10 January 2023: Clinical Research
Evaluation of Supraglottic Jet Oxygenation and Ventilation in 105 Patients During Bronchoscopy Using the Twinstream Microprocessor-Controlled Jet Ventilator and the Wei Nasal Jet Tube
Mingyuan Yang1ABCDEF, Huafeng Wei2EF, Qingwu Hou1B, Bin Wang1B, Qinghao Cheng1ABCDEFG*DOI: 10.12659/MSM.938602
Med Sci Monit 2023; 29:e938602






Abstract
BACKGROUND: The Twinstream® ventilator is a microprocessor-controlled electric jet ventilator that allows the simultaneous application of 2 different jet streams, one at low frequency and one at high frequency to result in pulsatile bi-level (p-BLV) mode of ventilation. This study aimed to evaluate supraglottic jet oxygenation and ventilation in 105 patients during bronchoscopy using the Twinstream® microprocessor-controlled jet ventilator and the Wei Nasal Jet® (WNJ) tube.
MATERIAL AND METHODS: Patients were randomly divided into 2 parallel groups (N=50 per group): group W using the WNJ tube and group M using an endoscopic face mask connected to Twinstream® microprocessor-controlled jet ventilator under monitored anesthesia care. Arterial blood gas was examined and recorded 15 minutes after the initiation of procedure. The demographic and clinical characteristics, procedure duration, doses of anesthetics, and adverse events in the 2 groups were also recorded.
RESULTS: The arterial partial pressure of carbon dioxide (PaCO₂) (P=0.006) and lactic acid (P=0.001) were significantly lower, while pH (P=0.024) was significantly higher than in the group M. Pearson analysis showed that PaCO₂ was significantly correlated with ventilation tools (P=0.006) and procedure duration (P=0.003). Multiple linear regression analysis showed that ventilation tools and procedure duration were both independent influencing factors (P=0.006, P=0.002).
CONCLUSIONS: Supraglottic jet oxygenation and ventilation using the WNJ tube can reduce PaCO2 and had advantages in enhancing oxygenation and ventilation function in patients during bronchoscopy intervention therapy under monitored anesthesia care.
Keywords: airway management, High-Frequency Jet Ventilation, Hypoxia, Humans, Bronchoscopy, Ventilators, Mechanical, Respiration
Background
The incidence of lung diseases and tumors has been increasing constantly [1]. Bronchoscopy intervention technology has remarkable advantages in the diagnosis and treatment of pulmonary airway diseases, which are often treated under monitored anesthesia care [2,3]. Studies have shown that more than half patients undergoing bronchoscopy intervention experienced intraoperative hypoxemia in the absence of adequate oxygen administration [4]. Another study found that the incidence of intraoperative hypoxemia was about 40% during bronchoscopy intervention therapy under monitored anesthesia care [5].
Ventilation strategies are mainly divided into supraglottic airway (SGA) and subglottic tools. SGA is a relatively non-traumatic ventilation method that can maintain airway oxygenation during bronchoscopy intervention therapy. The advantages of using SGA include easier placement, less need of anesthetic drugs, and lower incidence of laryngeal and vocal cord injuries [6]. Laryngeal mask airway (LMA) and I-gel are commonly used for this purpose [7,8]. However, the insertion of LMA requires a deeper depth of anesthesia and causes more damage to the larynx. Due to its comfort and simplicity of wearing, endoscopic face masks are more widely used in clinical practice. The Wei Nasal Jet® (WNJ) tube is a newly invented 2-wall nasal airway for supraglottic jet oxygenation and ventilation (SJOV) and end-tidal partial pressure of carbon dioxide (CO2) monitoring [9–12].
Its inner diameter is 5.0 mm, outer diameter is 7.5 mm, and length is 18 cm. Although the WNJ tube has been used during bronchoscopy [12], there are no studies comparing the effects of WNJ tube versus endoscopic face mask on pulmonary oxygenation and ventilation function during bronchoscopy intervention under monitored anesthesia care. SJOV is a minimally invasive technique of jet ventilation with the jet nozzle above the vocal cords and delivering high concentrations of oxygen with jet ventilation driving pressure [10]. It aims at improving oxygenation in patients with respiratory depression and is widely used in cases with difficult airways [6,10–17].
The WNJ tube was proposed to be a better choice than endoscopic face masks for patients during bronchoscopy intervention therapy under monitored anesthesia care. This clinical trial aimed to examine SJOV using the WNJ tube on pulmonary oxygenation and ventilation function during bronchoscopy intervention therapy compared to SGA devices with endoscopic face mask.
