25 May 2023: Clinical Research
Impact of Converting from Immediate-Release Tacrolimus to Envarsus on BK Viremia Incidence in Kidney Transplant Patients with Rapid Metabolism
Graham Towns1ABCDEFG, Gaurav Agarwal1ABCDEFG*, Ashutosh Tamhane1CDE, Clifton Kew1AEDOI: 10.12659/MSM.939748
Med Sci Monit 2023; 29:e939748






Abstract
BACKGROUND: BK infections have been observed more frequently among people who are rapid metabolizers. The tacrolimus c/d ratio identifies rapid metabolizers after transplantation. Envarsus has a lower peak drug level exposure than tacrolimus and is more pronounced in rapid metabolizers. This study hypothesized that less exposure to high tacrolimus levels through use of Envarsus would reduce the incidence of BK infections.
MATERIAL AND METHODS: This study prospectively converted 43 consecutive kidney transplant recipients (identified as rapid metabolizers by c/d ratio of <1) with negative serum BK viral load at month 2 following transplantation from IR tacrolimus to Envarsus. We compared their rates of BK infection with 45 historical well-matched rapid metabolizers who remained on IR tacrolimus. Bk urine and serum PCR were monitored at specified time points up to 12 months following transplantation.
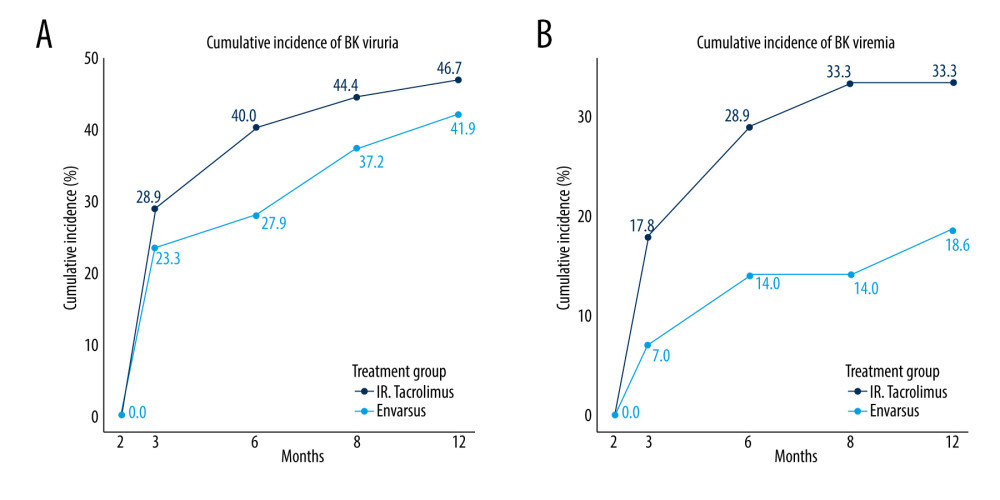
RESULTS: Most patients in the study cohort were deceased donor kidney transplant recipients, mean age 50 years, and predominantly of African American ethnicity. The incidences of BK viremia (18.6% vs 33.3%) and BK viruria (41.9% vs 46.7%) were numerically lower in the Envarsus-converted group as compared to patients remaining on IR tacrolimus at 1 year after transplantation. The cumulative risk ratio for the development of BK viremia for the Envarsus group was 0.53 compared to the IR tacrolimus group.
CONCLUSIONS: The study did not demonstrate a significant reduction in the incidence of BK virus infection in the Envarsus-converted group as compared to the IR tacrolimus group, although there was a numerical reduction. The study likely lacked sufficient statistical powered to detect a difference.
Keywords: Kidney Transplantation, Tacrolimus, BK Virus, Humans, Immunosuppressive Agents, Incidence, transplant recipients, Viremia, Polyomavirus Infections, Tumor Virus Infections
Background
BK virus infection is a well-known cause of graft dysfunction and premature graft loss. Screening has improved the identification of early infections due to their asymptomatic nature and unpredictable replication. The development of BK virus infection after transplantation is largely attributed to reactivation of the virus in the donor allograft. The risk factors are multifactorial and cannot be attributed to individual immunosuppressive agents alone. The degree of immunosuppression was the most consistent risk factor and immunosuppression reduction was the most effective treatment. The rates of BK, viremia, and nephropathy are 40%, 20%, and 1–10%, respectively [1,2]. BKVN (BK virus nephropathy) is strongly and independently associated with poor graft survival, and is associated with a high graft failure rate (>50%). The peak incidence of BK infection occurred in the first year after transplantation.
