12 June 2023: Review Articles
Frontiers in Understanding the Pathological Mechanism of Diabetic Retinopathy
Lei Zhan1ABDEF*DOI: 10.12659/MSM.939658
Med Sci Monit 2023; 29:e939658






Abstract
ABSTRACT: The retina is a light-sensitive membrane responsible for optical signal reception and concatenation with the optic nerve. Retinal damage causes blurred vision or visual dysfunction. Diabetic retinopathy (DR) is a common microvascular complication of diabetes mellitus (DM) that is induced by the interaction of multiple factors and mechanisms. Hyperglycemia and hypertension are potential risk factors for DR. With the growing number of DM patients, the incidence of DR increases if DM is untreated. Epidemiological data show that DR is a leading cause of blindness in working-aged adults. Regular ophthalmological check-ups, laser treatment, and interdisciplinary consultation for reducing visual atrophy can help prevent and treat DR. Although the pathogenesis of DR is complex, and the exact pathological mechanism of DR needs to be further elucidated to promote new drug research and development against DR. The entire pathological process of DR involves increased oxidative stress (microvascular dysfunction, mitochondrial dysfunction) and chronic inflammation (inflammatory infiltration, cell necrosis) and impairment of the renin-angiotensin system (microcirculation dysregulation). This review aims to summarize the pathological mechanisms underlying the development of DR to improve clinical diagnosis and effective treatment of DR.
Keywords: Diabetic Retinopathy, Blindness, Pathogen-Induced Protease, P69, Pathology, Molecular, Adult, Humans, Middle Aged, Retinal Diseases, Inflammation, Retina, Atrophy, Diabetes Mellitus
Background
DR is an ophthalmic disease clinically characterized by persistent retinal lesions caused by glucose metabolism dysfunction. As a severe symptom in DM, DR presents with blurred vision, decreased vision, and blindness [1]. Globally, the incidence and progression of DR have worsened in recent decades, and early diagnosis and effective treatment should be priorities [2]. Although clinical progress has been made in treatment DR, the poor lower fundus inspection rates limit screening of DR. Thus, understanding the pathogenesis of DR is important for expediting earlier treatment of DR to reduce the incidence of vision impairment and blindness [3]. However, the exact pathogenic mechanism of DR is not clearly understood. A growing body of evidence indicates that low-grade inflammation exerts a key role in the pathogenesis and development of DR, involving cytokine infiltration, tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), and monocyte chemotactic protein-1 (MCP-1) [4]. The actions of inflammatory cytokines and vascular endothelial growth factor can synergistically damage the blood–retinal barrier, induce vascular damage and neuroinflammation, promote pathological angiogenesis, and cause diabetic macular edema before development of DR [5]. Additionally, retinal cell types in DR, including Müller glia, astrocytes, microglia, retinal pigment epithelial cells, are activated to release inflammatory mediators, gradually inducing cell apoptosis and vascular damage [6]. Promising treatments targeting inflammatory or oxidative molecules or correlative signaling pathways help to suppress retinal injury and prevent DR progression. The present article reviews the existing literature and summarizes the molecular mechanisms involved in the pathogenesis of DR, and proposes inflammation- and oxidative stress-based treatments for DR.
