12 May 2023: Clinical Research
Outcomes of the Indonesian Chronic Disease Management Program (PROLANIS) in Patients with Hypertension During the COVID-19 Pandemic in Rural Areas: A Preliminary Evaluation Study
Sovia SalamahDOI: 10.12659/MSM.939797
Med Sci Monit 2023; 29:e939797






Abstract
BACKGROUND: The Indonesian Chronic Disease Management Program (PROLANIS) is a government program that aims to improve the health outcomes of patients with chronic diseases, including hypertension. This preliminary study aimed to evaluate the impacts of the coronavirus disease 2019 (COVID-19) pandemic on the health outcomes of hypertension patients in rural areas who were enrolled in PROLANIS.
MATERIAL AND METHODS: This study used data from 4 PROLANIS groups in East Java province. The data were collected from participants’ 6-month evaluations at 3 time points: before the COVID-19 pandemic in December 2019 (T0), during the COVID-19 pandemic in June 2020 (T1), and in December 2020 (T2). Evaluated parameters were body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol (TC), low-density lipid (LDL), high-density lipid (HDL), triglyceride (TG), and estimated glomerular filtration rate (eGFR).
RESULTS: There were 91 patients included in the analyses. Compared to T0, BMI, blood pressure, eGFR, and TC had significantly deteriorated at T1, but LDL, HDL, and TG showed no marked changes. At T2, BMI, DBP, and TC were similar to T0. On the other hand, SBP and eGFR did not improve, while HDL significantly deteriorated. Stratified based on age, worsening of DBP, TC, and LDL at T1 and eGFR at T1 and T2 was only observed in those aged 60 years and older.
CONCLUSIONS: This preliminary study showed that the health outcomes of hypertension patients in rural areas who were enrolled in PROLANIS were negatively impacted during the COVID-19 pandemic, with the elderly being the most affected.
Keywords: Chronic Disease, COVID-19, Government Programs, Hypertension, Indonesia, Primary Health Care, Aged, Humans, Middle Aged, Pandemics, COVID-19, Triglycerides, Blood Pressure, Disease Management, Cholesterol, HDL
Background
After coronavirus disease 2019 (COVID-19) cases increased by 13-fold globally in March 2020, the World Health Organization (WHO) classified the outbreak of this disease as a pandemic [1]. Because of the severity of this disease and its modes of transmission, half of the countries around the world limited access to non-urgent essential health services to avoid crowding in health facilities as well as to reallocate limited resources for COVID-19 mitigation [2–5]. The WHO, in their first pulse survey, revealed that up to 90% of countries experienced various levels of disruptions, with low- and middle-income countries (LMIC) experiencing greater disruption due to a longstanding shortage of healthcare providers, lack of medical resources, and challenging socioeconomic landscapes [5–7].
Difficulty in accessing health care and medicine during the COVID-19 pandemic led to worsening symptoms and uncontrolled blood pressure, as reported by a number of studies [2–4]. This consequently compromised their health status and progression of micro- and macrovascular complications, in addition to increasing the risk of more severe COVID-19 illness [1,5–7]. The healthcare settings most disrupted during the COVID-19 pandemic were outpatient service and community-based care [5,8]. This is worrying because these settings provide most essential health services, including health promotion, disease prevention, health maintenance, education, and rehabilitation, to reach the most vulnerable populations [9,10]. Patients with chronic diseases were among these vulnerable populations who suffered a disproportionate impact due to increased barriers to health access during the pandemic [3,4,11]. The disparity is even greater when accounting for other intersecting determinants such as living in rural areas and low economic status [4]. Out of all chronic non-communicable diseases, hypertension management was the most disrupted service, with disruption reported by 53% of surveyed countries [5].
In Indonesia, there is a government program called PROLANIS (PROgram pengeloLAan penyakit kroNIS/Chronic Disease Management Program) that is designated to improve the clinical outcomes and prevent disease complications of patients with chronic diseases, including hypertension. This special program is conducted in the primary healthcare setting and is managed by the Healthcare and Social Security Agency (Badan Penyelenggara Jaminan Sosial Kesehatan, BPJS Kesehatan). A wide array of services are offered by PROLANIS, including medical consultations and prescription of monthly drugs, health education, regular health monitoring that includes biannual laboratory checkup of lipid profiles and kidney function, home visits, reminders through a mobile short message service, as well as club activities [12]. While the concept is very comprehensive, implementation of this program is still suboptimal due to the lack of funding and manpower, as well as inadequate facilities and infrastructure [13].
