13 July 2023: Clinical Research
Deciphering Pediatric Root Canal Practices in Turkey: A Comparative Study Bridging the Gap between Practice and Literature
Tuğçe Nur ŞahinDOI: 10.12659/MSM.940296
Med Sci Monit 2023; 29:e940296






Abstract
BACKGROUND: Pediatric endodontics is a critical area of dental practice, involving the treatment of root canals in primary teeth. Treatment approaches can significantly vary due to a range of factors, potentially impacting the success of the procedure and patient comfort. This variability, often influenced by regional practices, individual dentist preferences, and the pace of dental technology advancements, warrants detailed examination to improve standardization and care outcomes. Accordingly, our study aims to scrutinize the endodontic practices of pedodontists in Turkey and compare them with contemporary literature.
MATERIAL AND METHODS: We conducted an online survey with 15 questions that 217 Turkish pedodontists answered. The questionnaire sought information about their preferences in canal length measurement, canal sealer, irrigation solution, and other procedural decisions. Chi-square test was used to analyze the responses, with a significance level of p<0.05.
RESULTS: The majority of respondents were associated with universities (123 out of 217). 103 preferred rotary file sets, and 114 used apex locators for canal length measurement. Iodoform pastes (160) and sodium hypochlorite (180) were the most popular choices for canal sealers and irrigation solution, respectively. 152 participants did not prefer using rubber dam, and 186 did not favor sonic-ultrasonic activators. Many reported using hand files as students (184), with 39 continuing this practice. Post-graduation, 64 participants took root canal treatment courses, while 72 were reluctant to perform the procedure under general anesthesia.
CONCLUSIONS: No single method stood out as superior for primary root canal treatments in deciduous teeth. Incorporating advanced technology into dental practice may potentially improve treatment success and patient comfort.
Keywords: Pediatric Dentistry, Root Canal Therapy, Surveys and Questionnaires, Tooth, Deciduous, Humans, Child, Turkey, Dental Pulp Cavity, Endodontics, Anesthesia, General
Background
Healthy primary dentition plays a key role in the development of the jaws in terms of preserving occlusion and arch length. The most important factor threatening primary dentition health is dental caries. Although preventive measures have reduced caries, early loss of primary teeth with pulp-involving caries remains a common problem. Fortunately, with successful root canal treatments, professionals can keep most of these deciduous teeth in the mouth until they normally fall out [1,2]. Root canal treatment of deciduous teeth should be performed within a short period and with minimal complications. Effective shaping and debridement without weakening the tooth structure and damaging the permanent tooth germ is crucial [3–5].
The first step of root canal treatment is a good isolation, which is ideally only possible with a rubber dam [6]. In addition to preventing the patient from talking and covering his or her mouth, it provides the clinician with a dry, safe surgical field, improves visibility, and thus increases the success of the procedure. Moreover, a rubber dam is also the most effective means of preventing cross-infection during dental treatments [7].
Root canal treatment progresses in stages, and the success of the treatment depends on the careful implementation of all these steps. As in permanent teeth, correct determination of the working length in primary teeth is also very important for the success of the next steps of root canal treatment [8,9]. However, as soon as the deciduous tooth roots have completed their formation, they begin to resorb [10]. With the progression of root resorption, the apical foramen begins to be positioned more coronally than the anatomical apex of the root. Radiographically, this makes determining the root canal length difficult [11]. There may be resorption along the root and into the root canal, and different connections can form with periapical tissues other than the apical foramina, lateral canals, and accessory canals. Therefore, the use of an electronic apex locator is not recommended for determining the root canal length in deciduous teeth [10]. There are, however, some studies that recommend using this method to determine the length of canals in deciduous teeth root canal treatments without exposing the patient to radiation [8].
Another factor in chemomechanical preparation is the canal file [12]. For this purpose, conventional hand files are still widely used in the endodontic treatment of devital primary teeth. However, with the developing technology, the use of rotary file systems developed for permanent teeth has become routine in endodontic treatment for adults over the past decade and it is well known that modern rotary file systems minimize procedural errors [13]. However, there is a lack of laboratory data showing how modern rotary filing systems alter deciduous tooth root morphology [14].