Material and Methods
ETHICS APPROVAL:
The study received ethics approval of the senior academic committee of Emergency General Hospital, Beijing, China (K21-39) on 29/11/2021. All patients agreed to participate in the study and signed informed consent before surgery. This study was registered and approved by the Chinese Clinical Trial Registry on 06/12/2021. The registration number of this study is: ChiCTR2100054001 (Chinese Clinical Trial Registry).
STUDY POPULATION:
Patients were selected by the Center of Bronchoscopy Intervention, Emergency General Hospital, to undergo bronchoscopy intervention from December 2021 to January 2022. Inclusion criteria were as follows: (1) Underwent electronic flexible bronchoscope; (2) Duration of operation, between 20 and 60 minutes; (3) Age, 18–80 years; (4) ASA classification I-III. Exclusion criteria were as follows: (1) Diagnosed with cardiac respiratory failure and coma; (2) T-tube, endotracheal intubation, and tracheotomy, or SpO2 <90% in ambient air before the surgery; (3) History of mental and neurological disorders, sedative or hypnotic drugs and alcohol abuse; (4) History of nasal disease and surgery; (5) Change the methods of anesthesia during the operation; (6) Intraoperative massive hemorrhage; (7) History of nasopharyngeal tumor and surgery.
In accordance with different ventilation tools, the eligible patients were randomized in a 1: 1 ratio into 2 parallel groups by a physician blinded to the study. The 2 groups were the Wei Nasal Jet® tube (Well Lead Medical Ltd., Guangzhou, China) group (group W) and endoscopic face mask group (group M). Preoperatively, the anesthesiologist opened an envelope containing a group allocation number to ensure study blinding. A data investigator collected and recorded all perioperative data. The statistician and investigator were independent and blinded to the treatment.
All bronchoscopy intervention therapy procedures were performed by experienced endoscopists using electronic flexible bronchoscopes (Pentax, Japan).
ANESTHETIC SETTINGS AND MAINTENANCE:
Electrocardiogram (ECG), pulse oximetry (SpO2), and blood pressure monitoring were performed upon entrance to the operating room. Lidocaine (1%, 10 ml) was administered via the spray-as-you-go technique before bronchoscopy intervention procedure. Oxygen was inhaled by endoscopic face mask during anesthesia induction. One ml remifentanil (40 μg·ml−1) was intravenously dripped with an interval of 1 min, and total bolus dose of remifentanil was 1 μg·kg−1. Propofol (1 mg·kg−1) was injected 2 min after remifentanil injection during anesthesia induction.
Before placing WNJ, the nasal cavity was cleaned and lubricated, and 5 ml lidocaine ointment was applied to the outer wall of the WNJ tube. After sedation, the WNJ tube was inserted into the unobstructed nostril of patients. If the first placement failed, a second attempt could be made through the patient’s contralateral nasal cavity. If the second attempt failed again, the placement would be abandoned and an endoscopic face mask would be used instead. If the patient had nasal cavity bleeding, the insertion of the WNJ tube would be stopped. The nasal bleeding would be observed by flexible electronic bronchoscopy, and the corresponding hemostatic measures would be given. The position of the WNJ tube was confirmed by the endoscopists through an electronic flexible bronchoscope. Then, we connected the WNJ to a Twinstream® ventilator (Carl Reiner GMBH, Vienna, Austria). The ventilator parameters were set as fractional inspired oxygen (FiO2) of 1.0, a driving pressure (DP) of 14.5 psi, respiratory rate (RR) of 15 bpm, and I/E ratio of 1: 1.5.
The patients of group M were ventilated by endoscopic face mask with a Twinstream® ventilator. The parameters were the same as for group W. The connection of the WNJ (A) and endoscopic face mask (B) to the Twinstream® ventilator are shown in Figure 1.
Continuous infusion of remifentanil (0.10~0.15 μg·kg−1·min−1) and propofol (30~50 μg·kg−1·min−1) by microinjection pumps was administered and stopped at the end of the operation. The patients of group W and group M breathed spontaneously during the bronchoscopy intervention, maintaining a Ramsey sedation scale (RSS) score of 4~5. When the SpO2 value was <95%, the anesthesiologists increased the driving pressure by 7.25 psi and RR by 5 bpm, and when the SpO2 value was <90%, the anesthesiologists rescued with mask-bag ventilation.
