17 April 2023: Clinical Research
Tri-Lock Bone Preservation Stem Versus Conventional Corail Stem in Primary Total Hip Arthroplasty via Direct Anterior Approach: A Short-Term, Retrospective, Comparative Study
Kun Chu1ABCDE, Yuchuan Wang1D, Meng Yang1A, Congcong Wei1B, Jia Huo1C, Mengxuan Yao1B, Zihang Li1D, Huijie Li1D*DOI: 10.12659/MSM.939635
Med Sci Monit 2023; 29:e939635






Abstract
BACKGROUND: he present study was performed to evaluate the clinical efficacy of Tri-Lock bone preservation stems vs conventional Corail stems in primary total hip arthroplasty via direct anterior approach.
MATERIAL AND METHODS: In this retrospective analysis, patients receiving THA via DAA in a single-center hospital from January 2019 to March 2020 were assessed for eligibility and assigned to either a Tri-Lock BPS group or a Corail group based on the use of prostheses. Outcome measures for the efficiency evaluation of the 2 prostheses included perioperative outcomes, imaging results, Harris Hip Score, Western Ontario and McMaster University Osteoarthritis Index, and visual analog scale scores at 3, 6, 12, and 24 months postoperatively.
RESULTS: A total of 204 patients were included, including 98 patients (98 hips) in the Tri-Lock BPS group and 106 patients (106 hips) in the Corail group. Patients receiving Tri-Lock BPS exhibited better pain relief than those with Coral stems. Tri-Lock BPS had a higher safety profile vs Corail stems by significantly reducing the risk of complications (P=0.004). A markedly increased HHS score (84.42±16.27 vs 78.61±12.78, P=0.002) and a lower WOMAC score (25.08±15.39 vs 32.14±11.56, P=0.001) at 3 months postoperatively were observed in patients with Tri-Lock BPS vs those with Corail stems, indicating better restoration of hip function using Tri-Lock BPS.
CONCLUSIONS: During total hip arthroplasty via DAA, Tri-Lock BPS causes a smaller surgical wound, reduces the operative time and intraoperative bleeding, and produces less soft-tissue damage vs Corail stems, providing great benefits in femoral prosthesis placement.
Keywords: Arthroplasty, Replacement, Hip, Hip Prosthesis, Male, Animals, Retrospective Studies, Femur, Treatment Outcome, Prosthesis Design
Background
Total hip arthroplasty (THA) is an effective treatment for end-stage hip function loss caused by femoral head necrosis, traumatic osteoarthritis, and hip dysplasia [1]. With advances in medical technology, THA is evolving toward minimal invasiveness and enhanced recovery to facilitate postoperative recovery and improve patient prognosis [2]. The direct anterior approach (DAA) in THA produces a small surgical wound, rapid recovery, and a short length of hospital stay [3,4]. However, difficulties in lateral femoral exposure and mounting in DAA are the main causes of a high risk of complications, prolonged operative time, intraoperative periprosthetic fractures, broad fascial tensor tears, and poor wound healing [5,6]. Despite special surgical positions and DAA-specific surgical instruments designed to address these issues, the surgical outcome is still unsatisfactory [7]. Accordingly, some orthopedic surgeons used shorter femoral stems to reduce the risk of periprosthetic fractures and muscle injuries [8]. Short stems have been frequently used in THA [9], as they have a small surgical incision, thereby preserving more bone tissues and providing more favorable surgical conditions [10,11]. Previous trials revealed a short-term survival of 94–100% and an incidence of thigh pain of 4%–18% in patients receiving THA with short stems [8,9,12–15]. Standard Corail stems (Depuy, Johnson & Johnson, Warsaw, IN, USA) are classic, biologic, all-hydroxyapatite-coated prostheses with a biconical interface trapezoidal design that increases the contact area with bones, provides rotational stability in the medullary cavity, and prevents subsidence, thereby facilitating early bone growth and reducing prosthetic micromotion [16]. However, Corail stems require a tight cortical fit and may compromise a large amount of proximal femoral bone volume to obtain sufficient initial stability, easily leading to increased intraoperative bone damage and even medically-induced fractures. In addition, the straight stem design also causes stresses concentrated in the isthmus of the femur, resulting in possible distal thigh pain in the long term [17].
Tri-Lock bone preservation stems (BPS) (Depuy, Johnson & Johnson, Warsaw, IN, USA) are modified Tri-Lock prostheses with shortened length and width of the distal stem, which obviates the need for distal reaming and allows more bone preservation than traditional stems. The triple locking approaches – axial taper locking, lateral rotation locking, and Gription layer locking – provide good initial and long-term stability, so as to form long-term osseointegration and avoid prosthesis loosening [3]. Moreover, the shortened distal stem length and skip pad of BPS preserve more bone volume of the greater trochanter, further reducing the risk of medically-induced fractures [9,18–20]. Previous literature has reported the clinical and imaging features of Tri-Lock BPS and Corail stems [3,9,21,22] but mostly in non-DAA-THA. To this end, the present study was designed to assess the efficacy of Tri-Lock BPS (Figure 1A) vs conventional Corail stem in primary THA via DAA (Figure 1B).
Material and Methods
INCLUSION AND EXCLUSION CRITERIA:
In this retrospective analysis, patients receiving THA via DAA in the Third Hospital of Hebei Medical University from January 2019 to March 2020 were assessed for eligibility and assigned to either a Tri-Lock BPS group or a Corail group based on the intraoperative use of prostheses.
Inclusion criteria were: (1) patients aged 18–80 years; (2) patients were diagnosed with ischemic necrosis of the femoral head, osteoarthritis of the hip, femoral neck fracture, rheumatoid arthritis, developmental dysplasia of the hip (DDH), and were treated for the first time with unilateral DAA-THA; (3) use of Corail stems or Tri-Lock BPS; (4) patients who were followed up for over 2 years.
