03 October 2022: Clinical Research
Effect of Vitamin D Concentration on Course of COVID-19
Magdalena Dominika Szerszeń12ABDEF*, Aleksandra Kucharczyk3BDEF, Katarzyna Bojarska-Senderowicz3BDEF, Monika Pohorecka32ADEF, Andrzej Śliwczyński4CD, Janusz Engel5C, Tomasz Korcz6B, Dariusz Kosior7A, Irena Walecka8A, Wojciech Stefan Zgliczyński9A, Waldemar Wierzba1011G, Adam Jerzy Sybilski32ADFDOI: 10.12659/MSM.937741
Med Sci Monit 2022; 28:e937741






Abstract
BACKGROUND: The course of COVID-19 disease is associated with immune deregulation and excessive release of pro-inflammatory cytokines. Vitamin D has an immunomodulatory effect. We aimed to assess the possible correlation between the incidence and severity of SARS-CoV-2 infection and serum vitamin D concentration.
MATERIAL AND METHODS: A total of 505 successive patients admitted to a COVID-19-dedicated hospital were included in the retrospective analysis. Serum 25-hydroxyvitamin D (25-OHD) levels and SARS-CoV-2 RT-PCR throat swab test results were determined for each patient. The course of COVID-19 was assessed on the basis of the serum Vitamin Modified Early Warning Score (MEWS), which includes respiratory rate, systolic blood pressure, heart rate, temperature, and state of consciousness), as well as number of days spent in the intensive care unit (ICU) and need for oxygen therapy.
RESULTS: There was no difference in 25-OHD concentration between COVID-19-confirmed and negative results of the PCR tests. No correlation was found between serum 25-OHD in the COVID(+) group and the need for and time spend in the ICU, as well as the MEWS score. Multivariate analyses showed a positive correlation between need for oxygen therapy and lower 25-OHD concentration, as well as older age (P<0.001) and similar positive correlation between need for ventilation therapy with lower 25-OHD concentration, as well as older age (P=0.005).
CONCLUSIONS: Our findings do not support a potential link between vitamin D concentrations and the incidence of COVID-19, but low vitamin D serum level in COVID-19 patients might worsen the course of the disease and increase the need for oxygen supplementation or ventilation therapy.
Keywords: 1,25-dihydroxy-16,23-diene vitamin D3, COVID-19, SARS-CoV-2, Calcitriol, COVID-19, Cytokines, Humans, Oxygen, Vitamin D, Vitamin D Deficiency, Vitamins
Background
The active form of vitamin D is 1,25-dihydroxyvitamin D3 (1,25(OH)2D), which is also referred to as calcitriol. It is structurally related to steroid hormones and is actively hormone-like. It acts on target cells through the nuclear receptor VDR (vitamin D receptor). The breakthrough was the discovery that this receptor was not only present in bone cells, renal tubules, and intestinal epithelium, like previously was thought, but also in most cells in the human body; for example, in heart, blood vessel walls, brain, intestines, lymphocytes, macrophages cancerous, and many others [1]. It determines the presence of the VDR on many types of cells with pleiotropic effects of vitamin D. Particular importance is attached to the anti-inflammatory and immunomodulatory effects of vitamin D. 1,25(OH)2D stimulates the innate response, enhancing functions of macrophages, including chemotactic and phagocytotic properties, as well as the production of antibacterial peptides such as cathelicidines [2]. It also affects the specificity of the body’s immune response, such as differentiation and function of T lymphocytes. It inhibits the maturation and differentiation of dendritic cells and indirectly causes the polarization of Th1 and Th17 lymphocytes toward cells with the Th2 phenotype [2]. 1,25 (OH)2D directly affects the response of T lymphocytes by reducing the secretion of pro-inflammatory cytokines by Th1 and Th17 cells, as well as increasing the secretion of cytokines produced by Th2 [1–3]. At the same time, it promotes the development of regulatory T cell lines, both directly and indirectly, by dendritic cells (DC) operation. It also reduces the production of IgG and IgM by plasma cells. Cells of the immune system also express CYP27B1, the enzyme that converts 25 (OH) D to its active form, 1,25 (OH) 2D [1,2]. It is believed that a severe course of COVID-19 is associated with immune deregulation and excessive release of pro-inflammatory cytokines [3].