A significant subset of patients require high tacrolimus doses to achieve the desired therapeutic level. These patients are referred to as rapid metabolizers and express the cyp 450 3a*5 allele. Genetic testing of this allele is not routinely performed in transplant recipients. A concentration/drug dose (c/d) ratio of <1 for tacrolimus has been validated as an indirect method to identify rapid metabolizers [3–7]. Thölking et al [5] grouped renal transplant patients as slow or rapid metabolizers based on their c/d ratio. Rapid metabolizers have a higher incidence of graft dysfunction, calcineurin inhibitor toxicity, and BK nephropathy. The use of the c/d ratio as a marker of cyp 450 3a5 metabolism has been further validated in several studies [3,4,8]. Thölking et al also demonstrated an increased association of BK infection among transplant patients with low c/d ratios compared with those with high c/d ratios.
In a single-center retrospective study [3] of 248 patients designed to investigate the effect of metabolism on renal function, the patients were grouped according to their c/d ratio (<1 for rapid metabolizers and >1.55 for slow metabolizers), and eGFR was assessed at 1, 2, 3, 6, 12, and 24 months. The incidences of BK viremia in the rapid and slow metabolizer groups were 8% and 1%, respectively. BKVN was observed only in the rapid-metabolizer group, with an incidence of 4%. The rapid-metabolizing group also showed significantly higher rates of CNI nephrotoxicity. We hypothesized that these findings were related to overexposure to tacrolimus during the peak hours after tacrolimus intake. A second retrospective study [6] assessed the c/d ratio in kidney transplant recipients, in which 86 BK-positive controls were compared to 86 BK-negative controls. Patients with BK viremia had lower tacrolimus c/d ratios 1, 3, and 6 months after transplantation.
The use of Envarsus instead of intermediate-release tacrolimus (IR-Tac) has been shown to provide equitable drug exposure and efficacy for the prevention of rejection and decreased adverse effects, presumably because of lower peak levels. It has also been shown to achieve therapeutic trough levels at lower overall dosing [9–13].
Rivera et al [14] have shown lower incidence of BK infection compared to transplant patients on Advagraf, the prolonged-release once-daily formulation of tacrolimus. Since high tacrolimus peak levels early after drug intake are a risk factor for BK viremia and Envarsus lowers tacrolimus peak exposure, we investigated whether the conversion of IR-Tac to Envarsus among patients identified as rapid metabolizers based on tacrolimus c/d ratios of <1 would lead to a reduction in the incidence of BK infection.
Material and Methods
IMMUNOSUPPRESSION AND DATA:
All patients were selected if they received standard-of-care immunosuppression with rabbit anti-thymocyte globulin induction (4.5–6 mg/Kg) and were maintained on IR-Tac with a goal trough level of 8–12 ng/mL, mycophenolate mofetil at least 2000 mg daily, and prednisone at month 1. All patients initially received corticosteroids as intravenous-pulse methylprednisolone followed by an oral taper to achieve a maintenance dose of 10 mg/day. After patients were enrolled in the study, maintenance immunosuppression dosing was adjusted per the transplant nephrologist as standard of care.
Standard demographic data for age, race, sex, date of transplantation, type of donor, and calculated PRA were collected via a medical chart review. Data were also collected for BK viruria, BK viremia, BK viral nephropathy, serum creatinine, glomerular filtration rate, urine protein, urine creatinine, tacrolimus trough level, cumulative daily IR-Tac, Envarsus dose, and cumulative MMF dose. The c/d ratio was calculated by dividing the tacrolimus whole-blood trough level by the cumulative daily IR-Tac or Envarsus dose. The study visits were conducted at 2, 3, 6, 9, and 12 weeks after transplantation. BK viruria was defined as any positive urine BK PCR, BK viremia as any positive serum BK PCR, and BK nephropathy was defined as the detection of viral inclusion on biopsy. In this analysis, the mycophenolic acid dose was converted to an equal dose of mycophenolate mofetil for comparison purposes.
The primary efficacy endpoint was a composite of BK infection, including viruria >500 copies/mL or viremia >500 copies/mL.
The Institutional Review Board (IRB) of the University of Alabama approved this study (IRB-150825006), and all study procedures adhered to the guidelines set forth in the Declaration of Helsinki.
