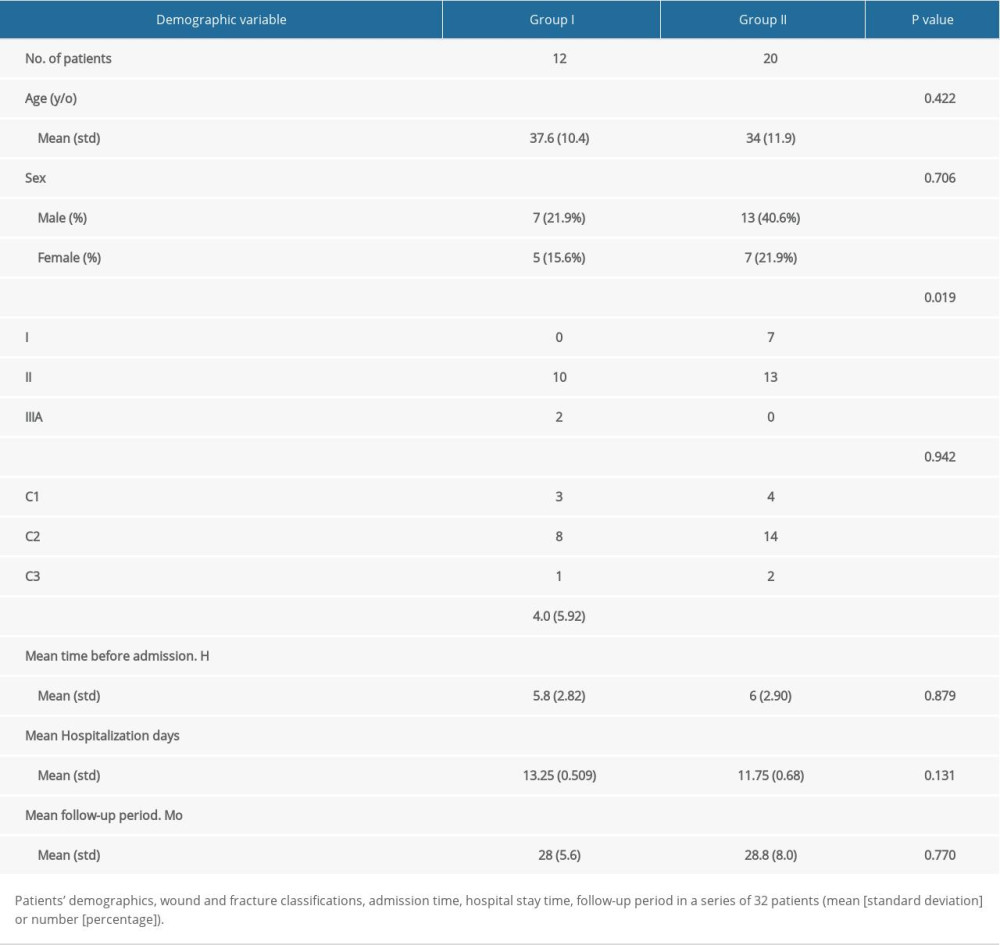
References
1. Wang C, Zhu Y, Long H, Three-dimensional mapping of distal humerus fracture: J Orthop Surg Res, 2021; 16; 545
2. Pan BQ, Huang J, Ni JD, Yan MM, Xia Q, Multiple rare causes of post-traumatic elbow stiffness in an adolescent patient: A case report and review of literature: World J Clin Cases, 2019; 7; 1191-99
3. Kwak JM, Sun Y, Kholinne E, Surgical outcomes for post-traumatic stiffness after elbow fracture: comparison between open and arthroscopic procedures for intra- and extra-articular elbow fractures: J Shoulder Elbow Surg, 2019; 28; 1998-2006
4. Erpelding JM, Mailander A, High R, Outcomes following distal humeral fracture fixation with an extensor mechanism – on approach: J Bone Joint Surg Am, 2012; 94; 548-53
5. Zimmer ZR, Horneff JG, Taylor RM, Evaluation and treatment of open distal humeral fractures: JBJS Rev, 2017; 5 01874474-201701000-0000
6. Sanchez-Sotelo J, Torchia ME, Driscoll SW, Complex distal humeral fractures: Internal fixation with a principle-based parallel-plate technique: J Bone Joint Surg Am, 2007; 89; 961-69
7. Bégué T, Articular fractures of the distal humerus: Orthop Traumatol Surg Res, 2014; 100; S55-63
8. Mostafavi HR, Tornetta P, Open fractures of the humerus treated with external fixation: Clin Orthop Relat Res, 1997; 337; 187-97
9. Desloges W, Faber KJ, King GJ, Athwal GS, Functional outcomes of distal humeral fractures managed nonoperatively in medically unwell and lower-demand elderly patients: J Shoulder Elbow Surg, 2015; 24; 1187-96
10. Kloen P, Helfet DL, Lorich DG, Temporary joint-spanning external fixation before internal fixation of open intra-articular distal humeral fractures: A staged protocol: J Shoulder Elbow Surg, 2012; 21; 1348-56
11. Scaglione M, Fabbri L, Dell Omo D, The role of external fixation in the treatment of humeral shaft fractures: A retrospective case study review on 85 humeral fractures: Injury, 2015; 46; 265-69
12. Korobeinikov A, Popkov D, Use of external fixation for juxta-articular fractures in children: Injury, 2019; 50(Suppl 1); S87-94
13. Chaudhary S, Patil N, Bagaria V, Open intercondylar fractures of the distal humerus: Management using a mini-external fixator construct: J Shoulder Elbow Surg, 2008; 17; 465-70
14. Al-Hamdani A, Rasmussen JV, Olsen BS, Good functional outcomes after open reduction and internal fixation for acute distal humeral fractures AO/OTA type 13C2 and C3 in patients aged over 45 years: J Shoulder Elbow Surg, 2021 [Online ahead of print]
15. Mighell MA, Stephens B, Stone GP, Cottrell BJ, Distal humerus fractures: Open reduction internal fixation: Hand Clin, 2015; 31; 591-604
