24 July 2022: Clinical Research
Safety of Dexmedetomidine as an Alternative Pediatric Magnetic Resonance Imaging (MRI) Sedative: A Retrospective Single-Center Study
Kristina Liaudanskytė1ABEF*, Ilona Razlevičė2ABCDEF, Tomas Bukauskas2ABCDEF, Vilija StremaitytėDOI: 10.12659/MSM.936599
Med Sci Monit 2022; 28:e936599






Abstract
BACKGROUND: Dexmedetomidine provides anxiolysis, sedation, dose-dependent hypnosis, and mild analgesia with minimal respiratory function effects. The aim of this study was to assess the efficacy and safety of dexmedetomidine for pediatric patients during MRI.
MATERIAL AND METHODS: We retrospectively analyzed 87 cases of pediatric sedations for MRI. Dexmedetomidine and a single dose of midazolam were used in all the cases, according to the in-house pediatric sedation protocol for MRI. The patients were divided in to 2 groups: group 1, who reached adequate sedation up to 10 min of induction and group 2, who achieved proper sedation after 10 min.
RESULTS: The median age was 3 years (0-17). The median duration of procedure was 75 min (40-150). The induction of standardized sedation was performed without additional sedatives and proper depth of sedation was reached in the majority of cases (94.3%). Five patients (5.7%) received additional sedative after 10 min of induction. The median time of adequate sedation was 8 min (3-13) after induction, and 51% of patients achieved RASS-4 in 8 min. There was no significant difference between groups 1 and 2. Ten patients (11.5%) experienced bradycardia, regardless of the usage of additional drugs, dexmedetomidine boluses, duration of the procedure, or induction time.
CONCLUSIONS: High-dose dexmedetomidine with a single dose of midazolam might be an effective combination at the induction stage for pediatric sedation for MRI, with very few adverse events. Over 50% of enrolled patients achieved an adequate level of sedation before 10 min. We conclude that induction of dexmedetomidine infusion can be shortened up to 8 min.
Keywords: Dexmedetomidine, Pediatrics, Adolescent, Child, Child, Preschool, Humans, Hypnotics and Sedatives, Infant, Infant, Newborn, Magnetic Resonance Imaging, Midazolam
Background
Magnetic resonance imaging (MRI) has enormous advantages in the examination of pediatric diseases [1]. However, children have a more difficult time tolerating this examination due to fear of enclosed space and loud noises. Most patients under the age of 6 years find it confusing to lie still and follow breathing instructions [2]. Therefore, the majority of children still require sedation to minimize the appearance of motion artifacts for optimal diagnostic quality. Pediatric sedation protocols differ among countries and hospitals and also depend on the particular practitioner [3].
Dexmedetomidine is a potent and highly selective alfa 2-adrenoreceptor agonist [4]. It produces dose-dependent hypnosis, anxiolysis, sedation, and mild analgesia with minimal effects on respiratory function and a relatively short elimination half-life of 2 h [5]. Intravenous dexmedetomidine has very fast distribution in plasma, and 94% of this anesthetic is bound to serum albumin and glycoprotein. Dexmedetomidine is mainly metabolized in the liver through the glucuronidase and cytochrome P450 systems. The vast majority of dexmedetomidine metabolites (about 95%) are eliminated from the body via the renal pathway and the rest are eliminated in feces [6].