Retinal Physiological Structure
The retinal tissue structure has highly interconnected functions, and can be subdivided into 10 layers from outside to inside: pigment epithelial cell layer, optic cell layer, outer membrane, outer nuclear layer, outer plexiform layer, inner nuclear layer, middle limiting membrane, ganglion cell layer, nerve fiber layer, and inner boundary membrane [7]. The physical structure and physiological function in each layer are described briefly as follows. (1) The pigment epithelial cell layer is composed of a single layer of dwarf columnar pigment cells, which maintains the metabolism. (2) The optic cell layer includes cone cells and rod cells. Cone cells can distinguish colors, but are only excited when stimulated by strong light. Rods cells, also known as photoreceptors, can accept light stimuli and convert them into electrical energy to release nerve impulses. (3) The outer membrane is a membrane-like structure formed by the interconnection of the tips of the lateral process of radial glial cells, which has the function of sensing light stimulation. (4) The outer nuclear layer consists of the cell bodies of cone cells and rod cells, which can stabilize the nuclear membrane. (5) The outer plexus layer consists of the endophytes of cone cells and rod cells and the dendrites of bipolar cells. (6) The inner nuclear layer is composed of bipolar cells, horizontal cells, non-spiky cells and radial glial cells. (7) The middle limiting membrane is composed of axons of bipolar cells, dendrites of non-elongated cells, and ganglion cells. (8) The ganglion cell layer is related to conduction function. (9) The nerve fiber layer is made up of axons of ganglion cells that can transmit commands from the brain. (10) The inner boundary membrane is a thin film between the inner surface of the retina and the surface of the vitreous body. The physical structure characteristics of the retina are highlighted in Figure 1.
Retinal tissue has a fine and complex structure, and damage to each layer of the structure can cause visual impairment and other symptoms, including retinal detachment, retinal periphlebitis, and maculopathy [8]. Retinal lesions, hemorrhages, and exudates are the critical pathological symptoms of DR [9]. Non-proliferative DR refers to the earliest condition of DR and is commonly asymptomatic. Clinically, the severity of DR is determined by using a semi-quantitative scoring system on the basis of retinal lesions [10]. Proliferative DR is characterized by retinal neovascularization, and it can lead to irreversible vision loss and impairment over time [11].
Blood–Retinal Barrier
The blood–retinal barrier (BRB) is composed of inner and outer components in which the inner BRB consists of tight junctions within retinal capillary endothelial cells, and the outer BRB is formed of tight junctions within retinal pigment epithelial cells. The BRB is important for maintaining normal visual function and eye tissue in specific locations [12]. The structural integrity of the BRB plays the pivotal role in maintenance of retinal function and microenvironment via modulation of transcellular and paracellular transport actions. Notably, BRB damage can cause formation of edema, a hallmark characteristic of retinal disorders [13]. The typical retinal diseases, such as DR and age-related macular degeneration (AMD), are directly related to abnormal changes of the BRB [14].
Pathological Changes of the BRB in DR
CHANGES OF BRB AND RETINAL HOMEOSTASIS IN DR:
In DR, high blood glucose levels caused by DM can disrupt cell–cell communication and then trigger impairment of retinal homeostasis. Hyperglycemia changes the activity of connexin genes and interrelated intercellular communication in retinal vascular cells [17]. Hyperglycemia causes cell death, damages vascular permeability, and affects retinal homeostasis and interactions between pericytes, endothelial cells, and Müller cells, which characterize the underlying pathogenesis of DR [18]. A previous study using an animal model of DR found reduced retinal blood flow, similar to that observed in the early stages of DM, induced by hyperglycemia, including breakdown of BRB, emergence of microhemorrhages, and development of ischemia [19]. It was reported that endogenous vascular endothelial growth factor (VEGF) can induce retinal leukostasis and breakdown of the BRB, and VEGF164 is a potential proinflammatory marker in early DR [20]. Platelet deposition in the vasculature of people with DR is secondary to endothelial cell death caused by leukocytes, subsequently affecting the BRB. Thus, platelet activation and its activated cytokines may be potential biomarkers of DR [21].
SELECTIVE LOSS OF PERICYTES: Selective pericyte loss is a pathological hallmark of early DR, and loss of pericytes may initiate disruption of the BRB in DM [22]. The structure of the BRB is mainly formed through tightly interconnected capillary endothelial cells covered with pericytes. The platelet-derived growth factor (PDGF) signaling pathway is required for construction of the BRB via targeting recruitment of pericytes to proliferating retinal vessels. Altered pericyte adhesion to retinal vessels, based on BRB impairment, may be responsible for the underlying pathogenesis of DR [23]. Therefore, targeting inhibition of loss of pericytes may be a potential treatment of DR.
