18 October 2022: Review Articles
Review of the Long-Term Outcomes of Guided Bone Regeneration and Autologous Bone Block Augmentation for Vertical Dental Restoration of Dental Implants
Eliza Drăgan1ABCDF*, Alexandru Nemţoi2EDOI: 10.12659/MSM.937433
Med Sci Monit 2022; 28:e937433






Abstract
ABSTRACT: Vertical bone resorption is a frequent consequence of tooth loss. Hence, implant-supported restorations imply, first of all, bone reconstruction. We aimed to review the current status of guided bone regeneration and autologous bone block augmentation for vertical dental restoration of dental implants. This review identified that between 2009 and 2022 there were few clinical studies that included more than 10 patients and a follow-up period of more than 5 years after bone restoration. The highest vertical bone gain was reported in the autologous bone grafting technique (4-7.6 mm), whereas the minimum augmentation was reported for one of the guided bone regeneration techniques. When comparing intraoral to extraoral bone blocks, the highest values for the mean vertical bone gains were obtained in the cases in which intraoral bone blocks were used as graft material. The highest rate of bone resorption was observed in the extraoral bone block group. Implant survival rate was not significantly influenced by surgical technique. Complications had a higher incidence in autologous bone block augmentation studies. Soft tissue recession showed similar results for guided bone regeneration as for autologous bone block augmentation. Vertical ridge augmentation is a predictable option for the reconstruction of alveolar ridges with severe atrophy, but complications can appear.
Keywords: Alveolar Ridge Augmentation, Dental Implants, Osseointegration, Bone Resorption, Bone Transplantation, Humans, Treatment Outcome
Background
Many surgical techniques are used for treating vertical bone deficiencies using autologous bone or different biomaterials, vertical-guided bone regeneration (GBR) procedures, alveolar distraction osteogenesis, titanium mesh, and onlay bone grafts. While the success of vertical augmentation techniques have been demonstrated with different techniques, the number of complications and failures of the augmentation procedure is still significant and includes postoperative morbidity, postoperative pain, swelling, and graft resorption [1]. It has been demonstrated that the autologous onlay bone graft is a predictable procedure, although the long-term dimensional stability of the grafted bone is not yet known [2]. Autogenous bone, with its osteogenic, osteoinductive, and osteoconductive characteristics, is considered the criterion standard in bone regeneration procedures. It contains osteoblasts, osteoclast precursor cells, undifferentiated mesenchymal cells, and monocytes, which promote bone remodeling and the formation of new bone. However, donor-site morbidity, limited available quantities, unpredictable graft resorption, and the need to include additional surgical sites are unavoidable disadvantages [3]. Autogenous bone grafts can be harvested from the patient’s iliac crest, mandibular ramus, or other intraoral sites. The donor site is chosen based on the volume of graft material required [4].
Osteogenesis is a process that takes place when osteoprogenitor cells in the graft material can survive bone transplantation and differentiate into young cells (osteoblasts), and later into adult cells (osteocytes). Osteoinduction occurs when undifferentiated mesenchymal cells from native bone are induced into osteoblasts or chondroblasts to develop new bone in the area of interest.
This is often dependent on bone morphogenic proteins. Osteoconductive material is defined as a material that encourages bone formation from already existing bone or differentiated mesenchymal cells via scaffolding [4].
The protocol for guided bone implies the prevention of undesirable, non-osteogenic cells from growing into the bony defect by providing a mechanical barrier. There is evidence for the high success rate of GBR in promoting vertical bone augmentation [2].
Vertical bone augmentation techniques are demanding because angiogenesis must be done at a significant distance from existing bone for new bone to be formed. Also, a correct flap design and tension-free closure must be ensured [5].
There are no published studies to compare GBR and autologous bone block augmentation (ABB), in terms of long-term outcome and predictability of vertical ridge augmentation.
In this article, we aimed to review the current status of GBR and ABB for vertical dental restoration of dental implants.