The best way to investigate whether the level of vitamin D is deficient, sufficient, or toxic is to measure 25-OHD levels in serum. Its half-life lasts 2–3 weeks and it reflects the concentration of vitamin D produced by the organism itself during sun exposure, as well as vitamin D that was taken as a supplement by the patient. Moreover, the level of 1,25(OH)2D can be influenced by hypocalcemia when increased secretion of parathyroid hormone can cause calcium mobilization from the skeleton and increase the renal production of 1,25(OH)2D while the patient is in fact vitamin D-insufficient or -deficient. The half-life of 1,25(OH)2D is only 4–6 [4] h, which is why in our study we decided to measure 25-OHD serum level.
Researchers in many countries have attempted to establish a correlation between the severity of the course of infection with the new coronavirus and the concentration of vitamin D in the serum and other factors [1,5–10].
The aim of our study was to determine whether vitamin D concentration influences the incidence and course of COVID-19 disease.
Material and Methods
This retrospective cohort study included 505 patients of the Central Clinical Hospital of the Ministry of the Interior and Administration (CSK MSWiA) in Warsaw discharged from the hospital between 21 April 2020 and 7 July 2020 (the observation period was 77 days). The study was conducted during the first wave of the COVID-19 pandemic in Poland, which was exceptionally mild for Poles. In each case, the end of the observation was the patient’s discharge from the hospital or death. Patient age was 1–97 years. The patients stayed in surgical wards, non-invasive treatment wards, the Intensive Care Unit (ICU), and the Hospital Emergency Ward. During the observation, serum 25-OHD level (later called vitamin D as an abbreviation; 25-OHD level best reflects real vitamin D level in serum [4]) was determined with the chemiluminescence method using the DiaSorin Liaison apparatus. A level <20 ng/ml was considered deficient, a level ≥20 and ≤30 ng/ml was considered a suboptimal level, and >30 ng/ml was considered an optimal level. The confirmation of the SARS-CoV-2 virus infection was the result of a RT-PCR throat swab test performed on an ELITe InGenius® instrument with a Gene FinderTM COVID-19 Plus RealAmp Kit produced by ELITechGroup. Patients were divided into 2 groups according to the presence or the lack of COVID-19 infection and according to comorbidities recorded in the patient’s medical history (or without comorbidities).
We analyzed the following associations: the prediction of COVID-19 incidence depending on the vitamin D level (comparative analysis of the COVID (+) and COVID (−) sub-cohorts), and the dependence of the course of the disease caused by SARS-CoV-2 on the vitamin D level (only in the group of COVID (+) patients) taking into account selected groups of comorbidities: respiratory tract diseases, cardiovascular disease, diabetes and others indicated by the patient. To assess the severity of COVID-19, the following criteria were used: use of oxygen therapy, use of ventilation therapy, patient’s death (or discharge from the hospital), stay in the ICU, and the MEWS score [11] calculated on the 1st, 2nd, 4th, 6th, and 8th days of hospitalization. The information was obtained using electronic medical records stored in the IT systems, kept by medical staff in individual departments.
The study protocol was approved by the Bioethics Commission of the CSK MSWiA in Warsaw (no. 57/2020). The collected data were compiled performing a statistical analysis using a chi-squared test, Mann-Whitney U Test, and MANOVA for independent groups. A
Results
The study included 256 males (M=50.69%) and 249 females (F=49.31%). There were 186 COVID (+) patients (M=93, F=93) and 219 COVID (−) patients (M=163, F=156). There were 5 patients <18 years old and they constituted 1% of the study population.