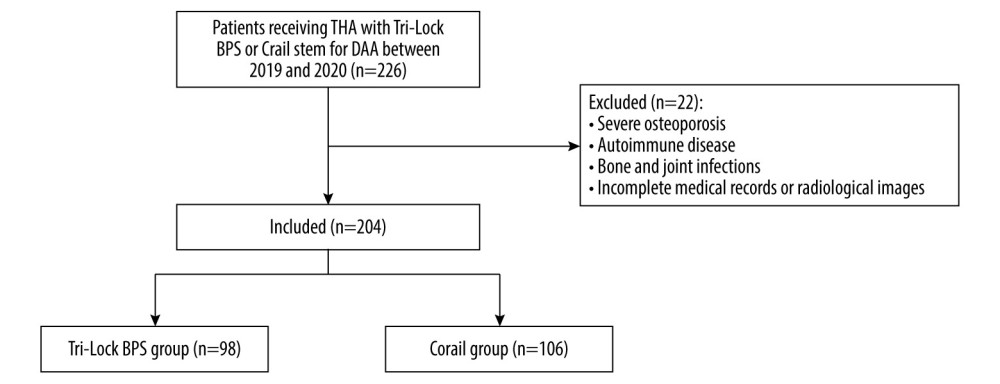
Exclusion criteria were: (1) severe osteoporosis; (2) autoimmune diseases; (3) bone and joint infections; (4) incomplete medical records or radiological images (Figure 2).
This study retrospective study with anonymous data was approved by the Ethics Committee of our hospital (approval number 2020-004-1), which waived the requirement for informed consent.
SURGICAL PROCEDURES:
THA was performed by a senior surgeon with specialist training using the DAA approach. Prior to surgery, the angle of the osteotomy and the size of the stem were evaluated according to preoperative planning. With the patient in a lateral position, after general anesthesia or continuous epidural anesthesia, an incision was made 2 cm lateral and inferior to the anterior superior iliac spine towards the small head of the fibula, and the subcutaneous tissue and the broad fascial tensor muscle were incised. The gap between the broad fascial tensor muscle and the sartorius muscle was separated first, then the rectus femoris space was separated and the ascending branch of the lateral femoral artery was ligated. After protecting the broad fascial tensor using a broad fascial tensor protector, the femoral neck was exposed after incising the anterior joint capsule. Based on preoperative template measurements, the femoral head was removed by osteotomy at an appropriate distance above the lesser trochanter, and the acetabular cup was adjusted before placing the lateral acetabular prosthesis and liner. The proximal femur was exposed by external rotation, internal rotation, and extreme posterior extension of the hip, and the medullary cavity was enlarged with reamers of increasing sizes. A Tri-Lock BPS was placed after a satisfactory mold fitting under C-arm fluoroscopy. The hip joint was repositioned after the placement of the femoral head prosthesis. After intraoperative determination of good hip stability and joint motion, the incision was irrigated and sutured layer by layer (Figure 3).
The procedure in the Corail group was largely consistent with that of the Tri-Lock BPS group. The only exception was that when exposing the proximal femur, hooks were placed at the medial aspect of the femoral neck and the greater trochanter to expose the femoral neck as far outward as possible. The incision was lengthened to further release the short external rotator muscle group and the lateral joint capsule of the greater trochanter until the proximal femur was exposed to meet the requirements of marrow expansion. The Corail stem was implanted after satisfactory mold fitting under fluoroscopy. The femoral head prosthesis was installed and repositioned, followed by irrigation and suturing (Figure 4).
POSTOPERATIVE MANAGEMENT AND REHABILITATION:
Preoperative cephalosporin was administered until 24 h postoperatively to prevent infection, and radiographs were performed to assess the position of the prosthesis. Low-molecular-weight heparin and appropriate functional exercise of the affected limb were administered to prevent lower-extremity deep vein thrombosis. Patients were allowed to use crutches for partial weight bearing as tolerated on the first postoperative day, and crutch use was recommended for 4 weeks.
BASELINE DATA COLLECTION:
Preoperative baseline data of all patients were recorded, including baseline clinical indicators such as gender, age, height, weight, body mass index (BMI), alcohol consumption, smoking, etiology of THA, and postoperative complications. Surgical indices were recorded, including operative time, bleeding, incision length, and intraoperative and postoperative complications. The visual analog scale (VAS) scores of the patients before and after treatment were recorded to evaluate their postoperative pain, ranging from 0 to 10 points. Higher scores indicate greater pain.
CLINICAL FUNCTION ASSESSMENT:
The clinical function of the patients was assessed preoperatively and 3, 6, 12, and 24 months postoperatively. The Harris hip score (HHS) was used to evaluate the hip function restoration of the patients [23] from 4 domains of pain, function, deformity, and range of motion. The total score was 100 points, with <70 for a poor functional recovery, 70–80 for a moderate recovery, and 90–100 for a good recovery. The Western Ontario and McMaster University Osteoarthritis Index (WOMAC) was used for the assessment of postoperative hip function recovery, comprising 24 parameters, with a total score of 96 [24]. Hip structure and function were assessed in terms of 3 major aspects – pain, stiffness, and joint function – with a maximum score of 96 indicating the worst hip function.
IMAGING ASSESSMENT:
All patients’ anterior-posterior pelvic orthoptic radiographs were assessed preoperatively, postoperatively, and at 2 years of follow-up. Anteroposterior radiographs were performed with the patient at a distance of 90 cm from the X-ray tube in a 15° inward standing position with feet placed shoulder-width apart.
