19 May 2023: Database Analysis
Causes of Death in Neonates, Infants, Children, and Adolescents at the University Children’s Clinical Hospital of Białystok Between 2018 and 2021
Monika Kamianowska1ABDE*, Aleksandra Kamianowska2BCDEF, Anna Wasilewska1ACDEDOI: 10.12659/MSM.939915
Med Sci Monit 2023; 29:e939915






Abstract
BACKGROUND: Monitoring of mortality rate and causes of death in pediatric hospitals is required in Poland. This study is aimed to evaluate the causes of death in neonates, infants, children, and adolescents obtained from the medical records of the University Children’s Clinical Hospital (UCCH) of Białystok between 2018 and 2021.
MATERIAL AND METHODS: This was an observational, cross-sectional study. Medical records of 59 patients (12 neonates, 17 infants, 14 children, 16 adolescents) who died in the UCCH of Białystok in 2018-2021 were analyzed. The records included personal data, medical history, and causes of death.
RESULTS: Between 2018 and 2021, the leading death causes were congenital malformations, deformations, and chromosomal abnormalities (25.42%, N=15) and conditions originating in the perinatal period (11.86%, N=7). The leading death causes in each age group were: in neonates – congenital malformations, deformations, and chromosomal abnormalities (50%, N=6), in infants –conditions originating in the perinatal period (29.41%, N=5), in children – diseases of the respiratory system (30.77%, N=4), and in teenagers – external causes of morbidity (31%, N=5). Before the COVID-19 pandemic (2018-2019), the leading death causes were congenital malformations, deformations, and chromosomal abnormalities (20.69%, N=6) and conditions originating in the perinatal period (20.69%, N=6). During the COVID-19 pandemic (2020-2021), congenital malformations, deformations, and chromosomal abnormalities (26.67%, N=8) and COVID-19 (10.00%, N=3) were the most common death causes.
CONCLUSIONS: Leading death causes varied among age groups. The COVID-19 pandemic had an impact on pediatric causes of death and changed their distribution. The results of this analysis should be discussed and conclusions should improve the quality of pediatric care.
Keywords: Child Mortality, Hospital Mortality, Hospitals, Pediatric, Pediatrics, Infant, Newborn, Pregnancy, Female, Humans, Child, Infant, Adolescent, Cause of Death, Pandemics, Universities, COVID-19, Chromosome Aberrations, Infant Mortality
Background
The child’s death is a tragedy for the family. It also impacts healthcare workers caring for the deceased child [1]. Since 1990, progress has been made in reducing child deaths. Unfortunately, many preventable child deaths still occur. They are mostly related to poor quality of care and adverse environmental and social conditions [1]. Pediatric mortality is thought to be not only a composite, but also a readily available way of measuring the health of the pediatric population [2].
Statistically analyzable underlying death causes were selected from the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10). Unified classification allows comparisons important for the purposes of the public health [3]. Analyses of leading causes of death among children provide the opportunity to understand pediatric mortality and burden of diseases, and allow improvement in establishing public health priorities [4]. Mortality monitoring is a source of information for assessing the population’s health needs and designing health policies. Changing patterns of mortality require modifications in health priorities to prevent avoidable deaths [1].
Analysis of causes of death should include whether the care provided was consistent with evidence-based clinical practice and standards of care [1]. Social and environmental risk factors should be analyzed, and attention should be paid to possible modifiable factors to improve the quality of care and avoid similar deaths [1]. Analysis of pediatric mortality improves the quality of care and provides an opportunity for reflection and education [1]. It also determines which areas of pediatric care need to be addressed and determines the most important goals aimed at improving the quality of care [5].
Therefore, this study aimed to evaluate the causes of death in neonates, infants, children, and adolescents obtained from the medical records of the University Children’s Clinical Hospital (UCCH) of Białystok between 2018 and 2021.
Material and Methods
ETHICS STATEMENT:
The study was approved by the Bioethics Committee at the Medical University of Białystok (approval number APK.002.306.2022) and complied with the Helsinki Declaration.
METHODS:
This observational, cross-sectional study [6] was performed according to the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines specific for cross-sectional studies [7].