The median age was 65 years, the mean age was 61.23 years, and the standard deviation was 20.84. The comparison of vitamin D level in the COVID-19 infected group vs the uninfected group showed a 6.7% higher proportion of patients with vitamin D deficiency in the infected group (Table 1).
Patients suffering from selected groups of comorbidities were distinguished in the study population. Cardiovascular disease dominated in both studied groups – COVID (+) and COVID (−) – with a total share of about 40%. The proportion of patients with diabetes was about 20%, and a similar percentage of patients had respiratory tract diseases. In both groups, 16–17% of patients, had no comorbidities in their medical history. There were no significant differences in frequencies of comorbidities in the 2 study groups (Table 2).
The need for oxygen therapy increased with the decrease in vitamin D level in patients with COVID-19, especially in the case of comorbidities of respiratory tract diseases (
Multivariate analysis (MANOVA for independent groups) confirmed an association between lower vitamin D status and older age with the need for oxygen therapy in COVID (+) patients (Table 4).
The necessity for COVID (+) patients to stay in the ICU was significantly dependent on the presence of comorbidities (
The association between patient death and vitamin D level was at the borderline of statistical significance (
No association was found between vitamin D concentration in COVID (+) patients and need for ventilation therapy (
However, multivariate analyses (MANOVA for independent groups) showed a positive correlation between the need to use ventilation therapy with lower 25-OHD concentration and older age (
Discussion
Our results show that low vitamin D level was associated with an increased frequency of using oxygen therapy and ventilation therapy in patients infected with SARS-CoV-2, and thus with a more severe course of disease.
Vitamin D reduces the risk of viral infections (eg, seasonal influenza) [1,2], and its deficiency is a risk factor for complicated course of some bacterial infections [12]. It is reasonable to check whether it has an impact on the incidence and course of COVID-19. In a systematic review of studies on the correlation between vitamin D level and respiratory tract infections in general and those caused by SARS-CoV-2, it was shown that serum 25-OHD deficiency increases the risk of severe acute respiratory infection (ARI), regardless of the etiological factor, and acute respiratory distress syndrome (ARDS), and worsens its course in children and adults [13]. It was found that higher 25-OHD level in the range of optimal level reduced the risk of respiratory tract infections in each age group [14]. In the study by Faul et al, a statistically significant association was found between low vitamin D level and the severity of COVID-19 and the development of ARDS [15]. There have also been several other key systematic review and meta-analysis studies that have the same conclusions, which are that reduced vitamin D levels are associated with an increased risk of infection from SARS-CoV-2 and increased duration and severity of COVID-19 [8–10].
We found no differences between the vitamin D level among those infected with SARS-CoV-2 and those uninfected, which indicates that the vitamin D level had no effect on the incidence of COVID-19 among the studied patients (
It should be considered that the vitamin D level decreases significantly with age, and the older the age, the worse the course of infection [19]. As a result, the likelihood of a more severe course of COVID-19 may be due to the patient’s age itself, not just vitamin D level. In the study from the United Kingdom, it was found that low vitamin D level affects the severity of COVID-19, but does not translate into an increase in mortality [20]. Multivariate analysis in our study proved dependence between lower vitamin D status and older age with the need for oxygen therapy as well as ventilation therapy in COVID (+) patients. We showed an association at the border of statistical significance between low vitamin D level and death. This association is the most noticeable in patients who also have diabetes. However, in the whole study, the absolute number of patients whose disease was fatal was small (40 out of 186 COVID (+) persons). It can be assumed that if the group of people under study was larger, the association would be significant. This may be supported by the fact that 76.9% of patients who died were deficient in vitamin D. In another study, low calcium and vitamin D levels were associated with an increased risk of organ damage, sepsis, and death in patients with COVID-19 [21].
Based on the data of Italian researchers [22], it can be stated that there is no correlation between the level of sunlight in a given country and the observed percentage of COVID-19 patients.
However, based on data from Italy, no such association was found [22]. It follows that vitamin D alone cannot be the only determinant in assessing the risk of the incidence of COVID-19 and mortality due to COVID-19.
