24 March 2023: Clinical Research
Risk Factors for Mortality in Severe Fever with Thrombocytopenia Syndrome Patients with Central Nervous System Complications
Xiao Fei1ABCDEFG*, Baobao FengDOI: 10.12659/MSM.938427
Med Sci Monit 2023; 29:e938427






Abstract
BACKGROUND: Severe fever with thrombocytopenia syndrome (SFTS) is a zoonotic viral hemorrhagic fever caused by the SFTS virus (SFTSV), which is a newly identified tick-borne bunyavirus, recently named Dabie bandavirus. In rural China, SFTSV or Dabie bandavirus is commonly transmitted by Haemaphysalis longicornis, the Asian longhorned tick. In recent years, SFTS has been of great concern due to its high morbidity and mortality. The present study investigated the risk factors for mortality in patients with SFTS complicated by central nervous system involvement.
MATERIAL AND METHODS: We studied 69 SFTS patients hospitalized between 2013 and 2020. We analyzed the laboratory test results and clinical data through univariate and multivariate regression.
RESULTS: Neurological complications occurred in 59 patients in the survival group and 10 in the mortality group. No significant gender difference was found between the 2 groups. No significant difference was found in age, hospitalization duration, or occurrence of encephalitis between the 2 groups. The mean duration of hospitalization and course of the disease in the mortality group were significantly shorter than those in the survival group (P<0.01). The mean values of platelet count, potassium, and sodium in the mortality group were significantly lower, while the mean values of aspartate aminotransferase, lactic dehydrogenase, creatine kinase-MB (CK-MB) and procalcitonin were higher than those in the survival group. Low platelet count and high CK-MB were independent risk factors for mortality in patients. For each unit increase in platelet count, the risk of mortality decreased by 24.2%, and for each unit increase in CK-MB, the probability of mortality increased by 118.6%.
CONCLUSIONS: Decreased platelets and increased CK-MB were independent risk factors for mortality in encephalitis patients. SFTS patients with encephalitis should be monitored for changes in these 2 indicators.
Keywords: Diagnostic Techniques, Neurological, SFTS Phlebovirus, Humans, Severe Fever with Thrombocytopenia Syndrome, Bunyaviridae Infections, Encephalitis, Risk Factors, China, Creatine Kinase, MB Form, Central Nervous System
Background
Severe fever with thrombocytopenia syndrome (SFTS) is a natural infectious disease caused by a virus transmitted by tick bites. The viral pathogen that causes SFTS was first isolated and characterized as a new bunyavirus, designated
The onset and severity of SFTS are acute and severe, and the main clinical manifestations are fever, chills, anorexia, nausea, vomiting, abdominal pain, diarrhea, lymphadenopathy, leukopenia, and thrombocytopenia. Some cases may be complicated by multiorgan dysfunction, including heart, liver, kidney, and brain dysfunction, as well as coagulation, and several organ disorders may occur in severe cases [15–17]. There is still a lack of effective antiviral drugs and preventive vaccines for this virus. Choi et al and Gai et al summarized the pathogenesis of SFTS as fever, multiple organ disorder, and recovery stages [8,18], believing that severely affected patients would develop multiple organ failure that would eventually lead to mortality. Neurological complications are among the serious complications of SFTS, most of which occur within 5–7 days. The incidence of neurological involvement in SFTS is 3–77% [4,15,18,19], mainly manifested as disturbance of consciousness, indifference, muscle fibrillation, epilepsy, and coma, and presence of these conditions is closely related to mortality [15,18]. A study on the cerebrospinal fluid of patients with SFTS complicated by neurological damage confirmed that the protein and glucose levels in cerebrospinal fluid were normal, and an increase in leukocytes in the cerebrospinal fluid was not common. Only a few patients tested positive for SFTSV, and the levels of MCP-1 and IL-8 in cerebrospinal fluid were higher than in serum. This suggests that these cytokines are very important in the pathogenesis from virus invasion of the nervous system [19]. About 90% of the non-survivors showed indifference, lethargy, muscle tremor, convulsion, coma, and other central nervous system symptoms before mortality. In comparison, 37% of the survivors showed these symptoms, mainly manifested as indifference and lethargy [18]. Neurological symptoms seriously affect the disease progression and prognosis in SFTS patients, a fact that clinicians should pay great attention to. We studied the clinical manifestations, laboratory test results, imaging examination results, and treatment of SFTS patients with neurological impairment to determine the risk factors for mortality, and to predict the disease progression and prognosis of patients with SFTS combined with neurological impairment, for clinicians.
