22 December 2022: Clinical Research
Impact of the De Ritis Ratio on the Prognosis of Patients with Stable Coronary Artery Disease Undergoing Percutaneous Coronary Intervention
Kai WangDOI: 10.12659/MSM.937737
Med Sci Monit 2022; 28:e937737






Abstract
BACKGROUND: The aim of this study was to emphasize the impact of the aspartate aminotransferase-to-alanine aminotransferase ratio (De Ritis ratio) on the prognosis of patients with stable coronary artery disease (SCAD) undergoing percutaneous coronary intervention (PCI).
MATERIAL AND METHODS: Patients with SCAD who underwent elective PCI at Shinonoi General Hospital were included. SCAD was defined as epicardial coronary artery diameter stenosis ≥90% or epicardial coronary artery diameter stenosis ≥75% accompanied by symptoms or stress-induced myocardial ischemia. Clinical data were collected, and cardiovascular events were followed after discharge. One-way Cox proportional risk analysis was performed to assess the risk stratification value of the De Ritis ratio, using major adverse cardiac and cerebrovascular events (MACCE) and all-cause mortality as the primary and secondary endpoints, respectively. The independent risk stratification value was evaluated by multivariate Cox proportional risk analysis.
RESULTS: Among 204 patients with SCAD undergoing PCI, during a median follow-up period of 706 days (24 months), 13.7% (28/204) patients experienced MACCE, and 8.8% (18/204) experienced all-cause mortality. Multifactorial Cox regression analysis revealed that a high De Ritis ratio was an independent risk factor for MACCE (HR=2.96, 95% CI: 1.29-6.78, P=0.01) and all-cause mortality (HR=3.61, 95% Cl: 1.31-9.86, P=0.012). The sensitivity analysis further confirmed the incremental value of the De Ritis ratio for adverse cardiovascular events.
CONCLUSIONS: A high De Ritis ratio was an independent and valuable risk stratification factor for MACCE and all-cause mortality in patients with SCAD after PCI.
Keywords: Alanine Transaminase, Aspartate Aminotransferases, Coronary Artery Disease, Prognosis, Humans, percutaneous coronary intervention, Constriction, Pathologic, Treatment Outcome, Coronary Stenosis
Background
Percutaneous coronary intervention (PCI) has reduced the incidence of major adverse cardiovascular and cerebrovascular events (MACCE) in patients with stable coronary artery disease (SCAD) with sufficient evidence of ischemia; however, some patients still have a poor prognosis [1]. Recent studies have shown that a high aspartate aminotransferase-to-alanine aminotransferase ratio (De Ritis ratio) is associated with a worse prognosis in patients with acute myocardial infarction [2,3] and acute heart failure [4]. Study also have shown that an elevated De Ritis ratio on admission was significantly associated with intensive care unit mortality and hospital mortality after cardiac arrest [5]. The De Ritis ratio reflects the severity of hepatic insufficiency [6], and patients with coronary artery disease complicated by hepatic insufficiency have a high incidence of perioperative complications [7,8]. However, research on the relationship between the De Ritis ratio and the prognosis of patients with SCAD undergoing PCI is still lacking. This study aimed to evaluate the relationship between the De Ritis ratio and prognosis in patients undergoing elective PCI for SCAD.
Material and Methods
STUDY POPULATION:
The population in this study was obtained from a single-center retrospective cohort using open data [9]. The study included patients with SCAD who underwent elective PCI at Shinonoi General Hospital from October 2014 to October 2017. SCAD was defined as epicardial coronary artery diameter stenosis ≥90% or epicardial coronary artery diameter stenosis ≥75% accompanied by exercise-induced chest pain or stress-induced myocardial ischemia, confirmed by any clinical stress test. Patients with diagnoses of old myocardial infarction and malignant tumors were excluded. Finally, 204 patients were included in this study. The study was approved by the Ethics Committee of Shinonoi General Hospital, and written informed consent was obtained from all patients. Our study was a secondary analysis based on the data described above, and all patient information was kept anonymous. Therefore, informed patient consent and ethics committee approval were not required.