The fluctuation of the patient’s mean arterial blood pressure (MAP) was controlled at a variation within 20% of the baseline. If the fluctuation of MAP was more than 20%, the depth of anesthesia was adjusted or a vasopressor was given.
DEMOGRAPHIC DATA INCLUDED: AGE, BODY MASS INDEX (BMI), AND GENDER:
Clinical data included: American Society of Anesthesiologists (ASA) classification, comorbidities, type of pulmonary disease, pathology, lesion location, degree of the airway stenosis, and procedure duration. The location of airway lesions was divided into 4 types: 1) main airway, 2) left or right main bronchial, 3) more than 2 lesion sites of airway, and 4) no airway lesion or distal bronchial. The degree of airway stenosis was graded to 4 levels: 1 for 0~49%, 2 for 50~74%, 3 for 75~89%, and 4 for above 90%.
Arterial blood gas analyses (arterial partial oxygen pressure [PaO2] and arterial partial pressure of carbon dioxide [PaCO2], pH, lactic acid) and glucose blood level were examined and recorded 15 minutes after initiation of the procedure.
Adverse events included: the incidence of intraoperative hypoxemia (SpO2 <90%), intraoperative severe hypercapnia (PaCO2 ≥80 mmHg), postoperative hypoxemia (SpO2 <90%), chemosis, and delayed recovery and transfer to the intensive care unit (ICU). The number of anesthetic doses was also recorded.
The primary aim was to evaluate the difference in PaO2 and PaCO2 between the 2 groups and its influencing factors. The secondary aims were to evaluate the differences in intraoperative glucose blood level, the incidence of adverse events, and number of anesthetic doses between the 2 groups.
STATISTICAL ANALYSIS:
In a pilot trial of 10 patients, PaCO2 was 54.5±8.62 mmHg and 62.4±13.19 mmHg. The sample size was estimated by the formula n=(μα±μβ)2(1+1/k) σ2/δ2 with a standard deviation of 0.8, and bilaterally equal to 0.05, or even 0.2 (power=0.8). This study thus planned to enroll 34 patients in each group, following sample size power analysis.
SPSS 20.0 software was used for data collation and statistical analysis. The Shapiro-Wilk method (W test) of SPSS was used to test normality of the data. The continuous data were expressed as mean±SD, and the count data were presented as the number and percentage. The chi-square test was used to compare the count data between the 2 groups. Univariate analysis of variance was used for overall comparison between the 2 groups, and least significance difference was used for multiple comparison between groups. Pearson analysis was used to investigate the correlation between blood gas indicators of PaO2 and PaCO2 and the clinical indicators of patients. Multiple linear regression analysis was used to explore the independent influencing factors of PaCO2.
Results
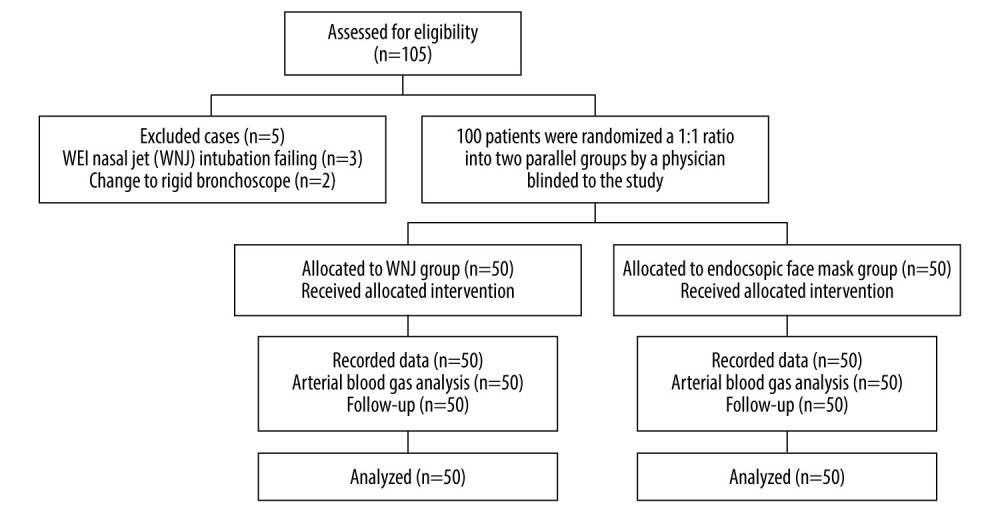
A total of 105 patients were enrolled. Three patients in group W were excluded because of failure of WNJ insertion and 2 patients in group M were excluded because of changing to a rigid bronchoscope under general anesthesia. All remaining patients tolerated the bronchoscopy intervention therapy well (Figure 2).