MATERIAL:
All pediatric deaths which occurred at the UCCH of Białystok between 2018 and 2021 were reported to the hospital computer system. Patients’ information cards of the UCCH of Białystok, available in the computer system, provided personal data and information about causes of deaths based on the ICD-10 classification and the department where the death was confirmed. The Death Analysis Committee and the Adverse Events Committee provided data on detailed medical procedures. The causes of death were established by the physician present at the child’s death. Patients who died in the hospital had confirmed post-mortem diagnosis. Only 1 patient, with an advanced neoplasm, did not have post-mortem diagnosis confirmed.
ANALYZED DATA:
Data of children and adolescents who died between 2018 and 2021 were analyzed in particular years, considering age, sex, length of hospitalization, and department where the death was confirmed. Patients were grouped by age as newborns (patients aged up to 28 days), infants (patients aged between 29 days and 1 year), children (patients aged between 2 and 10 years), and adolescents (patients aged between 11 and 17 years). The length of hospitalization was analyzed in the following ranges: 1 day, 2–3 days, 4–10 days, and >10 days. The main, secondary, and concomitant diagnoses, and the underlying, secondary, and direct causes of death were analyzed. Attention was paid to the participation of the Brain Death Adjudication Committee and the Committee for Abandoning Persistent Therapy. Special attention was paid to determining whether it was possible to change pre-hospital, hospital, and social or environmental factors to avoid pediatric death.
Due to the epidemiological situation, special attention was paid to deaths caused by COVID-19, and the medical history of these patients was analyzed in detail. The data obtained from the UCCH of Białystok were compared with data from the Central Statistical Office on causes of death in Poland in 2018–2021 [8].
STATISTICAL ANALYSIS:
Data were presented in numerical form and using percentages (%). To determine the association between patient characteristics and patient outcomes, we used the odds ratio (OR), defined as the ratio of the odds of the outcome when the patient characteristics are present vs absent [9].
Statistical analysis was performed using an Odds Ratio Calculator (MedCalc Software Ltd), determining the OR and the confidence interval (CI) of the OR [10]. The Calculator determined the OR, its standard error, and 95% CI according to Altman and the P value according to Sheskin [11, 12]. Results were considered statistically significant at P<0.05.
Results
BASIC CHARACTERISTIC OF DECEASED PATIENTS:
In 4 years (2018–2021), 59 deaths occurred at the departments of the UCCH of Białystok (boys=36, girls=23), and these deaths accounted for 0.07% of the 80 237 hospitalizations in this period). Further analysis included sex, age, duration of stay, and the department where the patient died. Detailed data are presented in Table 1.
The number of hospitalizations was significantly lower in 2020 than in other years (15 860 compared to 21 459). Among the hospitalized children, 45.04% were girls and 54.96% were boys.
The number of deaths in boys was higher than in girls; however, when the number of hospitalizations was assessed, the difference was not statistically significant (OR=0.78, 95% CI: 0.46 to 1.32,
The number of deaths in particular groups based on the length of hospital stay changed in the analyzed years. Most of the deceased patients stayed in the hospital >10 days (37.29%, N=21) or 2–3 days (30.51%, N=18), and the smallest group stayed 1 day (10.17%, N=6).
Most deaths occurred in the Pediatric Intensive Care Unit (N=56, 94.92%). Deaths were also confirmed in the Department of Pediatrics, Oncology, and Hematology (5.08%, N=3). The number of deaths was also analyzed in individual quarters, but it showed no regularity.
There were 9 referrals to the Brain Death Adjudication Committee (15.25% of deaths), and brain death was adjudicated in each case. The Committee for Withdrawal from Persistent Therapy was approached once (1.69% of deaths), which resulted in withdrawal from the persistent therapy.
THE MAIN AND SECONDARY DIAGNOSES OF THE DECEASED PATIENTS:
The most common main diagnoses among the deceased patients were diseases of the respiratory system (37.29%, N=22), and among these, acute respiratory failure (72.73%, N=16). The most common secondary diagnoses were diseases of the respiratory system (15.25%, N=9), and among these, acute respiratory failure (44.44%, N=4). Detailed data are presented in Table 2.