Material and Methods
SAMPLE SIZE:
From 2013 to 2020, 69 SFTS patients with central nervous system complications treated by Shandong Weifang Yidu Central Hospital were included in our study. If a suspected case met both of the following criteria, it was diagnosed as SFTS: 1. The patient had a history of tick bite 2 weeks before the onset of the disease, or worked, lived or travelled in hills, forests, or mountains during the epidemic season (April to June). 2. The patient had fever (most of the patients had temperatures above 38 degrees Celsius), peripheral blood thrombocytopenia (normal range: 100–400×109/L), and decreased white blood cell count (WBC, normal range: 4–10×109/L). Finally, the patient’s blood samples must be positive for SFTSV as detected by an SFTSV nucleic acid quantitative detection kit and polymerase chain reaction fluorescence probe. In the present study, these positive results served to determine that a suspected case would be classified as a confirmed case of SFTS. The detections were carried out in Weifang Center for Disease Control and Prevention. The patients were split into survival and mortality groups according to the clinical course.
Neurological symptoms caused by SFTSV were not defined in the 2010 version of the guidelines for SFTS. We defined and classified these symptoms based on published literature reports and the symptoms observed in clinical diagnosis and treatment [15,18–21]. As a result, SFTSV-associated neurological complications refer specifically to the occurrence of 1 or more symptoms as follows: (1) muscle tremor and limb tremor: in particular, involuntary muscle tremor of the tongue, jaw, or limbs; (2) cognitive dysfunction: decreased orientation, decreased memory and calculation ability, slow reaction time, inability to accurately answer questions, inability to complete simple instructions, inability to do fine movements and aphasia, speech communication disorders, including difficulty in speech and word finding, and/or naming disorders; (3) consciousness disorder: drowsiness, coma, delirium; (4) convulsions or seizures. The patients with these neurological complications in confirmed cases were split into survival and mortality groups. According to the condition of the patients at discharge, if all the indicators were improved or entered the recovery period, the patients were classified into the survival group. The patients who did not survive until discharge were classified into the mortality group. Mortality was determined by the following criteria: cardiac and respiratory arrest, electrocardiogram showing no cardiac electrical activity, dilated pupils, and absence of light reflex.
TREATMENT DATA:
Demographic factors, date of onset/admission/mortality, disease outcome, clinical manifestations, physical check, and laboratory parameters were collected retrospectively. These data were imported into EpiData (the designated database), and exported as an Excel file.
STATISTICAL VALIDATION:
Data were analyzed by SPSS 26.0 (IBM, New York, NY, USA). Categorical data were compared using the Chi-square test or Fisher’s exact test, and the results were expressed as n (%). Quantitative data were compared with the
Results
COMPARISON OF BASIC DATA BETWEEN THE MORTALITY GROUP AND THE SURVIVAL GROUP:
Neurological complications occurred in 59 patients in the survival group and 10 patients in the mortality group (Table 1). There was no obvious gender difference between the 2 groups; the male: female patients’ ratio in the survival and mortality group was 25: 34 and 5: 5, respectively. The mean age of the survival group was 64.02±10.8, and that in the mortality group was 71.7±14.91. There was no obvious age difference between the 2 groups. The mean duration of occurrence of encephalitis was 7.47±1.91 in the survival group and 7.2±3.16 in the mortality group; there was no significant difference in encephalitis occurrence between the 2 groups. The mean duration of hospitalization was 12.36±4.04 days in the survival group and 4.25±2.11 days in the mortality group, while the mean course of the disease was 17.98±4.50 days in the survival group and 10.00±2.68 days in the mortality group. These differences between the groups were statistically significant (P<0.01).