At the final follow-up, imaging measurements were evaluated using standardized anatomical landmarks, and all imaging measurements (neck stem angle, eccentric distance, prosthetic force line, difference in lower-limb length, prosthetic subsidence, osteolysis, heterotopic ossification, and stress shielding) were performed independently by 2 experienced orthopedic surgeons using data obtained from our hospital’s picture archiving and communication system, and the values were averaged between the 2 surgeons.
All measurements were performed by 2 senior operators, who were not involved in surgical operations. To assess intra- and inter-observer reproducibility, 20 patients were randomly chosen, and each measurement was performed twice independently, with an interval of 1 week. All intra-group correlation coefficients used to evaluate reproducibility in this study were >0.9.
STATISTICAL ANALYSIS:
All data were statistically analyzed using SPSS 20.0 (IBM, Armonk, USA). Continuous variables are expressed as mean±standard deviation, and categorical variables are expressed as counts and percentages. Data normality was tested using the Shapiro-Wilk test, and the chi-square test or Fisher’s exact probability method was used to compare the 2 sets of categorical variables, as appropriate. If the variables were non-normally distributed, the Mann-Whitney test was used to analyze continuous variables. Continuous variables were compared between the 2 groups using the
Results
PATIENT CHARACTERISTICS:
Between January 2019 and March 2020, we identified 98 patients (98 hips) who received DAA-THA with Tri-Lock BPS (Depuy, Johnson & Johnson, Warsaw, IN, USA) and 106 patients (106 hips) who received DAA-THA with Corail stem (Depuy, Johnson & Johnson, Warsaw, IN, USA).
This study extracted the medical data of 226 patients who underwent DAA-THA at the Third Hospital of Hebei Medical University from January 2019 to March 2020 from the database. After excluding 12 patients with incomplete medical history or radiological images, 8 with severe osteoporosis, and 2 with preoperative infection, a total of 204 patients (148 males and 56 females) were recruited. The eligible patients included 98 patients receiving DAA-THA with Tri-Lock BPS (98 hips) (Depuy, Johnson & Johnson, Warsaw, IN, USA) (72 males and 26 females) and 106 patients receiving DAA-THA with Corail stem (106 hips) (Depuy, Johnson & Johnson, Warsaw, IN, USA) (76 males and 30 females). The 2 groups were well-balanced in terms of patient characteristics (P>0.05), such as mean age (53.85±11.13 vs 52.43±10.60, P=0.351) and BMI (25.62±2.07 kg/m2 vs 24.93±3.30, P=0.076) (Table 1).
PERIOPERATIVE INDICES:
The length of stay was 6.84±2.15 days in the Tri-Lock BPS group and 7.23±1.95 days in the Corail group (
The study documented 6 (6.1%) cases of complications in the Tri-Lock BPS group and 21 (19.8%) cases in the Corail group, and the Corail group had 6 (5.6%) cases of poor wound healing vs 0 cases in the Tri-Lock BPS group. Four of these 6 patients were obese and 2 had diabetes mellitus, all presenting with wound dehiscence, peripheral hematoma, and delayed healing. They were treated conservatively with local wound care, dressing changes, and oral antibiotics until wound healing 22–30 days postoperatively. Subsequent follow-up confirmed good wound healing, and no further treatment was required (Table 2).
CLINICAL FUNCTION:
The preoperative VAS score was 3.69±1.04 in the Tri-Lock BPS group and 3.65±1.09 in the Corail group (P=0.776). Patients receiving Tri-Lock BPS exhibited better pain mitigation than those with Coral stems, as evidenced by the markedly lower VAS scores at 24 h, 48 h, and 72 h postoperatively (P<0.05) (Table 3).
The preoperative HHS and WOMAC scores were 54.21±12.56 and 56.47±12.86 in the Tri-Lock BPS group and 53.39±12.21 and 55.44±15.29 in the Corail group (P>0.005), respectively. At 3 months postoperatively, the HHS score was 84.42±16.27 in the Tri-Lock BPS group and 78.61±12.78 in the Corail group (P=0.002), respectively. The WOMAC score at 3 months postoperatively was 25.08±15.39 in the Tri-Lock BPS group and 32.14±11.56 in the Corail group (P=0.001), respectively. However, these discrepancies disappeared at 6 months postoperatively, and the hip function between the 2 groups of patients was similar at 1 year, 2 years, and at the final follow-up after surgery (P>0.05) (Table 4).
IMAGING RESULTS:
No significant differences were reported in the preoperative neck stem angle (132.78±4.31° vs 133.53±5.06°,
The Tri-Lock BPS group had 93 cases (94.8%) of neutral force line of the prosthesis, 3 cases (3.0%) of internal rotation, and 2 cases (2.0%) of external rotation, while the Corail group had 99 cases (93.3%) of neutral force line of the prosthesis, 4 cases (3.7%) of internal rotation, and 3 cases (2.8%) of external rotation (
The patients were followed up for 32.55±2.76 months in the Tri-Lock BPS group and 31.94±2.55 months in the Corail group. No prosthetic subsidence or osteolysis was reported during postoperative follow-ups in any patients.
Ectopic ossification was present in 2 cases in the Tri-Lock BPS group, with 1 (1.0%) case of grade 1 and 1 (1.0%) case of grade 2, and in 3 cases in the Corail group, with 2 (1.8%) cases of grade 1 and 1 (0.9%) case of grade 2 (
By the time of the final follow-up, 57 cases of stress shielding were present in the Tri-Lock BPS group, including 27 cases (27.5%) of grade 1, 21 cases (21.4%) of grade 2, 9 cases (9.1%) of grade 3, and 0 cases of grade 4. The Corail group had 64 cases, including 24 cases (22.6%) of grade 1, 28 cases (26.4%) of grade 2, 12 cases (11.3%) of grade 3, and 1 case of grade 4 (0.9%) (P=0.749) (Table 5).