The demographic and clinical characteristics of patients are represented in Table 1. There were no significant differences between 2 groups in terms of age, BMI, gender, ASA classification, comorbidities, type of pulmonary disease, pathological type, lesion location, the degree of the airway stenosis, and the duration of procedure (
The results of arterial blood gas analysis showed that there was no significant difference in PaO2 and glucose between 2 groups (
Perioperative factors associated with PaCO2 were assessed via Pearson analysis. Age, BMI, ASA classification, chronic obstructive pulmonary disease, tracheal fistula, lobectomy, pulmonary tuberculosis, pulmonary bulla, lesion location, and degree of stenosis were not statistical correlated with increased PaCO2. Increased PaCO2 was significantly correlated with ventilation tools used (
Multiple linear regression was performed to analyze the predictive value of ventilation tools and procedure duration for PaCO2. The results showed that ventilation tools and procedure duration were both independent influencing factors (
Discussion
Monitored anesthesia care is increasingly used during bronchoscopy intervention therapy. It is preferred because it is associated with reduced incidence of intraoperative cough and it alleviates patient discomfort [3], and it allows rapid anesthesia emergence and recovery [2]. Proper respiration support during pulmonary procedures is a key factor. However, frequent mandatory sharing of the airway with the endoscopist during bronchoscopy intervention therapy makes it difficult to maintain oxygenation in patients under monitored anesthesia care.
Hypoxemia is the most common and severe intraoperative complication, accounting for 25% of anesthesia-related deaths [16]. ASA difficult airway management algorithm guidelines suggest that the use of I-gel can be replaced with some new supraglottic airway devices [18]. The advantages of WNJ use include ease of use, fewer complications, and the potential to increase the functional residual capacity (FRC) of the lungs. WNJ has become a commonly used ventilation tool for difficult airway management, especially for patients with poor cardiopulmonary function [9]. Jet ventilation is a technique used to maintain oxygenation and ventilation. SJOV via WNJ keeps ventilation systems open with few complications [12] and can assist oxygenation and ventilation during spontaneous breathing and apnea [16], as well as elective or emergent difficult airway management [19] for up to 45 minutes [15].
Feng et al demonstrated that SJOV via WNJ can effectively maintain adequate oxygenation and improve safety in patients with BMI over 30 undergoing hysteroscopies [14]. It also maintains adequate oxygenation during multiple and prolonged intubations in urgent difficult airway management [11,14]. Behrens suggested that SGA maintains oxygenation effectively, reduces anesthetic doses needed, and decreases risk for pulmonary complications [6]. Qin et al applied SJOV in patients receiving upper gastrointestinal endoscopy under monitored anesthesia care and demonstrated that SJOV had a good risk-benefit ratio and improved patient safety [10]. In another study, SJOV via WNJ was effective in providing airway support and improving intraoperative oxygenation [20].
Airway intervention surgery is a complex and high-risk procedure. Hypoxemia can occur at any time during airway procedures under sedation. Making correct choices about anesthesia, ventilation tools, ventilation methods, and strategies are critical to minimizing hypoxia [21,22]. Various techniques had been applied to ensure intraoperative oxygenation and ventilation of patients [23]. A balance among adequate oxygenation, depth of anesthesia, and patient airway safety is the key to anesthesia management for bronchoscopy intervention therapy procedures. In previous studies, SJOV via WNJ tube was found to reduce the incidence of intraoperative hypoxemia compared with nasal oxygen [10,12] and face mask oxygen [14]. A previous study found that use of an endoscopic face mask combined with SJOV improved oxygenation better than mask combined with high-flow oxygen [13]. Therefore, this study compared the oxygenation and ventilation function in SJOV via WNJ tube and endoscopic face mask during bronchoscopy intervention therapy under monitored anesthesia care.
The results showed that there was no significant difference in PaO2 and incidence of hypoxemia in patients with WNJ tube and endoscopic face mask, although the incidence of hypoxemia with endoscopic face mask was relatively higher. However, the PaCO2 of patients with WNJ tube was significantly lower than that using an endoscopic face mask. Pearson and multiple liner regression analysis both showed that PaCO2 was significantly correlated with ventilation tools. Additionally, the lactic acid levels of patients with WNJ tube were significantly lower than that of patients with endoscopic face mask, and pH was significantly higher than that of patients with endoscopic face mask.