The use of rotary instruments in pediatric endodontics was first introduced by Barr et al [15]. They stated that the natural flexibility of these files preserves the original anatomy of the curved canals in deciduous molars [16]. On the other hand, Kuo et al [17] suggested that a rotary file with modified length, taper, and tip size would be more effective for pulpectomy in deciduous teeth. Different pediatric file sets have been developed under different brand names by many researchers who share this idea [18]. Since mouth opening is limited in pediatric patients, rotary files with longer lengths are difficult to use. Pediatric rotary files are designed with a shorter length. This feature provides ease of use when working with pediatric patients [16].
One of the most important steps of the endodontic treatment procedure is to remove the debris, pulp tissue, and microorganisms in the root canal system with chemomechanical preparation and to give the root canal a uniform canal shape [12]. Currently, sodium hypochlorite is the most widely used irrigation solution because it possesses many of the desired properties of an ideal irrigation solution in root canal treatments. Sodium hypochlorite has a broad spectrum and nonspecific ability to kill all microorganisms and dissolve necrotic tissues [19]. On the other hand, chlorhexidine has a bacteriostatic effect at low concentrations and a bactericidal effect at high concentrations by causing cell damage, cytoplasm coagulation, and precipitation of proteins and nucleic acids [20]. Chelating agents such as EDTA, which have a limited antibacterial effect, are frequently recommended, especially in narrow and calcified canals, for facilitating canal preparation with its lubricating properties and removing smear deposits [21–23]. Recent studies have indicated that the smear layer and debris can be removed more effectively by activating irrigation solutions in root canals and suggest manual or mechanical activation techniques [24].
The aim of primary tooth root canal treatment includes instrumentation with appropriate file and removal of pulp, bacteria, and bacterial toxins with appropriate irrigation solution and filling the canal with a resorbable material [18]. The ideal deciduous tooth root canal filling material should be antiseptic and nontoxic, easily filled into the canal or easily removed, resorb at the same rate as the deciduous tooth root, be harmless to periapical tissues and permanent tooth germ, and resorb when it overflows from the apex [25]. Zinc oxide eugenol (ZOE), iodoform, and calcium hydroxide paste are the most commonly used filling materials for root canal treatment. It has been found that ZOE is more effective than others in the hyperemic deciduous pulp. However, when it protrudes from the apex, it may alter the eruption path of the permanent tooth as it forms a hard mass and resorbs very slowly compared with physiological root resorption [26].
Although the effect of endodontic instruments and materials on permanent tooth germs is not fully known and compliance problems often seen in pediatric patients cause root canal treatment not to be preferred by some dentists, most dentists apply pulpectomy treatment as an alternative to extraction and space maintainer application [1].
In the literature review, there was no study evaluating the approach of pedodontists in Turkey to the root canal treatment of deciduous teeth and the procedures they follow. Therefore, the present questionnaire-based study aimed to examine the guidelines and approaches of pedodontists in our country when performing primary root canal treatment and to compare them with the current literature on the subject.
Material and Methods
ETHICS APPROVAL:
Approval for the study was obtained from the Clinical Research Ethics Committee of Karamanoglu Mehmetbey University, Faculty of Medicine, with decision no. 06-2022/18.
STUDY DESIGN AND DATA SETTING:
The sample size for the descriptive sampling technique was calculated using an expected response rate of between 60% and 80% and a 90% power calculation with a 95% confidence interval. For this purpose, a self-administered and online 15-question 2-part questionnaire (Table 1) prepared using Google Forms (Google, Inc., 2017, California, USA) was randomly sent to 300 pediatric dentists via e-mail and message with the help of the Turkish Pediatric Dentistry Association. To preserve the accuracy and confidentiality of the data, the questionnaire was made anonymous.
After the literature search, 15 questions about the primary tooth root canal treatment procedure and the demographic variables of the participants were prepared and emailed to 3 experts to validate the content using a 5-point Likert scale. As a result of the evaluation, each question was found appropriate and included in the study. The reliability of the questionnaire was checked with the help of the Cronbach α value using the test-retest method. Numbers between 0.697 and 1 and the median 1 were considered reliable.
The first 4 questions in the questionnaire consisted of questions about demographic variables such as age, gender, place of work and working year of pediatric dentists. The next questions question the attitudes and preferences of physicians regarding the choice of materials and techniques used during primary tooth root canal treatment, participation in any workshop of primary tooth root canal treatment after the completion of specialty/doctoral training, or application preferences under general anesthesia. The questionnaire consisted of open-ended and multiple-choice questions. Participants who answered “I want to participate” in the consent form in the first part moved on to the second part, answered the questions, and participated in the study. Forty-two people who answered “I do not want to participate” to the consent form in the first section of questionnaire and 41 people continuing their specialization or doctorate education were excluded from the study. Responses of 217 pediatric dentists who were answered were statistically analyzed.