During the pandemic, the implementation of this program was even less optimal because the healthcare system was overwhelmed [14]. Because of that, one might hypothesize that the health condition of patients with hypertension enrolled in this program would deteriorate. However, to the best of our knowledge, an evaluation study assessing the outcomes of patients with hypertension who were enrolled in PROLANIS during the pandemic has not been done yet. Therefore, this preliminary study aimed to evaluate the impacts of the COVID-19 pandemic on the health outcomes of hypertension patients in rural areas who were enrolled in PROLANIS.
Material and Methods
ETHICAL STATEMENT:
This study was conducted according to the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of the Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia (Approval number: 51/EC/KEPK/FKUA/2022; approval date: 21 February 2022).
STUDY DESIGN AND POPULATION:
This was an observational, retrospective, cohort study using secondary data from 4 PROLANIS groups located at 4 different areas in East Java province, Indonesia. The PROLANIS groups included in this study were from the following areas: Ngajum sub-district in Malang district, Balen sub-district in Bojonegoro district, Soko sub-district in Tuban district, and Sumberbaru sub-district in Jember district.
The study population was hypertension patients who joined the above-mentioned PROLANIS groups and attended the 6-month evaluation before the COVID-19 pandemic, in December 2019 (T0). Participants who quit, died, or did not attend the 6-month evaluation during the COVID-19 pandemic in June 2020 (T1) or in December 2020 (T2) were excluded from the analyses.
EVALUATED PARAMETERS:
Evaluated parameters during the 6-month evaluation were body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), lipid profiles (total cholesterol [TC], low-density lipid [LDL], high-density lipid [HDL], and triglyceride [TG]), and serum creatinine. BMI and BP were measured by the healthcare workers, while evaluation of other parameters was done by designated third-party laboratories. Creatinine serum was converted into estimated glomerular filtration rate (eGFR) using the CKD-EPI equation [15].
STATISTICAL ANALYSES:
Data analyses were performed using IBM SPSS Statistics for Windows version 25.0. (IBM Corp., Armonk, NY, USA) and visual presentation was made using GraphPad Prism version 8.0.0 for Windows (GraphPad Software, San Diego, California, USA). Data distribution was determined using the Kolmogorov-Smirnov test. Data with normal distribution were presented as mean±standard deviation (SD), data with skewed distribution were presented as median [interquartile range (IQR)], and nominal data were presented as frequency. The paired
Results
BASELINE CHARACTERISTICS:
There were 153 patients with hypertension who joined PROLANIS and came in T0, but only 91 of them were included in the final analyses. The mean age of the study participants was 61 years old, and 70 of them were female. More than half of the participants had been diagnosed with hypertension less than 5 years ago. Detailed baseline characteristics of the study participants and the evaluated parameters at T0 are presented in Table 1.
OUTCOMES EVALUATION:
Compared to T0, BMI, blood pressure, eGFR, and TC significantly had deteriorated at T1, whereas LDL, HDL, and TG showed no marked changes. At T2, BMI, DBP, and TC had improved, but SBP and eGFR did not. In contrast to other parameters, HDL was significantly deteriorated only at T2 (Figure 1). Details of the mean±SD or median [IQR] of the evaluated parameters in each time period are presented in Table 2.
Stratified based on age, worsening of DBP, TC, and LDL at T1 was only observed in participants aged 60 years and older. In addition, worsening of eGFR throughout the study period also only occurred in participants aged 60 years and older (Figures 2, 3). Details of the mean±SD or median [IQR] of the evaluated parameters, stratified by age, are presented in Table 3.
Discussion
This study evaluated the outcomes of patients with hypertension who enrolled in PROLANIS as part of health monitoring and complication prevention in rural areas during the COVID-19 pandemic. We found that some parameters deteriorated only in the beginning, some worsened throughout the study period, and some others were not affected by the pandemic. Deterioration in some parameters was observed only in elderly participants.