The limitation of the study is that we did not assess patients in terms of meeting the criteria of ARI and ARDS; therefore, the results obtained cannot be compared with other studies in this respect.
There is also a certain limitation associated with the retrospective character of our study, which made it difficult in certain cases to obtain specific information needed to make comparisons (eg, lack of assessing MEWS in certain patients).
Conclusions
The findings from this retrospective study from a single center in Poland supported the findings from other studies that low serum levels of vitamin D prolonged the course of COVID-19 disease and increased the need for oxygen therapy and respiratory support.
Another interesting conclusion is the patients with COVID-19 required hospitalization in the ICU more often if they had a comorbidity (without assessing the effect of vitamin D level). In our study, we showed that there is no effect of low vitamin D level in the serum on the incidence of COVID-19. Vitamin D level did not affect the transfer of the patient to the ICU, the length of the stay in the ICU (excluding patients who died), or the patient’s condition according to MEWS on the 1st, 2nd, 4th, 6th, and 8th days of hospitalization. From the point of view of public health, it is very important to supplement and maintain vitamin D levels at the right level. This allows for milder symptoms of infection, no need for advanced medical procedures like mechanical ventilation, or hospitalization in the ICU, which translates into lower costs for the healthcare system. Supplementation is cheap, generally available, and easy to administer. Considering the other activities of vitamin D, its role in maintaining public health is large and continues to grow.
Tables
Table 1. Vitamin D level in the study population.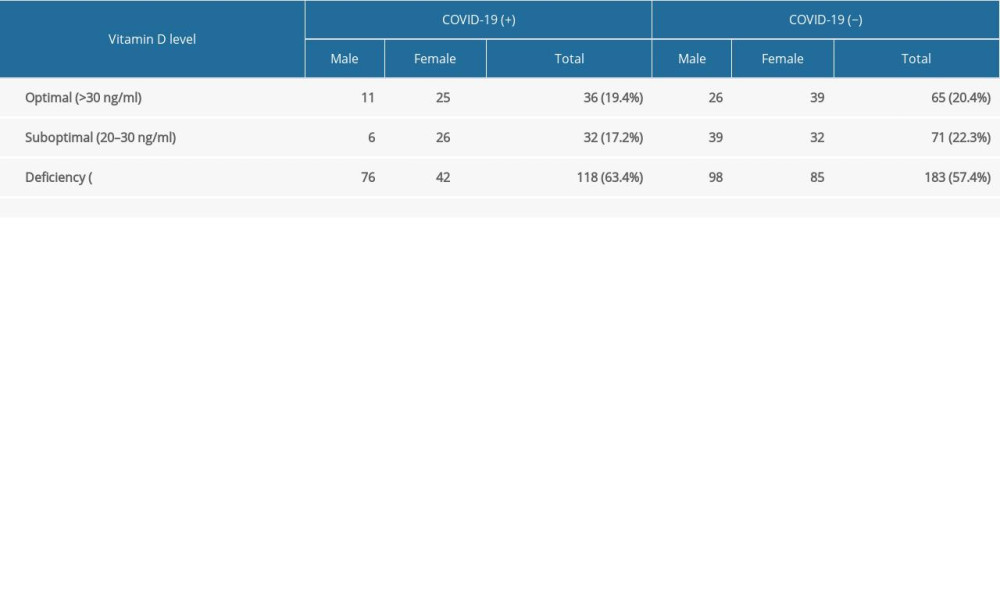 Table 2. Occurrence of comorbidities in study population.