COMPARISON OF LABORATORY TEST RESULTS:
The patients in the mortality group had a disease duration of up to 15 days. Therefore, we compared the laboratory measures during the first 2 weeks of disease duration. There was no significant difference in WBC, neutrophils (N), lymphocyte percentage (LY%), lymphocytes (LY), red blood cells (RBC), hemoglobin (HGB), creatinine kinase (CK), C-reactive protein (CRP), chloride (Cl), prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), alanine aminotransferase (ALT), total bilirubin (TBIL), direct bilirubin (DBIL), globulin (GLO), gamma glutamyl transferase (GGT), alkaline phosphatase (ALP), and brain natriuretic peptide (BNP) between the 2 groups. In contrast, the differences in platelet count (PLT), AST, LDH, CK-MB, procalcitonin (PCT), potassium (K) and sodium (Na) were statistically significant (P<0.05). The mean values of PLT, K, and Na in the mortality group were significantly lower than those in the survival group, while the mean values of AST, LDH, CK-MB, and PCT were significantly higher than those in survival group (Table 2).
COMPARISON OF CLINICAL SYMPTOMS AND SIGNS:
There were no significant differences between the 2 groups in headache, chills, muscle pain, arthralgia, nausea and vomiting, loss of appetite, abdominal pain, diarrhea, cough, expectoration, melena, hemorrhagic spots, lymphadenopathy, pulmonary rales, hemoptysis, gastrointestinal bleeding, sinus tachycardia, sinus bradycardia, premature beat, conduction block, atrial fibrillation, and t-wave abnormality (Table 3).
MULTIVARIATE LOGISTIC REGRESSION ANALYSIS:
Variables with statistically significant differences in univariate analysis were included in multivariate analysis. With mortality (mortality =1, survival =0) as the dependent variable and age, PLT, AST, LDH, CK-MB, PCT, K, and Na as the independent variables, a binary logistic regression model was established and the step-by-step regression method was adopted. The results are listed in Table 4.
Table 4 indicates that the regression coefficient of the variable PLT was P=0.038 (P<0.05), OR=0.758 (OR<1), indicating that low PLT is an independent risk factor for patient mortality. The probability of mortality decreased by 24.2% for each unit increase in the variable PLT.
The CK-MB regression coefficient was
Therefore, low PLT and high CK-MB were found to be independent influencing factors associated with patient mortality, while age, AST, LDH, PCT, K, and Na were not found to be independent influencing factors of patient mortality (Table 4).
Discussion
The pathogen that causes SFTS is
The nervous system symptoms seen in SFTS differ from those seen in other types of viral encephalitis. They include meningitis, muscle tremors, and limb jitter. In serious cases, gradual disturbances of consciousness are seen, such as delirium, sleepiness, and even convulsions and coma. Some of the patients in the mortality group showed early onset of severe disturbance of consciousness before multiple organ failure. At present, many studies have found that neurological symptoms are closely associated with mortality [1,12,17,18,24], indicating that neurological symptoms of SFTS are of great significance in clinical diagnosis and differential diagnosis. The main peripheral nervous system symptoms include muscle tremors and limb jitter, with the muscles of the patient’s lips and hands involuntarily quivering. The main central nervous system symptoms include irritability, delirium, sleepiness, nonsense speech, disorientation, memory loss, abnormal fidgetiness, and insomnia. Speech disorders can also occur, manifested as tongue-tied speech, inarticulate speech, or motor aphasia. Patients may experience heavy lethargy, convulsions, limb spasm symptoms, epilepsy, loss of consciousness, squinting or double vision, occasionally foaming at the mouth, urinary incontinence, a significant rise in heart rate, and blood oxygen saturation decline. A tic, which can be relieved by the application of sedative drugs, can manifest in 2 days; this was seen in 1 case of patient mortality. Another 3 patients in the mortality group had convulsions on the fourth day after onset, with frequent convulsions. Sedative drug treatment was not effective, and these patients fell into coma after frequent convulsions. All 3 of these patients died on the admission day or the next day. Among the surviving patients, there were 3 patients with convulsions. The neurological symptoms of these 3 patients appeared on the seventh, seventh, and eighth day, respectively. The initial neurological symptoms all appeared as muscle fibrillation. Convulsions occurred less frequently, and when they did occur, it was on the second or third day of hospitalization, and they could be relieved by sedative drug treatment after the seizures. Compared with the surviving patients, the convulsions of the non-surviving patients were more frequent in the early onset of the disease, and were difficult to control with drugs. The patients fell into coma after frequent convulsions, while the convulsions of the surviving patients occurred later and less frequently. After the control of convulsions, consciousness could be cleared, or the patient could be aroused from drowsiness. The duration of hospitalization and the course of disease in the mortality group were significantly shorter than those in the survival group, and most patients died within 2 weeks. It was because these severe neurological symptoms occurred in the early stage of the disease that the survival time of the patients was significantly shortened. Fatal neurological complications can significantly affect patient survival.