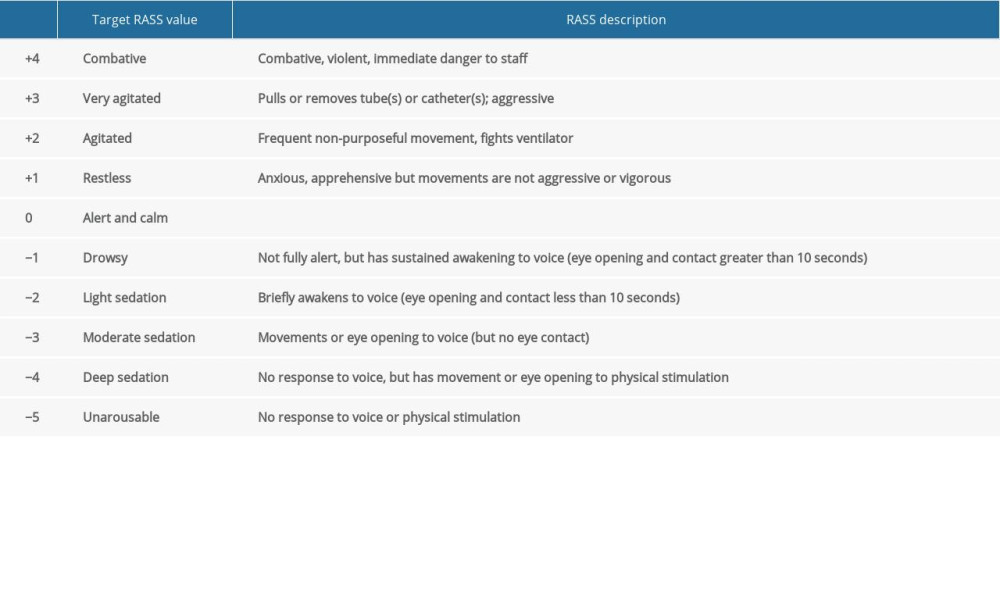
The aim of anesthesia or sedation outside the operating room is to facilitate the diagnostic and/or therapeutic procedure for the patient, suppress consciousness as necessary, and monitor and maintain stable vital functions. Several scales have been developed to determine the level of sedation. Some examples include the Richmond agitation and sedation scale (RAAS) [7–9] (Table 1), Ramsay scale [10], and the American Society of Anesthesiologists (ASA) scale [11]. Deep sedation while maintaining spontaneous breathing is often needed during diagnostic or therapeutic procedures outside the operating room. However, the boundary between deep sedation and general anesthesia is often too narrow and anesthesiologists must always be prepared to ensure airway patency and adequate patient oxygenation in advance [12]. The goals of non-operating room procedures include patient safety and satisfaction, healthcare team satisfaction, scheduling efficiency, and cost-effectiveness [13]. Non-operating room locations have essential differences from operating rooms. Firstly, non-operating room locations are often not adapted for the needs of the anesthesia team, lacking space and equipment, and allowing only limited access to the patient. Secondly, these procedures can generate hazardous environments, such as radiation and magnetic fields. Thirdly, the staff has a very specific nature of work, not extended to work with the anesthesia team, and finally, sometimes these places are not adequately equipped [14]. Therefore, patients need to receive only safe drugs for sedation outside the operating room. Dexmedetomidine has a low profile of harmful events such as apnea, respiratory depression, or airway obstruction and produces sedation that is closer to natural sleep. These are the reasons why dexmedetomidine is increasingly used for procedural sedation all around the world, including the Lithuanian University of Health Sciences Hospital, Kaunas Clinics.
Material and Methods
AIMS AND OBJECTIVES:
The aim of our study was to evaluate the efficacy and safety of dexmedetomidine and single-dose midazolam for pediatric non-operating room sedation in Lithuanian University of Health Sciences Hospital, Kaunas Clinics.
Efficacy was evaluated by 2 criteria: the sedation’s induction time until RAAS-4 is reached, and the need of additional dexmedetomidine boluses or additional medications.
Abnormal changes in vital signs (desaturation, bradycardia, hypotension, with or without the need of additional anesthetist intervention) were the safety criteria.
PATIENTS AND METHODS:
A retrospective single-center study of the use of dexmedetomidine was conducted in the Anesthesiology Department of Lithuanian University of Health Sciences Hospital, Kaunas Clinics. The study was approved by Kaunas Regional Biomedical Research Ethics Committee (ref. n. BEC-MF-114). Informed written parental consent was obtained before enrolment of every patient. All pediatric sedation cases performed outside the operating room were analyzed from July 18, 2019, to December 3, 2020. All cases were managed with dexmedetomidine. Data including patient demographics, drugs dosage, sedation induction time, duration of the procedure, vital signs, and adverse events were collected.