STATISTICAL ANALYSES:
For statistical analysis, participants were divided into 4 groups according to the institutions (University, Oral and Dental Health Center/Oral and Dental Health Hospital (ODHC/ODHH), Private outpatient clinic, Own Clinic) they worked in. The chi-square test was used to determine the association between categorical variables, and p<0.05 was considered significant. The data were analyzed using the IBM SPSS Statistics Version 27 (IBM SPSS Inc., Chicago, IL, ABD) package program.
Results
The answers of 217 participants were evaluated for this study, which aimed to evaluate the materials and methods used by pedodontists during the primary tooth root canal treatment process and their approaches, as shown in Table 1; 73.7% of the 217 participants were between the ages of 25–35 and 78.8% were female pedodontists (p<0.05).
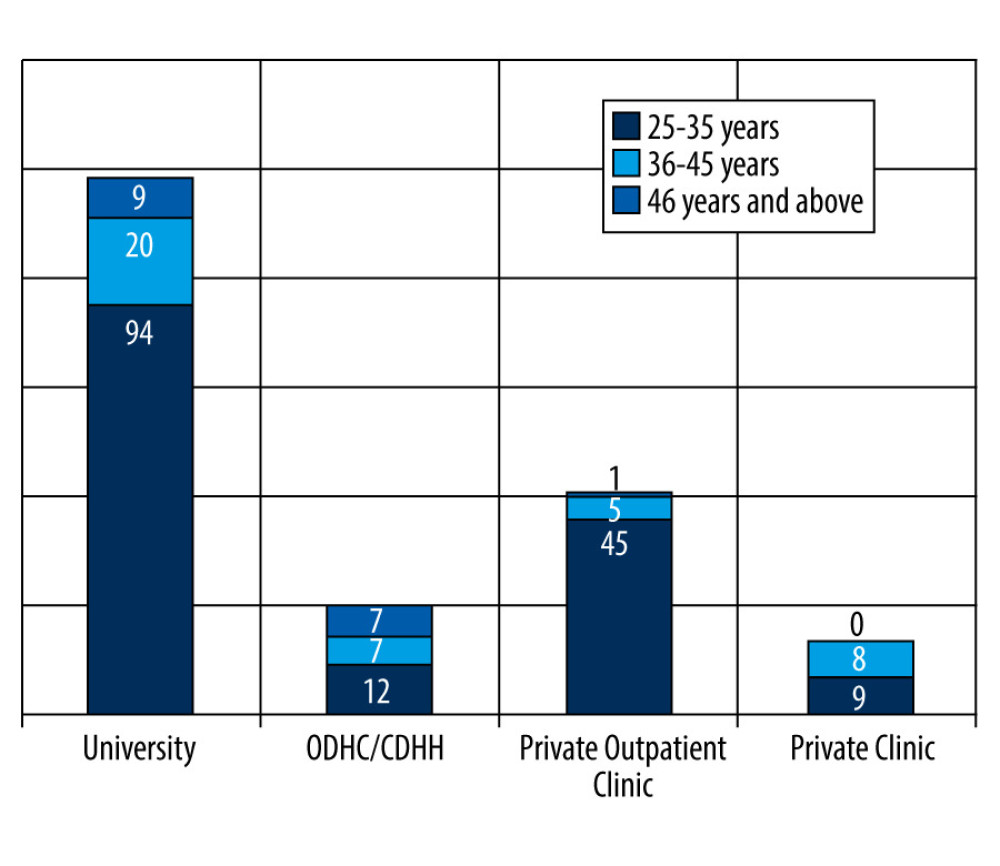
When evaluated according to institutions, as shown in Figure 1, the most participation was from universities (p<0.05).
When the participants were asked whether they preferred to use the rubber dam during root canal treatment of deciduous teeth, it was found that most of the participants did not prefer to use the rubber dam (146), except for pedodontists working in their private clinic, whereas only 35% of the pedodontists working in their private clinic did not (p<0.05).