Regarding other clinical manifestations in patients with neurological complications, in addition to influenza-like symptoms such as fever, chills and muscle soreness, lymph node enlargement, digestive system symptoms and respiratory system symptoms were more frequent, but there was no statistically significant difference between patients who survived and those who did not survive. According to the autopsy reports of the 2 patients who died of SFTS, there was gastrointestinal, abdominal, and pulmonary bleeding, liver necrosis, and pathological changes in the lymph nodes closest to the tick bite area [25–27]. Pulmonary edema, as well as hemorrhage, infarction, and diffuse alveolar injury, also occurred in the lungs of patients who died, suggesting acute lung injury [25]. Pathological results suggested that the location of organ damage was consistent with the clinical symptoms observed. However, there was no mention of brain biopsies in the autopsy reports.
In addition, SFTS can also cause damage to the bone marrow hematopoietic system, and leukocytes and platelets in patients can be significantly reduced. In our study, leukocytes were as low as 0.52×109/L and platelets were as low as 9×109/L. Platelet counts in the mortality group were obviously lower than those in the survival group, and the decrease in platelets is an independent risk factor related to mortality. We found that the decrease in WBC was mainly in lymphocytes and monocytes, unlike the increase caused by most viral infections. Some studies found that bone marrow specimens from patients showed HLH secondary to virus infection [28,29]. Phagocytosis of platelets and lymphocytes by macrophages leads to thrombocytopenia and lymphocytopenia [30], and the degree of HLH may be associated with the disease severity.
In terms of biochemical indexes, AST, LDH, CK, CK-MB, and ALP increased significantly in the 2 groups; the values were 5–10 times higher than the normal range, and AST, LDH, and CK-MB levels in the mortality group were obviously greater than those in the survival group. The increase in these enzymes often suggests serious myocardial injury. It is also a risk factor associated with mortality [8,12,31], and is the main enzyme that causes elevated SFTS. Our study also found that high CK-MB during the first 2 weeks of the disease course is an independent risk factor associated with mortality, suggesting that the heart is another important organ damaged by SFTSV. In SFTS patients, at the same time, we found that the possibility of electrolyte disorder is higher, especially hypokalemia or hyponatremia in patients with digestive tract symptoms severe enough to lead to lack of potassium and sodium intake. This might be a reason for a result confirmed in studies: that hyponatremia can have a significant influence on mortality [15], and hyponatremia can cause hypotonic encephalopathy, which will aggravate the disturbance of consciousness. Severe hypokalemia can cause arrhythmias, which may be the cause of mortality.
The main limitation of this study was that the sample size of the mortality group was not large enough. Moreover, this study was a single-center study, which can only reflect the characteristics of the disease in a single area, so further multi-center studies are needed. In addition, cerebrospinal fluid and MRI results were not available because of the poor cooperation of patients with neurological symptoms, so the diagnosis of neurological complications depended on clinical diagnosis.
Conclusions
In conclusion, we believe that the clinical manifestations of patients with SFTS complicated by central nervous system complications do not differ in surviving and non-surviving patients, but reduced PLT and increased CK-MB during the first 2 weeks of the disease course were independent risk factors related to mortality. The above indicators should be monitored in clinical diagnosis and treatment, which can help clinicians predict a high risk of mortality in advance, to facilitate reasonable and effective treatment.