RETINAL ENDOTHELIAL CELL DEATH: Recruitment of numerous leukocytes to the DR-related vasculature causes endothelial cell impairment or death and subsequent BRB breakdown [24]. An in vivo study found that leukocyte subsets induce retinal endothelial cell death as a leading cause of BRB damage in early DR, suggesting the role of natural killer T cells in modulating the pathophysiology of DR [25]. When leukostasis occurs, vasodilatation and inflammation can induce early BRB breakdown, eventually leading to retinal endothelial cell damage and death [26].
Molecular Mechanisms in DR
OXIDATIVE STRESS:
Oxidative stress is one of adverse outcomes in metabolic abnormalities mediated by high blood glucose levels, basically comprising activation of the polyol pathway and hexosamine pathway, over-expression of protein kinase C (PKC), and deposition of advanced glycation end-product (AGE). Oxidative stress has been identified as a key contributor to the pathological mechanism of DR [27]. Excessive production of reactive oxygen species (ROS) can lead to mitochondrial impairment, lipid peroxidation, cell apoptosis, inflammatory stress, and retinal dysfunction [28].
PKC PATHWAY:
PKC refers to a family of phospholipid-dependent serine/threonine protein kinases that are mainly expressed in the retina, kidney, and heart tissues. PKC activation is related to cellular events, including proliferation, differentiation, and apoptosis [29]. Other studies have indicated that activation of PKC can exert an important role in the development of DR, as shown in an in vitro DR model [30]. Furthermore, induction of PKC enhances excessive expression of endothelin, a potent vasoconstrictor, causing retinal impairment through impairing endothelial function in blood vessels [31]. High glucose levels can cause activation of PKC isoforms, increase production of AGE, increase levels of glucose, and activate release of ROS [32]. In addition, an in vivo study found increased PKC expression and activation of the PKC signaling pathway in chemical-induced DR [33], suggesting that the PKC pathway is a potential mechanism in development of DR.
POLYOL PATHWAY:
The polyol pathway is involved in glucose metabolism in the activated stage in DM, affecting stabilization between nicotinamide adenine dinucleotide (NADH) and NAD+. Dysregulation of the polyol pathway can cause oxidative injury to DNA and proteins, subsequently causing DM and its associated complications, including DR [34]. Human endothelial cells in retinal vessels participate in the process of aldose reductase. Some promoter region polymorphisms in the aldose reductase gene are involved in susceptibility to and progression of DR [35]. It is reported that superabundant expression of aldose reductase may be a molecular mechanism of human DR through regulating the polyol (sorbitol) pathway for glucose metabolism [36]. Additionally, the specific polymorphisms in polyol pathway genes of ALR2 rs759853 and SDH rs2055858 are found to be associated with different levels of risk of DR [37]. The underlying mechanism by which the polyol pathway is associated with the pathogenesis of DR may involve modulating oxidative stress, inflammatory reactions, and homeostasis [38].
HEXOSAMINE PATHWAY:
The hexosamine pathway is associated with the protein-functional maturation and cellular communications involved in regulating age-related proteotoxicity [39]. The hexosamine biosynthetic pathway mediates nutrient utilization and cellular stress response via glucose metabolism [40]. Interestingly, the potential role of the hexosamine biosynthetic pathway may contribute to the occurrence and development of metabolic diseases, including DM [41]. DR is one of the most severe microvascular complications caused by high blood glucose levels via the main molecular pathways, such as the hexosamine pathway [42]. Furthermore, most stages in DR pathogenesis closely involve excessive ROS release, inflammatory stress, and cell death [43].
INFLAMMATORY STRESS:
Inflammation plays a crucial role in the pathogenesis of DM and in the metabolic symptoms and subsequent development of DM-related complications, such as DR [44]. Microvascular lesions are a DR-associated feature, and chronic inflammation contributes to the molecular pathogenesis of DR [45]. VEGF is highly activated through induction of hyperglycemic changes and hypoxia stress in the tissues. Other proinflammatory molecules are mediated by diversified cytokines, including TNF-α and interleukin-6 (IL-6) and other growth factors inducing vasopermeability and proliferative DR. There is evidence of inflammation and angiogenesis crosstalk in DR [46]. A growing body of evidence suggests that DR is a low-level inflammatory disease caused by hyperglycemia, and its main features are oxidative stress, cell apoptosis, and neovascularization. Toll-like receptors are a functional family of pattern-recognition receptors that contribute to development of inflammatory stress [47]. Thus, anti-inflammatory strategies may be promising treatments for clinical DR.