Children corresponding to an American Society of Anesthesiologists (ASA) physical status I–III, aged 0–17 years were enrolled. Normal ranges for pediatric vital signs were used as published by Fleming et al [15]. Heart rate, pulse oximetry, and non-invasive blood pressure were monitored and documented every 5 min during sedation as per standard of care. All patients received additional oxygen of 6 L/min via the nasal cannula. Saturation levels <92% were marked as abnormal [16].
The pediatric sedation protocol for MRI approved in our Anesthesiology Department includes midazolam 0.15 mg/kg i.v. bolus with dexmedetomidine 3 μg/kg per 10 min, followed by a continuous dexmedetomidine infusion of 2 μg/kg/h. Sedation level was monitored every 1 min from the beginning of sedation induction until the RASS scores reached-4. Additional dexmedetomidine boluses or additional medications (fentanyl, propofol, or midazolam) were used in cases when adequate sedation levels (RASS-4) after 10 min of induction were not achieved or when spontaneous movements appeared.
According to the time patients achieved RASS-4, they were divided into 2 groups: group 1, who reached adequate level of sedation up to 10 min of dexmedetomidine infusion, and group 2, who achieved proper sedation level after 10 min. Patients with and without particular adverse effects of sedation were compared.
Exclusion criteria were defined as allergy to any drug included in the protocol, sedation, and mechanical ventilation before the procedure.
STATISTICAL ANALYSIS:
Statistical analysis was performed with SPSS software for Windows, version 20.0. The Kolmogorov-Smirnov test was used to evaluate the normality of distributions. Abnormally distributed data were described using non-parametric statistics and expressed as median with minimum and maximum value (min-max). Categorical variables were summarized using frequencies and percentages. The Mann-Whitney test was used for comparison of groups with and without particular adverse effects of sedation and for groups according to the adequate sedation time achievement (group 1 and group 2). Incidence of adverse effects and additional medications were analyzed with a chi-square test. The level of statistical significance was set as 0.05.
Results
We analyzed 91 cases in which dexmedetomidine was used for pediatric sedation during MRI. Three cases were excluded due to lack of medical data, and 1 case was excluded due to sedation and mechanical ventilation before MRI (final n=87). Demographic characteristics are presented in Table 2.
The majority of patients (n=71, 81.6%) had MRI for suspected or proven neurological disorders (eg, hydrocephalus, epilepsy, oncological disorders), other patients had MRI due to suspected or proven musculoskeletal (n=6, 6.9%), parenchymal organs (n=4, 4.6%), and other (n=6, 6.9%) disorders. The median procedure duration was 75 min (40–150).
Standard sedation induction includes midazolam 0.15 mg/kg i.v. bolus with dexmedetomidine infusion of 3 μg/kg per 10 min. This regimen achieved adequate sedation induction without any additional sedatives in the majority of cases (n=82, 94.3%), but 5 patients (5.7%) received additional dexmedetomidine, propofol, midazolam, or fentanyl doses after 10 min of induction due to insufficient sedation level. The median time when adequate sedation was achieved after the beginning of induction was 8 min (3–13), and 44 (51%) out of 87 patients reached a deep level of sedation (RASS-4) before 10 min (within 8 min).
No cases of desaturation (SpO2 <92%) or hypotension were found. Ten patients (11.5%) had bradycardia during sedation: 5 (5.7%) received 1 dose of atropine 0.02 mg/kg, 3 (3.4%) received 2 doses of atropine, and 2 (2.3%) returned to normal heart rate without further intervention. Nine out of 10 patients who developed bradycardia received a single dose of midazolam and dexmedetomidine induction, and 1 patient received full-dose induction medications and additional weight-adjusted doses of midazolam and propofol.
There were no statistically significant differences in adverse effects between groups who reached adequate level of sedation up to 10 min and longer (
All MRI scanning procedures were performed successfully with adequate levels of sedation using our pediatric sedation protocol for MRI. No of other adverse events were documented during sedation.