Tables
Table 1. Comparison of basic data between surviving and non-surviving cases.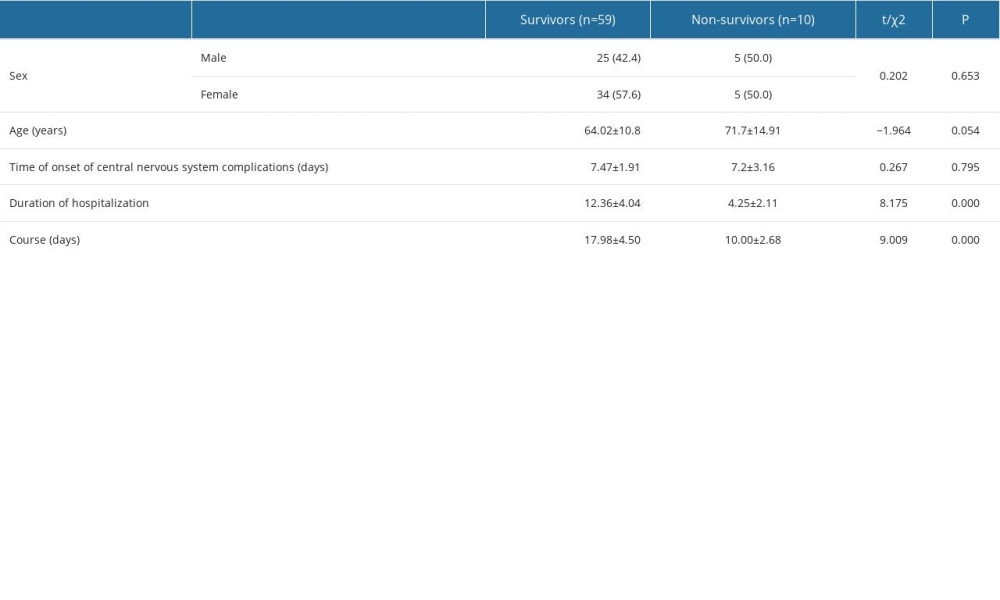 Table 2. Comparative results of laboratory tests between the survivor and non-survivor groups.
Table 2. Comparative results of laboratory tests between the survivor and non-survivor groups.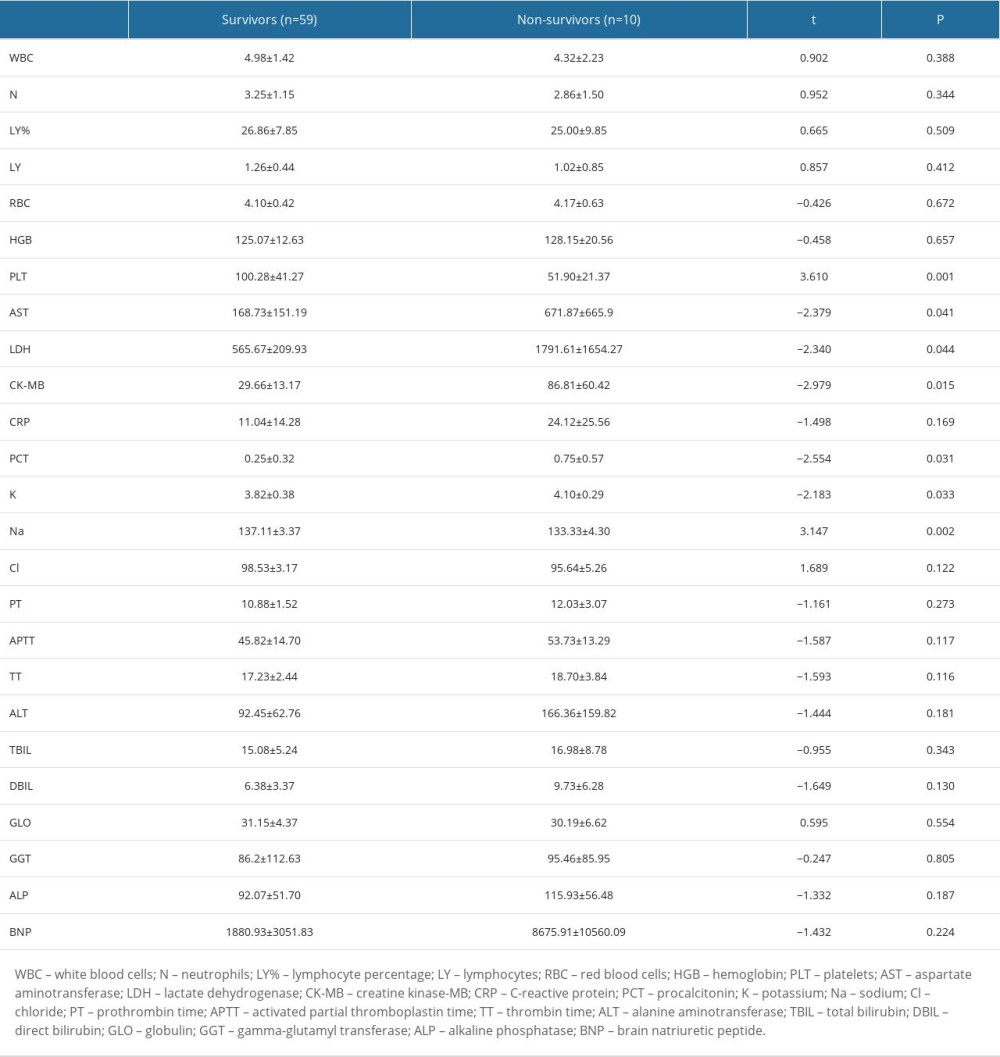 Table 3. Comparison of clinical symptoms and signs between the survivor and non-survivor groups.