RENIN-ANGIOTENSIN SYSTEM:
It is clinically observed that hypertension increases the risk of developing DR, and hypertension inhibitors can be used to treat retinopathy. The renin-angiotensin system (RAS) can be activated by prolonged high blood glucose levels, characterized by increased angiotensin II (AII) expression in proliferative DR [48]. Therefore, the use of AII Type 1 (AT1) inhibitors seems to be an effectively therapeutic option to clinically manage DR [49]. Additionally, Ang II, which is a known bioactive ingredient of the RAS, is significantly elevated in DR patients, in which Ang II mediates neurovascular impairment, contributing to the development of DR. These ongoing events reveal that the Ang II pathway in DR may an early mechanism involved in blurred vision in people with DR [50]. Other evidence suggests that actions of AGEs and RAS affect diverse pathological processes in DR, characterized by crosstalk between the AGEs and RAS molecular pathways [51]. Taken together, the above evidence suggests that pharmacologically targeting inhibition of RAS or related pathways may be a promising regimen for clinical treatment of DR [52].
Conclusions
As a multifactorial ophthalmic disease, the pathological mechanisms of DR are involved in a variety of molecular signaling pathways, which have not yet been sufficiently defined. The underlying mechanisms are strongly associated with hyperglycemia-induced chronic inflammation, oxidative stress, and retinal microvascular damage. Figure 2 summarizes the integrative review findings of the present article, showing that modern medical treatment of DR mainly includes lowering blood glucose levels, anti-VEGF and anti-oxidative stress actions, laser therapy, hormonotherapy, and surgical treatment. Interestingly, Chinese medicine is an important option for DR prevention and treatment, but further research is needed to screen out the active components with pharmacological efficacy against DR from complex Chinese herbs. A limitation of the present review is that there is insufficient literature on precise details of the pathological mechanisms and pathways involved in DR. Researchers need to continue to monitor DR research results and provide updated reviews.
Figures
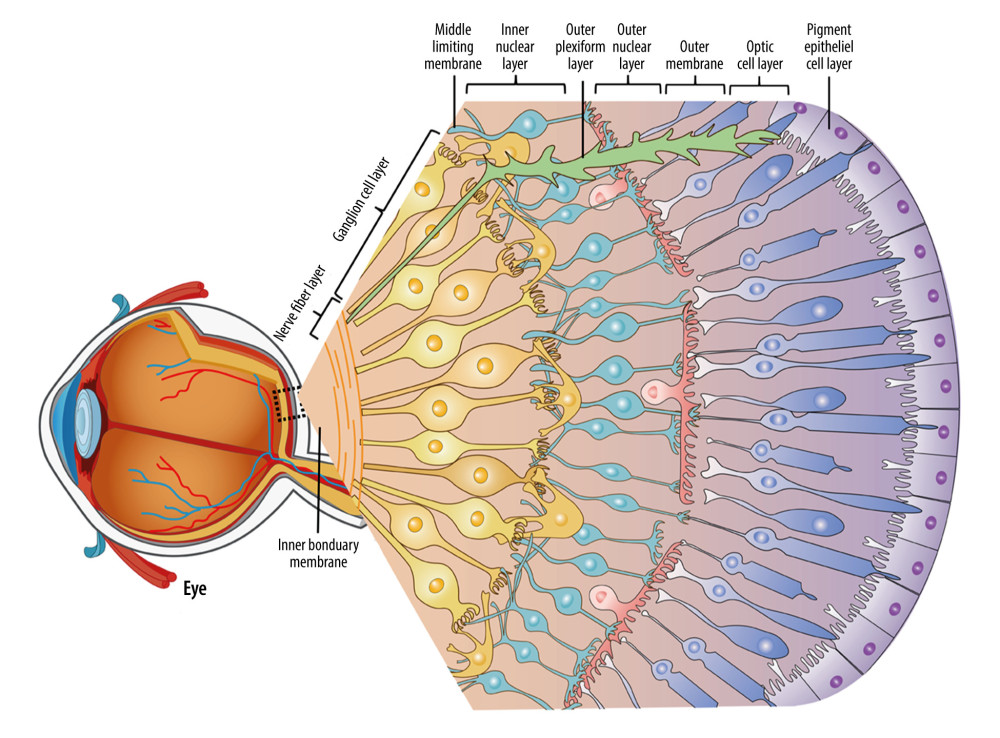 Figure 1. Characterization of retinal physiological structure. The retina is composed of 10 physiological layers, each with its own function.