SBP of our study participants worsened throughout the pandemic (T1 and T2). This finding aligns with population-based studies in the United States showing a significant increase in SBP during the COVID-19 pandemic [16,17]. Another study within a paid digital chronic disease management program also showed that participants’ BP significantly increased during the pandemic, and the proportion of participants with uncontrolled BP also rose [18]. A vast body of literature has identified many potential factors affecting BP during the pandemic, especially as a result of lockdowns and work-from-home policy that results in sedentary lifestyle, leading to an increase in food consumption, including snack and comfort foods rich in salt and carbohydrate, less physical activity, decrease in sleep quality, increased stress and anxiety level, and less adherence to therapy [18,19]. Furthermore, misinformation on COVID-19 that was rampant in Indonesia led to distrust of the medical community and authorities, which may impact medication adherence and further disrupt BP control [20–22].
In addition to BP, BMI was also significantly worsened, but only at T1. In Indonesia, the strict lockdown took place after T1 and then was eased. This is in line with findings from a recent worldwide cohort study, where a significant increase in BMI was observed during COVID-19 lockdown [23]. The rise in BMI indicated a weight gain among participants, which prior studies have linked to various lifestyle changes during the lockdown period of the pandemic, such as less physical activity and stress eating that leads to increased food consumption [19].
For the lipid profiles, TC was the only parameter that significantly worsened, and the worsening occurred only at T1. Prior studies observing lipid profiles during the pandemic yielded various results across the panel, with a study of patients with hypertension reporting a decline only in LDL, while other lipid profiles remained unchanged [17]. One study in healthy adults also observed worsening of most lipid profiles, characterized by increasing TC and LDL, as well as decreasing HDL [24]. This study confirmed worsening of lipid profiles, even though the deteriorating markers varied from other studies. Two factors associated with lifestyle changes that might contribute to this deterioration are heightened stress level due to isolation and fear of contracting COVID-19, which leads to an increase in cortisol level, which releases more lipid to the body, as well as excess intake of saturated fatty acid during lockdown, which has previously been identified to be associated with worsening TC [25,26].
We found that eGFR was worsening throughout the study period. Indeed, hypertension has been found to be closely linked with declining kidney function under a complex mechanism in which hypertension is both the cause and the result of kidney failure [26,27]. Thus, when blood pressure is not well regulated, deterioration of kidney function is to be expected. Dietary changes that include high-sodium intake during the pandemic may also contribute to the decline in this parameter [19].
Stratification based on age revealed worse outcomes in participants 60 years old and older. The elderly are more vulnerable due to the degenerative process affecting vasculature and hemodynamic changes, autonomic dysregulation, and kidney function decline [27]. Prior studies have shown a significant decrease of kidney function with aging, in which filtration rate declines by 10 mL/min, putting them at a disadvantage as compared to the younger age groups, as it increases risk of electrolyte disturbances that can further disrupt BP control [28]. Aging has also been found to be negatively correlated with TC and LDL, which are 2 parameters that were also observed to worsen in older adults in this study [29]. Furthermore, during the peak of the pandemic, older adults tended to experience heightened fear and anxiety as media consistently reported the increased risk of mortality and morbidity in this population when contracting COVID-19, which in turn negatively impacted their overall health status [30–32].
While there are many personal factors that can contribute to worsening outcomes of the evaluated parameters, systemic factors that resulted in disruption of the chronic management program also need to be acknowledged and addressed. To prevent the spread of COVID-19, the Indonesian government decided to temporarily close primary healthcare facilities and halt PROLANIS activities during the COVID-19 lockdown. However, it has been shown in prior studies that closure of primary healthcare facilities and interruption of routine programs compromise patient health [33,34]. In addition, the rising number of COVID-19 cases led to reallocation of primary care providers as well as health facilities to accommodate the need for COVID-19 mitigation and contact tracing [35–37]. Deprioritization of personal protective equipment (PPE) in primary healthcare also increased fear and anxiety for primary healthcare workers, further compromising the strength of the primary healthcare system [14,37,38].
Even after primary healthcare reopened, these reallocation strategies limited services to those that were urgent in nature, while routine services were temporarily halted. In the case of PROLANIS, these efforts translated into the suspension of medical appointments in some areas where conversion to digital visits are not yet available, which is the case in the sites observed in this study. The switch to telemedicine, an innovation also adopted by the Indonesian Ministry of Health, is not as effective in rural areas where connectivity and digital literacy are still an issue [39–41]. Furthermore, low health literacy also contributed to low telemedicine utilization in chronic disease patients in Indonesia [42].