DATA COLLATION AND VARIABLE DEFINITION:
Clinical features, including clinical characteristics, medical history, major risk factors for coronary artery disease, complications, laboratory tests, electrocardiogram, echocardiography, angiography data, and discharge medications, were collected. A multivessel lesion was defined as a 3-vessel lesion. The patients were subsequently followed up after discharge to document all-cause mortality, non-fatal myocardial infarction, and non-fatal stroke outcomes. The main endpoint of this study was MACCE, including all-cause mortality, non-fatal myocardial infarction, and non-fatal stroke. The secondary endpoint was all-cause mortality.
STATISTICAL ANALYSIS:
Continuous variables are expressed as mean and standard deviation, and the
Results
POPULATION INFORMATION:
A total of 204 patients who underwent PCI for SCAD were included in the study (Table 1). Among these patients (142 men, 69.6%), 74.0% had hypertension and 35.8% had diabetes mellitus. The high De Ritis ratio group had a higher age and lower BMI, albumin levels, hemoglobin concentration, and creatinine clearance than the low De Ritis ratio group. During the median follow-up period of 706 days (24 months), MACCE occurred in 13.7% (28/204) of patients, and all-cause mortality occurred in 8.8% (18/204). MACCE and all-cause mortality occurred in 33.3% and 10.7% of the patients in the high De Ritis ratio group, respectively, compared with 10.7% and 6.2% in the low De Ritis ratio group.
SINGLE FACTOR ANALYSIS:
Taking MACCE and all-cause mortality as dependent variables and the De Ritis ratio as the independent variable, the results of the univariate analysis showed that a high De Ritis ratio was related to MACCE (hazard ratio [HR]=3.60, 95% CI: 1.60–7.90, P=0.002) and all-cause mortality (HR=4.70, 95% CI: 1.80–12.00, P=0.001). The Kaplan-Meier analysis showed the same results (Figure 1).
MULTIVARIATE REGRESSION ANALYSIS:
In the multivariate Cox regression analysis, MACCE and all-cause mortality were used as dependent variables, De Ritis ratio as the independent variable, and age, BMI, serum albumin, and C-reactive protein as covariates. Similar to the single-factor analysis, the De Ritis ratio was related to MACCE (HR=2.96, 95% CI: 1.29–6.78, P=0.01) and all-cause mortality (HR=3.61, 95% CI: 1.31–9.86, P=0.012) (Figure 2).
SENSITIVITY ANALYSIS:
Cox proportional risk model A was fitted with age, BMI, serum albumin, and C-reactive protein, and model B was fitted by incorporating the De Ritis ratio into model A. The De Ritis ratio increased the predictive value of model B compared with that of model A for MACCE and all-cause mortality, with the improved concordance index during the follow-up period (Figure 3).
Discussion
This study evaluated the correlation between the De Ritis ratio and prognosis in patients with SCAD undergoing selective PCI. The results revealed that a high De Ritis ratio was independently and significantly associated with a high risk of MACCE and all-cause mortality, and that the De Ritis ratio was another valuable risk stratification factor.
Previous studies have demonstrated that a low BMI [10], low serum albumin [9], high C-reactive protein level [11], and multivessel lesion [12] are associated with a high risk of MACCE in patients with SCAD. Also, Alqahtani et al found an increased risk of acute myocardial infarction and in-hospital mortality in patients undergoing PCI for liver cirrhosis compared with in those with non-liver cirrhosis [13]. Thus, Steininger et al included 1355 patients with acute myocardial infarction and attempted to investigate the predictive potential of the De Ritis ratio on the prognosis of patients after acute myocardial infarction from a long-term perspective. Those results showed that the De Ritis ratio was a strong and independent predictor of their long-term mortality, with an adjusted HR of 1.23 (95% CI: 1.07–1.42,
Previous studies have shown that the degree of hepatic fibrosis is related to the development of atherosclerosis [15]. Chronic liver disease and coronary artery disease have similar pathogeneses, but the exact mechanism remains unclear. Some possible pathways include insulin resistance, lipid disorders, inflammation [16], and increased production of various thromboplastins by the liver, such as fetuin A, which promotes the formation of atherosclerotic plaques and accelerates vascular calcium deposition in patients with hepatic fibrosis [17]. Gjin et al showed that alanine aminotransferase was negatively correlated with 3-year cardiovascular mortality in patients with coronary artery disease diagnosed as having no abnormal liver function and that low alanine aminotransferase levels may reflect the risk of cardiovascular disease better than traditional risk factors [18]. Furthermore, identifying the cause of liver damage and active intervention can help to optimize secondary prevention strategies and improve patient prognosis.
