24 April 2023: Clinical Research
Clinical Study of Volar Median Approach Combined with Lateral Radial Auxiliary Approach in Treatment of C-Type Distal Radius Fractures: Our Clinical and Radiological Results
Yanqing Gu1ABC, Lei Zhao1BD, Yan Ren1E, Nakibuuka Joan Nyeenya2E, Yang Wang1F, Chenyang Xu1EF, Chunzhi Jiang1EFG*DOI: 10.12659/MSM.938806
Med Sci Monit 2023; 29:e938806






Abstract
BACKGROUND: The aim of the study was to explore the clinical implications of median approach combined with radial auxiliary plate in the treatment of C-type distal radius fractures.
MATERIAL AND METHODS: From January 2017 to January 2022, a total of 20 cases were collected, including 6 male and 14 female patients with closed fresh distal radius fractures. All patients received volar medium approach T-shaped locking plate treatment, as well as radial auxiliary plate open reduction and internal fixation. We recorded the incidence of median nerve injury, incidence of radial artery and vein or their branches injury, postoperative X-ray measurement of radial styloid process height, ulnar declination, palmar inclination, and Gartland-Werley score.
RESULTS: All surgical procedures were successful, and all patients were monitored for 3 to 12 months after the procedure. In the postoperative follow-up, there was no obvious loss of reduction. At the last follow-up, all patients’ articular surface flatness was less than 2 mm, and the mean values for palmar inclination and ulnar declination were (14.36°±3.55°) and (19.79°±2.57°), respectively. The average height of a radial styloid was 117±2.42 mm; functional evaluation: excellent in 12 (60%), good in 6 (30%), and fair in 2 cases (10%) cases. Five patients showed slight nerve injury, but all recovered quickly within 6 months.
CONCLUSIONS: The volar median approach, which combines a T-locking plate with a radial auxiliary plate for open reduction and internal fixation, is an effective treatment for unstable distal radius fractures.
Keywords: Fractures, Bone, distal radius fractures, Volar Median Approach, Radial Auxiliary Plate, Humans, Male, Female, Wrist Fractures, Radius Fractures, Range of Motion, Articular, Radiography, Treatment Outcome, Fracture Fixation, Internal, Bone Plates
Background
The wrist joint is an important part of the human body for fine movements, but it is also fragile; distal radius fracture accounts for approximately one-sixth of all body fractures and is the most common upper limb fracture [1]. Volar approach reduction and locking plate fixation is the current first-line treatment for distal radius fracture [2]. We discovered that internal fixation with a volar T-locking plate could not effectively support the lateral column in the treatment of unstable distal radius fractures of the lateral column due to severe bone fragmentation. This also increases the risk of fracture displacement following surgery, and plaster external fixation is frequently required to avoid loss of reduction. This could have a negative impact on the affected limb’s early functional exercise, lowering the level of functional recovery of the wrist joint. As a result, for unstable lateral column, distal radius fractures, the radial auxiliary plate combined with the volar T-locking plate can firmly fix the radial column fragment while stabilizing the medial column of the distal radius. It can also resist the pull of the brachioradialis muscle and effectively support the articular surface of the wrist joint, thus avoiding the postoperative loss of fracture reduction, and effectively maintain the length of the radius, palm inclination, ulnar declination, early postoperative functional exercise, and better functional recovery of wrist function.
The most frequently used classification system is that of the Arbeitsgemeinschaft für Osteosynthesefragen (AO). Morphologically, the fracture is divided into 3 types: extra-articular (A), unicondylar or combined metaphyseal (B), and intra-articular fractures (C). Each fracture type is subdivided into 3 groups (1, 2, or 3) based on fracture location and fracture morphology (complexity of the fracture) [3–5]. For the treatment of type C distal radius fractures, we used a median approach combined with an auxiliary radial incision, which allows us to effectively observe the ulnar column of the distal radius fracture and the medial column bone fragment through the median incision. Additionally, we can decide whether to make carpal tunnel incision based on the type of fracture, avoiding symptoms of median nerve entrapment [6,7]. In comparison to the traditional Henry approach, the median incision can pull the radial artery branch radially when making a radial auxiliary incision, avoiding injury to the radial artery branch and significantly lowering the risk of muscle necrosis between the 2 incisions. Lower radial bone fragment reduction and fixation may be visible through the radial auxiliary incision, which can be very beneficial for strong fixation of distal radius fractures.
Following-up examinations revealed that the volar median approach combined with radial incision can effectively repair distal radius fractures. As a result, this treatment is ideal for type C fractures (particularly types C2 and C3), lateral column, instability, and unstable distal radius fractures of the lateral column.