Discussion
The use of femoral stems of different lengths can affect postoperative recovery and complications. It has been shown that in DAA-THA, conventional standard-length stems were associated with poorer pain mitigation and function recovery, and a higher incidence of periprosthetic fractures when compared with short stems [31]. Tri-Lock BPS has been reported to produce more pain alleviation and a higher safety profile vs conventional Corail stems [3,22]. These perioperative functional differences are attributable to the steeper DAA learning curve, and the incidence of these perioperative complications decreases as the surgeon becomes more experienced in surgery [32]. As a result, controversies remain as to whether Tri-Lock BPS exhibits better clinical outcomes in terms of early functional recovery, pain control, and prosthesis implantation imaging position compared to Corail stems in DAA-THA. The present study showed that the Tri-Lock BPS and the Corail stem had similar outcomes in terms of prosthetic implantation imaging results at 2-year follow-up. However, compared with Corail stems, Tri-Lock BPS in DAA-THA provided substantial benefits in reducing surgical wound and intraoperative hemorrhage and enhancing pain mitigation and hip function restoration.
Proximal femoral exposure is a major factor affecting surgical incision, operative time, and intraoperative bleeding [31–33]. The superior perioperative indices with Tri-Lock BPS vs Corail stems in the current study may be attributable to the short and curved design of Tri-Lock BPS. This type of femoral prosthesis requires a small incision for implantation and can be well implanted with low requirements for soft-tissue release and elevation of the proximal femur. It protects the greater trochanter while enlarging the femoral medullary cavity, reducing the pressure on the greater trochanter during implantation. The shortened distal length of the stem and the skip pad are effective in avoiding periprosthetic fractures. The 50° femoral neck osteotomy angle of the Tri-Lock BPS allows for better preservation of the femoral spur, enhances proximal fixation, and offers shallower depth of medullary file reaming compared to Corail stems, thereby reducing surgical blood loss and shortening operative time.
Prolonged operative time and intraoperative bleeding are also positively associated with anesthesia-related risks, wound problems, and perioperative complication incidences [34,35]. Studies have shown that Tri-Lock BPS offers more advantages over Corail stems in terms of perioperative complications during DAA-THA [3,22]. The results are consistent with our current research findings. Previous studies found increased pressure on the greater trochanter from a standard-length femoral stem when the proximal femur is not adequately exposed during DAA surgery, resulting in an increased risk of fracture [36,37]. Moli et al [8] compared the fracture rate between short stems and conventional standard stems and found a lower intraoperative fracture rate in the short stem group (0.4% vs 3.1% P<0.05). However, Daniell et al [38] compared the incidence of periprosthetic fractures in Tri-Lock BPS and control groups and found a similar incidence of fractures, consistent with our research results. Periprosthetic fractures occurred in 1 case (1.0%) in the Tri-Lock BPS group and 4 cases (3.7%) in the Corail group, both of which were proximal femoral fractures, with no statistically significant difference between the 2 groups (
The morphology of the surgical implant is a key factor affecting wound healing. It has been reported that the incidence of poor wound healing in initial DAA-THA ranges from 1% to 11.5% [5,35]. During femoral marrow expansion, standard long stems are more prone to skin and proximal femoral soft-tissue injury than short wedge-shaped stems. This may be related to the higher elevation of the proximal femur required for longer stems [39]. In the present study, there were 6 cases (5.6%) of poor wound healing in the Corail group and no cases in the Tri-Lock BPS group, of which 4 patients were obese and 2 were diabetic. Despite the influence of obesity and diabetes on wound healing, we found a certain degree of wear and subcutaneous hematoma at the proximal end of the postoperative incision in patients with poor wound healing. The main causes may be the difficulty in lifting the proximal femur and compression and abrasion of the femoral expansion stem and femoral stem during implantation. The Tri-Lock BPS group had a lower incidence of poor wound healing.