Studies have also identified medication interruption during the pandemic due to the difficulty in obtaining medication [33,42]. Lack of money due to loss of income during the COVID-19 pandemic has been noted as the main cause of this issue. In addition, shortages of medications in the healthcare facilities and closure of the healthcare facilities also contributed to the disruption in obtaining routine medication [33,43].
Now that the end of the COVID-19 pandemic is in sight, implementation of PROLANIS needs to get up to speed. As routine health services are in place and community health outreach continues, it is essential to follow up with patients who dropped out of PROLANIS because patients who missed their appointments during the pandemic are twice as likely to have poor clinical outcomes [44]. This should be a major concern for the healthcare systems, as patients with hypertension with poorly controlled blood pressure are at increased risk of developing or worsening pre-existing cardiovascular, cerebrovascular, and renal diseases, which can lead to high utilization of emergency services that are more costly for the healthcare system [45]. Beyond the ground level implementation, stakeholders in Indonesia should pay more attention to many concerns raised even before the pandemic related to the suboptimal chronic disease management implementation across the board due to overlapping of non-communicable disease (NCD) programs, which leads to overburdened primary healthcare workers [46–48]. Streamlining programs and reporting procedures are a few solutions to this [41]. Ultimately, these efforts will not only benefit PROLANIS participants, but also strengthen the primary healthcare systems in tackling NCDs and give facilities in rural areas an opportunity to thrive and achieve health equity.
There were several limitations in this study. First, this preliminary study was conducted using data from only 91 PROLANIS participants, whereas the latest data in 2016 showed there were 44 999 registered PROLANIS participants in the province where this study was conducted and nationwide there were 260 364 participants [12]. Thus, our study did not entirely reflect the PROLANIS outcome nationwide. Second, as this study used secondary data from the PROLANIS group report, we could not provide data on the list of medications, medication adherence, history of smoking, or daily food intake of the study participants. Data about health service utilization before and during the COVID-19 pandemic were also unavailable. Third, although sex is known to play an important role in hypertension and its complications [49], we did not evaluate the trend differences between males and females because of the low frequency of males included in this study. Fourth, this study only evaluates outcomes until December 2020 to avoid more study participants being excluded in the final analyses. However, the outcome might be different in mid-2021, when Indonesia became the epicentrum of the COVID-19 pandemic in Asia due to the Delta variant outbreak [50].
Conclusions
This is the first study to evaluate the impact of the COVID-19 pandemic on PROLANIS outcomes of patients with hypertension in Indonesia. This preliminary study showed that the health outcomes of hypertension patients in rural areas who were enrolled in PROLANIS were negatively impacted during the COVID-19 pandemic, with the elderly being most affected. These findings highlight the importance of restarting the PROLANIS program and strengthening the role of primary care in health promotion and disease prevention. A nationwide evaluation study is needed to scrutinize the magnitude of the impact of the COVID-19 pandemic on the health outcome of hypertension patients enrolled in PROLANIS.
Figures
![Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS)Data are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). The paired t test was used for normally distributed data and non-parametric Wilcoxon signed-rank test was used for skewed data. * P value <0.05 was considered statistically significant.](https://jours.isi-science.com/imageXml.php?i=medscimonit-29-e939797-g001.jpg&idArt=939797&w=1000) Figure 1. Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS)Data are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). The paired t test was used for normally distributed data and non-parametric Wilcoxon signed-rank test was used for skewed data. * P value <0.05 was considered statistically significant.
Figure 1. Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS)Data are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). The paired t test was used for normally distributed data and non-parametric Wilcoxon signed-rank test was used for skewed data. * P value <0.05 was considered statistically significant. ![Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS) in study participants aged below 60 years oldData are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). Paired t test was used for normally distributed data and non-parametric Wilcoxon signed-rank test was used for skewed data. * P<0.05 was considered statistically significant.](https://jours.isi-science.com/imageXml.php?i=medscimonit-29-e939797-g002.jpg&idArt=939797&w=1000) Figure 2. Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS) in study participants aged below 60 years oldData are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). Paired t test was used for normally distributed data and non-parametric Wilcoxon signed-rank test was used for skewed data. * P<0.05 was considered statistically significant.