STATISTICAL ANALYSIS:
Power analysis was performed with the assumption that the risk of BK viremia was 35% in the IR-Tac group and 10% in the Envarsus conversion group. Forty-three patients were needed in each arm to achieve 80% power, with an alpha of 0.05. Data are presented as counts, percentages, means, or medians. Continuous variables were assessed for normality. Significant differences were identified using the
Results
We compared 43 prospective patients who converted from IR-Tac to Envarsus with 45 historical patients who remained on IR-Tac therapy. Most patients in the cohort were deceased donor kidney transplant recipients (89.7%), with a mean age of 50.19±10.26 years, and predominantly of African American ethnicity (88.64%). The cohorts were comparable at enrollment (2 months after transplantation) except that the tacrolimus dose was higher in the study group (17.28±5.22 mg/day vs 14.27±3.19 mg/day,
The study group was converted from IR-Tac to Envarsus dose at study enrollment (month 2). After conversion, at 3 months after transplantation, there was no difference in the tacrolimus levels (8.80±2.86 mg/dL in the Envarsus group vs 9.59±2.74 mg/dL in the IR-Tac group,
Although there was a numerically lower risk of developing BK viremia during the first year after transplantation in the Envarsus group (18.6% vs 33.3%,
At 3, 6, and 9 months after transplantation, there was also no statistically significant difference in the cumulative incidence of BK viruria or BK viruria (Table 2, Figure 1). Overall, the risk of developing BK viremia (>500 copies/ml) during the first year after transplantation was 26.14% in the entire cohort of rapid metabolizers. Of the 11 patients who developed BK viremia in the first 3 months after transplantation, 3 were in the Envarsus group and 8 were in the IR-Tac group. Moreover, the cumulative incidence of BK viremia in the cohort was 23 (8 patients in the Envarsus group and 15 patients in the IR-Tac group; Table 2). The cumulative risk ratio for development of BK viremia for the Envarsus group was 0.53 compared to the IR-Tac group.
The largest increase in the incidence of BK viremia in both groups occurred by month 3, with a rate of 7% (3/43) in the Envarsus group and 17.8% (8/45) in the IR-Tac group. The second largest increase occurred between months 3 and 6 in the IR-Tac group, from 17.8% to 2.8.9% (13/45). During the same time interval, the Envarsus group only increased from 7% to 14% (6/43). The cumulative incidence at month 9 did not increase in the Envarsus group, but increased by another 4% in the IR-Tac group.
Among the cohort patients, kidney allograft biopsy was performed on 30 out of 43 patients in the Envarsus group and 36 out of 45 patients in the IR-Tac group. The incidence of BKVN at 12 months after transplantation was 3.4% (n=3; 3 in the Envarsus group and none in the IR-Tac group,
No patients in the Envarsus group withdrew from the study or discontinued Envarsus.
There were no death-censored graft failures, although there was 1 death related to CMV infection in the Envarsus group. There was 1 rejection in the Envarsus group related to medication nonadherence and 1 rejection in the IR-Tac group.
Discussion
There is a high incidence of BK viremia in patients requiring higher immunosuppression doses as determined by the tacrolimus c/d ratio <1. We sought to identify patients requiring high tacrolimus dose and converted them to Envarsus to lower the peak exposure and determine its effect on the incidence of BK infection. Overall, our center has a disproportionately high number of African American kidney transplant recipients. In 2019, we performed 250+ transplants, of which approximately 60% were performed in African Americans. As expected, rapid metabolizers were predominantly African Americans (88.64%). There was an overall high incidence of BK (44.4%) and BK (26.1%) in our cohort of rapid metabolizers.
While AUC is the most accurate method for measuring exposure to tacrolimus, the testing is not practical or convenient for patients. Compared to IR-Tac, Envarsus has been shown to have similar AUC and trough levels, with lower peak levels and fewer adverse effects [12]. This has been observed to be more pronounced in rapid metabolizers, who require higher IR-Tac doses to achieve goal trough levels [14]. AUC measurements would not have been available for the control group given the chronology of the study. While proving a lower peak level in the Envarsus group would have been ideal, it was not practical. This study applied a validated screening tool to identify rapid metabolizers, converted them to Envarsus, and applied the proven pharmacokinetic principle of lower peak levels in these 2 groups, who maintained the same target trough levels and statistically similar trough values at all time points.