In THA, VAS, HHS, and WOMAC scores are important indicators for evaluating hip function [40–42]. Vahdet et al [39] compared the VAS, HHS, and WOMAC scores of short vs standard stems in DAA-THA preoperatively vs 2 years postoperative follow-up and revealed no significant differences between the 2 groups. Guo et al [3] compared the VAS, HHS, and WOMAC scores of Tri-Lock BPS vs Corail stems in non-DAA-THA, preoperatively vs 4 years postoperatively, and also found no significant differences between the 2 groups. These results demonstrated that both Tri-Lock BPS stems and Corail stems showed similar benefits in terms of long-term postoperative hip pain mitigation and functional recovery in DAA-THA. However, disparities in the VAS, HHS, and WOMAC scores between Tri-Lock BPS and Corail stems in DAA-THA have not yet been explored. Here, we found a superior functional restoration of the hips after the implantation of Tri-Lock BPS vs Corail stems. This result may be attributed to the more significant muscle soft-tissue injury around the femoral prosthesis caused by standard stems vs short stems. A prior study suggested that the magnitude of muscle damage and serum markers of inflammation could objectively measure the invasiveness of surgery [43]. Moreover, it has been shown that the level of inflammatory markers after DAA-THA was positively correlated with the duration of surgery and the severity of soft-tissue damage [44]. This suggests that the better functional outcome of the Tri-Lock BPS compared to Corail stems at 3 months postoperatively in the current study may be related to the significantly shorter duration of surgery and the milder soft-tissue damage with Tri-Lock BPS vs Corail stems. The hip function showed similar functional outcomes at all time points after 6 months postoperatively. In addition, we found significantly greater pain relief with the Tri-Lock BPS than with the Corail stem in the early postoperative period (24 h, 48 h, 72 h) (
The implantation position of the prosthetic component is associated with the function and durability of THA [45]. Inappropriate eccentric spacing may lead to compromised hip function and deteriorated prosthetic instability, while offset errors in the femoral prosthesis and differences in lower-limb length may result in poor recovery of hip function, rotor bursitis, claudication, and gait disturbances [46,47]. Stress shielding, prosthesis subsidence, and osteolysis expedite aseptic loosening of the prosthesis and decrease long-term survival [48]. Vahdet et al [39] found no significant differences between short stems and standard stems, showing good outcomes in radiological indices at 2-year follow-up after DAA-THA. In contrast, Guo et al [3] showed that Tri-Lock BPS and Corail stems exhibited favorable outcomes in most radiological indices without significant differences at 4-year follow-up, but Tri-Lock BPS outperformed Corail stems in reducing bone loss around the stem while ensuring initial stability of the prosthesis [3]. This may be attributed to the fact that short wedge stems can differentially reduce the effective load on the distal femur to achieve a better fit with the proximal femur, providing a relatively greater load on the proximal bone and thus reducing the stress shielding of the femur [48,49]. Nonetheless, comparison analyses of radiological indices of Tri-Lock BPS vs Corail stems in DAA-THA have not been conducted. In the current study, the short-term radiological indices (cervical stem angle, eccentric distance, prosthetic body line, difference in lower limb length, prosthetic subsidence, osteolysis, heterotopic ossification, and stress shielding) in both groups were consistent with the results of the study by Vahdet et al, with favorable results without significant inter-group differences. In contrast, the different results of the stress shielding may be caused by the short follow-up, for which long-term results are required. Overall, both Tri-Lock BPS and Corail stems provide promising radiographic results in DAA-THA.
The limitations of the current study include the small sample size and the short-term follow-ups. To the best of our knowledge, no retrospective studies have examined the clinical and imaging outcomes of Tri-Lock BPS vs Corail stems in DAA-THA. However, studies with larger sample sizes and longer-term follow-ups are needed to assess the long-term benefits of Tri-Lock BPS vs Corail stems. All procedures in our study were performed by the same surgeon. Although this can avoid the effect of different surgical techniques, our results should be validated and confirmed in a study of multiple randomized surgeons.
Conclusions