Table 2 shows that the majority of institutions found only apex locators sufficient for canal length determination (p<0.05).
When examining the file preferences according to the institutions, it was found that pedodontists working in universities and ODHC/Hs mostly preferred rotary file sets, while pedodontists working in their private clinics and private outpatient clinics mostly preferred pediatric canal files (p<0.05).
It is shown in Table 3 that approximately 85% of the participants used only hand files during primary tooth root canal treatment when they were interns and only 39 people continued with the same system, while none of the participants who used a rotary or pediatric file set during their education preferred to use only hand files for primary tooth root canal treatment after graduation, and all 6 people who had experienced the pediatric file set during their student years continued their treatment with the same method (p<0.05).
There was no significant difference in the preference for irrigation solutions between the institutions, with sodium hypochlorite being the most preferred in each institution, while EDTA was not preferred by any of the pedodontists (p>0.05).
As a final irrigation solution, serum was preferred by the majority regardless of the canal irrigation solution (p<0.05). Table 4 also shows that the number of participants who preferred to use a single solution during treatment was 103 (p<0.05).
While there was no significant difference between the institutions regarding the use of sonic or ultrasonic activators during treatment, 86% of the participants did not use them (p>0.05).
Although there was no significant difference in preference for root canal paste between the institutions for deciduous tooth root canal treatment, 73.7% of the participants preferred iodoform paste (p>0.05).
The mean duration of root canal treatment for deciduous teeth, excluding the restoration phase, was calculated to be 22 minutes, with pedodontists working in ODHC/Hs having the shortest mean duration (p>0.05).
Based on the file system used, the mean duration of root canal treatment was 22.33 minutes with rotary files, 22.24 minutes with hand files alone, and 22.16 minutes with pediatric root canal files (p>0.05).
It was found that 33% of the participants preferred extraction to root canal treatment under general anesthesia, preferring a more radical approach than most participants (p<0.05).
The majority of the participants who worked in the state institution and 70% of the participants regardless of their institutional affiliations did not attend any canal treatment courses after they completed their specialization training (p<0.05).
Discussion
Survey studies enable us to assess whether our views or approaches are in accordance with current trends [27]. The aim of this study was to compare the procedures followed by pedodontists in Turkey when applying root canal treatment to deciduous teeth considering the current literature.
There are several factors that complicate the use of rubber dams in the studies published in the literature, including increased costs, difficulty in accessing rubber dams, inadequate education, and patients’ refusal [28,29]. Patients’ low acceptance of rubber dams has been generally reported in the literature as the most important reason for not using rubber dams [30]. However, many studies that question patients’ approaches to rubber dams found that patient acceptance was high [31,32]. Likewise, in our study, most of the pedodontists did not prefer rubber dam isolation for similar reasons.
In some studies, the rubber dam is reported to cause less stress to patients than cotton rolls [33] and reduces stress for physicians during treatment as well [34]. According to the 2020 AAPD guidelines [35], rubber dam isolation is the gold standard for pulpal treatments. Nonetheless, many studies have reported, in accordance with our findings, that rubber dams are highly preferable in pediatric patients [27,36,37].
It has been reported in a survey study of 100 dentists in India that half preferred rotary files [38], whereas in a study of 50 dentists, 62% preferred only using hand files [39]. According to a retrospective study examining pediatric dentists’ file preferences [40], 86% of pedodontists preferred rotary files when treating their patients. Similarly, in our study, in which the participants reported that rotary files were preferred the most (47%), 85% of them used only hand files during deciduous root canal treatment when they were trainee students, but today they predominantly use rotary or pediatric file sets, suggesting that physicians prefer more technological techniques thanks to the reduced risk of aspiration of the instruments and the shorter treatment period.
It is noteworthy that although we did not observe a significant difference in the duration of treatment when we compared the file preference with the duration of treatment in our study, many recent studies have reported that a pediatric canal file or rotary file facilitates a faster preparation process [5,41–45].
Moreover, in studies comparing the preparation and filling quality of hand files, rotary files, and pediatric files, it has been found that pediatric files were generally superior to the others, and the use of these files is recommended during root canal treatment [16,46,47]. Meanwhile, the AAPD guideline [35] states that hand files or rotary files are preferred.