16. Moharram AN, Mahmoud M, Lymona A, Temporary spanning plate across the elbow for complex fractures of the distal humerus: BMC Musculoskelet Disord, 2021; 22; 875
17. Yetter TR, Weatherby PJ, Somerson JS, Complications of articular distal humeral fracture fixation: A systematic review and meta-analysis: J Shoulder Elbow Surg, 2021; 30; 1957-67
18. Silluzio N, De Santis V, Marzetti E, Clinical and radiographic outcomes in patients operated for complex open tibial pilon fractures: Injury, 2019; 50(Suppl 2); S24-28
19. Bahrs C, Stojicevic T, Blumenstock G, Trends in epidemiology and patho-anatomical pattern of proximal humeral fractures: Int Orthop, 2014; 38; 1697-704
20. Lewicky YM, Sheppard JE, Ruth JT, The combined olecranon osteotomy, lateral paratricipital sparing, deltoid insertion splitting approach for concomitant distal intra-articular and humeral shaft fractures: J Orthop Trauma, 2007; 21; 133-39
21. Habib M, Tanwar YS, Jaiswal A, Anconeus pedicle olecranon flip osteotomy: An approach for the fixation of complex intra-articular distal humeral fractures: Bone Joint J, 2014; 96-B; 1252-57
22. Anderson A, Miller AD, Brandon Bookstaver P, Antimicrobial prophylaxis in open lower extremity fractures: Open Access Emerg Med, 2011; 3; 7-11
23. Back DA, Scheuermann-Poley C, Willy C, Recommendations on negative pressure wound therapy with instillation and antimicrobial solutions – when, where and how to use: What does the evidence show: Int Wound J, 2013; 10(Suppl 1); 32-42
24. Pape HC, Tornetta P, Tarkin I, Timing of fracture fixation in multitrauma patients: the role of early total care and damage control surgery: J Am Acad Orthop Surg, 2009; 17; 541-49
25. Sproston NR, Ashworth JJ, Role of C-reactive protein at sites of inflammation and infection: Front Immunol, 2018; 9; 754
26. Winkler S, Springorum HR, Vaitl T, Comparative clinical study of the prophylaxis of heterotopic ossifications after total hip arthroplasty using etoricoxib or diclofenac: Int Orthop, 2016; 40; 673-80
27. Ashwood N, Verma M, Hamlet M, Transarticular shear fractures of the distal humerus: J Shoulder Elbow Surg, 2010; 19; 46-52
28. Pollak AN, Jones AL, Castillo RCLEAP Study Group, The relationship between time to surgical debridement and incidence of infection after open high-energy lower extremity trauma: J Bone Joint Surg Am, 2010; 92; 7-15
29. Ul Islam S, Glover AW, Waseem M, Challenges and solutions in management of distal humerus fractures: Open Orthop J, 2017; 11; 1292-307
30. Gou Q, Xiong X, Cao D, Volar locking plate versus external fixation for unstable distal radius fractures: A systematic review and meta-analysis based on randomized controlled trials: BMC Musculoskelet Disord, 2021; 22; 433