THE UNDERLYING, SECONDARY, AND IMMEDIATE CAUSES OF DEATH:
The most common underlying causes of death were congenital malformations, deformations, and chromosomal abnormalities (25.42%, N=15) and conditions originating in the perinatal period (11.86%, N=7). The most common secondary causes of death were diseases of the respiratory system (15.25%, N=9), including acute respiratory failure (66.67%, N=6). The most common direct causes of death were acute respiratory failure (18.64%, N=11) and neonatal heart failure (11.86%, N=7). Detailed data are presented in Table 3.
The underlying causes of deaths were analyzed in particular age groups. The most common causes of neonatal deaths were congenital malformations, deformations, and chromosomal abnormalities (50.00%, N=6). The leading cause of infant deaths was conditions originating in the perinatal period (29.41%, N=5). The most common cause of death in children was diseases of the respiratory system (30.77%, N=4) and in teenagers it was external causes of morbidity (31.25%, N=5). Detailed data are presented in Table 4.
We also analyzed deaths due to external (traumatic) causes. There were 5 accidents and 2 suicides, which accounted for 8.47% and 3.39%, respectively, of all deaths in 2018–2021. Death due to external causes was reported only in children (1 death) and teenagers (5 deaths), and were the most common leading causes of deaths among deceased teenagers.
The analysis of the Medical Records showed that 13 of 59 deaths (22.03%) were avoidable. The detailed data are presented in Table 5.
COVID-19-RELATED DEATHS:
At the UCCH of Białystok in 2020–2021, there were 823 hospitalizations of patients with COVID-19. COVID-19 was the underlying cause of death in 3 patients (5.08% of deaths), and the secondary cause of death in 2 patients (3.39% of deaths). Deceased patients accounted for 0.61% of hospitalized COVID-19 patients. Detailed data are presented in the Table 6.
We also compared the causes of deaths before (2018 and 2019) and during (2020 and 2021) the COVID-19 pandemic. Before the COVID-19 pandemic (2018–2019), the most common underlying causes of deaths among pediatric patients were congenital malformations, deformations, and chromosomal abnormalities (20.69%, N=6) and conditions originating in the perinatal period (20.69%, N=6). Deaths due to external (traumatic) causes ranked second among all causes of death. During the COVID-19 pandemic (2020–2021), congenital malformations, deformations, and chromosomal abnormalities were still the leading causes of death (26.67%, N=8). COVID-19 was an underlying cause of 3 deaths, ranking second among pediatric causes of death (10.00%, N=3).
When compared with before the pandemic, during the COVID-19 pandemic, more deaths associated with infectious diseases were reported among all causes of death (OR=0.2308, 95% CI: 0.06 to 0.95, P=0.04). No differences were found in suicides (OR=1.04, 95% CI: 0.06 to 17.38, P =0.98) and deaths due to external causes (OR=1.44, 95% CI: 0.30 to 7.08, P=0.65) between the years before and during COVID-19 pandemic. The numbers of deaths due to chronic diseases, congenital anomalies, and prematurity did not differ between 2018–2019 and 2020–2021 (OR=1.85, 95% CI: 0.66 to 5.24, P=0.25). The detailed data are presented in Table 7.
Discussion
LIMITATIONS OF THE STUDY:
The main limitations of the study are the short period analyzed and the small number of analyzed deaths. It would be valuable to conduct further analyses involving retrospective data and similar studies to obtain the most accurate information on trends in pediatric deaths. Moreover, it would be valuable to conduct similar analyses in other hospitals in Poland and search for similarities or differences in causes of deaths among regions.
This was a cross-sectional study, so it is difficult to prove causal relationships, and associations and direction of associations should be carefully interpreted [6]. The main statistical method used in the study, the odds ratio, also presents some limitations. It is thought to be a good starting point in investigation of the association between binary characteristics. However, this kind of association should not be used to predict outcomes [27].
In this study, we considered COVID-19 only as the main cause of death. However, COVID-19 is thought to be able to amplify impacts of other diseases. Therefore, it cannot be excluded that COVID-19 had any impact on the conditions of other deceased children, especially those who died from infectious diseases [28].