Many studies have focused on oxygen supply rather than CO2 exhalation. After the administration of anesthetic drugs, the tendency for relaxation and collapse in upper respiratory tract tissue and muscle are inevitable [24], and the pharynx is the only segment of the upper airway that is not bounded by bony structures [25]. Glossocoma can cause significant upper airway obstruction and insufficient ventilation [26]. When ventilation is insufficient, SpO2 may be maintained in the normal range, but expiratory function may be impaired, resulting in hypercapnia and cardiovascular complications [27]. Lactic acid is the product of anerobic metabolism in the body and is considered as an indicator of tissue hypoxia [28] and a predictor of prognosis in critically ill patients. Increased blood lactic acid may occur when respiratory failure is accompanied with hypoxia, but most patients with respiratory failure have a normal or only mild increased blood lactic acid level. When severe respiratory failure occurs, it can also be accompanied by a significant increase in lactic acid, which may be caused by insufficient ventilation and hypoxia in the early stage. In this study, SJOV via WNJ delivered a high concentration of oxygen from the nasal cavity to the glottis, creating an artificial airway directly to the glottis and avoiding upper airway obstruction, thus improving ventilation. Although no difference in PaO2 was found between the WNJ and endoscopic mask groups, the slight increase in lactic acid also indicated a difference in ventilation capacity.
PaCO2 levels of patients increased with longer procedure duration and obstructive upper airway, leading to hypercapnia. Hypercapnia during bronchoscopy intervention therapy has long been a concern, as a sharp increase in CO2 levels can increase intracranial pressure and reduce cerebral perfusion, leading to cerebral ischemia [29,30]. Cheng et al proposed that hypercapnia (PaCO2 ≤100 mmHg) does not cause postoperative delirium and it improved postoperative cognitive function of patients, but it has an adverse effect on cognitive function when it is above 100 mmHg [31–33]. Jet ventilation at high frequency can impair CO2 elimination. Cheng and colleagues used an endoscopic mask in combination with high-frequency jet ventilation (HFJV) to supply oxygen for patients undergoing bronchoscopy intervention therapy and found that HFJV did not aggravate hypercapnia compared with normal frequency jet ventilation and conventional oxygenation [13].
Accordingly, the present study shows that the use of SJOV via a WNJ tube can improve ventilation function during bronchoscopy intervention therapy. Appropriate ventilation tools can meet the needs of surgery and improve intraoperative pulmonary function.
The present study has some limitations showed. First, we did not use bispectral index and neuromonitoring to determine the depth of sedation. RSS can be influenced by the concentration, dose, and rate of administration of anesthetics. BIS monitoring could potentially eliminate it. Second, no evaluation or comparison of postoperative pharyngeal conditions between groups was conducted. Thirdly, the Mallampati score was not used, which may affect ventilation function after anesthesia.
Conclusions
In summary, SJOV via WNJ tube and endoscopic face mask can both maintain oxygenation during bronchoscopy intervention therapy under monitored anesthesia care. SJOV via WNJ tube can reduce PaCO2 and lactic acid levels by preventing upper respiratory tract collapse, enhancing pulmonary ventilation function during bronchoscopy intervention therapy under monitored anesthesia care.