31. Meng YC, Zhou XH, External fixation versus open reduction and internal fixation for tibial pilon fractures: A meta-analysis based on observational studies: Chin J Traumatol, 2016; 19; 278-82
32. Guo Y, Tong L, Li S, Liu Z, External fixation combined with limited internal fixation versus open reduction internal fixation for treating ruedi-allgower type III pilon fractures: Med Sci Monit, 2015; 21; 1662-67
33. Barrientos-Mendoza C, Brañes J, Wulf R, The role of anterior supra-acetabular external fixator as definitive treatment for anterior ring fixation in unstable pelvic fractures: Eur J Trauma Emerg Surg, 2021 [Online ahead of print]
34. Chen CM, Chiu FY, Lo WH, Chung TY, Cerclage wiring in displaced both-column fractures of the acetabulum: Injury, 2001; 32; 391-94
35. Chen X, Lu M, Xu W, Treatment of pediatric femoral shaft fractures with elastic stable intramedullary nails versus external fixation: A meta-analysis: Orthop Traumatol Surg Res, 2020; 106; 1305-11
36. Griffin M, Malahias M, Khan W, Hindocha S, Update on the management of open lower limb fractures: Open Orthop J, 2012; 6; 571-77
37. Hao ZC, Xia Y, Xia DM, Treatment of open tibial diaphyseal fractures by external fixation combined with limited internal fixation versus simple external fixation: A retrospective cohort study: BMC Musculoskelet Disord, 2019; 20; 311
Figures
Figure 1. Radiographs from a 35-year-old man who had a grade II open distal humeral fracture in a motor vehicle accident. (A) Anteroposterior and (B) lateral radiographs of AO/OTA type 13-C2 intra-articular fracture of distal humerus on admission. (C) Postoperative anteroposterior and (D) lateral radiographs showing fractures of the distal humeral stabilized by uniplanar external fixation (EF) following debridement. (E) Anteroposterior and (F) lateral radiographs of plate fixation immediately after surgery. EF had been converted to a plate on day 10 after injury. (G) Anteroposterior and (H) lateral radiographs (the internal fixation plates were removed 1 year after plate fixation) showing excellent bony union.Figure 2. (A) Anteroposterior and (B) lateral images of the injured right elbow showing the well-healed elbow wound when the distal humeral fractures were stabilized by uniplanar external fixation following debridement on day 10 after injury. The red arrow indicates the wound from the motor vehicle accident. Postoperative elbow function. One year after internal fixation, the patient’s (C) elbow flexion and (D) extension function images were presented when the elbow joint internal fixation plates were removed. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387