Conclusions
In 2018–2021, the most common underlying causes of death in children and adolescents were congenital malformations, deformations, and chromosomal abnormalities, conditions originating in the perinatal period, and external causes of death. There were more deaths in boys than in girls, however, but when the number of hospitalizations was assessed, the difference did not appear to be significant. No difference in the number of deaths was found between age groups. The main causes of death in each age group were: in neonates – congenital malformations, deformations, and chromosomal abnormalities; in infants – certain conditions originating in the perinatal period; in children – diseases of the respiratory system; and in teenagers – external causes of death.
Before the COVID-19 pandemic, the most common underlying causes of deaths among pediatric patients were congenital malformations, deformations, and chromosomal abnormalities and conditions originating in the perinatal period. During the COVID-19 pandemic, congenital malformations, deformations, and chromosomal abnormalities were still the leading causes of death, but COVID-19 ranked second among pediatric causes of death. During the COVID-19 pandemic, more deaths associated with infectious diseases were reported among all deaths. The results of this analysis should be discussed and conclusions should improve the quality of care.
Tables
Table 1. Characteristics of deceased children and adolescents in 2018–2021 at the University Children’s Clinical Hospital of Białystok. Table 2. Characteristics of the most common main and secondary diagnoses among patients hospitalized in 2018–2021 at the University Children’s Clinical Hospital of Białystok.
Table 2. Characteristics of the most common main and secondary diagnoses among patients hospitalized in 2018–2021 at the University Children’s Clinical Hospital of Białystok.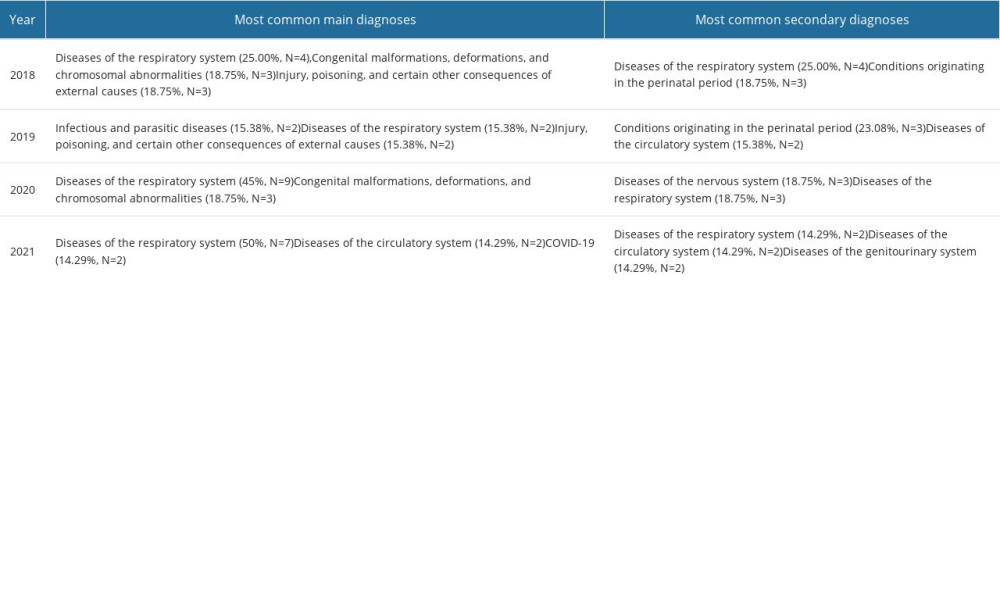 Table 3. The main underlying, secondary, and immediate causes of death of patients who died in 2018–2021 at the University Children’s Clinical Hospital of Białystok.