Table 3. Comparison of clinical symptoms and signs between the survivor and non-survivor groups.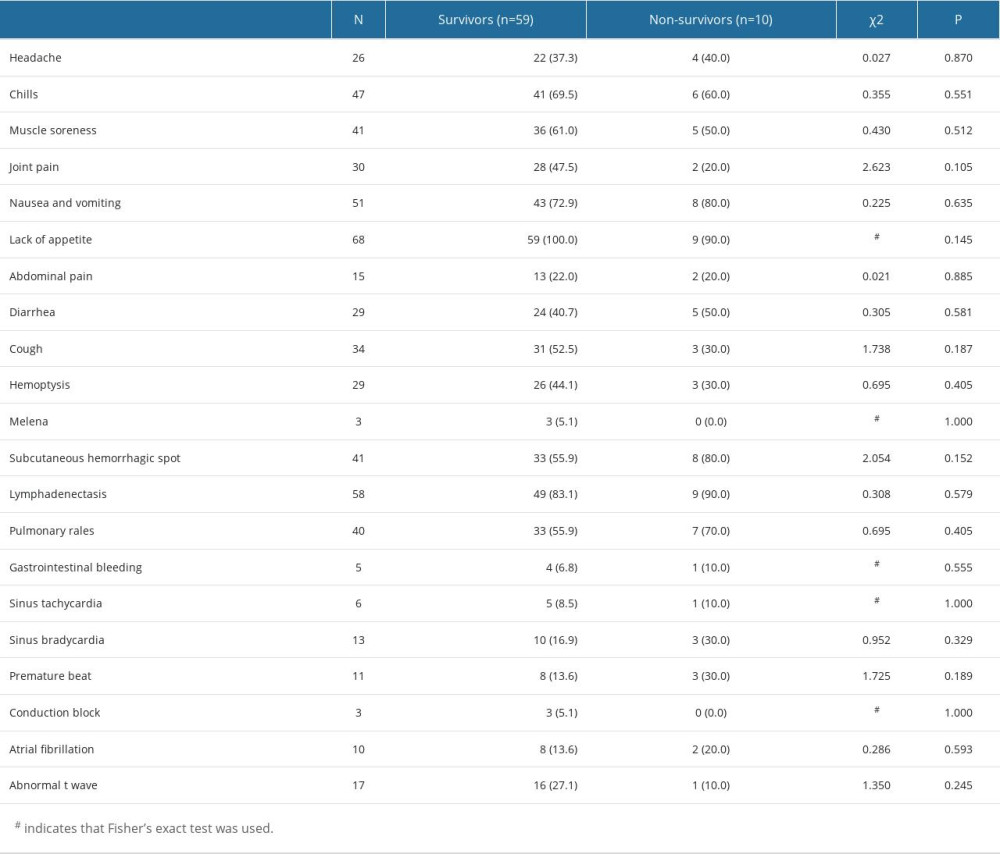 Table 4. Results of multiple logistic regression analysis.