Material and Methods
SURGICAL APPROACH:
Patients were placed on the operating table in a supine position with their limbs abducted and their forearms fully supinated for brachial plexus or general anesthesia. A long incision was made from the volar side of the distal forearm to the transverse crease of the wrist; incising skin, subcutaneous tissue, and deep fascia in turn. The palmar branch of the median nerve was freed, and we gently freed the palmar branch of the median nerve, which is very important to reduce the symptoms of median nerve injury. The palmaris longus tendon was separated from the flexor pollicis longus tendon, and we pulled the palmaris longus tendon, median nerve, superficial finger, and deep finger tendon to the ulnar side with a hook, and pulled the flexor pollicis longus tendon and the flexor carpi radialis tendon to the radial edge. The pronator muscle was cut at the radial attachment site, and the other tendons were pulled toward the ulnar border. Following subperiosteal dissection, the fracture was revealed. We then decided whether to perform carpal tunnel decompression and fragment bone reduction, cut off part of the transverse carpal ligament, and ulnar declination based on the patient’s wrist joint swelling and bone fragmentation. Fine Kirschner wires were used if necessary to maintain reduction through the fracture line, and the bone plate was placed on the volar side of the distal radius, then the sliding hole was fixed with a common screw. The position of the plate was then adjusted, and the distal cancellous bone area of the fracture was secured with locking screws, as was the proximal end.
An auxiliary radial incision was made after the volar plate was placed. The radial auxiliary incision enters from the space between the brachioradialis muscle and the abductor pollicis longus tendon. The bone pry peels the extensor retinaculum without directly cutting the relevant muscles. The superficial branch of the radial nerve bypasses the wrist joint through the deep surface of the brachioradialis nerve fiber to the outside of the radius and reaches the back of the hand. Then, a radial anatomical plate was screwed onto the radial side of the distal radius. To ensure satisfactory fixation, the position of the steel plate screws was examined using imaging, fracture fixation was rigorously tested by passive wrist movement, and the abductor pollicis longus tendon could move freely. Finally, the severed pronator muscle was sutured, and the wound was cleaned and bandaged (Figures 1, 2).
POSTOPERATIVE MEASUREMENT AND FOLLOW-UP:
From January 2017 to January 2022, a total of 20 cases were collected, including 6 male and 14 female patients with closed fresh distal radius fractures according to AO classification type C who were admitted to Nanjing Hospital Affiliated to Nanjing Medical University. The radial styloid process height, ulnar declination, palmar inclination, and Gartland–Werley score were all measured postoperatively. Based on observational and evaluation criteria, we instructed patients to perform functional rehabilitation exercises in the early postoperative period, followed up with them, and recorded any wrist pain and functional recovery. (1) Compared radial styloid process height, ulnar declination, palmar inclination,mean ulnar variance and mean radial height X-ray results 3-month after surgery. We compared wrist function scores, and the Gartland-Werley wrist joint score was used, which primarily included: residual deformity, subjective evaluation, objective evaluation, complications, and arthritic changes: 0–2 is excellent, 3–8 is good, 9–20 is fair, and ≥21 is poor [5]. Subjective neurologic disorders, especially paresthesia in the median nerve fingers, were monitored by asking the patient about the presence or absence of prickling sensations in the thumb, the index finger, and the long finger. The occurrence of such symptoms was regarded as median nerve dysfunction. The superficial branch of the radial nerve injury is characterized by hypoesthesia of the skin on the dorsal side of the hand and three and a half fingers on the radial side, as well as the weakness of wrist extension. Electrophysiological evaluation was performed when these symptoms persisted 12 weeks after surgery.
STATISTICAL ANALYSIS:
The obtained data were statistically analyzed using SPSS 24.0 software, and measurement data were displayed as (χ±
Results
A total of 20 patients (6 males, 14 females; mean age 56.5±19.5; range, 25 to 76 years) who met the criteria were included. Union was achieved in all fractures. No patient experienced implant irritation, implant prominence, implant migration, hardware loosening, malunion, osteonecrosis, or plate/screw breakage, and none had infection, tendon ruptures, major nerve injuries, or hypertrophic scarring. No secondary surgery was required for any patient. Implants were not removed from any patient, and no neurovascular damage occurred. All patients were followed up for 3 to 12 months after surgery, and they were all satisfied with the healing of the surgical incision, with no necrosis between the 2 incisions in any of the patients. The flatness of the articular surface is less than 2 mm 3 months after surgery, and the mean values for palmar inclination and ulnar declination were 14.36°±3.55° and 19.79±2.57°, respectively. The average height of a radial styloid was 11.7±2.42 mm; mean ulnar variance was 1±1.5 (range, −3 to 3) mm, and the mean radial height was 10.3±3.4 (7 to 18) mm. Functional evaluation was excellent in 12 cases (60%), good in 6 cases (30%), and fair in 2 cases (10%). Regarding postoperative complications, there was no obvious loss of reduction in the postoperative review, but there was 1 case of postoperative pull injury of the superficial branch of the radial nerve accompanied by numbness, which resolved after 2 weeks of oral mecobalamin tablets treatment. Four out of 20 patients reported median nerve dysfunction such as prickly sensations and numb fingers. In all 4 patients, these symptoms resolved spontaneously without any further intervention or specific therapy within 3 months after surgery. There was no obvious traumatic arthritis or tendon adhesions due to the short follow-up time.