Table 2. Occurrence of comorbidities in study population.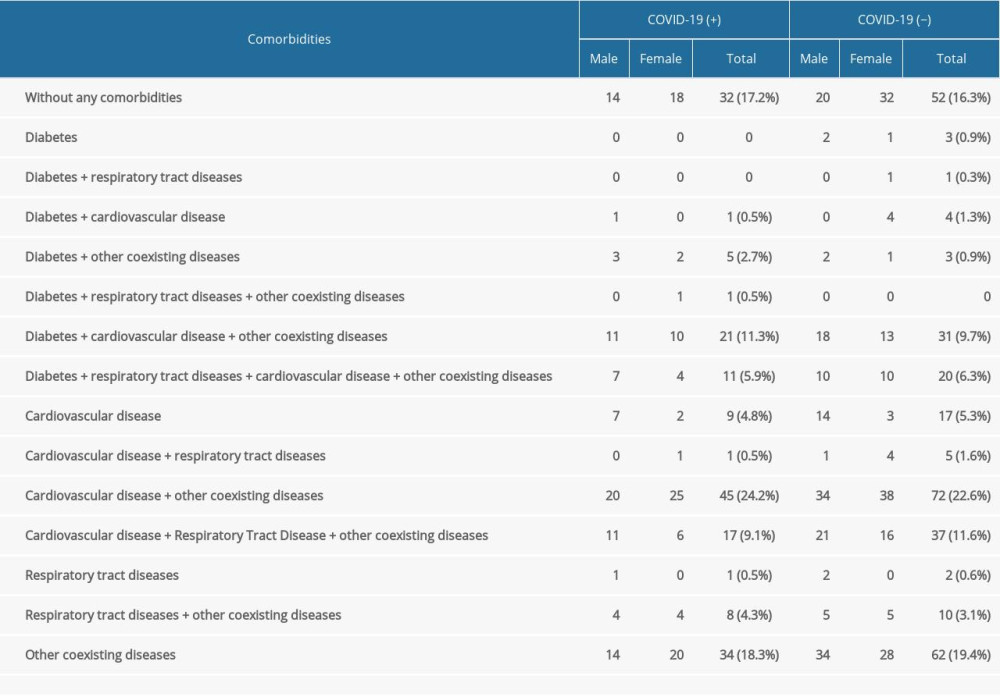 Table 3. Correlation between vitamin D level in serum and oxygen therapy (Mann-Whitney U test).
Table 3. Correlation between vitamin D level in serum and oxygen therapy (Mann-Whitney U test).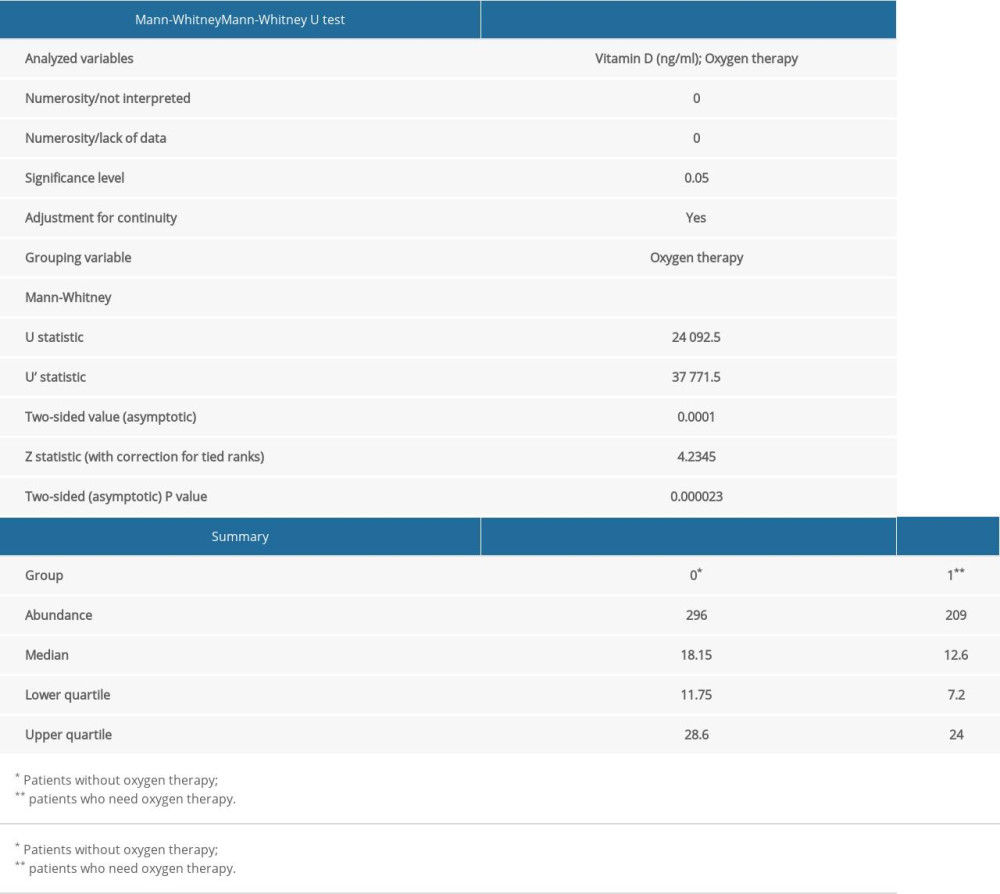 Table 4. Correlation between age, vitamin D serum level, and oxygen therapy (MANOVA test).