Table 4. Results of multiple logistic regression analysis.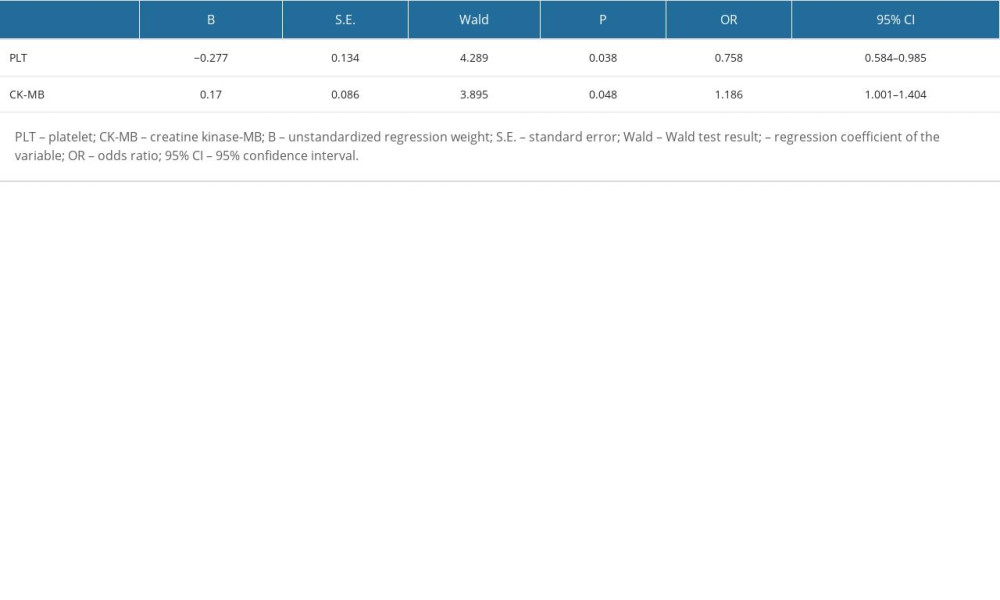
References
1. Yu XJ, Liang MF, Zhang SY, Fever with thrombocytopenia associated with a novel Bunyavirus in China: N Engl J Med, 2011; 364(16); 1523-32
2. Schoch CL, Ciufo S, Domrachev M, NCBI Taxonomy: A comprehensive update on curation, resources and tools: Database (Oxford), 2020; 2020; baaa062
3. Liu MM, Lei XY, Yu XJ, Meta-analysis of the clinical and laboratory parameters of SFTS patients in China: Virol J, 2016; 13(1); 198
4. Shin J, Kwon D, Youn SK, Characteristics and factors associated with death among patients hospitalized for severe fever with thrombocytopenia syndrome, South Korea, 2013: Emerg Infect Dis, 2015; 21(10); 1704-10
5. Li Z, Hu J, Cui L, Hong Y, Increased prevalence of severe fever with thrombocytopenia syndrome in eastern china clustered with multiple genotypes and reasserted virus during 2010–2015: Sci Rep, 2017; 7(1); 6503
6. Liu K, Zhou H, Sun RX, A national assessment of the epidemiology of severe fever with thrombocytopenia syndrome, China: Sci Rep, 2015; 5; 9679
7. Denic S, Janbeih J, Nair S, Acute thrombocytopenia, leucopenia, and multiorgan dysfunction: The first case of SFTS Bunyavirus outside China?: Case Rep Infect Dis, 2011; 2011; 204056
8. Choi SJ, Park SW, Bae IG, Severe fever with thrombocytopenia syndrome in South Korea, 2013–2015: PLoS Negl Trop Dis, 2016; 10(12); e0005264
9. Yoshikawa T, Shimojima M, Fukushi S, Phylogenetic and geographic relationships of severe fever with thrombocytopenia syndrome virus in China, South Korea, and Japan: J Infect Dis, 2015; 212(6); 889-98
10. Hayasaka D, Shimada S, Aoki K, Epidemiological survey of severe fever with thrombocytopenia syndrome virus in ticks in Nagasaki, Japan: Trop Med Health, 2015; 43(3); 159-64
11. Hayasaka D, Fuxun Y, Yoshikawa A, Seroepidemiological evidence of severe fever with thrombocytopenia syndrome virus infections in wild boars in Nagasaki, Japan: Trop Med Health, 2016; 44; 6
12. Kato H, Yamagishi T, Shimada T, Epidemiological and clinical features of severe fever with thrombocytopenia syndrome in Japan, 2013–2014: PLoS One, 2016; 11(10); e0165207
13. Hu JL, Li ZF, Wang XC, Risk factors for Bunyavirus-associated severe fever with thrombocytopenia syndrome: A community-based case-control study: PLoS One, 2016; 11(11); e0166611
14. McMullan LK, Folk SM, Kelly AJ, A new phlebovirus associated with severe febrile illness in Missouri: N Engl J Med, 2012; 367(9); 834-41
15. Deng B, Zhou B, Zhang S, Clinical features and factors associated with severity and fatality among patients with severe fever with thrombocytopenia syndrome Bunyavirus infection in Northeast China: PLoS One, 2013; 8(11); e80802
16. Chen Y, Jia B, Liu Y, Risk factors associated with fatality of severe fever with thrombocytopenia syndrome: A meta-analysis: Oncotarget, 2017; 8(51); 89119-29