Although there are studies in the literature [39,48] reporting that the most preferred deciduous tooth root canal paste by participating dentists is eugenol paste, unlike this result, similar to our study, in a survey of 360 pedodontists [27], iodoform paste was the most preferred, and in a retrospective study of 2496 case papers [49], Metapex was the most preferred (96.6%). A recent meta-analysis [50] reported that there was no difference between the short- and long-term outcomes of iodoform and pastes with iodoform, but added that the certainty of the evidence in the studies reviewed ranged from low to very low. In another meta-analysis [51], there was no significant difference between iodoform and eugenol paste, but the long-term success of eugenol paste was higher, and the researchers suggested that iodoform paste should be preferred if the tooth to be treated is close to the physiologic fall time, and eugenol paste should be preferred if it is not.
In light of the lack of absolute evidence that one paste is superior to another, many publications and books leave it up to the clinician to choose the paste [10,35,52,53]. However, the AAPD [35], in its guideline, added that eugenol paste is more successful in the long run than other pastes.
Because ZOE paste is resorbed later than deciduous tooth roots, there have been reports of cases where the material left after pulpectomy caused delayed eruption, resulting in moderate foreign body reaction in the patient and the eruption of the permanent tooth from more palatal or anterior crossbite [54,55]. Based on our study, we believe that participants preferred iodoform paste over ZOE paste due to the mentioned disadvantages.
In a study of 2400 patients in South India [56], it was reported that serum was preferred over sodium hypochlorite during root canal treatment of deciduous teeth of patients aged 0–5 years. Likewise, in a study [48] of 221 dentists, serum was again the most preferred irrigation solution. Meanwhile, in our study, it was found that the participants mostly used sodium hypochlorite as the irrigation solution and serum as the final irrigation solution. This may have been caused by the fact that sodium hypochlorite is also mostly preferred during root canal treatment in permanent teeth [57]. The most recent study [58] and many other studies have determined that sodium hypochlorite is the best agent for disinfection, and the AAPD guideline [35] reports that there is no significant difference between solutions and that sodium hypochlorite should be used carefully.
The use of apex locators to determine the canal length of deciduous teeth is still a matter of debate. Although there are resources in the literature that do not recommend its use [59], resources that suggest its use but argue that there is not enough research on the subject [60], and resources that recommend its use [61] and references report that apex locators are much more acceptable by children than traditional radiography [62], no conclusive evidence has been provided as to which of the methods is the best.
In a survey of 237 physicians [63], the use of apex locators was reported to be less common than the radiographic technique, but due to the limitations of radiographic interpretation and the high probability of overinstrumentation and consequent flood filling of unevenly resorbed roots, the use of apex locators has been recommended regardless of the stage of root resorption. Similarly, the participants (52.5%) preferred apex locators alone most for this purpose because of their advantages, such as saving time for the physician and protecting patients from radiation.
Although there are few studies on the use of ultrasonic/sonic activators in primary teeth, it has been found to be quite successful in the studies in which it has been evaluated [64,65]; however, 85% of the participants in our study did not prefer to use it. It is thought that this might have been caused by the divergent and narrow structure of the deciduous tooth roots.
The results of a study [66] conducted in Saudi Arabia aimed at assessing the level of knowledge of participants regarding root canal treatment of deciduous teeth were similar to our results, in that most participants did not attend courses or workshops after graduation. The reason for this can be attributed to the fact that the pedodontists participating in the study found their specialist training sufficient or that there are few courses or workshops in our country about primary tooth root canal treatment. The reason why the courses on new developments in the field of pedodontics are quite limited in our country may be that features such as low-noise instruments [67] or computerized anesthesia devices [68] are new, and more studies are needed.
An alternative treatment method for primary tooth root canal treatment is extraction [69]. In the early extraction of primary teeth, the need for orthodontic treatment may occur in the future [70]. To prevent this, space maintainers are used. Similar to the results of our study (67%), it has been reported in many studies that instead of extracting the primary tooth, it is preferred to keep the tooth in the mouth with root canal treatment, and the survival rates after primary tooth root canal treatment under general anesthesia are high and the techniques are successful and reliable [68,69].
The limitations of the study are that although the study group comprised an estimated 10.5% [71] of the pedodontists in the country, it was small study group, the participants were mostly from the central, southeast, and western regions of the country, and age distribution is not homogeneous, which may affect experience and preferences.