During total hip arthroplasty with DAA, Tri-Lock BPS causes a smaller surgical wound, reduces the operative time and intraoperative bleeding, and produces less soft-tissue damage vs Corail stems, providing great benefits in femoral prosthesis placement. Use of Tri-Lock BPS was associated with faster recovery of hip function than with Corail stems in the early postoperative period. The imaging results of Tri-Lock BPS were similar to those of Corail stems in the short term, whereas the long-term outcomes require further investigation.



References
1. Christensen CP, Jacobs CA, Comparison of patient function during the first six weeks after direct anterior or posterior total hip arthroplasty (THA): A randomized study: J Arthroplasty, 2015; 30(9 Suppl); 94-7
2. Ma MY, Progress of research on femoral side complications and treatment of total hip arthroplasty with direct anterior approach: Chinese Journal of Bone and Joint Surgery, 2022; 15(3); 221-27
3. Guo J, Tan J, Peng L, Comparison of Tri-Lock bone preservation stem and the conventional standard corail stem in primary total hip arthroplasty: Orthop Surg, 2021; 13(3); 749-57
4. Zawadsky MW, Paulus MC, Murray PJ, Johansen MA, Early outcome comparison between the direct anterior approach and the mini-incision posterior approach for primary total hip arthroplasty: 150 consecutive cases: J Arthroplasty, 2014; 29(6); 1256-60
5. Christensen CP, Karthikeyan T, Jacobs CA, Greater prevalence of wound complications requiring reoperation with direct anterior approach total hip arthroplasty: J Arthroplasty, 2014; 29(9); 1839-41
6. Lee GC, Marconi D, Complications following direct anterior hip procedures: Costs to both patients and surgeons: J Arthroplasty, 2015; 30(9 Suppl); 98-101
7. Melman WP, Mollen BP, Kollen BJ, Verheyen CC, First experiences with the direct anterior approach in lateral decubitus position: Learning curve and 1 year complication rate: Hip Int, 2015; 25(3); 251-57
8. Molli RG, Lombardi AV, Berend KR, A short tapered stem reduces intraoperative complications in primary total hip arthroplasty: Clin Orthop Relat Res, 2012; 470(2); 450-61
9. Burt CF, Garvin KL, Otterberg ET, Jardon OM, A femoral component inserted without cement in total hip arthroplasty. A study of the Tri-Lock component with an average ten-year duration of follow-up: J Bone Joint Surg Am, 1998; 80(7); 952-60
10. Attenello J, Chan S, Naito K: J Orthop, 2019; 16(2); 118-22
11. Darwich A, Pankert K, Ottersbach A, 5-year clinical and radiographic results of the direct anterior approach for total hip arthroplasty using a collared cementless femoral short-stem prosthesis: J Clin Med, 2022; 11(2); 346
12. Hozack W, Gardiner R, Hearn S, Taperloc femoral component. A 2-6-year study of the first 100 consecutive cases: J Arthroplasty, 1994; 9(5); 489-93
13. Keisu KS, Orozco F, Sharkey PF, Primary cementless total hip arthroplasty in octogenarians. Two to eleven-year follow-up: J Bone Joint Surg Am, 2001; 83(3); 359-63
14. McLaughlin JR, Lee KR, Total hip arthroplasty with an uncemented femoral component. Excellent results at ten-year follow-up: J Bone Joint Surg Br, 1997; 79(6); 900-7
15. McLaughlin JR, Lee KR, The outcome of total hip replacement in obese and non-obese patients at 10- to 18-years: J Bone Joint Surg Br, 2006; 88(10); 1286-92
16. Vidalain JP, Twenty-year results of the cementless Corail stem: Int Orthop, 2011; 35(2); 189-94
17. Yakkanti RR, Greif DN, Berge DJV, Robinson RP, Survival and performance of a dual tapered-wedge fully HA-coated press fit femoral stem: Arch Orthop Trauma Surg, 2023; 143(3); 1651-61
18. Bobyn JD, Pilliar RM, Cameron HU, Weatherly GC, The optimum pore size for the fixation of porous-surfaced metal implants by the ingrowth of bone: Clin Orthop Relat Res, 1980(150); 263-70
19. Ulivi M, Orlandini LC, Meroni V, Lombardo MDM, Peretti GM, Clinical performance, patient reported outcome, and radiological results of a short, tapered, porous, proximally coated cementless femoral stem: results up to seven years of follow-up: J Arthroplasty, 2018; 33(4); 1133-38
20. Teloken MA, Bissett G, Hozack WJ, Ten to fifteen-year follow-up after total hip arthroplasty with a tapered cobalt-chromium femoral component (tri-lock) inserted without cement: J Bone Joint Surg Am, 2002; 84(12); 2140-44
21. Liu Y, Wei WX, Zeng Y, Comparison of femoral bone mineral density changes around 3 common designs of cementless stems after total hip arthroplasty – a retrospective cohort study: Orthop Surg, 2022; 14(6); 1059-70
22. Yang F, Evaluation of the efficacy of the Tri-Lock bone-preserving femoral stem vs the Corail femoral stem prosthesis in total hip arthroplasty: Electronic Journal of Modern Medicine and Health Research, 2022; 6(14); 27-30
23. Huang BL, Yu NS, Harris score after artificial total hip arthroplasty: Journal of Modern Clinical Medical Bioengineering, 2004(01); 44-46
24. Bellamy N, WOMAC: A 20-year experiential review of a patient-centered self-reported health status questionnaire: J Rheumatol, 2002; 29(12); 2473-76
25. Bellamy N, Buchanan WW, Goldsmith CH, Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee: J Rheumatol, 1988; 15(12); 1833-40