Discussion
Distal radius fractures are those that occur within 3 cm of the articular surface of the distal radius and have a high fracture rate. In 1996, Daniel of the Swiss AO group proposed the three-column theory of the distal radius [9]. The distal radius is divided into 3 columns: medial, intermediate, and lateral. The medial column, also known as the ulnar column, is made up of the ulnar styloid process and serves as the rotation axis of the forearm and wrist; the intermediate column is made up of the lunate fossa and the radial semilunar notch, and serves as the foundation for the stability of distal radius; and the lateral column is made up of the scaphoid fossa and the radial styloid process, which supports the carpal bone and provides an attachment point for the ligaments in the joint capsule. Because of the ulnar declination of the distal radius, any impact on the scaphoid of the articular surface of the hand could cause a shearing force at the radial styloid process, causing damage to the lateral cortex of the radius. Thus, supporting the lateral cortex is the best way to stabilize the lateral column. Furthermore, the lunate fossa and radial meniscus notch form the middle column, which is the foundation of the radius’s stability; damage to the middle column is typically caused by the entrapment of the lunate articular surface and is frequently accompanied by dorsal comminuted fracture; direct support on the ulnar dorsal side of the radius can stabilize this column. An auxiliary radial incision is an option for distal radius fractures and partial radial column fractures. According to previous publications, only the radial bone fragment including the radial styloid process, was fixed with Kirschner wire during treatment; however, radial fixation of distal radius fractures was not emphasized, which frequently results in internal fixation breakage, loss of reduction, and pin tract infection. Other clinical studies have found that radial bone fragments can be kept in place by radial screws when performing volar fixation of distal radius fractures with T-plates [10–12]. With the introduction of the three-column theory, radial fixation has become especially important when dealing with complex types and patients with osteoporotic distal radius fractures. Good radial fixation can better maintain radial ulnar declination and radial height, thus avoiding postoperative reduction loss and malunion.
The volar approach and locking plate internal fixation can effectively stabilize the middle column. The transvolar approach with locking compression plate cannot effectively prevent the displacement in patients with extremely unstable distal radius fractures on the radial side. When a fracture occurs, a portion of the cancellous bone of the distal radius compresses and deforms; even if the reduction is satisfactory during surgery, there is a risk of loss of reduction later [13]. Neither the volar plate nor the dorsal plate provides optimal adequate support for the lateral cortex of the lateral radial column, and fracture fragment fixation at the radial styloid process is ideal. Taylor believed that the radial additional small bone plate has a significantly higher strength to directly fix the radial dorsal bone fragment than the volar locking plate [14].
The traditional approach for the treatment of unstable distal radius fractures is the volar approach with locking plates. However, for extremely radially deviated distal radius fractures, most of these fractures are comminuted by the radial column. Due to the flip displacement caused by compression of the radiocarpal articular surface and stretch of the brachioradialis muscle, locking screws on the transverse arms of the T-plate will not provide precise fixation to all, especially the radial fragment, and thus cannot meet the “Fragment-specific fixation” standard [15,16]. In a cadaver study, Blythe et al found that the single volar steel plate was significantly weaker than the double steel plate in terms of stability and fatigue resistance [17]. Brandon et al investigated the use of a single volar plate in the treatment of AO type C3 fractures and found postoperative loss of fracture reduction in 10.4% [18]. The radial auxiliary plate combined with the volar anatomical plate can effectively fix the radial column on the basis of the effective fixation of the central column. It not only neutralizes the pulling effect of the brachioradialis muscle and prevents the radial and proximal displacement of the radial styloid process fragment, but also cross-fixes the mid-column fragment with the volar plate and screw, which greatly improves the fixation effect.