Augmentation Methods
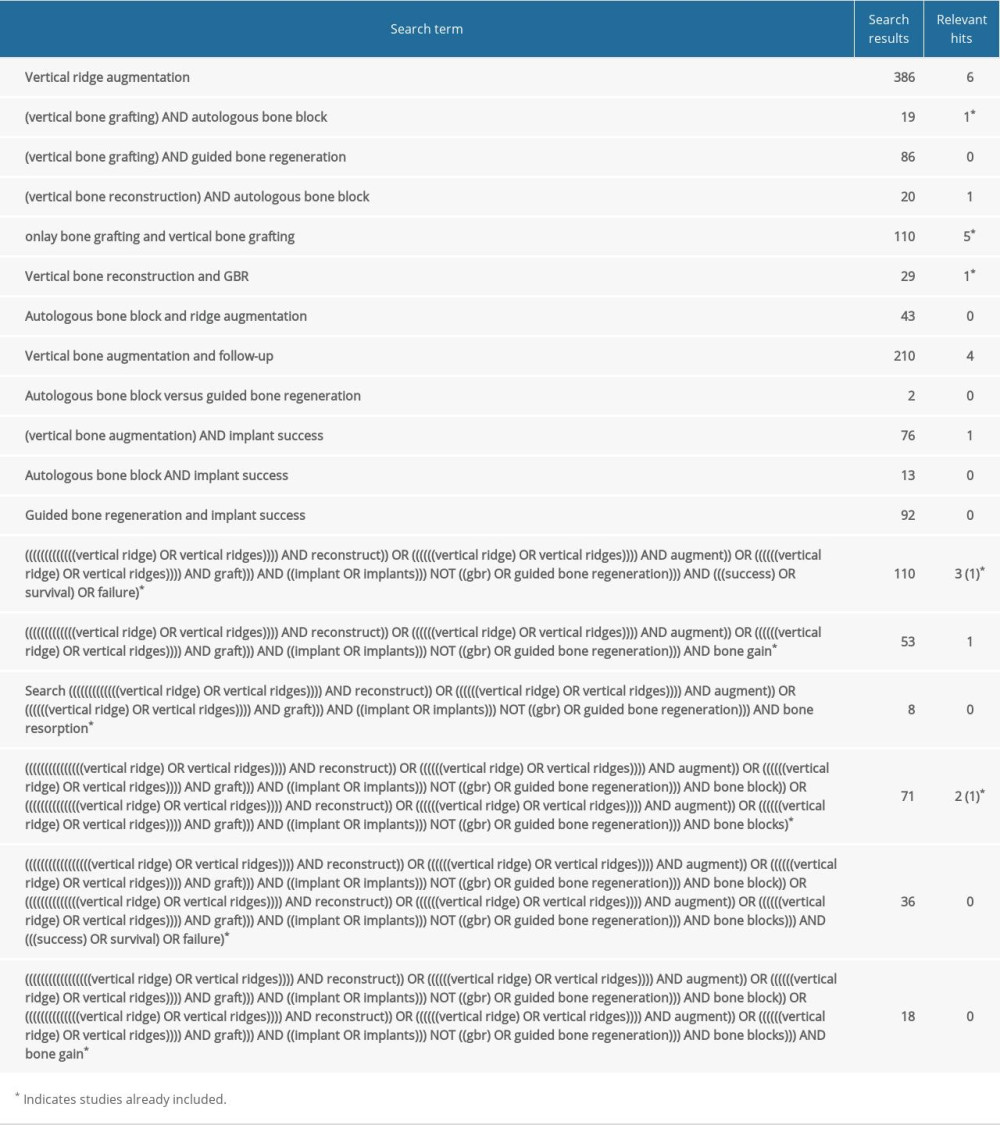
This review identified that between 2009 and 2022 there were few clinical studies that included more than 10 patients and a follow-up period of more than 5 years after bone restoration.