Table 4. Correlation between age, vitamin D serum level, and oxygen therapy (MANOVA test).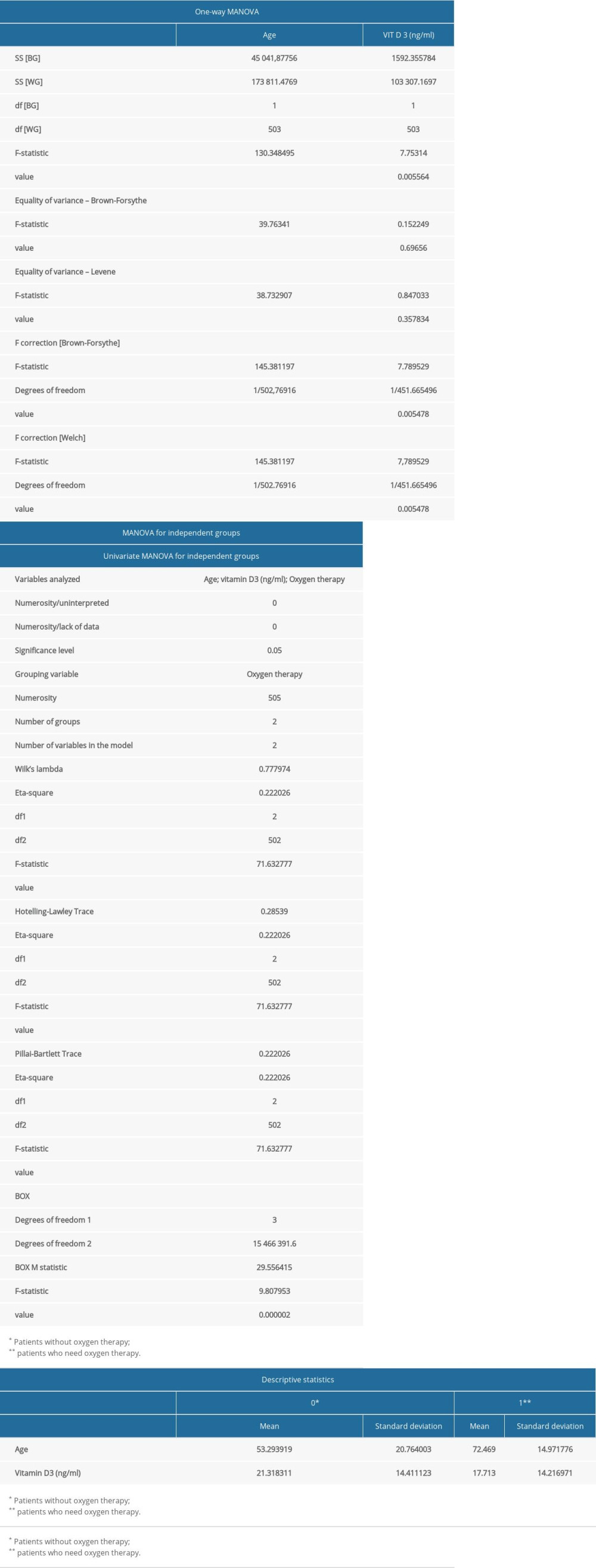 Table 5. Correlation between ICU hospitalization and comorbidities (Mann-Whitney U test).