This study has several limitations. First, this was a post hoc analysis of a retrospective cohort study, which inevitably had selection or regression bias. Second, the population analyzed in the study was solely from a Japanese hospital, and the research conclusion needs more analysis of populations from different regions and races. Third, patients with high levels of both aspartate aminotransferase and alanine aminotransferase can have evident liver damage, but the De Ritis ratio may not be high, which is the limitation of this ratio.
Conclusions
This study demonstrated that a high De Ritis ratio in patients with SCAD undergoing PCI was an independent and valuable risk stratification factor for MACCE and all-cause mortality. This conclusion needs to be confirmed in a multi-center study.
Figures
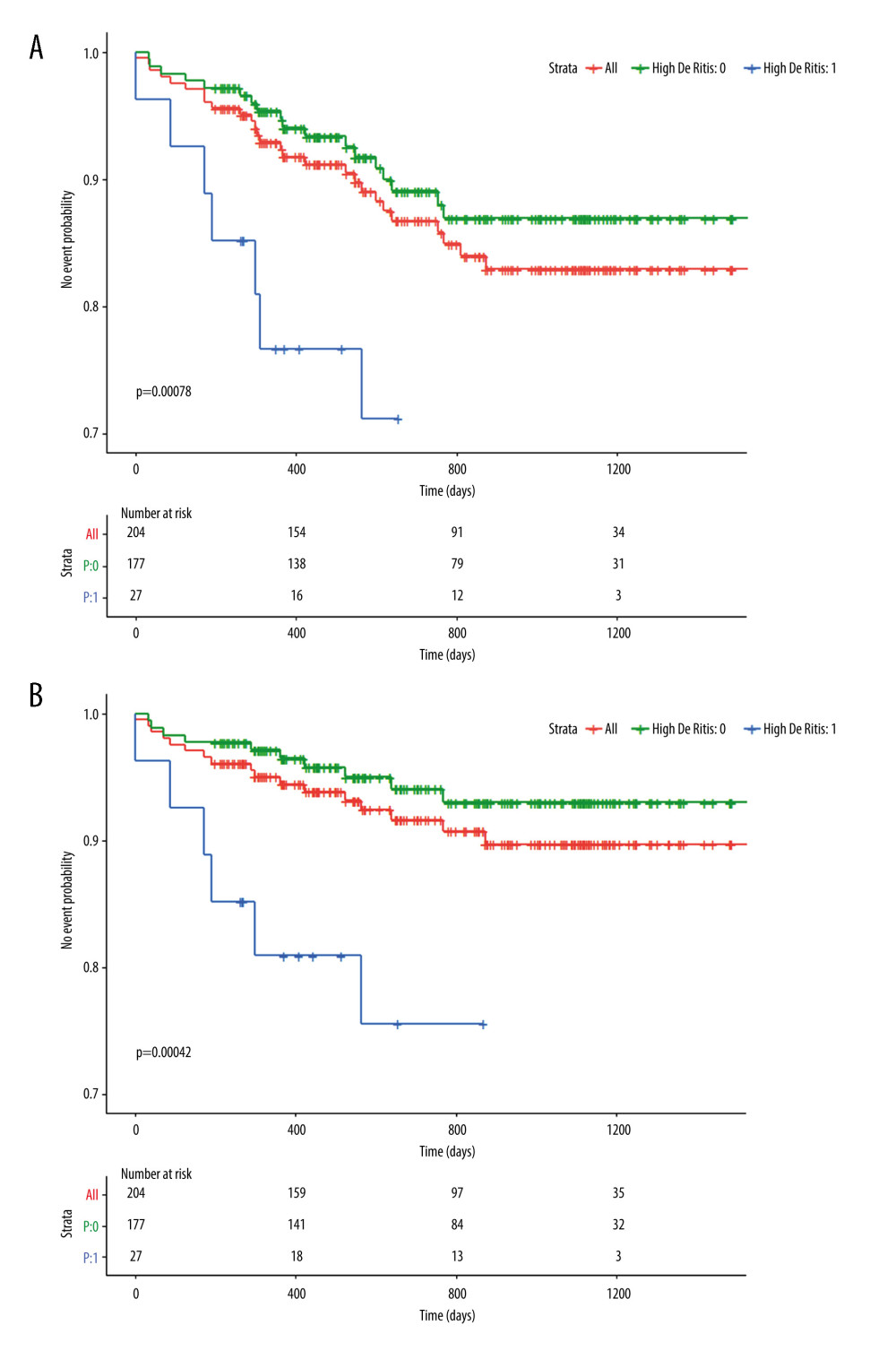 Figure 1. Kaplan-Meier survival curves of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality in patients with a high De Ritis ratio and a low De Ritis ratio in 2 years after percutaneous coronary intervention. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). 0 – low De Ritis ratio; 1 – high De Ritis ratio.