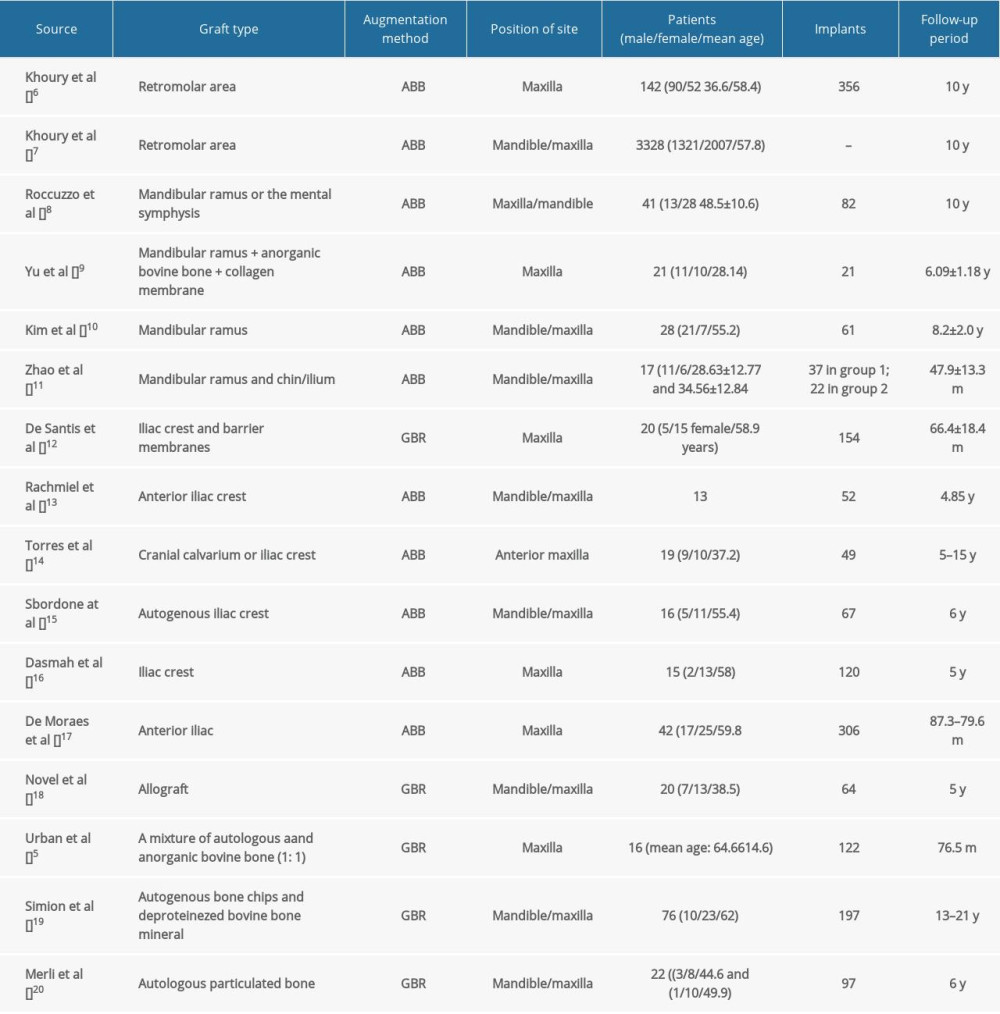
The characteristics of augmentation methods, such as type of graft, position of the site, surgical technique, number of implants, and follow-up period, are summarized in Table 1. The surgical site varied among studies; however, in most of the studies, there was a preference for the maxilla. The follow-up period ranged from 5 to 21 years.
Among the most relevant clinical studies, 75% of them utilized ABB, with extraoral and intraoral locations distributed almost evenly among them. Only 25% of the studies used GBR.
While the preferred technique in ABB studies was the onlay technique, in the GBR studies, the space was filled with graft material and covered by a resorbable or non-resorbable membrane [6].