Table 3. The main underlying, secondary, and immediate causes of death of patients who died in 2018–2021 at the University Children’s Clinical Hospital of Białystok.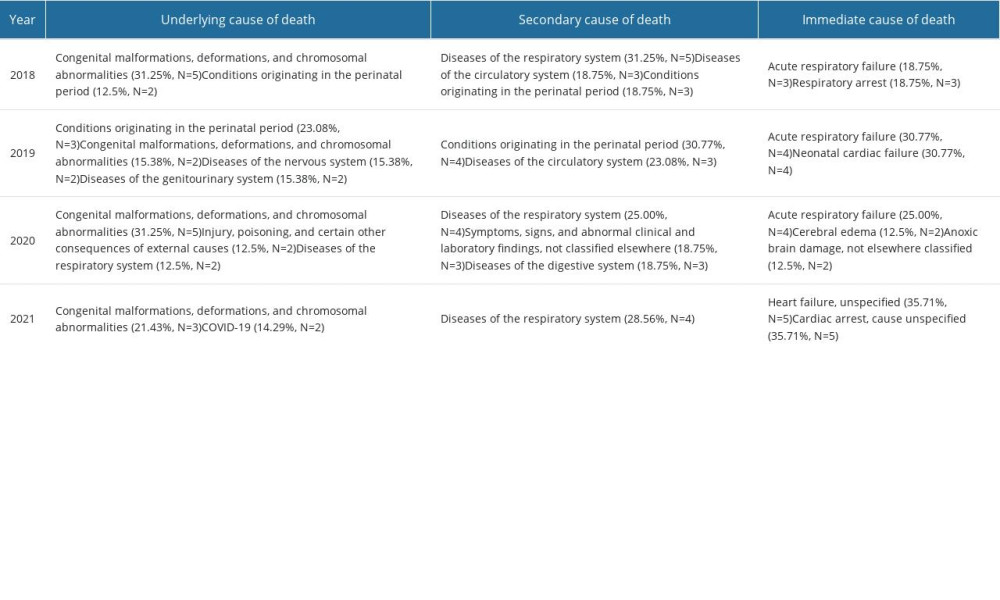 Table 4. Leading main causes of deaths among neonates, infants, children and teenagers deceased at the University Children’s Clinical Hospital of Białystok in 2018–2021.
Table 4. Leading main causes of deaths among neonates, infants, children and teenagers deceased at the University Children’s Clinical Hospital of Białystok in 2018–2021.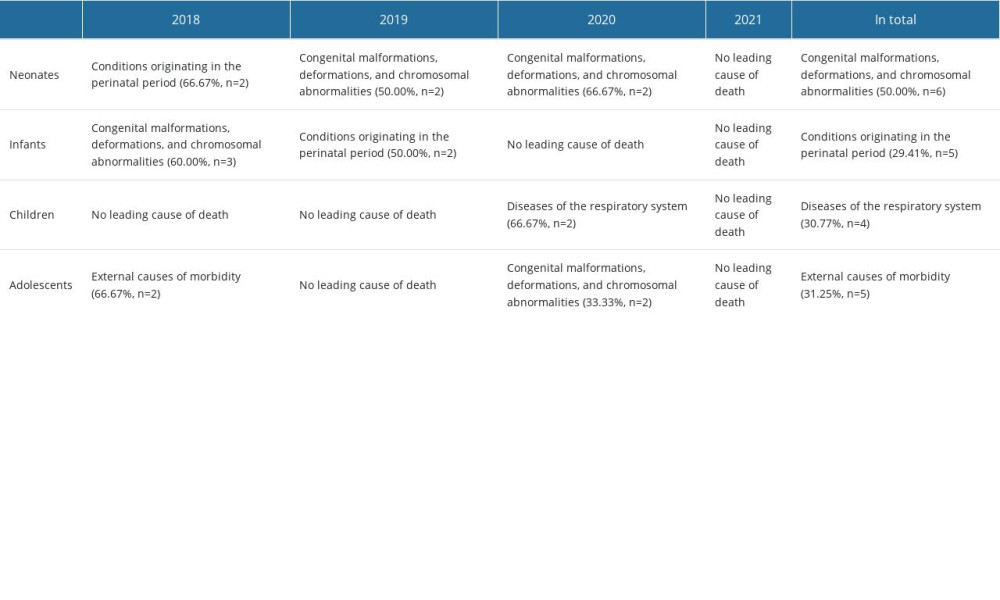 Table 5. The characteristics of avoidable deaths in 2018–2021 at the University Children’s Clinical Hospital of Białystok.