Figure 2. Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS) in study participants aged below 60 years oldData are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). Paired t test was used for normally distributed data and non-parametric Wilcoxon signed-rank test was used for skewed data. * P<0.05 was considered statistically significant. ![Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS) in study participants aged 60 years old and olderData are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). The paired t test was used for normally distributed data and the non-parametric Wilcoxon signed-rank test was used for skewed data. * P<0.05 was considered statistically significant.](https://jours.isi-science.com/imageXml.php?i=medscimonit-29-e939797-g003.jpg&idArt=939797&w=1000) Figure 3. Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS) in study participants aged 60 years old and olderData are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). The paired t test was used for normally distributed data and the non-parametric Wilcoxon signed-rank test was used for skewed data. * P<0.05 was considered statistically significant.
Figure 3. Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS) in study participants aged 60 years old and olderData are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). The paired t test was used for normally distributed data and the non-parametric Wilcoxon signed-rank test was used for skewed data. * P<0.05 was considered statistically significant. References
1. Cucinotta D, Vanelli M, WHO declares COVID-19 a pandemic: Acta Biomed, 2020; 91(1); 157-60
2. Rodriguez GM, Ferguson JM, Kurian A, The impact of COVID-19 on patients with cancer: A national study of patient experiences: Am J Clin Oncol, 2021; 44(11); 580-87
3. Gadsden T, Downey LE, Vilas VDR, Peiris D, Jan S, The impact of COVID-19 on essential health service provision for noncommunicable diseases in the South-East Asia region: A systematic review: Lancet Reg Health Southeast Asia, 2022; 1; 100010
4. Singh K, Kondal D, Mohan S, Health, psychosocial, and economic impacts of the COVID-19 pandemic on people with chronic conditions in India: A mixed methods study: BMC Public Health, 2021; 21(1); 685
5. World Health Organization: Pulse survey on continuity of essential health services during the COVID-19 pandemic: Interim report August 27, 2020 [updated 27 August 2020; cited 13 October 2022. Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-EHS_continuity-survey-2020=1
6. Bong CL, Brasher C, Chikumba E, The COVID-19 pandemic: Effects on low- and middle-income countries: Anesth Analg, 2020; 131(1); 86-92
7. Muzammil S, Lopes G, Lack of primary health care services in developing countries during pandemic: An urgent reminder!: J Fam Med Dis Prev, 2021; 7; 138
8. Sacks E, Schleiff M, Were M, Communities, universal health coverage and primary health care: Bull World Health Organ, 2020; 98(11); 773-80
9. van Weel C, Kidd MR, Why strengthening primary health care is essential to achieving universal health coverage: CMAJ, 2018; 190(15); E463-E66
10. Binagwaho A, Adhanom Ghebreyesus T, Primary healthcare is cornerstone of universal health coverage: BMJ, 2019; 365; l2391
11. Singh K, Xin Y, Xiao Y, Impact of the COVID-19 pandemic on chronic disease care in India, China, Hong Kong, Korea, and Vietnam: Asia Pac J Public Health, 2022; 34(4); 392-400
12. Khoe LC, Wangge G, Soewondo P, The implementation of community-based diabetes and hypertension management care program in Indonesia: PLoS One, 2020; 15(1); e0227806
13. Rachmawati S, Prihhastuti-Puspitasari H, Zairina E, The implementation of a chronic disease management program (Prolanis) in Indonesia: A literature review: J Basic Clin Physiol Pharmacol, 2019; 30(6); jbcpp-2019-0350
14. Mahendradhata Y, Andayani N, Hasri ET, The capacity of the Indonesian healthcare system to respond to COVID-19: Front Public Health, 2021; 9; 649819
15. Levey AS, Stevens LA, Schmid CH, A new equation to estimate glomerular filtration rate: Ann Intern Med, 2009; 150(9); 604-12