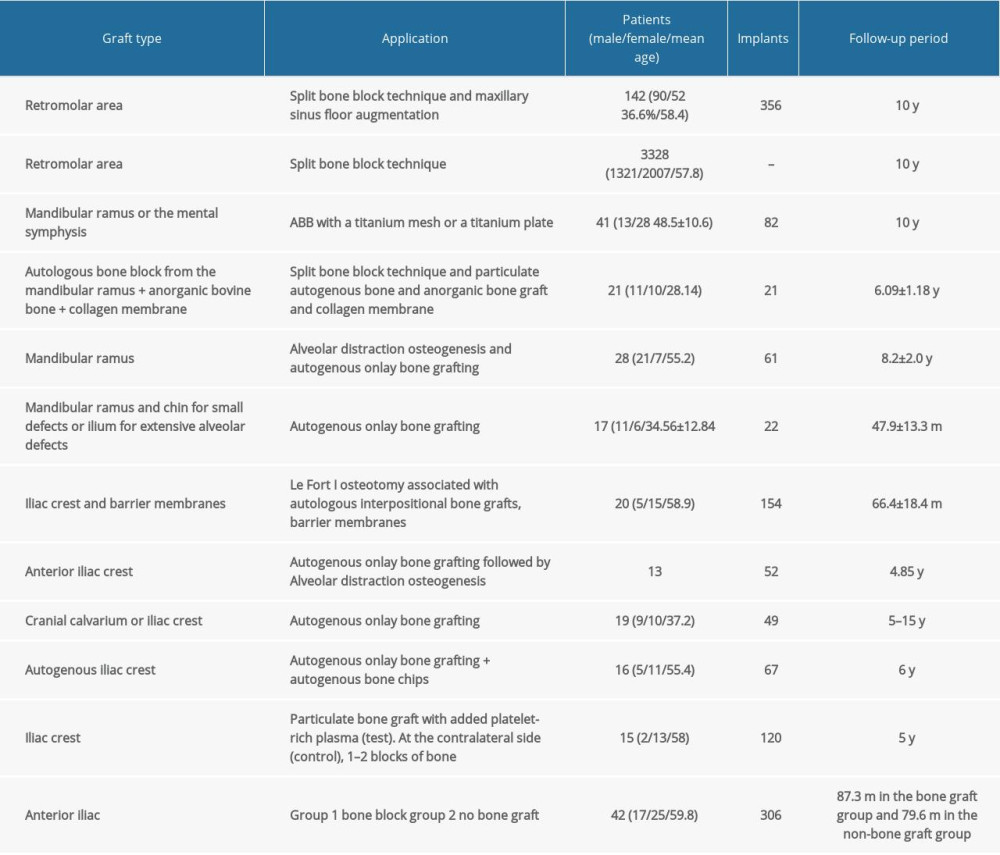
The most used surgical technique for intraoral ABB was the split bone block technique using bone blocks from the linia obliqua externa (mandibular ramus; Table 2).
For extraoral ABB, the preferred surgical technique was onlay bone grafting using bone harvested from the iliac crest. The average time required to harvest a bone block was 6.5±2.5 min. The mean volume of the harvested bone graft was 1.9±0.9 cm3. The surgical scars in the mandibular donor site disappeared radiographically within 6 to 12 months, but the lamina dura of the external oblique ridge had not regenerated; exceptions were patients in whom reimplantation of half the bone block was performed (Table 3).
The GBR techniques are represented by autologous particulate bone from areas adjacent to the implant site, bone collected during the implant preparation site, or anorganic bovine bone that is covered with resorbable collagen membranes supported by osteosynthesis plates or with non-resorbable titanium, reinforced e-PTFE barriers.
Influence of Augmentation Method on Clinical Parameters
BONE GAIN:
Key clinical studies showed that GBR resulted in a mean bone gain of 5.16±1.8 mm [5], and resorbable membrane, 2.14 mm, and non-resorbable, 2.48 mm [7]. In some clinical studies, the implants were inserted in a second-stage surgery [5], while in the study by Merli et al, the implants were inserted in the same stage [7].
Considering the type of autologous bone used, the mean vertical bone gain ranged from 4 to 7.6 mm for intraoral ABB. The low value was obtained when the healing time was 6 months, while the high value was obtained after a healing time of 3 months.
For extraoral ABB, the mean vertical bone gain ranged from 5.3 to 7 mm. The low value was assessed after a mean follow-up of 4.85 years, while the high values were after a follow-up of 5 to 15 years.
EFFECT OF MEMBRANE:
Several clinical studies have shown that, for ABB, the vertical mean bone gain is higher (5.12 mm) when using a resorbable collagen membrane than when using a non-resorbable membrane (4 mm) [8–11]. In the GBR studies, resorbable and non-resorbable membranes were used. The study by Merli et al is the only one that made a comparison between the 2 types of membranes, with results showing that there was no difference in the mean vertical bone gain when comparing resorbable (2.16 mm) to non-resorbable membranes (2.48 mm) [7]. The results of the study by Urban et al differed, with a mean vertical bone gain of 5.16±1.8 mm; however, the authors did not specify the type of membrane used [5].
EFFECT OF GRAFT MATERIAL:
Based on the type of intervention, the largest vertical bone gain was noted in the ABB technique (4–7.6 mm), whereas the smallest augmentation was reported for one of the GBR techniques: autologous particulate bone from areas adjacent to the implant site or collected during the implant preparation site and covered with resorbable collagen membranes supported by osteosynthesis plates or non-resorbable titanium, reinforced e-PTFE barriers (2.16 mm) [7].