Figure 1. Characterization of retinal physiological structure. The retina is composed of 10 physiological layers, each with its own function. 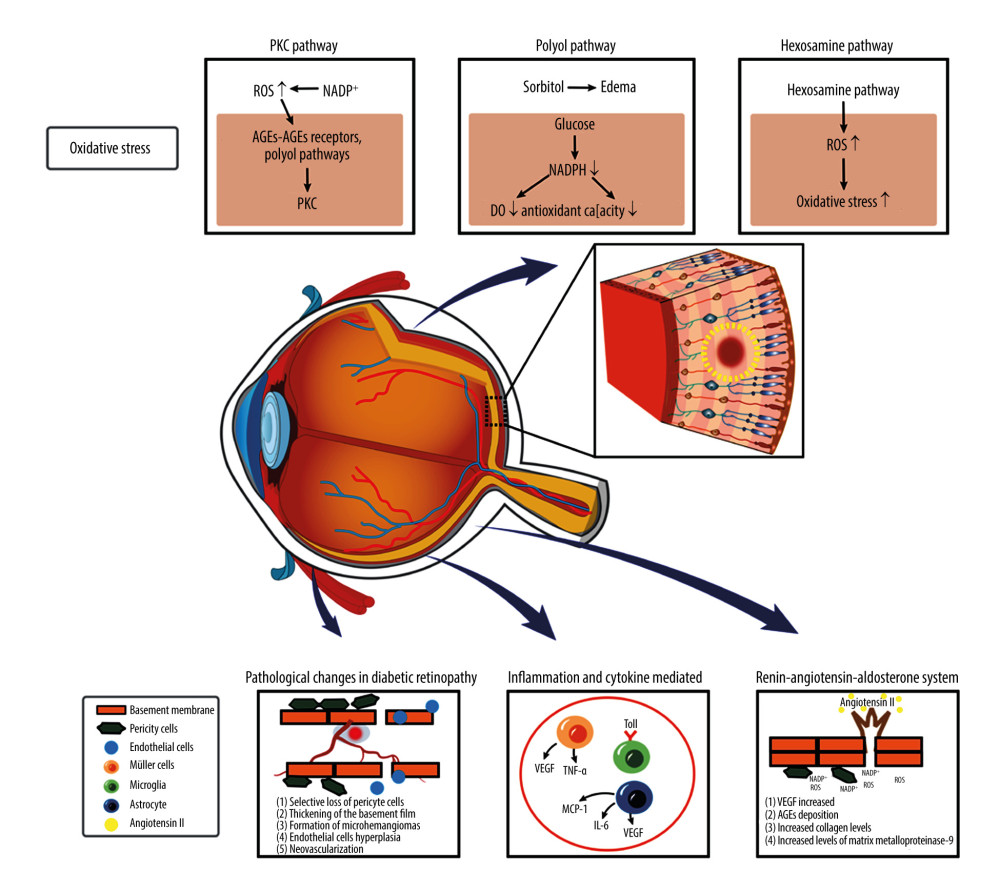 Figure 2. Schematic diagram of pathological mechanism in DR. The main molecular mechanisms involved in DR pathogenesis are the PKC pathway, polyol pathway, and hexosamine pathway. The occurrence and development of DR can involve increased inflammatory/oxidative stress and impairment of the renin-angiotensin system, respectively.