Screening and enrollment of patients 2 months after transplantation may have allowed more immunosuppression exposure for BK infections to manifest, although patients with positive BK viremia within the first 2 months after transplantation were excluded. Including viremic patients in the study would have confounded the data. In addition, the study group had a significantly higher dose requirement than the control group at the time of conversion to Envarsus in month 2. This, along with a lower tacrolimus c/d ratio, suggests a higher peak exposure in the study group at the time of drug conversion. Approximately half of patients who developed BK viremia in this study did so by month 3 after transplantation; 8 of these 11 patients were in the IR-Tac group and 3 were in the Envarsus group. It appears there is an early signal for BK replication, and conversion to Envarsus appears to halt this progression. It is possible that earlier post-transplant use of Envarsus at month 1 or de-novo would have more effectively prevented the early development of BK viremia. However, identification of rapid metabolizers based on c/d ratio would not be possible at time of transplantation and could be misleading in patients who require high tacrolimus doses at month 1 but no longer require high tacrolimus dosing by month 2. Ideally, rapid metabolizers can be identified at the time of transplantation using genetic testing, and converted to Envarsus early after transplantation. This would result in a cohort with lower peak tacrolimus exposure and possibly lower BK viremia.
We hypothesized that the lower exposure to high peak levels afforded by Envarsus would lead to a lower incidence of BK infection. Figure 1B illustrates the lower absolute and relative cumulative incidence of BK viremia at each time point that was maintained throughout the study. The cumulative incidence of BK viremia among rapid metabolizers converted to Envarsus was less than the incidence of BK viremia among rapid metabolizers who remained on IR-Tac. The cumulative incidence ratio showed that the patients with Envarsus were 47% less likely to develop BK viremia. In this matched cohort, when compared to the patients remaining on IR-Tac, there were no statistically significant differences in the Envarsus conversion group.
Table 2 shows the cumulative incidence of BK viruria and viremia at each time point. The most significant increases in cumulative incidence occurred in the IR-Tac group by month 3 (17.8%) and month 6 (28.9%), with unchanged incidence in the Envarsus group at month 6 (14%) and month 9 (14%). This growing separation between the 2 groups accounts for the trend toward statistical significance at month 9, with a
The power calculations were performed with an expected difference in BK viremia of 25% (35% in the IR-Tac group and 10% in the Envarsus group), but we did not achieve this difference at the end of the study. Although not statistically significant, there was a lower incidence of BK viremia and BK viruria in patients who converted from IR-Tac to Envarsus in the first year after transplantation. A likely explanation is that this study was underpowered to determine such a large difference in BK viremia. At the end of 12 months, we found a difference in BK viremia, with 18.6% in the Envarsus group and 33.3% in the IR-Tac group. To discern a difference with 80% power and a 0.05 significance level, our data indicates that 150 participants would be required for each arm. A larger study cohort is required to demonstrate a statistically significant difference. The cumulative incidence ratio and absolute difference of 15% less BK viremia in the Envarsus group support a clinically meaningful benefit of conversion to Envarsus among rapid metabolizers.
Conclusions
Patients identified as rapid metabolizers with a tacrolimus c/d ratio <1 had a high tacrolimus exposure with IR-Tac. The use of the long-action Envarsus lowered the peak tacrolimus exposure. This study did not demonstrate a significant difference in the incidence of BK infection with conversion to Envarsus from IR-Tac, but the study may have been underpowered. This study revealed a lower cumulative incidence of BK viremia in rapid metabolizers who were converted from IR-Tac to Envarsus.