Discussion
During diagnostic procedures performed outside the operating room, sedation and anesthesia for children is necessary not only to obtain reliable data and to avoid movement artifacts, but also to reassure children, as they are usually intimidated by the entire process. New technologies have emerged to prevent the use of anesthetics in pediatric patients outside the operating room [17]. However, the need for anesthetics remains the same in most hospitals. Therefore, our aim was to find the safest and most effective way to do as little harm as possible, especially in pediatric patients. Historically, midazolam and chloral hydrate were the most popular sedatives for pediatric sedation [18]. A few authors have compared dexmedetomidine and propofol in children undergoing MRI procedures and revealed that use of propofol can put patients at higher risk of hypotension and desaturation [19]. However, dexmedetomidine appeared as a new medication in everyday clinical practice. Even though dexmedetomidine is already approved for clinical usage in intensive care unit and surgical/procedural sedation in adult patients [20], there is still uncertainty about its use in pediatrics. However, off-label use of dexmedetomidine has been increasing over the past decade in pediatric anesthesiology [21]. Olgun et al [22] tried to use intranasal dexmedetomidine as a solo sedative for pediatric MRI and noticed that dexmedetomidine seemed to be appropriate option for pediatric sedation outside the operating room [19]. Nevertheless, the effective dosage to perform MRI or other long-lasting investigation safely has not been proposed yet. The doses that are used by our protocol are high but have been described previously in the pediatric population [23,24]. Therefore, this drug could have an important role as a primary sedative drug for pediatric MRI or other non-invasive diagnostic procedures in the future.
The ability to maintain upper airway patency and spontaneous breathing while maintaining stable hemodynamics makes dexmedetomidine an appealing option for procedural sedation outside the operating room. There are many studies demonstrating that dexmedetomidine is a good option for non-operating room sedation [23,25,26]. However, recommended doses vary accross different institutions, and identification of the optimal dose still remains a key challenge, especially among children of various ages. Earlier studies have shown that 0.1–0.7 μg/kg/h of dexmedetomidine gives provides effective sedation [27,28]. However, more research indicated that this dose is unlikely to be beneficial for MRI sedation for children when higher doses of dexmedetomidine are required to achieve adequate sedation. Although doses were lower in older reports, higher doses were recently identified and were well tolerated [29].
Tug et al [30] compared 2 different intranasal doses of dexmedetomidine in children for MRI sedation and found that 4 μg/kg of intranasal dexmedetomidine was more effective than 3 μg/kg of intranasal dexmedetomidine. Cozzi et al [31] assessed a combination of single-dose 3 μg/kg intranasal dexmedetomidine and 0.5 μg/kg oral midazolam for pediatric sedation during MRI, finding that addition of oral midazolam improved the efficacy of intranasal dexmedetomidine. Also, Li et al [32] compared intranasal dexmedetomidine and oral chloral hydrate in their meta-analysis and found that dexmedetomidine is an easier to use and more effective sedation method for pediatric patients undergoing diagnostic procedures compared to oral chloral hydrate. Ahmed et al [33] assessed dexmedetomidine in 544 pediatric patients undergoing MRI; 70.2% of all patients received 1 bolus of sedative, while 29.8% were given 2 boluses. Additional drugs (midazolam or fentanyl) were used in 21.5% to suppress involuntary movements and prevent motion artifacts that can impact MRI quality.
Using high doses of dexmedetomidine to maintain adequate sedation for procedures can lead to important hemodynamic instability, especially bradycardia. Gong et al [34] reported that the incidence of bradycardia was 3% when dexmedetomidine was used as the sole sedative. Al-Taher et al [35] used atropine sulfate during premedication and found 0% incidence of bradycardia. The standard pediatric sedation protocol during MRI in our Anesthesiology Department includes midazolam 0.15 mg/kg i.v. bolus with dexmedetomidine 3 μg/kg over 10 min, followed by a continuous dexmedetomidine infusion of 2 μg/kg/h. We analyzed 87 cases of pediatric sedation when a combination of midazolam and dexmedetomidine was used during MRI. Bradycardia was documented in 10 cases (11.5%). Five patients received 1 dose of atropine 0.02 mg/kg and 3 patients received 2 doses. Two children returned to normal heart rate without any additional medications. All patients received supplemental oxygen and sustained normal oxygen saturation (92% or higher), even during short episodes of bradycardia. No cases of hypotension were documented. In summary, dexmedetomidine is a very effective drug and can be safely used at therapeutic doses for pediatric sedation during MRI. Additionally, dexmedetomidine is an effective, extremely safe drug with a low profile of adverse events for pediatric sedation outside the operating room.