16. Laffin LJ, Kaufman HW, Chen Z, Rise in blood pressure observed among US adults during the COVID-19 pandemic: Circulation, 2022; 145(3); 235-37
17. Goitia J, Patel S, Chen A, The impact of the COVID-19 pandemic on management of chronic cardiovascular disease: J Am Coll Cardiol, 2022; 79(9); 1135
18. Shah NP, Clare RM, Chiswell K, Trends of blood pressure control in the U.S. during the COVID-19 pandemic: Am Heart J, 2022; 247; 15-23
19. Kreutz R, Dobrowolski P, Prejbisz A, Lifestyle, psychological, socioeconomic and environmental factors and their impact on hypertension during the coronavirus disease 2019 pandemic: J Hypertens, 2021; 39(6); 1077-89
20. Bogart LM, Ojikutu BO, Tyagi K, COVID-19 related medical mistrust, health impacts, and potential vaccine hesitancy among Black Americans living with HIV: J Acquir Immune Defic Syndr, 2021; 86(2); 200-7
21. Tejamaya M, Widanarko B, Erwandi D, Risk perception of COVID-19 in Indonesia during the first stage of the pandemic: Front Public Health, 2021; 9; 731459
22. Kim HK, Ahn J, Atkinson L, Kahlor LA, Effects of COVID-19 misinformation on information seeking, avoidance, and processing: A multicountry comparative study: Sci Commun, 2020; 42(5); 586-615
23. Urzeala C, Duclos M, Chris Ugbolue U, COVID-19 lockdown consequences on body mass index and perceived fragility related to physical activity: A worldwide cohort study: Health Expect, 2022; 25(2); 522-31
24. Ramirez Manent JI, Altisench Jane B, Sanchis Cortes P, Impact of COVID-19 lockdown on anthropometric variables, blood pressure, and glucose and lipid profile in healthy adults: A before and after pandemic lockdown longitudinal study: Nutrients, 2022; 14(6); 1237
25. Hooper L, Martin N, Abdelhamid A, Davey Smith G, Reduction in saturated fat intake for cardiovascular disease: Cochrane Database Syst Rev, 2015(6); CD011737
26. de Guia RM, Rose AJ, Herzig S, Glucocorticoid hormones and energy homeostasis: Horm Mol Biol Clin Investig, 2014; 19(2); 117-28
27. Oliveros E, Patel H, Kyung S, Hypertension in older adults: Assessment, management, and challenges: Clin Cardiol, 2020; 43(2); 99-107
28. Mohamadi M, Goodarzi A, Aryannejad A, Geriatric challenges in the new coronavirus disease-19 (COVID-19) pandemic: A systematic review: Med J Islam Repub Iran, 2020; 34; 123
29. Feng L, Nian S, Tong Z, Age-related trends in lipid levels: A large-scale cross-sectional study of the general Chinese population: BMJ Open, 2020; 10(3); e034226
30. Mueller AL, McNamara MS, Sinclair DA, Why does COVID-19 disproportionately affect older people?: Aging (Albany NY), 2020; 12(10); 9959-81
31. Agrawal S, Drozdz M, Makuch S, The assessment of fear of COVID-19 among the elderly population: A cross-sectional study: J Clin Med, 2021; 10(23); 5537
32. D’Cruz M, Banerjee D, ‘An invisible human rights crisis’: The marginalization of older adults during the COVID-19 pandemic – an advocacy review: Psychiatry Res, 2020; 292; 113369
33. Koomazawa O, Suriastini NW, Wijayanti IY: Older people and COVID-19 in Indonesia, 2021; 82, Jakarta Pusat, Indonesia, Economic Research Institute for ASEAN and East Asia (ERIA)
34. UNICEF Indonesia: Impact of COVID-19 on maternal, newborn child and adolescent health in Indonesia, 2022 [updated September 2022; cited 30 November 2022]. Available from: https://www.unicef.org/indonesia/reports/impact-covid-19-maternal-newborn-child-and-adolescent-health-indonesia
35. Fekadu G, Bekele F, Tolossa T, Impact of COVID-19 pandemic on chronic diseases care follow-up and current perspectives in low resource settings: A narrative review: Int J Physiol Pathophysiol Pharmacol, 2021; 13(3); 86-93
36. Yunus F, Andarini S, Letter from Indonesia: Respirology, 2020; 25(12); 1328-29
37. Stachteas P, Symvoulakis M, Tsapas A, Smyrnakis E, The impact of the COVID-19 pandemic on the management of patients with chronic diseases in Primary Health Care: Popul Med, 2022; 31(4); 1-13
38. Lugito NPH, Kurniawan A, Lorens JO, Sieto NL, Mental health problems in Indonesian internship doctors during the COVID-19 pandemic: J Affect Disord Rep, 2021; 6; 100283