26. Mahmood SS, Mukka SS, Crnalic S, Sayed-Noor AS, The influence of leg length discrepancy after total hip arthroplasty on function and quality of life: A prospective cohort study: J Arthroplasty, 2015; 30(9); 1638-42
27. Kim YH, Kim JS, Joo JH, Park JW, A prospective short-term outcome study of a short metaphyseal fitting total hip arthroplasty: J Arthroplasty, 2012; 27(1); 88-94
28. Zweymüller KA, Schwarzinger UM, Steindl MS, Radiolucent lines and osteolysis along tapered straight cementless titanium hip stems: A comparison of 6-year and 10-year follow-up results in 95 patients: Acta Orthop, 2006; 77(6); 871-76
29. Hug KT, Alton TB, Gee AO, Classifications in brief: Brooker classification of heterotopic ossification after total hip arthroplasty: Clin Orthop Relat Res, 2015; 473(6); 2154-57
30. Teloken MA, Bissett G, Hozack WJ, Ten to fifteen-year follow-up after total hip arthroplasty with a tapered cobalt-chromium femoral component (tri-lock) inserted without cement: J Bone Joint Surg Am, 2002; 84(12); 2140-44
31. Dietrich M, Kabelitz M, Dora C, Zingg PO, Perioperative fractures in cementless total hip arthroplasty using the direct anterior minimally invasive approach: Reduced risk with short stems: J Arthroplasty, 2018; 33(2); 548-54
32. Tissot C, Vautrin M, Luyet A, Borens O, Are there more wound complications or infections with direct anterior approach total hip arthroplasty?: Hip Int, 2018; 28(6); 591-98
33. Rivera F, Bardelli A, Giolitti A, Promising medium-term results of anterior approach with an anatomical short stem in primary hip arthroplasty: J Orthop Traumatol, 2021; 22(1); 8
34. Obata R, Bito H, Ohmura M, The effects of prolonged low-flow sevoflurane anesthesia on renal and hepatic function: Anesth Analg, 2000; 91(5); 1262-68
35. Surace P, Sultan AA, George J, The association between operative time and short-term complications in total hip arthroplasty: An analysis of 89,802 surgeries: J Arthroplasty, 2019; 34(3); 426-32
36. Berend KR, Mirza AJ, Morris MJ, Lombardi AV, Risk of periprosthetic fractures with direct anterior primary total hip arthroplasty: J Arthroplasty, 2016; 31(10); 2295-98
37. Yu H, Liu H, Jia M, A comparison of a short vs a conventional femoral cementless stem in total hip arthroplasty in patients 70 years and older: J Orthop Surg Res, 2016; 11; 33
38. Ponzio DY, Shahi A, Park AG, Purtill JJ, Intraoperative proximal femoral fracture in primary cementless total hip arthroplasty: J Arthroplasty, 2015; 30(8); 1418-22
39. Uçan V, Ezici V, Aliyev O, Comparison of tapered-wedge short and standard-length femoral stems in single-stage bilateral direct anterior total hip arthroplasty: Int Orthop, 2021; 45(12); 3119-27
40. Vishwanathan K, Akbari K, Patel AJ, Is the modified Harris hip score valid and responsive instrument for outcome assessment in the Indian population with pertrochanteric fractures?: J Orthop, 2018; 15(1); 40-46
41. Roorda LD, Jones CA, Waltz M, Satisfactory cross cultural equivalence of the Dutch WOMAC in patients with hip osteoarthritis waiting for arthroplasty: Ann Rheum Dis, 2004; 63(1); 36-42
42. Leiss F, Götz JS, Maderbacher G, Excellent functional outcome and quality of life after primary cementless total hip arthroplasty (THA) using an enhanced recovery setup: J Clin Med, 2021; 10(4); 621
43. Larsson K, van der Linden W, Creatine kinase in tibial shaft fractures. Serum creatine kinase levels in patients with tibial shaft fractures: Arch Orthop Trauma Surg (1978), 1981; 98(1); 41-43
44. Mjaaland KE, Kivle K, Svenningsen S, Comparison of markers for muscle damage, inflammation, and pain using minimally invasive direct anterior vs direct lateral approach in total hip arthroplasty: A prospective, randomized, controlled trial: J Orthop Res, 2015; 33(9); 1305-10
45. Siebenmorgen JP, Stronach BM, Mears SC, Stambough JB, The use of intraoperative digital radiography alignment software to assess implant placement in total hip arthroplasty: Curr Rev Musculoskelet Med, 2021; 14(6); 369-77
46. Flecher X, Ollivier M, Argenson JN, Lower limb length and offset in total hip arthroplasty: Orthop Traumatol Surg Res, 2016; 102(1 Suppl); S9-20
47. Small SR, Berend ME, Howard LA, Acetabular cup stiffness and implant orientation change acetabular loading patterns: J Arthroplasty, 2013; 28(2); 359-67
48. Wilkinson JM, Hamer AJ, Rogers A, Bone mineral density and biochemical markers of bone turnover in aseptic loosening after total hip arthroplasty: J Orthop Res, 2003; 21(4); 691-96
49. Westphal FM, Bishop N, Puschel K, Morlock MM, Biomechanics of a new short-stemmed uncemented hip prosthesis: An in-vitro study in human bone: Hip Int, 2006; 16(Suppl 3); 22-30
Figures
Tables
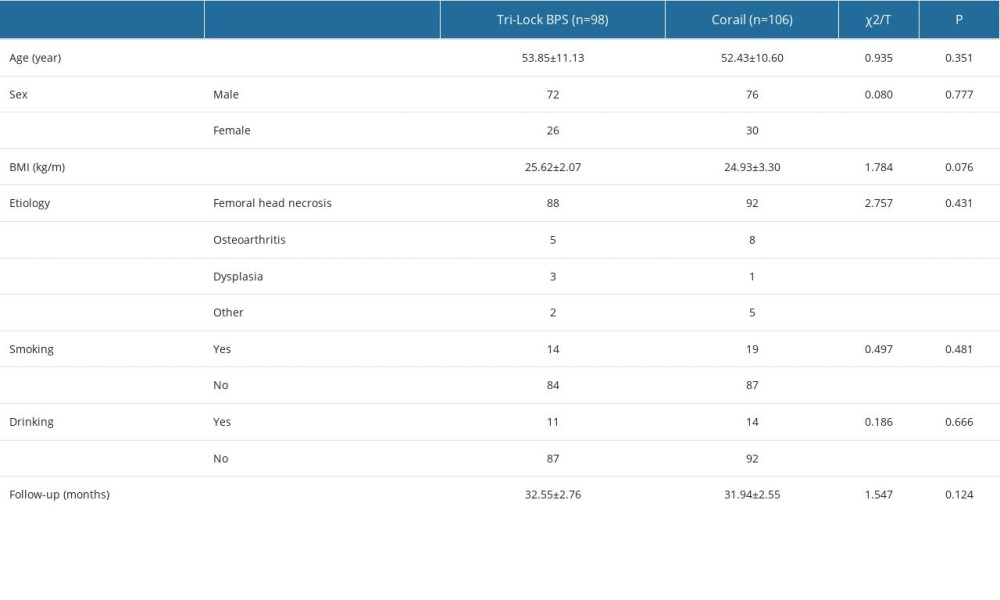 Table 1. Patient characteristics.
Table 1. Patient characteristics. Table 2. Perioperative indices and complications.
Table 2. Perioperative indices and complications.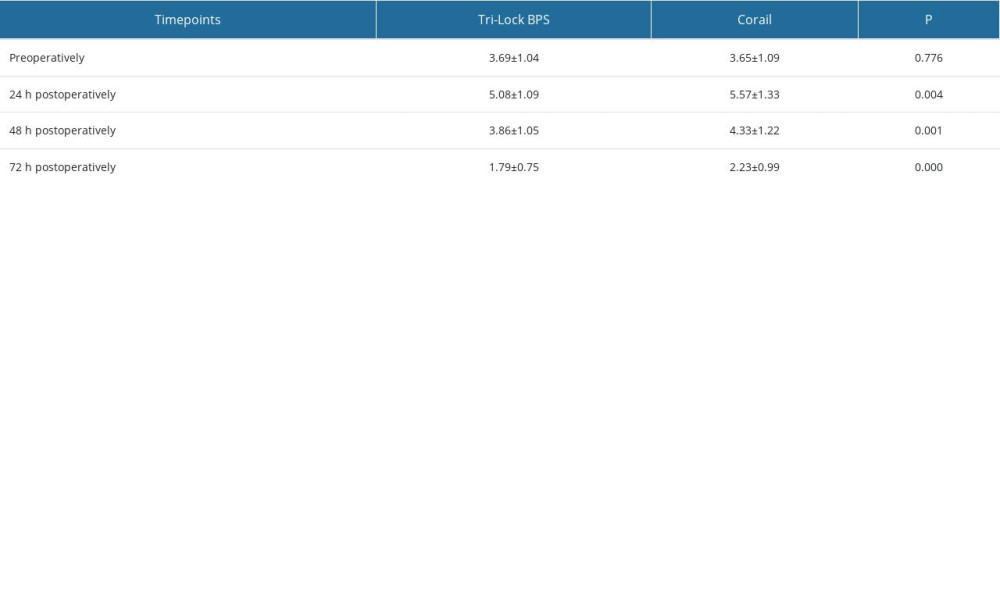 Table 3. Preoperative and postoperative VAS scores.