Figure 1. Kaplan-Meier survival curves of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality in patients with a high De Ritis ratio and a low De Ritis ratio in 2 years after percutaneous coronary intervention. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). 0 – low De Ritis ratio; 1 – high De Ritis ratio. ![Forest plot of Cox regression analysis of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality in 2 years after percutaneous coronary intervention. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). Age – age (years), divided into 4 levels: <60, 60–69, 70–79, and ≥80; BMI – body mass index (kg/m2), divided into 3 levels: <18.5, 18.5–24.9, and ≥25.0 [10]; Alb – serum albumin (g/dL), divided into 2 levels <4.0 and ≥4.0 [9]; CRP – C-reactive protein (mg/dL), divided into 4 levels: 0.01–0.03, 0.04–0.11, 0.12–0.33, and 0.34–9.20 [11].](https://jours.isi-science.com/imageXml.php?i=medscimonit-28-e937737-g002.jpg&idArt=937737&w=1000) Figure 2. Forest plot of Cox regression analysis of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality in 2 years after percutaneous coronary intervention. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). Age – age (years), divided into 4 levels: <60, 60–69, 70–79, and ≥80; BMI – body mass index (kg/m2), divided into 3 levels: <18.5, 18.5–24.9, and ≥25.0 [10]; Alb – serum albumin (g/dL), divided into 2 levels <4.0 and ≥4.0 [9]; CRP – C-reactive protein (mg/dL), divided into 4 levels: 0.01–0.03, 0.04–0.11, 0.12–0.33, and 0.34–9.20 [11].
Figure 2. Forest plot of Cox regression analysis of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality in 2 years after percutaneous coronary intervention. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). Age – age (years), divided into 4 levels: <60, 60–69, 70–79, and ≥80; BMI – body mass index (kg/m2), divided into 3 levels: <18.5, 18.5–24.9, and ≥25.0 [10]; Alb – serum albumin (g/dL), divided into 2 levels <4.0 and ≥4.0 [9]; CRP – C-reactive protein (mg/dL), divided into 4 levels: 0.01–0.03, 0.04–0.11, 0.12–0.33, and 0.34–9.20 [11]. 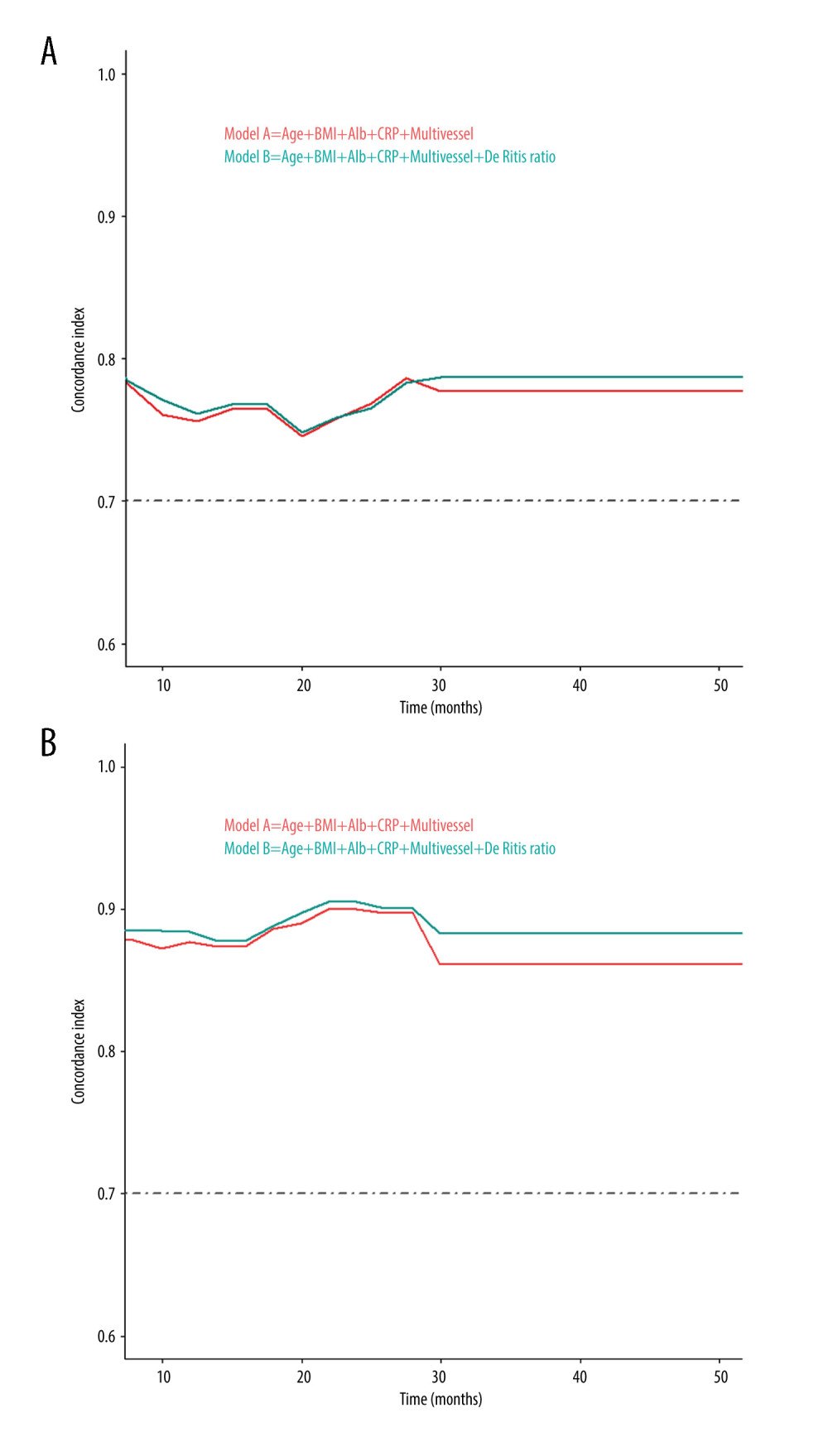 Figure 3. Concordance index of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality predicted by model A and model B during the follow-up period. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). Model A was fitted with age, BMI, albumin, C-reactive protein levels, and multivessel which have been proven to have prognostic value. Model B was a new model that introduced the De Ritis ratio to model A. BMI – body mass index; CRP – C-reactive protein; Alb – serum albumin; Multivessel – multivessel lesion.