When comparing intraoral with extraoral techniques, the highest values for the mean vertical bone gain were obtained in the cases in which intraoral bone blocks were used as graft material.
EFFECT OF LOCATION:
Implants inserted in the grafted maxillae with autologous bone grafts in cases of severe maxillary atrophy were found to be just as efficient as implants installed in maxillae without bone graft [12]. In some clinical GBR studies, there are no results regarding the influence of the surgical site (maxilla/mandible) on the outcome.
Bone Resorption
The amount of bone resorption from implant placement was calculated from the top of the shoulder of the implant fixture to the most coronal level of direct bone-to-implant contact. To minimize the distortion factor on panoramic radiographs, a calibration procedure was performed according to the actual dimension of the implants. The real bone resorption amount was calculated using the following formula: real bone resorption amount=actual implant length radiologic bone resorption amount/radiologic implant length.
Recent key clinical studies assessed GBR techniques and found bone resorption ranged from 0.49 to 3.16 mm. Some of the clinical studies evaluated intraoral ABB, and results of bone resorption ranged from 0.58±0.57 mm up to 2.3±1.5. For extraoral ABB, some of the clinical studies declared bone resorption ranging from 1.24±0.87 mm up to 3.1±2.21 mm. One clinical study reported complete resorption of the graft (105.5%) [13].
There have been clinical studies with the iliac crest [14,15] and with GBR [16] that showed that most of the marginal bone resorption occurs during the first year of loading, whereas the radiological measurements after 5 years of loading revealed only limited additional resorption. Zhao et al noticed a meaningful relationship between oral hygiene and bone resorption [17].
Patients with a history of periodontitis showed statistically significantly greater bone loss [9]. There were active smokers with complete graft resorption. No graft resorption was associated with graft infection or graft exposure [18]. Bone gain and bone resorption were evaluated using cone beam computed tomography only in some clinical studies [12,14,19]. In summary, the highest rate of bone resorption was observed in the extraoral bone block groups.
Graft Failure Rates
Osseointegration of the graft implies no pain or discomfort, graft stability at the time of implant placement, absence of infection during the healing period, and absence of radiographic signs of bone graft resorption [10]. Graft failure is defined as the inability to insert the implant [13].
Sbordone et al assessed the differences in volumetric measurements and the percentages of remaining bone in the extraoral ABB and noticed a progressive resorption rate of almost the entire osseous graft in the maxilla and mandible, with resorption rates of 105.5% for the maxilla and 87% for the mandible [13].
Torres et al analyzed the amount of bone resorption in the extraoral ABB and noticed a gradual increase in marginal bone level over time, peaking at 11 years after surgery before reaching a stable value [14]. No graft resorption was associated with graft infection or graft exposure. When graft failure was reported, the origin was the iliac crest and the calvarial bone. In some studies, patients with congenital hypodontia (38%) presented a small percentage of graft failure, and this result reflects the osteogenic potential of autologous onlay bone graft in such defects.
Graft failure was mentioned only in the clinical studies in which the bone was harvested from the iliac crest. The implant survival rate was more than 90%. Most of the studies did not evaluate graft failure rates, but implant failures that ranged from 0 to 30 implants.
Perspectives
There is a wide range of surgical techniques and graft materials described in the literature that obtain vertical bone gain. Therefore, our aim in this study was to analyze the literature from 2009 to 2022 to identify the best technique offering results for successful implant placement and long-term function. This review showed that both GBR and ABB significantly augment the vertical crest dimension, but the result was influenced by the type of surgery.
The highest values for the mean vertical bone gain, 4 to 7.6 mm, were obtained in cases in which intraoral bone blocks were used as graft material with the split bone block technique. The second best was 5.3 to 7 mm for autologous onlay bone block graft with extraoral bone block, and the third was 2.16 to 5.16±1.8 mm for GBR.
These results generally agree with the current comparative literature on bone graft materials. One reason for this could be the use of the soft tissue approach tunneling technique and also the fact that the author did not use any artificial membranes [8]. The clinical use of ABB seems to be indispensable for a predictable vertical reconstruction.
If we plan a standard-length implant, for a ridge less than 8 mm, intraoral bone blocks and the split bone block technique is the most reliable approach to achieve vertical bone gain.