39. Gudi N, Konapur R, John O, Sarbadhikari S, Landry M, Telemedicine supported strengthening of primary care in WHO South East Asia region: Lessons from the COVID-19 pandemic experiences: BMJ Innovations, 2021; 7(3); 580-85
40. Clare CA, Telehealth and the digital divide as a social determinant of health during the COVID-19 pandemic: Netw Model Anal Health Inform Bioinform, 2021; 10(1); 26
41. Mahendradhata Y, Trisnantoro L, Listyadewi S: The Republic of Indonesia health system review, 2017, New Delhi, WHO Regional Office for South-East Asia
42. Kshanti IA, Epriliawati M, Mokoagow MI, The impact of COVID-19 lockdown on diabetes complication and diabetes management in people with diabetes in Indonesia: J Prim Care Community Health, 2021; 12; 21501327211044888
43. Sabarudin , Ihsan S, Nirmala F, Mahmudah R, Quality of drug management during the COVID-19 pandemic at outpatient health center, Kendari City: Int J Curr Sci Res Rev, 2022; 5(10); 3805-11
44. Ayele TA, Shibru H, Mequanent Sisay M, The effect of COVID-19 on poor treatment control among ambulatory Hypertensive and/or Diabetic patients in Northwest Ethiopia: PLoS One, 2022; 17(5); e0266421
45. Elnaem MH, Kamarudin NH, Syed NK, Associations between socio-demographic factors and hypertension management during the COVID-19 pandemic: Preliminary findings from Malaysia: Int J Environ Res Public Health, 2021; 18(17); 9306
46. Widyaningsih V, Febrinasari RP, Pamungkasari EP, Missed opportunities in hypertension risk factors screening in Indonesia: A mixed-methods evaluation of integrated health post (POSBINDU) implementation: BMJ Open, 2022; 12(2); e051315
47. Putri LP, Mawarni D, Trisnantoro L, Challenges of shifting diabetes mellitus care from secondary- to primary-level care in urban and rural districts: A qualitative inquiry among health providers: J Prim Care Community Health, 2020; 11; 2150132720924214
48. Arsyad DS, Hamsyah EF, Qalby N, The readiness of public primary health care (PUSKESMAS) for cardiovascular services in Makasar city, Indonesia: BMC Health Serv Res, 2022; 22(1); 1112
49. Azizi Z, Alipour P, Raparelli V, The role of sex and gender in hypertension: J Hum Hypertens, 2022 [Online ahead of print]
50. Dyer O, COVID-19: Indonesia becomes Asia’s new pandemic epicentre as delta variant spreads: BMJ, 2021; 374; n1815
Figures
Figure 1. Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS)Data are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). The paired t test was used for normally distributed data and non-parametric Wilcoxon signed-rank test was used for skewed data. * P value <0.05 was considered statistically significant.Figure 2. Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS) in study participants aged below 60 years oldData are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). Paired t test was used for normally distributed data and non-parametric Wilcoxon signed-rank test was used for skewed data. * P<0.05 was considered statistically significant.Figure 3. Routine 6-month evaluation of hypertension patients who were enrolled in the Indonesian Chronic Disease Management Program (PROLANIS) in study participants aged 60 years old and olderData are displayed as mean±SD for normally distributed data (TC, LDL, and eGFR) and displayed as median [IQR] for skewed data (BMI, SBP, DBP, TG, and HDL). BMI – body mass index; DBP – diastolic blood pressure; eGFR – estimated glomerular filtration rate calculated using CKD-EPI equation; HDL – high-density lipid; LDL – low-density lipid; SBP – systolic blood pressure; TC – total cholesterol; TG – triglyceride. T0 – evaluation in December 2019 (before the COVID-19 pandemic); T1 – evaluation in June 2020 (during the COVID-19 pandemic); T2 – evaluation in December 2020 (during the COVID-19 pandemic). The paired t test was used for normally distributed data and the non-parametric Wilcoxon signed-rank test was used for skewed data. * P<0.05 was considered statistically significant. Tables
 Table 1. Baseline characteristics of study participants.