Our data indicate that 44 patients (51%) out of 87 reached a deep level of sedation (RASS-4) before 10 min. The median time when adequate sedation was achieved after the beginning of induction was 8 min. We suggest that the duration might be adjusted from 10 min to 8 min for the initial dexmedetomidine bolus.
The current study has some limitations. It was a retrospective, observational, single-center study. The study had a relatively small sample size and the patient population was not homogenous due to different age groups. This may have affected the low incidence of adverse events. The results need to be interpreted with caution and confirmed by larger multicenter studies.
Conclusions
In conclusion, dexmedetomidine with single-dose midazolam offers a safe and effective method for pediatric sedation during MRI. Firstly, dexmedetomidine produces a condition similar to natural sleep and has a low profile for clinically important harmful events such as apnea, respiratory depression, or airway obstruction. The anticipated hemodynamic variability with dexmedetomidine is usually well tolerated. Secondly, dexmedetomidine has a reasonably short half-life, which makes it suitable for use as a single sedative or in combination with other medications. We approved a regimen with midazolam for pediatric sedation during MRI in our Anesthesiology Department. Thirdly, more than 50% of patients achieved an adequate level of sedation prior to 10 min in our study. Therefore, we suggest that the initial duration of dexmedetomidine bolus could be shortened.


References
1. Dore M, Triana Junco P, Bret M, Advantages of cardiac magnetic resonance imaging for severe pectus excavatum assessment in children: Eur J Pediatr Surg, 2018; 28(1); 34-38
2. Dong SZ, Zhu M, Bulas D, Techniques for minimizing sedation in pediatric MRI: J Magn Reson Imaging, 2019; 50(4); 1047-54
3. Ahmad R, Hu HH, Krishnamurthy R, Krishnamurthy R, Reducing sedation for pediatric body MRI using accelerated and abbreviated imaging protocols: Pediatr Radiol, 2018; 48(1); 37-49
4. Naaz S, Ozair E, Dexmedetomidine in current anaesthesia practice-a review: J Clin Diagn Res, 2014; 8(10); GE01-4
5. Weerink MAS, Struys MMRF, Hannivoort LN, Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine: Clin Pharmacokinet, 2017; 56(8); 893-913
6. Li A, Yuen VMY, Goulay-Dufay S, Kwok PCL, Pharmacokinetics and pharmacodynamics of dexmedetomidine: Drug Dev Ind Pharm, 2016; 42(12); 1917-27
7. Sessler CN, Grap MJ, Brophy GM, Multidisciplinary management of sedation and analgesia in critical care: Semin Respir Crit Care Med, 2001; 22(2); 211-25
8. Ely EW, Truman B, Shintani AT, Monitoring sedation status over time in ICU patients: Reliability and validity of the Richmond Agitation-Sedation Scale (RASS): JAMA, 2003; 289(22); 2983-91
9. Sessler CN, Gosnell MS, Grap MJ, The Richmond Agitation-Sedation Scale: Validity and reliability in adult intensive care unit patients: Am J Respir Crit Care Med, 2002; 166(10); 1338-44
10. Ramsay MAE, Savege TM, Simpson BRJ, Goodwin R, Controlled sedation with alphaxalone-alphadolone: Br Med J, 1974; 2(5920); 656-59
11. Xiong J, Gao J, Lancaster JL, Fox PT, Assessment and optimization: Hum Brain Mapp, 1996; 167; 1-2
12. Hinkelbein J, Lamperti M, Akeson J, European Society of Anaesthesiology and European Board of Anaesthesiology guidelines for procedural sedation and analgesia in adults: Eur J Anaesthesiol, 2018; 35(1); 6-24
13. Warner ME, Martin DP, Scheduling the nonoperating room anesthesia suite: Curr Opin Anaesthesiol, 2018; 31(4); 492-97
14. Boggs SD, Barnett SR, Urman RD: Curr Opin Anaesthesiol, 2017; 30(6); 644-51