The regenerative and remodeling outcomes of block grafting might be influenced by the region of placement. Host vascular supply, which is the most important biological activity required for bone formation and graft integration, has been reported to be more extensive in the maxilla than in the mandible, which might be the reason for good integration during implant placement in the maxilla [20]. This means that bone augmentation is more predictable in the maxilla.
Supplementary precautions should be taken in the mandible to improve the vascular supply with an appropriate flap design and suture technique to avoid wound dehiscence and the use of autologous bone as graft material.
The highest rate of bone resorption was observed in the extraoral bone block group (105.5% and 87% for the upper and lower arches, respectively). In the GBR and intraoral ABB techniques, the results were similar, with a low rate for resorption: 0.49 to 3.16 mm in the GBR group, and 0.58 to 2.3 mm in the intraoral ABB group.
The outcome of this review could be influenced by the fact that the included studies mixed different clinical conditions [5]. Most of the included studies also failed to report the initial bone height before implant placement. This means that the rate of resorption before implant placement was not considered, and this could influence our results, because bone resorption was most pronounced during healing before implant placement [19]. These results generally agree with the current comparative literature. The factors that influence bone resorption can be related to the donor site, handling, size of the defect, size of the graft, surgical technique, time of implant placement, healing protocol, prosthetic factors, or patient-related factors [15]. This is an important aspect, because we have to choose the advocated technique with minimum resorption and complications. Extraoral ABB should be limited to cases in which extensive bone augmentation is needed.
The healing period, type of bone block (monocortical, bicortical, or tricortical) and type of bone graft (particulated or bone block) are important factors that could influence bone resorption. For autologous bone blocks, a healing period of 3 months could prevent bone resorption. Also, grafted tricortical blocks harvested from donor sites instead of bicortical, monocortical cancellous, or particulated iliac blocks and grafting with bone blocks containing greater volumes of cortical bone might prevent severe resorption [20]. These results generally agree with the current comparative literature.
The risk of resorption is reduced in cases of cortical bone blocks, but the osseointegration can be influenced owing to the limited revascularization and poor regeneration potential of the block [20].
Surgeons should consider graft resorption when planning surgery. Graft failure was mentioned only in 2 studies, in which the bone was harvested from the iliac crest. In both studies, the implant survival rate was more than 90%. This agrees with other studies. Resorption in the iliac bone grafting group was significantly higher than that in the GBR group [20]. Johansson et al reported a mean resorption rate of 50% at onlay autogenous iliac bone-grafted maxillary sites after 6 months of healing [21]. In another study, Sbordone et al reported an average resorption rate of 42% in iliac block grafts placed in the anterior maxilla after 1 year of follow-up [22]. When comparing iliac to calvarium, Mertens et al showed that calvarial bone has significantly higher stability than iliac crest bone grafts [23].
The same factors that were attributed to bone resorption and mentioned above can be implicated in graft failure. Although there was a complete remodeling of the bone graft, the survival rate of the dental implants was at a maximum, suggesting that bone graft resorption did not imply a loss of implant stability; this was most likely due to the preservation of osseointegration, at least in its apical portion, where, probably, only native bone was present [13].
This means that the decision to use extraoral ABB as a treatment choice should be based on patient-specific considerations: if the cone beam computed tomography shows that sufficient intraoral autogenous bone can be harvested, it should be the preferred technique, and not extraoral ABB.
In a recent clinical study, the use of root structures derived from autogenous extracted teeth and ABB grafts appear to be associated with comparable efficacy and safety outcomes for combined vertical and horizontal alveolar ridge augmentation [24].
In another study, based on microcomputed tomography analysis, 2 different surgical approaches, like guided bone regeneration with titanium-reinforced polytetrafluoroethylene membrane and guided bone regeneration with titanium mesh and collagen membrane, facilitated the obtention of approximately 30% of newly formed bone with the same microarchitecture [25]. In this study, native bone influenced the quality and microarchitecture of the obtained bone, irrespective of the technique used [25]. This represents a very important factor that needs to be considered in future analysis.