Figure 2. Schematic diagram of pathological mechanism in DR. The main molecular mechanisms involved in DR pathogenesis are the PKC pathway, polyol pathway, and hexosamine pathway. The occurrence and development of DR can involve increased inflammatory/oxidative stress and impairment of the renin-angiotensin system, respectively. References
1. Antonetti DA, Klein R, Gardner TW, Diabetic retinopathy: N Engl J Med, 2012; 366(13); 1227-39
2. Sabanayagam C, Banu R, Chee ML, Incidence and progression of diabetic retinopathy: A systematic review: Lancet Diabetes Endocrinol, 2019; 7(2); 140-49
3. Lin KY, Hsih WH, Lin YB, Update in the epidemiology, risk factors, screening, and treatment of diabetic retinopathy: J Diabetes Investig, 2021; 12(8); 1322-25
4. Forrester JV, Kuffova L, Delibegovic M, The role of inflammation in diabetic retinopathy: Front Immunol, 2020; 11; 583687
5. Kowluru RA, Cross Talks between oxidative stress, inflammation and epigenetics in diabetic retinopathy: Cells, 2023; 12(2); 300
6. Tang L, Xu GT, Zhang JF, Inflammation in diabetic retinopathy: Possible roles in pathogenesis and potential implications for therapy: Neural Regen Res, 2023; 18(5); 976-82
7. Hoon M, Okawa H, Della Santina L, Wong RO, Functional architecture of the retina: development and disease: Prog Retin Eye Res, 2014; 42; 44-44
8. Wert KJ, Lin JH, Tsang SH, General pathophysiology in retinal degeneration: Dev Ophthalmol, 2014; 53; 33-43
9. Kar SS, Maity SP, Automatic detection of retinal lesions for screening of diabetic retinopathy: IEEE Trans Biomed Eng, 2018; 65(3); 608-18
10. Sivaprasad S, Pearce E, The unmet need for better risk stratification of non-proliferative diabetic retinopathy: Diabet Med, 2019; 36(4); 424-33
11. Vaz-Pereira S, Zarranz-Ventura J, Sim DA, Optical coherence tomography features of active and inactive retinal neovascularization in proliferative diabetic retinopathy: Retina, 2016; 36(6); 1132-42
12. Cunha-Vaz J, Bernardes R, Lobo C, Blood–retinal barrier: Eur J Ophthalmol, 2011; 21; 3-9
13. O’Leary F, Campbell M, The blood–retina barrier in health and disease: FEBS J, 2023; 290(4); 878-91
14. Rudraraju M, Narayanan SP, Somanath PR, Regulation of blood–retinal barrier cell-junctions in diabetic retinopathy: Pharmacol Res, 2020; 161; 105115
15. Zhang C, Wang H, Nie J, Wang F, Protective factors in diabetic retinopathy: Focus on blood–retina barrier: Discov Med, 2014; 18(98); 105-12
16. Simó R, Villarroel M, Corraliza L, Hernández C, Garcia-Ramírez M, The retinal pigment epithelium: something more than a constituent of the blood–retina barrier – implications for the pathogenesis of diabetic retinopathy: J Biomed Biotechnol, 2010; 2010; 190724
17. Klaassen I, Van Noorden CJ, Schlingemann RO, Molecular basis of the inner blood–retina barrier and its breakdown in diabetic macular edema and other pathological conditions: Prog Retin Eye Res, 2013; 34; 19-48
18. Roy S, Kim D, Lim R, Cell-cell communication in diabetic retinopathy: Vision Res, 2017; 139; 115-22
19. Harris NR, Leskova W, Kaur G, Blood flow distribution and the endothelial surface layer in the diabetic retina: Biorheology, 2019; 56(2–3); 181-89
20. Yi QY, Deng G, Chen N, Metformin inhibits development of diabetic retinopathy through inducing alternative splicing of VEGF-A: Am J Transl Res, 2016; 8(9); 3947-54