15. Fleming S, Thompson M, Stevens R, Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: A systematic review of observational studies: Lancet (London, England), 2011; 377(9770); 1011-18
16. Fouzas S, Priftis KN, Anthracopoulos MB, Pulse oximetry in pediatric practice: Pediatrics, 2011; 128(4); 740-52
17. Serai SD, Hu HH, Ahmad R, Newly developed methods for reducing motion artifacts in pediatric abdominal MRI: Tips and pearls: Am J Roentgenol, 2020; 214(5); 1042-53
18. Kamat PP, McCracken CE, Simon HK, Trends in outpatient procedural sedation: 2007–2018: Pediatrics, 2020; 145(5); e20193559
19. Koroglu A, Teksan H, Sagir O, Yucel A, A comparison of the sedative, hemodynamic, and respiratory effects of dexmedetomidine and propofol in children undergoing magnetic resonance imaging: Anesth Analg, 2006; 103(1); 63-67
20. Yu S-B, Dexmedetomidine sedation in ICU: Korean J Anesthesiol, 2012; 62(5); 405-11
21. van Hoorn CE, Flint RB, Skowno J, Off-label use of dexmedetomidine in paediatric anaesthesiology: An international survey of 791 (paediatric) anaesthesiologists: Eur J Clin Pharmacol, 2021; 77(4); 625-35
22. Olgun G, Ali MH, Use of intranasal dexmedetomidine as a solo sedative for MRI of infants: Hosp Pediatr, 2018; 8(2); 68-71
23. Mason KP, Zurakowski D, Zgleszewski SE, High dose dexmedetomidine as the sole sedative for pediatric MRI: Paediatr Anaesth, 2008; 18(5); 403-11
24. Lee S, Dexmedetomidine: Present and future directions: Korean J Anesthesiol, 2019; 72(4); 323-30
25. Kiski D, Malec E, Schmidt C, Use of dexmedetomidine in pediatric cardiac anesthesia: Curr Opin Anaesthesiol, 2019; 32(3); 334-42
26. Goswami M, Sangal A, Rahman B, Chawla S, Comparison of the safety and efficacy of dexmedetomidine with midazolam for the management of paediatric dental patients: A systematic review: J Indian Soc Pedod Prev Dent, 2021; 39(3); 233-39
27. Triltsch AE, Welte M, Von Homeyer P, Bispectral index-guided sedation with dexmedetomidine in intensive care: A prospective, randomized, double blind, placebo-controlled phase II study: Crit Care Med, 2002; 30(5); 1007-14
28. Tobias JD, Berkenbosch JW, Russo P, Additional experience with dexmedetomidine in pediatric patients: South Med J, 2003; 96(9); 871-75
29. Li LQ, Wang C, Xu HY, Effects of different doses of intranasal dexmedetomidine on preoperative sedation and postoperative agitation in pediatric with total intravenous anesthesia undergoing adenoidectomy with or without tonsillectomy: Medicine (Baltimore), 2018; 97(39); e12140
30. Tug A, Hanci A, Turk HS, Comparison of two different intranasal doses of dexmedetomidine in children for magnetic resonance imaging sedation: Paediatr Drugs, 2015; 17(6); 479-85
31. Cozzi G, Monasta L, Maximova N, Combination of intranasal dexmedetomidine and oral midazolam as sedation for pediatric MRI: Paediatr Anaesth, 2017; 27(9); 976-77
32. Li L, Zhou J, Yu D, Intranasal dexmedetomidine versus oral chloral hydrate for diagnostic procedures sedation in infants and toddlers: A systematic review and meta-analysis: Medicine (Baltimore), 2020; 99(9); e19001
33. Ahmed SS, Unland T, Slaven JE, Nitu ME, High dose dexmedetomidine: Effective as a sole agent sedation for children undergoing MRI: Int J Pediatr, 2015; 2015; 397372
34. Gong M, Man Y, Fu Q, Incidence of bradycardia in pediatric patients receiving dexmedetomidine anesthesia: A meta-analysis: Int J Clin Pharm, 2017; 39(1); 139-47
35. Al Taher WMA, Mansour EE, El Shafei MN, Comparative study between novel sedative drug (dexmedetomidine) versus midazolam – propofol for conscious sedation in pediatric patients undergoing oro-dental procedures: Egyptian Journal of Anaesthesia, 2019; 26(4); 299-304
In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387