Table 5. Correlation between ICU hospitalization and comorbidities (Mann-Whitney U test).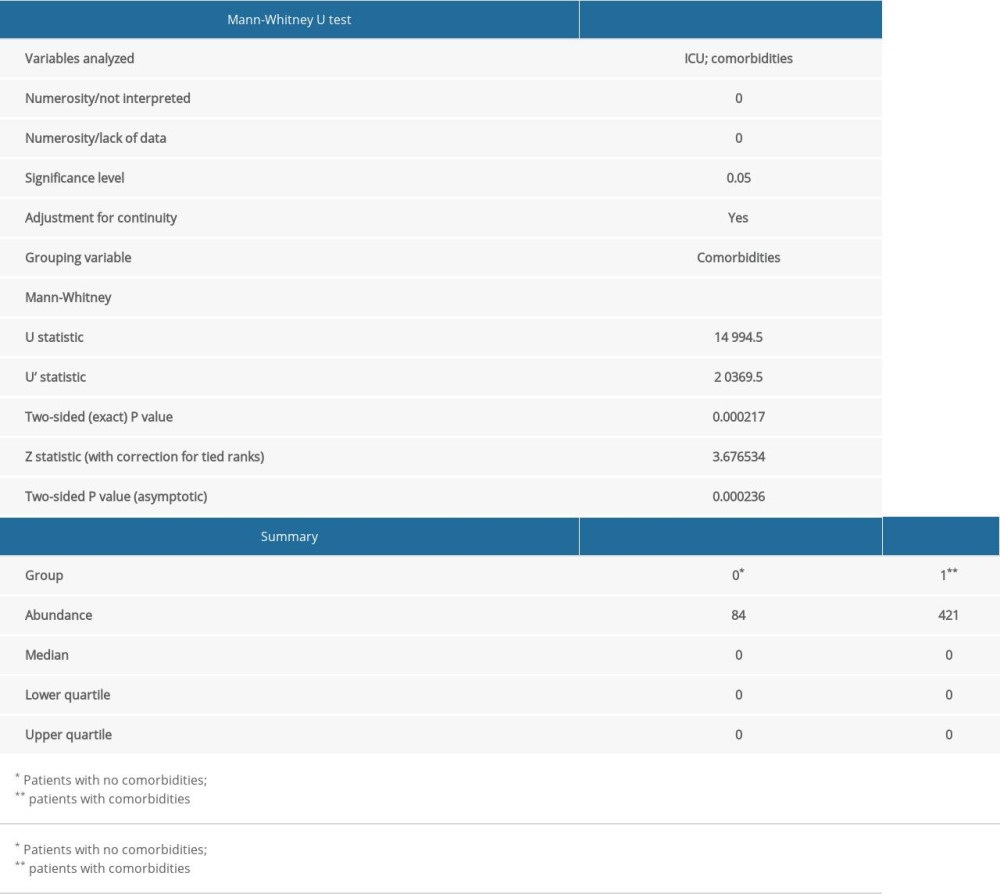
References
1. Teymoori-Rad M, Shokri F, Salimi V, The interplay between vitamin D and viral infections: Rev Med Virol, 2019; 29; 2032
2. Grant WB, Lahore H, McDonnell SL, Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths: Nutrients, 2020; 12; 88
3. Guo YR, Cao QD, Hong ZS, The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status: Mil Med Res, 2020; 7; 11
4. Holick MF, Vitamin D status: Measurement, interpretation, and clinical application: Ann Epidemiol, 2009; 19(2); 73-78
5. Entrenas Castillo M, Entrenas Costa LM, Vaquero Barrios JM, Effect of calcifediol treatment and best available therapy versus best available therapy on Intensive Care Unit admission and mortality among patients hospitalized for COVID-19: J Steroid Biochem Mol Biol, 2020; 203; 105751
6. Rhodes JM, Subramanian S, Laird E, Editorial: Low population mortality from COVID-19 in countries south of latitude 35 degrees North supports vitamin D as a factor determining severity: Aliment Pharmacol Ther, 2020; 51; 1434-37
7. Bianconi V, Bronzo P, Banach M, Particulate matter pollution and the COVID-19 outbreak: Results from Italian regions and provinces: Arch Med Sci, 2020; 16(5); 985-92
8. D’Ecclesiis O, Gavioli C, Martinoli C, Vitamin D and SARS-CoV2 infection, severity and mortality: A systematic review and meta-analysis: PLoS One, 2022; 17(7); e0268396
9. Liu N, Sun J, Wang X, Low vitamin D status is associated with coronavirus disease 2019 outcomes: A systematic review and meta-analysis: Int J Infect Dis, 2021; 104; 58-64
10. Kaya MO, Pamukçu E, Yakar B, The role of vitamin D deficiency on the COVID-19: A systematic review and meta-analysis of observational studies: Epidemiol Health, 2021; 43; e2021074
11. Flisiak R, Horban A, Jaroszewicz J, Recommendations of management in SARS-CoV-2 infection of the Polish Association of Epidemiologists and Infectiologists: Pol Arch Intern Med, 2020; 130; 352-57