Table 5. The characteristics of avoidable deaths in 2018–2021 at the University Children’s Clinical Hospital of Białystok.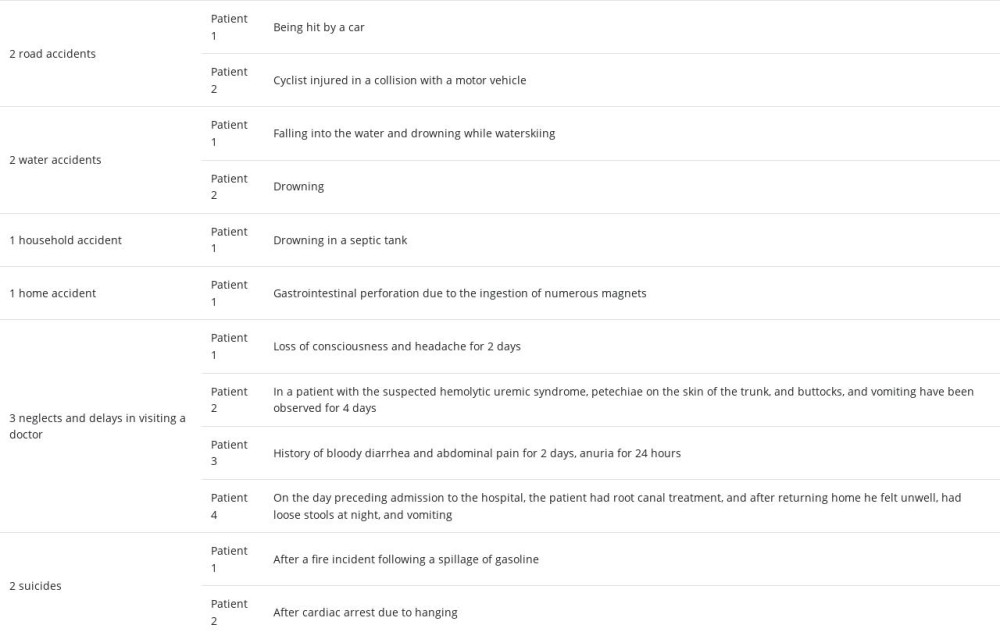 Table 6. The characteristics of COVID-19-related deaths in 2018–2021 at the University Children’s Clinical Hospital – the patients’ concomitant diagnoses.
Table 6. The characteristics of COVID-19-related deaths in 2018–2021 at the University Children’s Clinical Hospital – the patients’ concomitant diagnoses.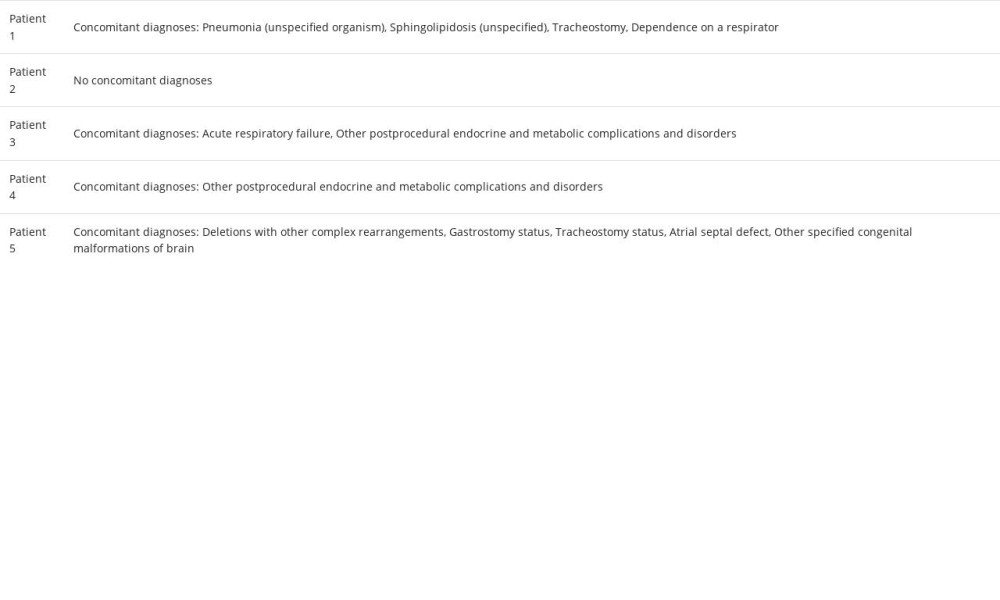 Table 7. The characteristics of pediatric deaths before (2018 and 2019) and during the COVID-19 pandemic (2020 and 2021) at the University Children’s Clinical Hospital of Białystok.