17. Hu J, Li S, Zhang X, Correlations between clinical features and death in patients with severe fever with thrombocytopenia syndrome: Medicine (Baltimore), 2018; 97(22); e10848
18. Gai ZT, Zhang Y, Liang MF, Clinical progress and risk factors for death in severe fever with thrombocytopenia syndrome patients: J Infect Dis, 2012; 206(7); 1095-102
19. Park SY, Kwon JS, Kim JY, Severe fever with thrombocytopenia syndrome-associated encephalopathy/encephalitis: Clin Microbiol Infect, 2018; 24(4); 432e1-e4
20. Park SW, Song BG, Shin EH, Prevalence of severe fever with thrombocytopenia syndrome virus in Haemaphysalis longicornis ticks in South Korea: Ticks Tick Borne Dis, 2014; 5(6); 975-77
21. Yun SM, Lee WG, Ryou J, Severe fever with thrombocytopenia syndrome virus in ticks collected from humans, South Korea, 2013: Emerg Infect Dis, 2014; 20(8); 1358-61
22. Sun Y, Jin C, Zhan F, Host cytokine storm is associated with disease severity of severe fever with thrombocytopenia syndrome: J Infect Dis, 2012; 206(7); 1085-94
23. Deng B, Zhang S, Geng Y, Cytokine and chemokine levels in patients with severe fever with thrombocytopenia syndrome virus: PLoS One, 2012; 7(7); e41365
24. Xu Y, Shao M, Liu N, Clinical feature of severe fever with thrombocytopenia syndrome (SFTS)-associated encephalitis/encephalopathy: A retrospective study: BMC Infect Dis, 2021; 21(1); 904
25. Hiraki T, Yoshimitsu M, Suzuki T, Two autopsy cases of severe fever with thrombocytopenia syndrome (SFTS) in Japan: A pathognomonic histological feature and unique complication of SFTS: Pathol Int, 2014; 64(11); 569-75
26. Saijo M, Pathophysiology of severe fever with thrombocytopenia syndrome and development of specific antiviral therapy: J Infect Chemother, 2018; 24(10); 773-81
27. Li S, Li Y, Wang Q, Multiple organ involvement in severe fever with thrombocytopenia syndrome: An immunohistochemical finding in a fatal case: Virol J, 2018; 15(1); 97
28. Takahashi T, Maeda K, Suzuki T, The first identification and retrospective study of severe fever with thrombocytopenia syndrome in Japan: J Infect Dis, 2014; 209(6); 816-27
29. Kim KH, Lee MJ, Ko MK, Severe fever with thrombocytopenia syndrome patients with hemophagocytic lymphohistiocytosis retrospectively identified in Korea, 2008–2013: J Korean Med Sci, 2018; 33(50); e319
30. Mendoza CA, Ebihara H, Yamaoka S, Immune modulation and immune-mediated pathogenesis of emerging tickborne banyangviruses: Vaccines (Basel), 2019; 7(4); 125
31. Jia B, Yan X, Chen Y, A scoring model for predicting prognosis of patients with severe fever with thrombocytopenia syndrome: PLoS Negl Trop Dis, 2017; 11(9); e0005909
Tables
Table 1. Comparison of basic data between surviving and non-surviving cases.Table 2. Comparative results of laboratory tests between the survivor and non-survivor groups.Table 3. Comparison of clinical symptoms and signs between the survivor and non-survivor groups.Table 4. Results of multiple logistic regression analysis. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387