12. Shalaby SA, Handoka NM, Amin RE, Vitamin D deficiency is associated with urinary tract infection in children: Arch Med Sci, 2018; 14(1); 115-21
13. Dancer RC, Parekh D, Lax S, Vitamin D deficiency contributes directly to the acute respiratory distress syndrome (ARDS): Thorax, 2015; 70; 617-24
14. Pham H, Rahman A, Majidi A, Acute respiratory tract infection and 25-hydroxyvitamin D concentration: A systematic review and meta-analysis: Int J Environ Res Public Health, 2019; 16; 3020
15. Faul JL, Kerley CP, Love B, Vitamin D deficiency and ARDS after SARS-CoV-2 infection: Ir Med J, 2020; 113; 84
16. Meltzer DO, Best TJ, Zhang H, Association of vitamin D status and other clinical characteristics with COVID-19 tyest results: JAMA Netw Open, 2020; 3; 2019722
17. Merzon E, Tworowski D, Gorohovski A, Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: An Israeli population-based study: FEBS J, 2020; 287; 3693-702
18. Hastie CE, Mackay DF, Ho F, Vitamin D concentrations and COVID-19 infection in UK Biobank: Diabetes Metab Syndr, 2020; 14; 561-65
19. Boucher BJ, The problems of vitamin d insufficiency in older people: Aging Dis, 2012; 3; 313-29
20. Panagiotou G, Tee SA, Ihsan Y, Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalized with COVID-19 are associated with greater disease severity: Clin Endocrinol, 2020; 93; 508-11
21. Sun JK, Zhang WH, Zou L, Serum calcium as a biomarker of clinical severity and prognosis in patients with coronavirus disease 2019: Aging (Albany NY), 2020; 12; 11287-95
22. Ferrari D, Locatelli M, Briguglio M, Is there a link between vitamin D status, SARS-CoV-2 infection risk and COVID-19 severity?: Cell Biochem Funct, 2021; 39; 35-47
Tables
Table 1. Vitamin D level in the study population.Table 2. Occurrence of comorbidities in study population.Table 3. Correlation between vitamin D level in serum and oxygen therapy (Mann-Whitney U test).Table 4. Correlation between age, vitamin D serum level, and oxygen therapy (MANOVA test).Table 5. Correlation between ICU hospitalization and comorbidities (Mann-Whitney U test). In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387