References
1. Nankivell , BK virus nephropathy: Histological evolution by sequential pathology: Am J Transplant, 2017; 17(8); 2065-77
2. Hirsch HH, Randhawa P, BK polyomavirus in solid organ transplantation: Am J Transplant, 2013; 13(Suppl 4); 179-88
3. Thölking G, Influence of tacrolimus metabolism rate on renal function after solid organ transplantation: World J Transplant, 2017; 7(1); 26-33
4. Thölking G, Siats L, Fortmann C, Tacrolimus concentration/dose ratio is associated with renal function after liver transplantation: Ann Transplant, 2016; 21; 167-79
5. Thölking G, Fortmann C, Koch R, The tacrolimus metabolism rate influences renal function after kidney transplantation: PLoS One, 2014; 9; e111128
6. Thölking G, Schmidt C, Koch R, Influence of tacrolimus metabolism rate on BKV infection after kidney transplantation: Sci Rep, 2016; 6; 32273
7. Hirsch HH, Brennan DC, Drachenberg CB, Polyomavirus-associated nephropathy in renal transplantation: Interdisciplinary analyses and recommendations: Transplantation, 2005; 79; 1277-86
8. Brennan DC, Agha I, Bohl DL, Incidence of BK with tacrolimus versus cyclosporine and impact of preemptive immunosuppression reduction: Am J Transplant, 2005; 5; 582-94
9. Gaber AO, Alloway RR, Bodziak K, Conversion from twice-daily tacrolimus capsules to once-daily extended release tacrolimus (LCPT): A phase 2 trial of stable renal transplant recipients: Transplantation, 2013; 96(2); 191-97
10. Bunnapradist S, Ciechanowski K, West-Thielke P, Conversion from twice-daily tacrolimus to once-daily extended-release tacrolimus (LCPT): The phase III randomized MELT trial: Am J Transplant, 2013; 13(3); 760-69
11. Budde K, Bunnapradist S, Grinyo JM, Novel once-daily extended-release tacrolimus (LCPT) versus twice-daily tacrolimus in de novo kidney transplants: One-year results of phase III, double-blind, randomized trial: Am J Transplant, 2014; 14(12); 2796-806
12. Tremblay S, Nigro V, Weinberg J, A steady-state head-to-head pharmacokinetic comparison of All FK506 (Tacrolimus) formulations (ASTCOFF): An open-label, prospective, randomized, two-arm, three-period crossover study: Am J Transplant, 2017; 17(2); 432-42
13. Fernandez Rivera C, Calvo Rodriguez M, Poveda JL, Bioavailability of once-daily tacrolimus formulations used in clinical practice in the management of de novo kidney transplant recipients: The better study: Clin Transplant, 2022; 36(3); e14550
14. Trofe-Clark J, Brennan D, Bloom R, Results of ASERTAA, a randomized prospective crossover pharmacogenetic study of immediate-release versus extended-release tacrolimus in African American kidney transplant recipients: Am J Kidney Dis, 2017; 71(3); 315-26
Tables
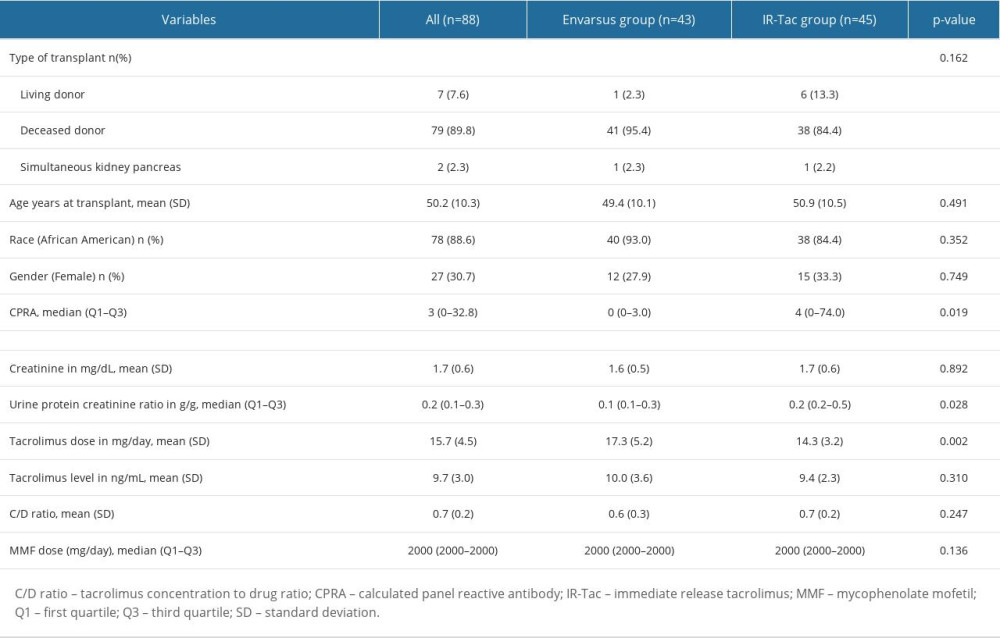 Table 1. Demographic data at baseline and at enrollment at 2 months post-transplant.