Regarding the use of a membrane in the GBR technique, resorbable or non-resorbable, the results are contradictory. Urban et al reported that resorbable membranes were more likely to develop complications than non-resorbable membranes [5]. Urban used resorbable and non-resorbable membranes that have been proven to exclude fibroblast-like cell ingrowth into the grafted defect. The reinforcement of the membrane with titanium strips makes it more moldable and stable for vertical bone augmentation, especially in large-sized defects. Moreover, in the authors’ experience, wound dehiscence and membrane exposure typically occur in the proximity of the dental structures [5]. In contrast, the results of Merli et al showed that there was no difference in complications when comparing resorbable to non-resorbable membranes [7].
In the ABB technique, it is less common to use a membrane. Yu et al reported that the lower resorption rate might be explained by the use of Bio-Oss and collagen membranes to cover the reconstruction site [10]. De Santis et al used a barrier membrane in Le Fort I osteotomy and increased the predictability of the procedure. Their results show that implant failure might be avoided by placing a membrane [11]. On the contrary, Khoury et al used autogenous bone in the form of a thin block in combination with autogenous chips without any biomaterial or membrane and found clinical volume stability as well as a success rate above 95% [26].
Another systematic review with a follow-up period of at least 4 to 5 years concluded there was a trend that the onlay technique, alveolar distraction, and GBR were stable for at least 4 to 5 years [27].
There are many factors for success in GBR, including patient and defect analysis, blood supply, flap passivation, membrane fixation, and primary closure [27]. The timing of healing should always be greater than 6 months, and soft-tissue management seems to be another important factor for long-term success [28].
Conclusions
Vertical bone augmentation is a predictable option for the reconstruction of alveolar ridges with bone deficiency. Considering the results from the studies included in this systematic review, no clear conclusions can be made regarding the superiority of any technique, whether GBR or ABB.
References
1. Tanaka K, Sailer I, Kataoka Y, Nogami S, Takahashi T, Sandwich bone graft for vertical augmentation of the posterior maxillary region: A case report with 9-year follow-up: Int J Implant Dent, 2017; 3(1); 20
2. Annibali S, Bignozzi I, Sammartino G, Horizontal and vertical ridge augmentation in localized alveolar deficient sites: A retrospective case series: Implant Dent, 2012; 21(3); 175-85
3. Al-Nawas B, Schiegnitz E, Augmentation procedures using bone substitute materials or autogenous bone – a systematic review and meta-analysis: Eur J Oral Implantol, 2014; 7; S219-34
4. Chavda S, Levin L, Human studies of vertical and horizontal alveolar ridge augmentation comparing different types of bone graft materials: A systematic review: J Oral Implantol, 2018; 44(1); 74-84
5. Urban IA, Monje A, Lozada JL, Wang HL, Long-term evaluation of peri-implant bone level after reconstruction of severely atrophic edentulous maxilla via vertical and horizontal guided bone regeneration in combination with sinus augmentation: A case series with 1 to 15 years of loading: Clin Implant Dent Relat Res, 2017; 19(1); 46-55
6. Kim JW, Cho MH, Kim SJ, Kim MR, Alveolar distraction osteogenesis versus autogenous onlay bone graft for vertical augmentation of severely atrophied alveolar ridges after 12 years of long-term follow-up: Oral Surg Oral Med Oral Pathol Oral Radiol, 2013; 116(5); 540-49
7. Merli M, Moscatelli M, Mariotti G, Bone level variation after vertical ridge augmentation: Resorbable barriers versus titanium-reinforced barriers. A 6-year double-blind randomized clinical trial: Int J Oral Maxillofac Implants, 2014; 29(4); 905-13
8. Khoury F, Hanser T, Mandibular bone block harvesting from the retromolar region: A 10-year prospective clinical study: Int J Oral Maxillofac Implants, 2015; 30(3); 688-97
9. Roccuzzo M, Savoini M, Dalmasso P, Ramieri G, Long-term outcomes of implants placed after vertical alveolar ridge augmentation in partially edentulous patients: A 10-year prospective clinical study: Clin Oral Implants Res, 2017; 28(10); 1204-10