Table 7. The characteristics of pediatric deaths before (2018 and 2019) and during the COVID-19 pandemic (2020 and 2021) at the University Children’s Clinical Hospital of Białystok.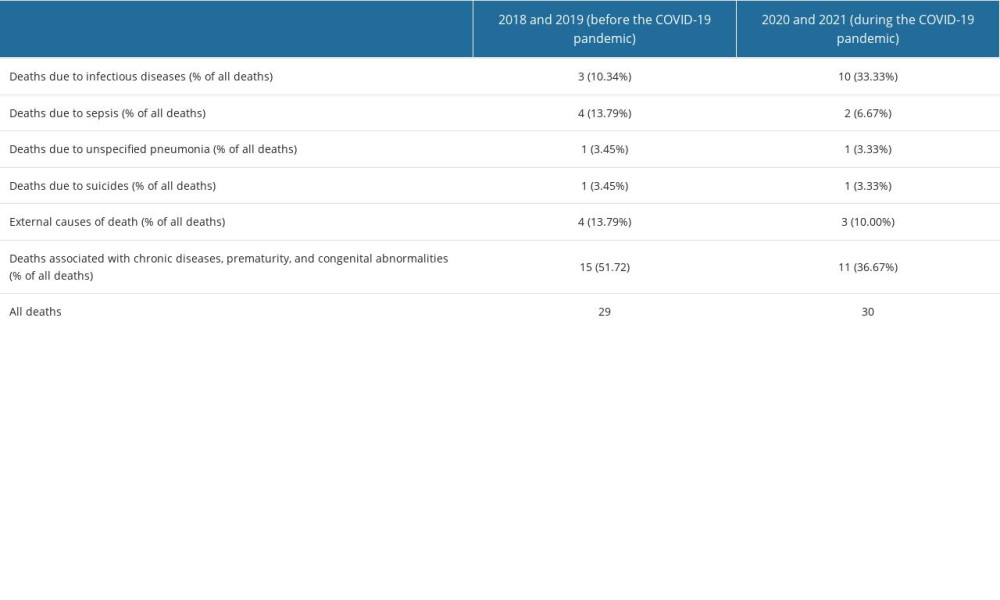
References
1. World Health Organization (WHO), Improving the quality of paediatric care: Operational guide for facility-based audit and review of paediatric mortality October 2, 2018 Available at: https://www.who.int/publications/i/item/9789241515184
2. Karlsson O, Kim R, Hasman A, Subramanian SV, Age distribution of all-cause mortality among children younger than 5 years in low- and middle-income countries: JAMA Netw Open, 2022; 5(5); e2212692
3. McNeill VF, Corsi R, Huffman JA, Room-level ventilation in schools and universities: Atmos Environ X, 2022; 13; 100152
4. Flaxman S, Whittaker C, Semenova E, Assessment of COVID-19 as the underlying cause of death among children and young people aged 0 to 19 years in the US: JAMA Netw Open, 2023; 6(1); e2253590
5. Ali H, Aziz S, Rising pediatric morbidity and mortality in the developing world: Cureus, 2021; 13(4); e14728
6. Setia MS, Methodology series module 3: Cross-sectional studies: Indian J Dermatol, 2016; 61(3); 261-64
7. Vandenbroucke JP, von Elm E, Altman DG, Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration: PLoS Med, 2007; 4(10); e297
8. Statistics Poland: Mortality and deaths by causes Available at: https://stat.gov.pl/en/topics/population/mortality-and-deaths-by-causes-/
9. Szumilas M, Explaining odds ratios [published correction appears in J Can Acad Child Adolesc Psychiatry. 2015;24(1):58]: J Can Acad Child Adolesc Psychiatry, 2010; 19(3); 227-29
10. MedCalc Software Ltd: Odds ratio calculator Available at: https://www.medcalc.org/calc/odds_ratio.p
11. Altman DG: Practical statistics for medical research, 1991, London, Chapman and Hall
12. Sheskin DJ: Handbook of parametric and nonparametric statistical procedures, 2004, Boca Raton, Chapman & Hall/CRC
13. Strong KL, Pedersen J, White Johansson E, Patterns and trends in causes of child and adolescent mortality 2000–2016: Setting the scene for child health redesign: BMJ Glob Health, 2021; 6(3); e004760
14. Cunningham RM, Walton MA, Carter PM, The major causes of death in children and adolescents in the United States: N Engl J Med, 2018; 379(25); 2468-75
15. Lingsma HF, Bottle A, Middleton S, Evaluation of hospital outcomes: The relation between length-of-stay, readmission, and mortality in a large international administrative database: BMC Health Serv Res, 2018; 18(1); 116
16. Penchaszadeh VB, Preventing congenital anomalies in developing countries: Community Genet, 2002; 5(1); 61-69
17. Koshida S, Yanagi T, Ono T, Possible prevention of neonatal death: A regional population-based study in Japan: Yonsei Med J, 2016; 57(2); 426-29