Table 1. Demographic data at baseline and at enrollment at 2 months post-transplant.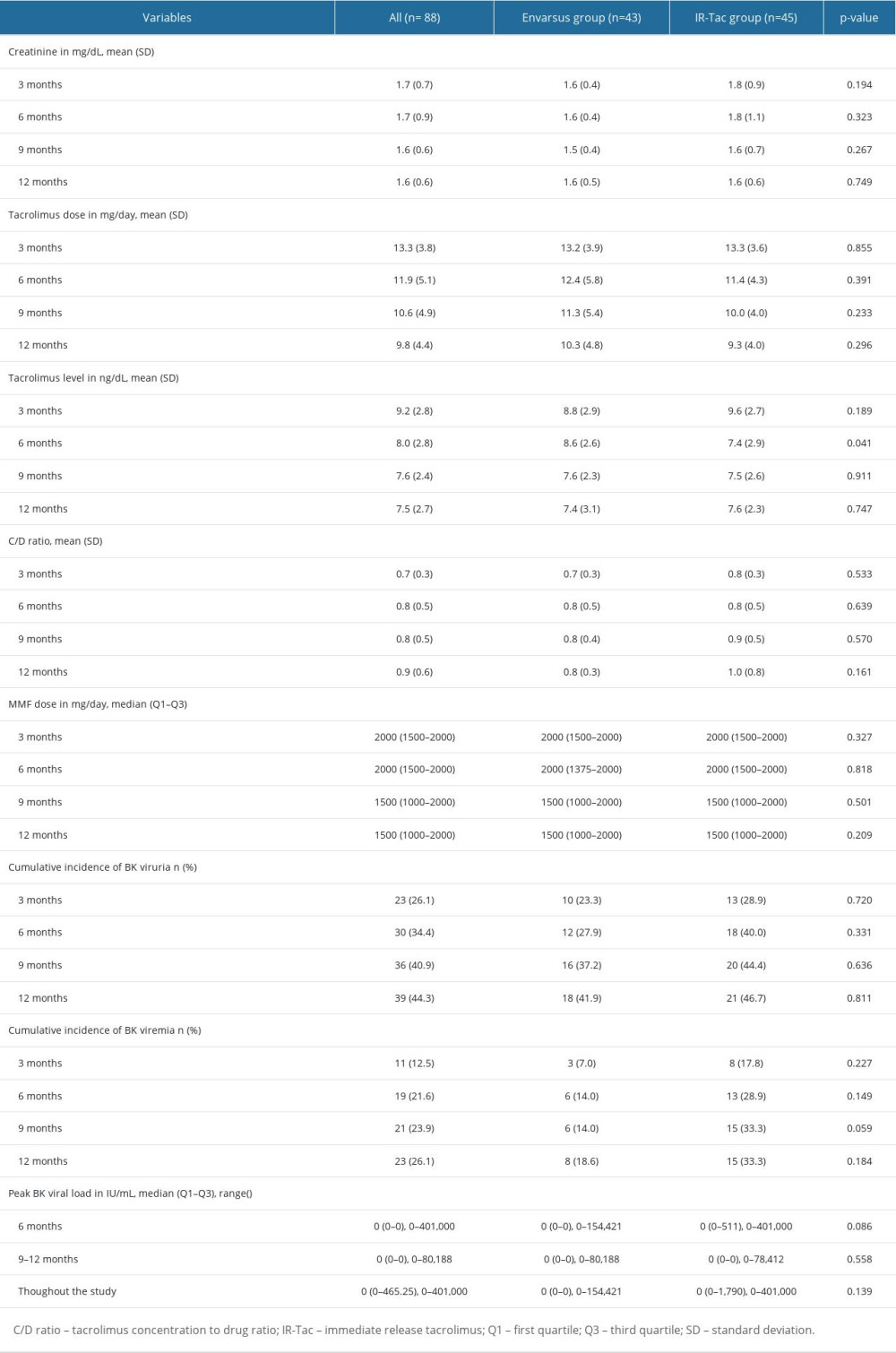 Table 2. Results comparing the groups converted from IR-Tac to Envarsus and those kept on IR-Tac at various time points post-transplant.Table 1. Demographic data at baseline and at enrollment at 2 months post-transplant.Table 2. Results comparing the groups converted from IR-Tac to Envarsus and those kept on IR-Tac at various time points post-transplant.
Table 2. Results comparing the groups converted from IR-Tac to Envarsus and those kept on IR-Tac at various time points post-transplant.Table 1. Demographic data at baseline and at enrollment at 2 months post-transplant.Table 2. Results comparing the groups converted from IR-Tac to Envarsus and those kept on IR-Tac at various time points post-transplant. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387