21. Kucuk I, Tural E, Doğantekin B, Evaluation of platelet indices and pro-inflammatory cytokines in type 2 diabetic patients with retinopathy: Rev Assoc Med Bras (1992), 2022; 68(11); 1537-41
22. Rangasamy S, Monickaraj F, Legendre C, Transcriptomics analysis of pericytes from retinas of diabetic animals reveals novel genes and molecular pathways relevant to blood–retina barrier alterations in diabetic retinopathy: Exp Eye Res, 2020; 195; 108043
23. Park DY, Lee J, Kim J, Plastic roles of pericytes in the blood–retina barrier: Nat Commun, 2017; 8; 15296
24. Joy SS, Siddiqui K, Molecular and pathophysiological mechanisms of diabetic retinopathy in relation to adhesion molecules: Curr Diabetes Rev, 2019; 15(5); 363-71
25. Suvas P, Liu L, Rao P, Systemic alterations in leukocyte subsets and the protective role of NKT cells in the mouse model of diabetic retinopathy: Exp Eye Res, 2020; 200; 108203
26. Herdade AS, Silva IM, Calado Â, Effects of diabetes on microcirculation and leukostasis in retinal and non-ocular tissues: Implications for diabetic retinopathy: Biomolecules, 2020; 10(11); 1583
27. Kang Q, Yang C, Oxidative stress and diabetic retinopathy: Molecular mechanisms, pathogenetic role and therapeutic implications: Redox Biol, 2020; 37; 101799
28. Volpe CMO, Villar-Delfino PH, Dos Anjos PMF, Nogueira-Machado JA, Cellular death, reactive oxygen species (ROS) and diabetic complications: Cell Death Dis, 2018; 9(2); 119
29. Wu QW, Kapfhammer JP, Serine/threonine kinase 17b (STK17B) signalling regulates Purkinje cell dendritic development and is altered in multiple spinocerebellar ataxias: Eur J Neurosci, 2021; 54(7); 6673-84
30. Sarikaya M, Yazihan N, Daş Evcimen N, Relationship between aldose reductase enzyme and the signaling pathway of protein kinase C in an in vitro diabetic retinopathy model: Can J Physiol Pharmacol, 2020; 98(4); 243-51
31. Kida T, Oku H, Horie T, Protein kinase C-mediated insulin receptor phosphorylation in diabetic rat retina: Graefes Arch Clin Exp Ophthalmol, 2019; 257(7); 1427-34
32. Qin J, Peng Z, Yuan Q, AKF-PD alleviates diabetic nephropathy via blocking the RAGE/AGEs/NOX and PKC/NOX Pathways: Sci Rep, 2019; 9(1); 4407
33. Zhang M, Zhou M, Cai X, VEGF promotes diabetic retinopathy by upregulating the PKC/ET/NF-κB/ICAM-1 signaling pathway: Eur J Histochem, 2022; 66(4); 3522
34. Garg SS, Gupta J, Polyol pathway and redox balance in diabetes: Pharmacol Res, 2022; 182; 106326
35. Abu-Hassan DW, Al-Bdour MD, Saleh I, The relationship between aldose reductase gene C106T polymorphism and the severity of retinopathy in Type 2 diabetic patients: A case-control study: J Res Med Sci, 2021; 26; 2
36. Niimi N, Yako H, Takaku S, Aldose reductase and the polyol pathway in schwann cells: Old and new problems: Int J Mol Sci, 2021; 22(3); 1031
37. Li W, Chen S, Mei Z, Polymorphisms in sorbitol-aldose reductase (polyol) pathway genes and their influence on risk of diabetic retinopathy among Han Chinese: Med Sci Monit, 2019; 25; 7073-78
38. Obrosova IG, Kador PF, Aldose reductase/polyol inhibitors for diabetic retinopathy: Curr Pharm Biotechnol, 2011; 12(3); 373-85
39. Denzel MS, Antebi A, Hexosamine pathway and (ER) protein quality control: Curr Opin Cell Biol, 2015; 33; 14-18