In the treatment of unstable distal radius fractures of the lateral column with a double volar-radial plate, we used a median incision. The advantages of this incision include sufficient exposure to fully expose the volar aspect of the distal radius and the inferior radioulnar joint, and it allows us to decide whether to perform carpal tunnel release based on the type of fracture to avoid symptoms of median nerve entrapment. None of the 20 patients who were followed up had symptoms of median nerve entrapment. Compared with the traditional Henry incision, the additional radial auxiliary incision has a longer distance between the 2 incisions, which can better avoid skin and muscle necrosis between the 2 incisions.
Overall, lateral column unstable distal radius fractures, mostly C-type fractures, especially C2 and C3 types, usually have lost stability of the lateral column and have marked radial instability of the distal fragment, all of which are good indications for the use of palmar-radial double plate fixation. When compared to single volar locking plate internal fixation, a radial auxiliary plate combined with volar T-shaped locking plate can firmly fix the radial column fragment while stabilizing the medial column of the distal radius. It is an effective method for clinical treatment of unstable distal radius fractures of the lateral column by resisting the pull of the brachioradialis muscle, avoiding loss of postoperative fracture reduction, and enabling early postoperative functional exercise to better restore wrist function.
Conclusions
The volar median approach, which combines a T-locking plate with a radial auxiliary plate for open reduction and internal fixation, is an effective treatment for unstable distal radius fractures. This can help to reconstruct the normal anatomy of the distal radius while also achieving strong fracture fixation, preventing postoperative loss of reduction and allowing for early functional exercise of the affected limb.
Figures
 Figure 1. Diagram for distal radius fracture surgery. The medial approach and radial auxiliary approach were used.
Figure 1. Diagram for distal radius fracture surgery. The medial approach and radial auxiliary approach were used. 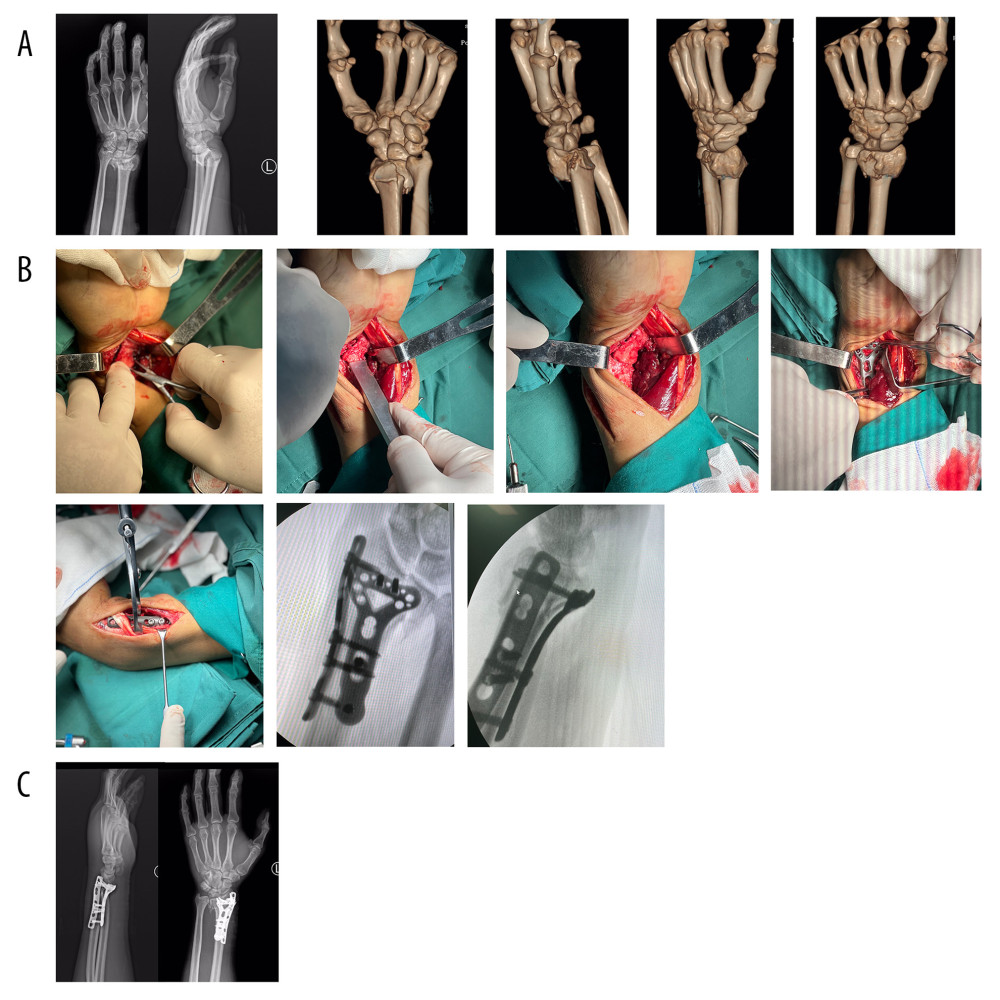 Figure 2. (A) X-ray and 3D CT examination of a typical surgical case prior to surgery. (B) Sharing of a typical case’s operation process. (C) X-ray examination of a typical case 3 months after surgery.