Figure 3. Concordance index of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality predicted by model A and model B during the follow-up period. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). Model A was fitted with age, BMI, albumin, C-reactive protein levels, and multivessel which have been proven to have prognostic value. Model B was a new model that introduced the De Ritis ratio to model A. BMI – body mass index; CRP – C-reactive protein; Alb – serum albumin; Multivessel – multivessel lesion. 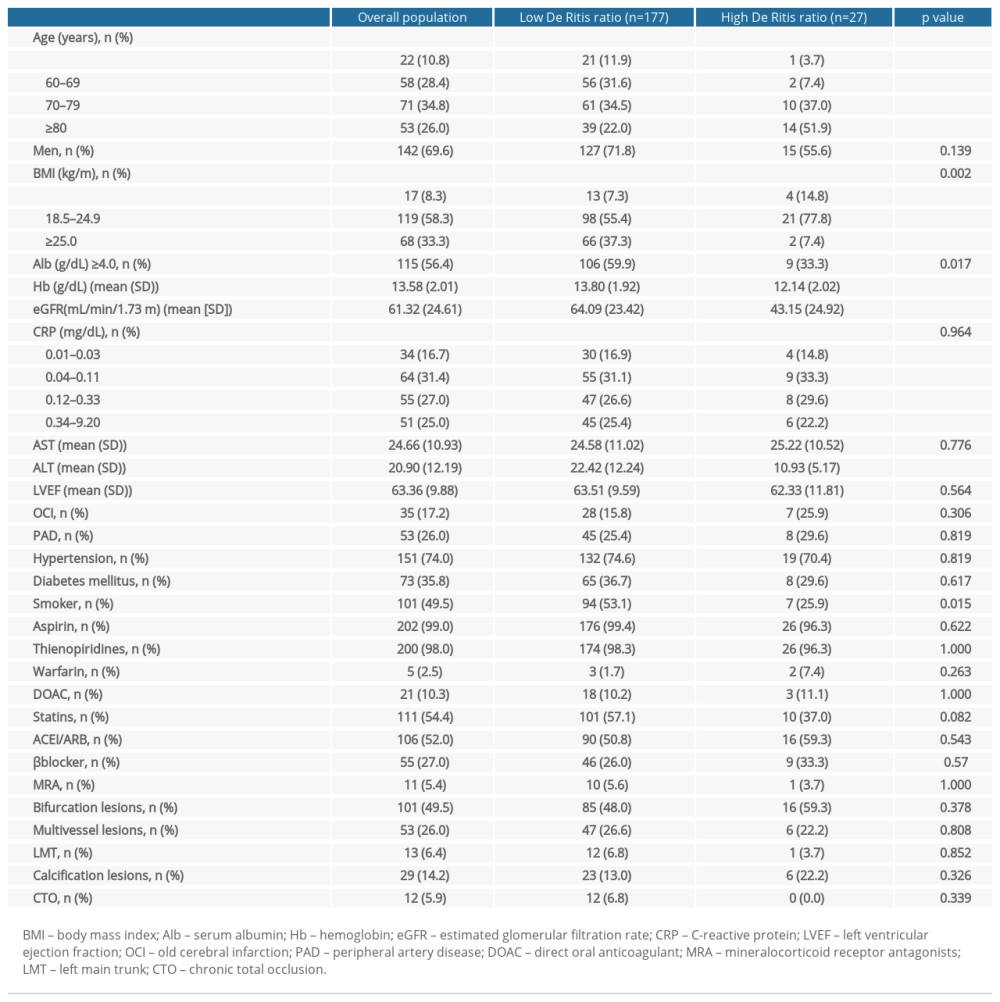
References
1. Wang Y, Wang W, Jia S, Development of a nomogram for the prediction of in-hospital mortality in patients with acute St-elevation myocardial infarction after primary percutaneous coronary intervention: A multicentre, retrospective, observational study in Hebei Province, China: BMJ Open, 2022; 12(2); e056101
2. Ndrepepa G, Holdenrieder S, Kastrati A, Prognostic value of De Ritis ratio in patients with acute myocardial infarction: Clin Chim Acta, 2022; 535; 75-81
3. Steininger M, Winter MP, Reiberger T, De-Ritis ratio improves long-term risk prediction after acute myocardial infarction: J Clin Med, 2018; 7(12); 474
4. Maeda D, Sakane K, Kanzaki Y, Relation of aspartate aminotransferase to alanine aminotransferase ratio to nutritional status and prognosis in patients with acute heart failure: Am J Cardiol, 2021; 139; 64-70
5. Lu Z, Ma G, Chen L, De-Ritis ratio is associated with mortality after cardiac arrest: Dis Markers, 2020; 2020; 8826318
6. Giannini E, Botta F, Fasoli A, Progressive liver functional impairment is associated with an increase in Ast/Alt ratio: Dig Dis Sci, 1999; 44(6); 1249-53
7. Wu VC, Chen SW, Chou AH, Nationwide cohort study of outcomes of acute myocardial infarction in patients with liver cirrhosis: A nationwide cohort study: Medicine (Baltimore), 2020; 99(12); e19575
8. Hillerson D, Ogunbayo GO, Salih M, Outcomes and characteristics of myocardial infarction in patients with cirrhosis: J Invasive Cardiol, 2019; 31(7); E162-69
9. Suzuki S, Hashizume N, Kanzaki Y, Prognostic significance of serum albumin in patients with stable coronary artery disease treated by percutaneous coronary intervention: PLoS One, 2019; 14(7); e0219044
10. Liu X, Liu P, Body mass index and major adverse cardiovascular events: A secondary analysis based on a retrospective cohort study: Med Sci Monit, 2020; 26; e919700
11. Luo F, Feng C, Zhuo C, C-reactive protein and all-cause mortality in patients with stable coronary artery disease: A secondary analysis based on a retrospective cohort study: Med Sci Monit, 2019; 25; 9820-28
12. Bauters C, Deneve M, Tricot O, Prognosis of patients with stable coronary artery disease (from the coronor study): Am J Cardiol, 2014; 113(7); 1142-45
13. Alqahtani F, Balla S, Alhajji M, Temporal trends in the utilization and outcomes of percutaneous coronary interventions in patients with liver cirrhosis: Catheter Cardiovasc Interv, 2020; 96(4); 802-10