40. Lam C, Low JY, Tran PT, Wang H, The hexosamine biosynthetic pathway and cancer: Current knowledge and future therapeutic strategies: Cancer Lett, 2021; 503; 11-18
41. Cairns M, Joseph D, Essop MF, The dual role of the hexosamine biosynthetic pathway in cardiac physiology and pathophysiology: Front Endocrinol (Lausanne), 2022; 13; 984342
42. Wu MY, Yiang GT, Lai TT, Li CJ, The oxidative stress and mitochondrial dysfunction during the pathogenesis of diabetic retinopathy: Oxid Med Cell Longev, 2018; 2018; 3420187
43. Kowluru RA, Kowluru A, Mishra M, Kumar B, Oxidative stress and epigenetic modifications in the pathogenesis of diabetic retinopathy: Prog Retin Eye Res, 2015; 48; 40-61
44. Forrester JV, Kuffova L, Delibegovic M, The role of inflammation in diabetic retinopathy: Front Immunol, 2020; 11; 583687
45. Spencer BG, Estevez JJ, Liu E, Pericytes, inflammation, and diabetic retinopathy: Inflammopharmacology, 2020; 28(3); 697-709
46. Capitão M, Soares R, Angiogenesis and inflammation crosstalk in diabetic retinopathy: J Cell Biochem, 2016; 117(11); 2443-53
47. Bayan N, Yazdanpanah N, Rezaei N, Role of toll-like receptor 4 in diabetic retinopathy: Pharmacol Res, 2022; 175; 105960
48. Wilkinson-Berka JL, Suphapimol V, Jerome JR, Angiotensin II and aldosterone in retinal vasculopathy and inflammation: Exp Eye Res, 2019; 187; 107766
49. Wang MH, Ibrahim AS, Hsiao G, A novel interaction between soluble epoxide hydrolase and the AT1 receptor in retinal microvascular damage: Prostaglandins Other Lipid Mediat, 2020; 148; 106449
50. Ola MS, Alhomida AS, Ferrario CM, Ahmad S, Role of tissue renin-angiotensin system and the chymase/angiotensin-(1-12) axis in the pathogenesis of diabetic retinopathy: Curr Med Chem, 2017; 24(28); 3104-14
51. Jeganathan VS, The therapeutic implications of renin-angiotensin system blockade in diabetic retinopathy: Curr Pharm Biotechnol, 2011; 12(3); 392-95
52. Miller AG, Zhu T, Wilkinson-Berka JL, The renin-angiotensin system and advanced glycation end-products in diabetic retinopathy: Impacts and synergies: Curr Clin Pharmacol, 2013; 8(4); 285-96
Figures
Figure 1. Characterization of retinal physiological structure. The retina is composed of 10 physiological layers, each with its own function.Figure 2. Schematic diagram of pathological mechanism in DR. The main molecular mechanisms involved in DR pathogenesis are the PKC pathway, polyol pathway, and hexosamine pathway. The occurrence and development of DR can involve increased inflammatory/oxidative stress and impairment of the renin-angiotensin system, respectively. In Press
11 Mar 2024 : Clinical Research
Comparison of Effects of Sugammadex and Neostigmine on Postoperative Neuromuscular Blockade Recovery in Pat...Med Sci Monit In Press; DOI: 10.12659/MSM.942773
12 Mar 2024 : Clinical Research
Comparing Neuromuscular Blockade Measurement Between Upper Arm (TOF Cuff®) and Eyelid (TOF Scan®) Using Miv...Med Sci Monit In Press; DOI: 10.12659/MSM.943630
11 Mar 2024 : Clinical Research
Enhancement of Frozen-Thawed Human Sperm Quality with Zinc as a Cryoprotective AdditiveMed Sci Monit In Press; DOI: 10.12659/MSM.942946
12 Mar 2024 : Database Analysis
Risk Factors of Age-Related Macular Degeneration in a Population-Based Study: Results from SHIP-TREND-1 (St...Med Sci Monit In Press; DOI: 10.12659/MSM.943140
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952