References
1. Ten Haaf K, van der Aalst CM, de Koning HJ, Personalising lung cancer screening: An overview of risk-stratification opportunities and challenges: Int J Cancer, 2021; 149(2); 250-63
2. de Lima A, Kheir F, Majid A, Pawlowski J, Anesthesia for interventional pulmonology procedures: A review of advanced diagnostic and therapeutic bronchoscopy: Can J Anaesth, 2018; 65(7); 822-36
3. Chadha M, Kulshrestha M, Biyani A, Anaesthesia for bronchoscopy: Indian J Anaesth, 2015; 59(9); 565-73
4. Fruchter O, Tirosh M, Carmi U, Prospective randomized trial of bispectral index monitoring of sedation depth during flexible bronchoscopy: Respiration, 2014; 87(5); 388-93
5. Lo YL, Lin TY, Fang YF, Feasibility of bispectral index-guided propofol infusion for flexible bronchoscopy sedation: A randomized controlled trial: PLoS One, 2011; 6(11); e27769
6. Behrens KM, Galgon RE, Supraglottic airway versus endotracheal tube during interventional pulmonary procedures – a retrospective study: BMC Anesthesiol, 2019; 19(1); 196
7. Garg R, Thakore S, Madan K, Use of i-gel for laser ablation of a bronchial lesion: BMJ Case Rep, 2017; 2017; bcr2017221679
8. Krecmerova M, Schutzner J, Michalek P, Laryngeal mask for airway management in open tracheal surgery – a retrospective analysis of 54 cases: J Thorac Dis, 2018; 10(5); 2567-72
9. Feng Y, Hou Y, Liang H, Wei H, WEI nasal jet tube during monitored anaesthesia care for removal of oesophageal foreign body for a patient with fragile cardiopulmonary function: Indian J Anaesth, 2019; 63(5); 403
10. Qin Y, Li LZ, Zhang XQ, Supraglottic jet oxygenation and ventilation enhances oxygenation during upper gastrointestinal endoscopy in patients sedated with propofol: A randomized multicentre clinical trial: Br J Anaesth, 2017; 119(1); 158-66
11. Liang H, Hou Y, Wei H, Feng Y, Supraglottic jet oxygenation and ventilation assisted fiberoptic intubation in a paralyzed patient with morbid obesity and obstructive sleep apnea: A case report: BMC Anesthesiol, 2019; 19(1); 40
12. Zha B, Wu Z, Xie P, Supraglottic jet oxygenation and ventilation reduces desaturation during bronchoscopy under moderate to deep sedation with propofol and remifentanil: A randomised controlled clinical trial: Eur J Anaesthesiol, 2021; 38(3); 294-301
13. Yang M, Wang B, Hou Q, High frequency jet ventilation through mask contributes to oxygen therapy among patients undergoing bronchoscopic intervention under deep sedation: BMC Anesthesiol, 2021; 21(1); 65
14. Liang H, Hou Y, Sun L, Supraglottic jet oxygenation and ventilation for obese patients under intravenous anesthesia during hysteroscopy: A randomized controlled clinical trial: BMC Anesthesiol, 2019; 19(1); 151
15. Li Q, Xie P, Zha B, Supraglottic jet oxygenation and ventilation saved a patient with ‘cannot intubate and cannot ventilate’ emergency difficult airway: J Anesth, 2017; 31(1); 144-47
16. Gupta S, Supraglottic jet oxygenation and ventilation – a novel ventilation technique: Indian J Anaesth, 2020; 64(1); 11
17. Shao L-J-Z, Zou Y, Liu F-K, Comparison of two supplemental oxygen methods during gastroscopy with propofol mono-sedation in patients with a normal body mass index: World J Gastroenterol, 2020; 26(43); 6867-79