Table 1. Baseline characteristics of study participants.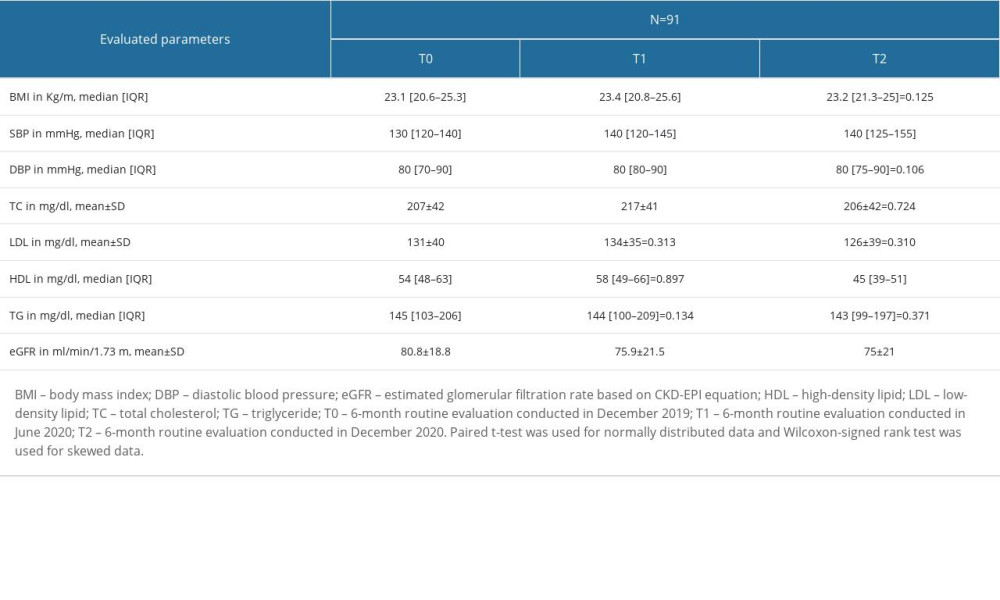 Table 2. Six-month routine follow-up evaluation.
Table 2. Six-month routine follow-up evaluation.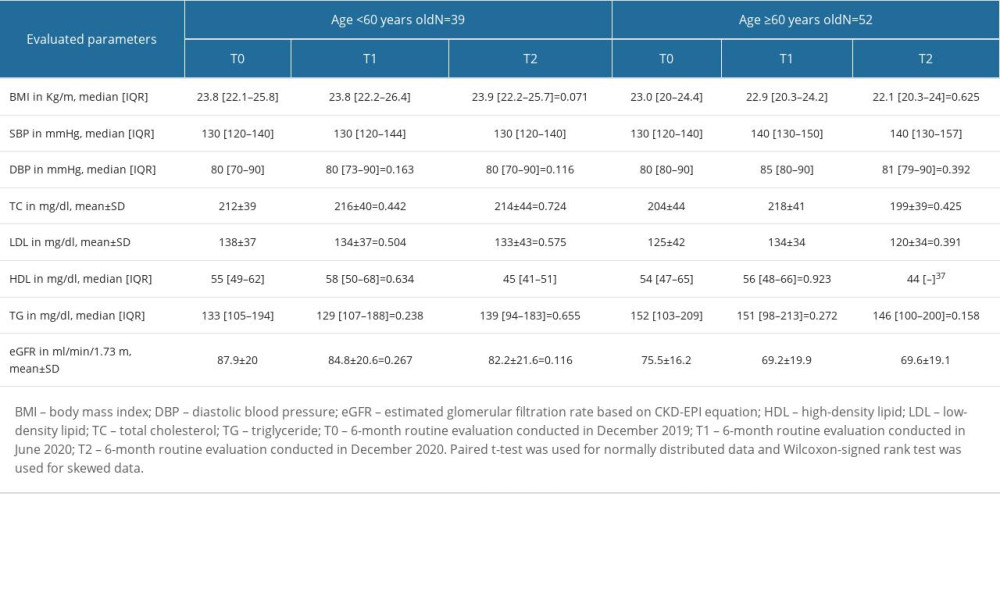 Table 3. Six-month routine follow-up evaluation of study participants stratified based on their age.Table 1. Baseline characteristics of study participants.Table 2. Six-month routine follow-up evaluation.Table 3. Six-month routine follow-up evaluation of study participants stratified based on their age.
Table 3. Six-month routine follow-up evaluation of study participants stratified based on their age.Table 1. Baseline characteristics of study participants.Table 2. Six-month routine follow-up evaluation.Table 3. Six-month routine follow-up evaluation of study participants stratified based on their age. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387