Table 3. Preoperative and postoperative VAS scores.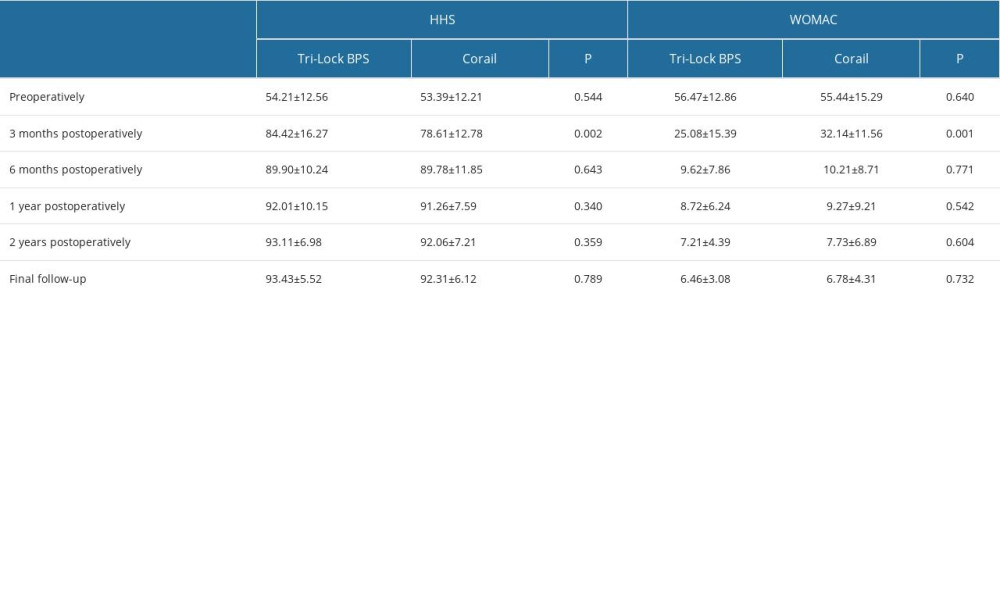 Table 4. HHS and WOMAC scores.
Table 4. HHS and WOMAC scores.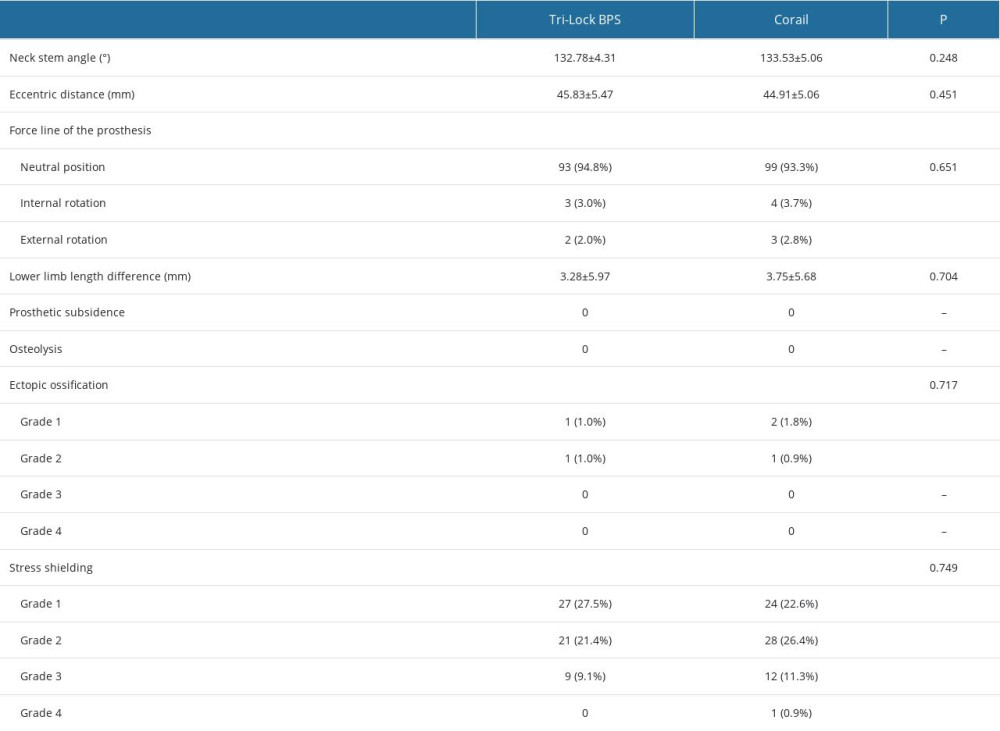 Table 5. Postoperative prosthesis imaging results.Table 1. Patient characteristics.Table 2. Perioperative indices and complications.Table 3. Preoperative and postoperative VAS scores.Table 4. HHS and WOMAC scores.Table 5. Postoperative prosthesis imaging results.
Table 5. Postoperative prosthesis imaging results.Table 1. Patient characteristics.Table 2. Perioperative indices and complications.Table 3. Preoperative and postoperative VAS scores.Table 4. HHS and WOMAC scores.Table 5. Postoperative prosthesis imaging results. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387