18. Shofer SL, Wahidi MM, Davis WA, Significance of and risk factors for the development of central airway stenosis after lung transplantation: Am J Transplant, 2013; 13(2); 383-89
19. Wu CN, Ma WH, Wei JQ, Laryngoscope and a new tracheal tube assist lightwand intubation in difficult airways due to unstable cervical spine: PLoS One, 2015; 10(3); e0120231
20. Cavaliere S, Bezzi M, Toninelli C, Foccoli P, Management of post-intubation tracheal stenoses using the endoscopic approach: Monaldi Arch Chest Dis, 2016; 67(2); 73-80
21. Hohenforst-Schmidt W, Zarogoulidis P, Huang H, A new and safe mode of ventilation for interventional pulmonary medicine: The ease of nasal superimposed high frequency jet ventilation: J Cancer, 2018; 9(5); 816-33
22. Galway U, Zura A, Khanna S, Anesthetic considerations for bronchoscopic procedures: A narrative review based on the Cleveland Clinic experience: J Thorac Dis, 2019; 11(7); 3156-70
23. Inglis D, Gilhooly M, Patel A, The simultaneous use of three ventilatory techniques to maintain oxygenation in a patient undergoing tracheal laser resection of tumour: Anaesth Rep, 2019; 7(2); 70-72
24. Zhang W, Zhu C, Chen X, Comparison of the innovative endoscopic oropharyngeal airway and the conventional mouthpiece in elderly outpatients undergoing esophagogastroduodenoscopy under sedation: A prospective and randomized study: BMC Gastroenterol, 2022; 22(1); 8
25. Lahav YRE, Heyman Z, Doljansky J, Tongue base ultrasound: A diagnostic tool for predicting obstructive sleep apnea: Ann Otol Rhinol Laryngol, 2009; 118(3); 179-84
26. Karan SB, Rackovsky ED, Voter WA, Validation of a measurement to predict upper airway collapsibility during sedation for colonoscopy: J Clin Monit Comput, 2012; 26(6); 451-57
27. Ayuse T, Sawase H, Ozawa E, Study on prevention of hypercapnia by nasal high flow in patients undergoing endoscopic retrograde cholangiopancreatography during intravenous anesthesia: Medicine, 2020; 99(19); e20036
28. Pino RM, Singh J, Appropriate clinical use of lactate measurements: Anesthesiology, 2021; 134(4); 637-44
29. Marshall O, Chawla S, Lu H, Cerebral blood flow modulation insufficiency in brain networks in multiple sclerosis: A hypercapnia MRI study: J Cereb Blood Flow Metab, 2016; 36(12); 2087-95
30. Zhou Q, Cao B, Niu L, Effects of permissive hypercapnia on transient global cerebral ischemia-reperfusion injury in rats: Anesthesiology, 2010; 112(2); 288-97
31. Cheng Q, Li L, Lin D, Effects of acute hypercapnia on cognitive function in patients undergoing bronchoscope intervention: J Thorac Dis, 2019; 11(3); 1065-71
32. Cheng Q, Zhang J, Wang H, Effect of acute hypercapnia on outcomes and predictive risk factors for complications among patients receiving bronchoscopic interventions under general anesthesia: PLoS One, 2015; 10(7); e0130771
33. Cheng Q, Li L, Yang M, Moderate hypercapnia may not contribute to postoperative delirium in patients undergoing bronchoscopic intervention: Medicine, 2019; 98(22); e15906
Figures
Tables
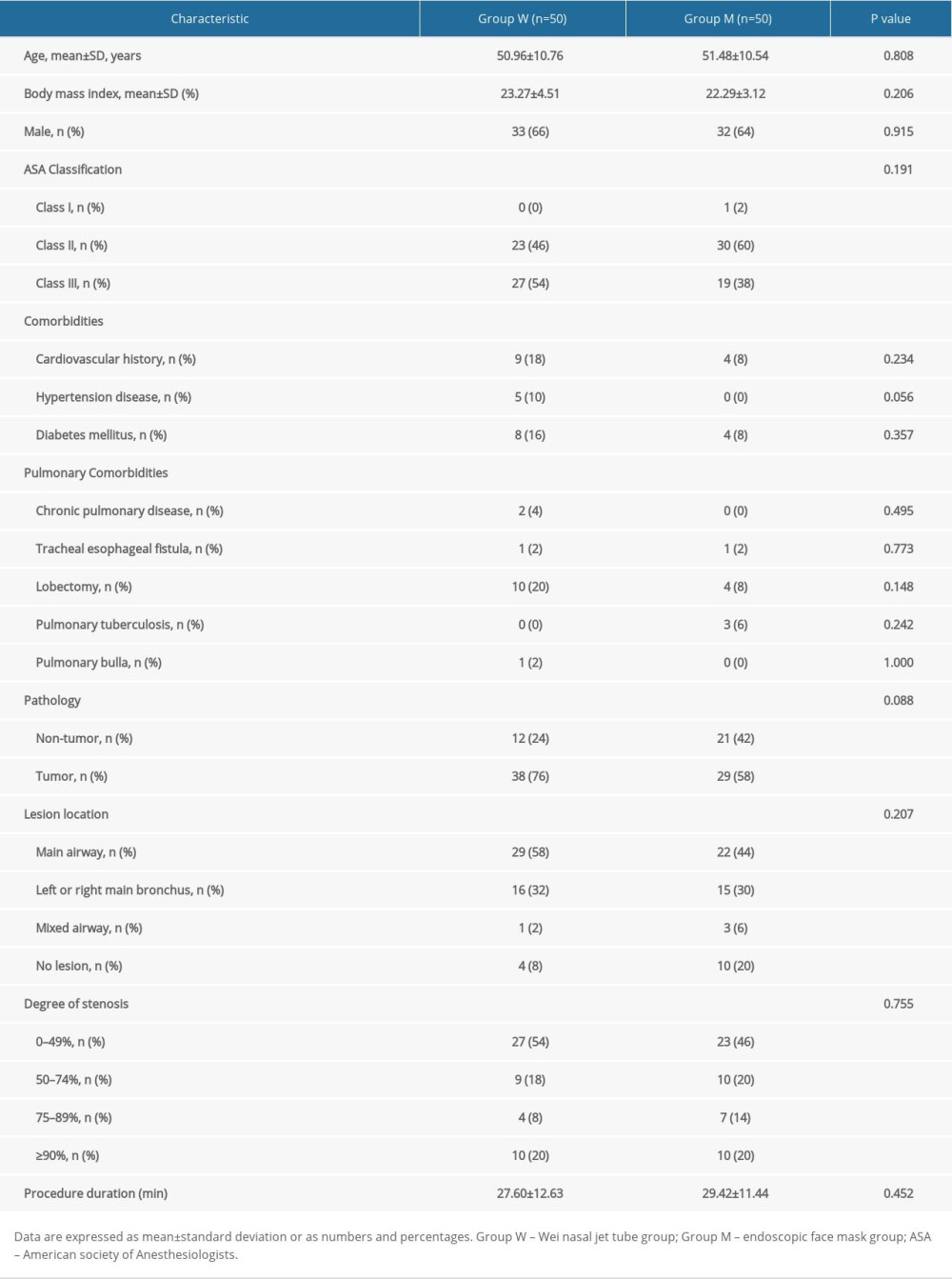 Table 1. Comparison of demographic and clinical patient characteristics between the 2 groups.