14. Nam JS, Kim WJ, An SM, Age-dependent relationship between preoperative serum aminotransferase and mortality after cardiovascular surgery: Aging (Albany NY), 2019; 11(20); 9060-74
15. Turan Y, The nonalcoholic fatty liver disease fibrosis score is related to epicardial fat thickness and complexity of coronary artery disease: Angiology, 2020; 71(1); 77-82
16. Lonardo A, Nascimbeni F, Mantovani A, Hypertension, diabetes, atherosclerosis and nash: Cause or consequence?: J Hepatol, 2018; 68(2); 335-52
17. Sato M, Kamada Y, Takeda Y, Fetuin – a negatively correlates with liver and vascular fibrosis in nonalcoholic fatty liver disease subjects: Liver Int, 2015; 35(3); 925-35
18. Ndrepepa G, Holdenrieder S, Colleran R, Inverse association of alanine aminotransferase within normal range with prognosis in patients with coronary artery disease: Clin Chim Acta, 2019; 496; 55-61
Figures
Figure 1. Kaplan-Meier survival curves of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality in patients with a high De Ritis ratio and a low De Ritis ratio in 2 years after percutaneous coronary intervention. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). 0 – low De Ritis ratio; 1 – high De Ritis ratio.Figure 2. Forest plot of Cox regression analysis of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality in 2 years after percutaneous coronary intervention. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). Age – age (years), divided into 4 levels: <60, 60–69, 70–79, and ≥80; BMI – body mass index (kg/m2), divided into 3 levels: <18.5, 18.5–24.9, and ≥25.0 [10]; Alb – serum albumin (g/dL), divided into 2 levels <4.0 and ≥4.0 [9]; CRP – C-reactive protein (mg/dL), divided into 4 levels: 0.01–0.03, 0.04–0.11, 0.12–0.33, and 0.34–9.20 [11].Figure 3. Concordance index of (A) major adverse cardiac and cerebrovascular events and (B) all-cause mortality predicted by model A and model B during the follow-up period. Created with R software (version 4.1.3; The R foundation for Statistical Computing, Vienna, Austria). Model A was fitted with age, BMI, albumin, C-reactive protein levels, and multivessel which have been proven to have prognostic value. Model B was a new model that introduced the De Ritis ratio to model A. BMI – body mass index; CRP – C-reactive protein; Alb – serum albumin; Multivessel – multivessel lesion. In Press
Meta-Analysis
Effectiveness of Cardiac Telerehabilitation in Improving Functional Capacity, Quality Of Life and Cardiovas...Med Sci Monit In Press; DOI: 10.12659/MSM.953366
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,468
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,759,966
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,248
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,898
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387