Figure 2. (A) X-ray and 3D CT examination of a typical surgical case prior to surgery. (B) Sharing of a typical case’s operation process. (C) X-ray examination of a typical case 3 months after surgery. References
1. Konrads C, Gonser C, Bahrs CFractures of the Distal Radius: Z Orthop Unfall, 2021; 159(2); 217-31 [in German]
2. Wichlas F, Haas N, Disch A, Machó D, Tsitsilonis SJ, Complication rates and reduction potential of palmar versus dorsal locking plate osteosynthesis for the treatment of distal radius fractures: Traumatology, 2014; 15(4); 259-64
3. Tannan SC, Pappou IP, Gwathmey FW, The extended flexor carpi radialis approach for concurrent carpal tunnel release and volar plate osteosynthesis for distal radius fracture: J Hand Surg Am, 2015; 40(10); 2026-31.e1
4. Kural C, Sungur I, Kaya I, Evaluation of the reliability of classification systems used for distal radius fractures: Orthopedics, 2010; 33; 801
5. Colton CL, Telling the bones: J Bone Joint Surg Br, 1991; 73; 362-64
6. Johnstone DJ, Radford WJ, Parnell EJ, Interobserver variation using the AO/ASIF classification of long bone fractures: Injury, 1993; 24; 163-65
7. Medici A, Meccariello L, Rollo G, Does routine carpal tunnel release during fixation of distal radius fractures improve outcomes?: Injury, 2017; 48(Suppl 3); S30-S33
8. Lozano-Calderón SA, Souer S, Mudgal C, Wrist mobilization following volar plate fixation of fractures of the distal part of the radius: J Bone Joint Surg Am, 2008; 90(6); 1297-304
9. Rikli DA, Regazzoni P, Fractures of the distal end of the radius treated by internal fixation and early function. A preliminary report of 20 cases: J Bone Joint Surg Br, 1996; 78(4); 588-92
10. Hoffmann JD, Stewart J, Kusnezov N, Radial plate fixation: A novel technique for distal radius fractures: Hand (N Y), 2017; 12(5); 471-75
11. Ring D, Prommersberger K, Jupiter JB, Combined dorsal and volar plate fixation of complex fractures of the distal part of the radius: J Bone Joint Surg Am, 2005; 87(Suppl 1); 195-212
12. Sagerfors M, Bjorling P, Niklasson J, Pettersson K, Combined volar T-plate and dorsal Pi-plate for distal radius fractures: A consecutive series of 80 AO type C2 and C3 cases: J Wrist Surg, 2019; 8; 180-85
13. Chhabra AB, Yildirim B, Adult distal radius fracture management: J Am Acad Orthop Surg, 2021; 29(22); e1105-e16
14. Taylor KF, Parks BG, Segalman KA, Biomechanical stability of a fixed-angle volar plate versus fragment-specific fixation system: Cyclic testing in a C2-type distal radius cadaver fracture model: J Hand Surg Am, 2006; 31(3); 373-81
15. Geissler WB, Clark SM, Fragment-specific fixation for fractures of the distal radius: J Wrist Surg, 2016; 5(1); 22-30
16. Hozack BA, Tosti RJ, Fragment-specific fixation in distal radius fractures: Curr Rev Musculoskelet Med, 2019; 12(2); 190-97
17. Blythe M, Stoffel K, Jarrett P, Kuster M, Volar versus dorsal locking plates with and without radial styloid locking plates for the fixation of dorsally comminuted distal radius fractures: A biomechanical study in cadavers: J Hand Surg Am, 2006; 31(10); 1587-93
18. Earp BE, Foster B, Blazar PE, The use of a single volar locking plate for AO C3-type distal radius fractures: Hand (N Y), 2015; 10(4); 649-53
Figures
Figure 1. Diagram for distal radius fracture surgery. The medial approach and radial auxiliary approach were used.Figure 2. (A) X-ray and 3D CT examination of a typical surgical case prior to surgery. (B) Sharing of a typical case’s operation process. (C) X-ray examination of a typical case 3 months after surgery. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387