Table 1. Comparison of demographic and clinical patient characteristics between the 2 groups.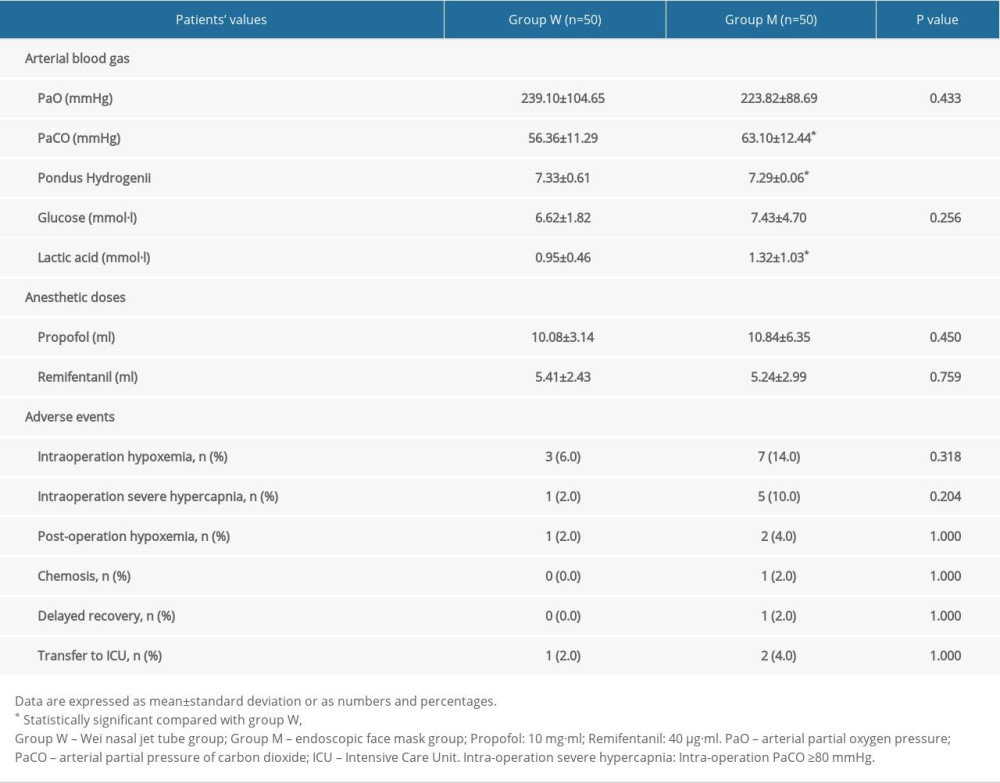 Table 2. Arterial blood gas analysis, anesthetic doses, and adverse events between the 2 groups.Table 1. Comparison of demographic and clinical patient characteristics between the 2 groups.Table 2. Arterial blood gas analysis, anesthetic doses, and adverse events between the 2 groups.
Table 2. Arterial blood gas analysis, anesthetic doses, and adverse events between the 2 groups.Table 1. Comparison of demographic and clinical patient characteristics between the 2 groups.Table 2. Arterial blood gas analysis, anesthetic doses, and adverse events between the 2 groups. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387