18. Harvey A, Towner E, Peden M, Injury prevention and the attainment of child and adolescent health: Bull World Health Organ, 2009; 87(5); 390-94
19. Public Health Agency of Canada (Canada): Child and youth injury in review 2009 edition: spotlight on consumer product safety, 2009, Ottawa (ON), The Agency
20. Rosenfield D, Strickland M, Fecteau A, Magnet ingestion by a 3-year-old boy: CMAJ, 2013; 185(11); 972-74
21. World Health Organization (WHO), Global health estimates: Leading causes of death: Cause-specific mortality, 2000, 2019 Available at: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates
22. Bertran M, Amin-Chowdhury Z, Davies HG, COVID-19 deaths in children and young people in England, March 2020 to December 2021: An active prospective national surveillance study: PLoS Med, 2022; 19(11); e1004118
23. Sharma R, Agarwal A, Ranjan A, Mortality audit of COVID-19 infection among children: Indian J Med Res, 2022; 155(5&6); 505-9
24. Emami A, Javanmardi F, Pirbonyeh N, Akbari A, Prevalence of underlying diseases in hospitalized patients with COVID-19: A systematic review and meta-analysis: Arch Acad Emerg Med, 2020; 8(1); e35
25. Price AM, Olson SM, Patel MM, BNT162b2 protection against the Omicron variant in children and adolescents. Reply: N Engl J Med, 2022; 386(24); 2346
26. McNeill VF, Corsi R, Huffman JA, Room-level ventilation in schools and universities: Atmos Environ X, 2022; 13; 100152
27. Chatterjee A, Woodruff H, Wu G, Lambin P, Limitations of only reporting the odds ratio in the age of precision medicine: A deterministic simulation study: Front Med (Lausanne), 2021; 8; 640854
28. Swets MC, Russell CD, Harrison EM, SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses: Lancet, 2022; 399(10334); 1463-64
Tables
Table 1. Characteristics of deceased children and adolescents in 2018–2021 at the University Children’s Clinical Hospital of Białystok.Table 2. Characteristics of the most common main and secondary diagnoses among patients hospitalized in 2018–2021 at the University Children’s Clinical Hospital of Białystok.Table 3. The main underlying, secondary, and immediate causes of death of patients who died in 2018–2021 at the University Children’s Clinical Hospital of Białystok.Table 4. Leading main causes of deaths among neonates, infants, children and teenagers deceased at the University Children’s Clinical Hospital of Białystok in 2018–2021.Table 5. The characteristics of avoidable deaths in 2018–2021 at the University Children’s Clinical Hospital of Białystok.Table 6. The characteristics of COVID-19-related deaths in 2018–2021 at the University Children’s Clinical Hospital – the patients’ concomitant diagnoses.Table 7. The characteristics of pediatric deaths before (2018 and 2019) and during the COVID-19 pandemic (2020 and 2021) at the University Children’s Clinical Hospital of Białystok. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387