10. Yu H, Chen L, Zhu Y, Qiu L, Bilamina cortical tenting grafting technique for three-dimensional reconstruction of severely atrophic alveolar ridges in anterior maxillae: A 6-year prospective study: J Craniomaxillofac Surg, 2016; 44(7); 868-75
11. De Santis D, Trevisiol L, D’Agostino A, Guided bone regeneration with autogenous block grafts applied to Le Fort I osteotomy for treatment of severely resorbed maxillae: A 4- to 6-year prospective study: Clin Oral Implants Res, 2012; 23(1); 60-69
12. de Moraes PH, Olate S, Lauria A, 8–10 year follow-up survival of dental implants in maxillae with or without autogenous bone graft reconstruction: Int J Clin Exp Med, 2015; 8(10); 19282-89
13. Sbordone C, Toti P, Guidetti F, Volume changes of iliac crest autogenous bone grafts after vertical and horizontal alveolar ridge augmentation of atrophic maxillas and mandibles: A 6-year computerized tomographic follow-up: J Oral Maxillofac Surg, 2012; 70(11); 2559-65
14. Torres Y, Raoul G, Lauwers L, Ferri J, The use of onlay bone grafting for implant restoration in the extremely atrophic anterior maxilla. A case series: Swiss Dent J, 2019; 129(4); 274-85
15. Dasmah A, Thor A, Ekestubbe A, Marginal bone-level alterations at implants installed in block versus particulate onlay bone grafts mixed with platelet-rich plasma in atrophic maxilla. A prospective 5-year follow-up study of 15 patients: Clin Implant Dent Relat Res, 2013; 15(1); 7-14
16. Simion M, Ferrantino L, Idotta E, Zarone F, Turned implants in vertical augmented bone: A retrospective study with 13 to 21 years follow-up: Int J Periodontics Restorative Dent, 2016; 36(3); 309-17
17. Zhao K, Wang F, Huang W, Comparison of dental implant performance following vertical alveolar bone augmentation with alveolar distraction osteogenesis or autogenous onlay bone grafts: A retrospective cohort study: J Oral Maxillofac Surg, 2017; 75(10); 2099-114
18. Rachmiel A, Emodi O, Aizenbud D, Two-stage reconstruction of the severely deficient alveolar ridge: Bone graft followed by alveolar distraction osteogenesis: Int J Oral Maxillofac Surg, 2018; 47(1); 117-24
19. Novell J, Novell-Costa F, Ivorra C, Five-year results of implants inserted into freeze-dried block allografts: Implant Dent, 2012; 21(2); 129-35
20. Gultekin BA, Cansiz E, Borahan MO, Clinical and 3-dimensional radiographic evaluation of autogenous iliac block bone grafting and guided bone regeneration in patients with atrophic maxilla: J Oral Maxillofac Surg, 2017; 75(4); 709-22
21. Johansson B, Grepe A, Wannfors K, Hirsch JM, A clinical study of changes in the volume of bone grafts in the atrophic maxilla: Dentomaxillofac Radiol, 2001; 30(3); 157-61
22. Sbordone L, Toti P, Menchini-Fabris GB, Sbordone C, Volume changes of autogenous bone grafts after alveolar ridge augmentation of atrophic maxillae and mandibles: Int J Oral Maxillofac Surg, 2009; 38(10); 1059-65
23. Mertens C, Decker C, Seeberger R, Early bone resorption after vertical bone augmentation – a comparison of calvarial and iliac grafts: Clin Oral Implants Res, 2013; 24(7); 820-25
24. Schwarz F, Obreja K, Mayer S, Efficacy of autogenous tooth roots for a combined vertical and horizontal alveolar ridge augmentation and staged implant placement. A prospective controlled clinical study: J Clin Periodontol, 2022; 49(5); 496-505
25. Cucchi A, Vignudelli E, Sartori M, A microcomputed tomography analysis of bone tissue after vertical ridge augmentation with non-resorbable membranes versus resorbable membranes and titanium mesh in humans: Int J Oral Implantol (Berl), 2021; 14(1); 25-38
26. Khoury F, Hanser T, Three-dimensional vertical alveolar ridge augmentation in the posterior maxilla: A 10-year clinical study: Int J Oral Maxillofac Implants, 2019; 34(2); 471-80
27. Keestra JA, Barry O, Jong Ld, Wahl G, Long-term effects of vertical bone augmentation: A systematic review: J Appl Oral Sci, 2016; 24(1); 3-17
28. Cucchi A, Chierico A, Fontana F, Statements and recommendations for guided bone regeneration: Consensus report of the Guided Bone Regeneration Symposium Held in Bologna, October 15 to 16, 2016: Implant Dent, 2019; 28(4); 388-99
In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387