Conclusions
There is no compelling evidence to prove the absolute superiority of any irrigation solution, root canal paste, root canal length determination method, or file system in terms of deciduous tooth root canal treatment. We are of the opinion that keeping up to date with current information, technological advancements, and changes will increase the dentist’s chances of success in treatment as well as the patient’s comfort during treatment.
Tables
Table 1. Responses of the participants to the questions.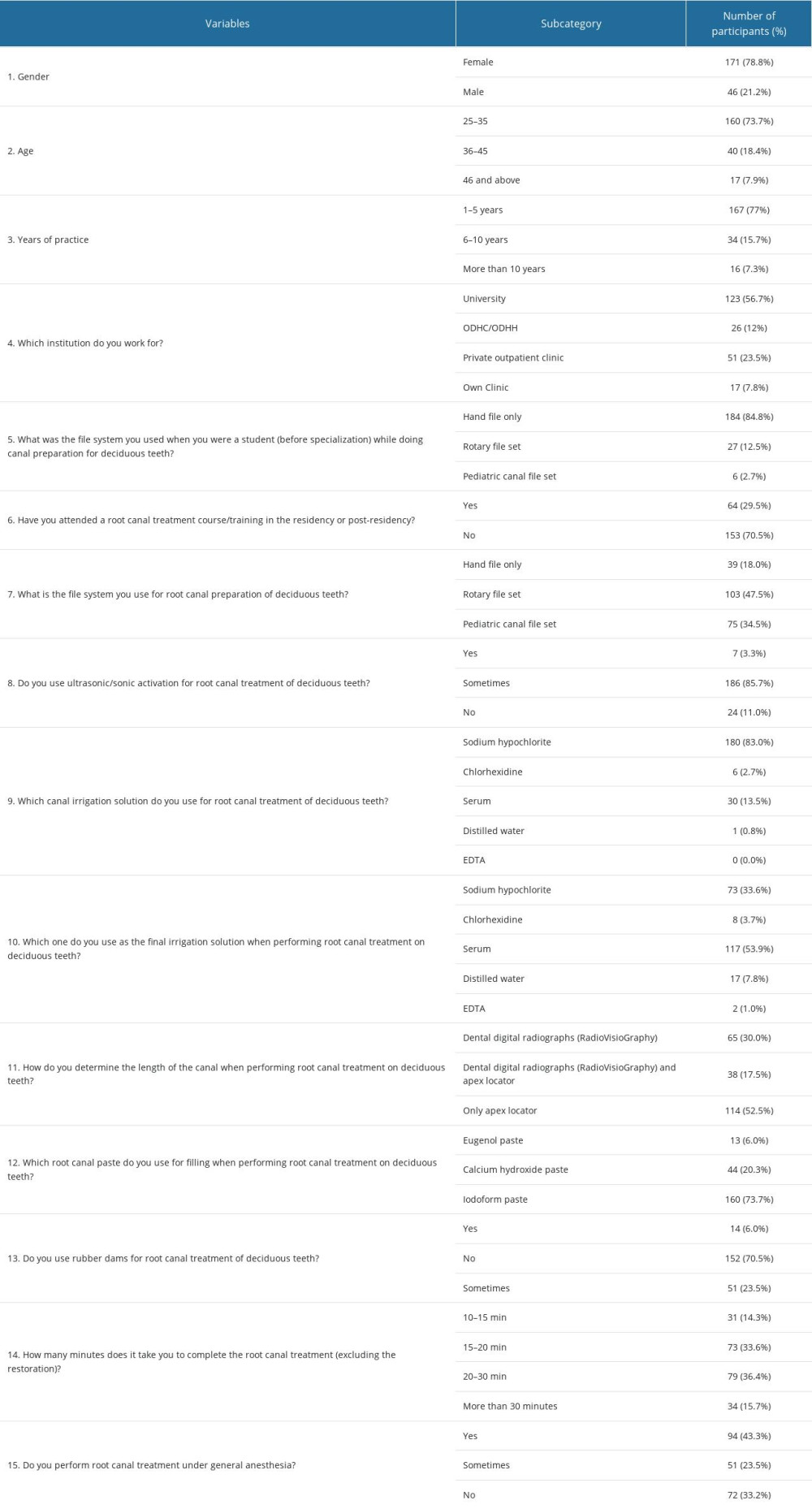 Table 2. Distribution of canal length determination technique preferences by institutions.
Table 2. Distribution of canal length determination technique preferences by institutions.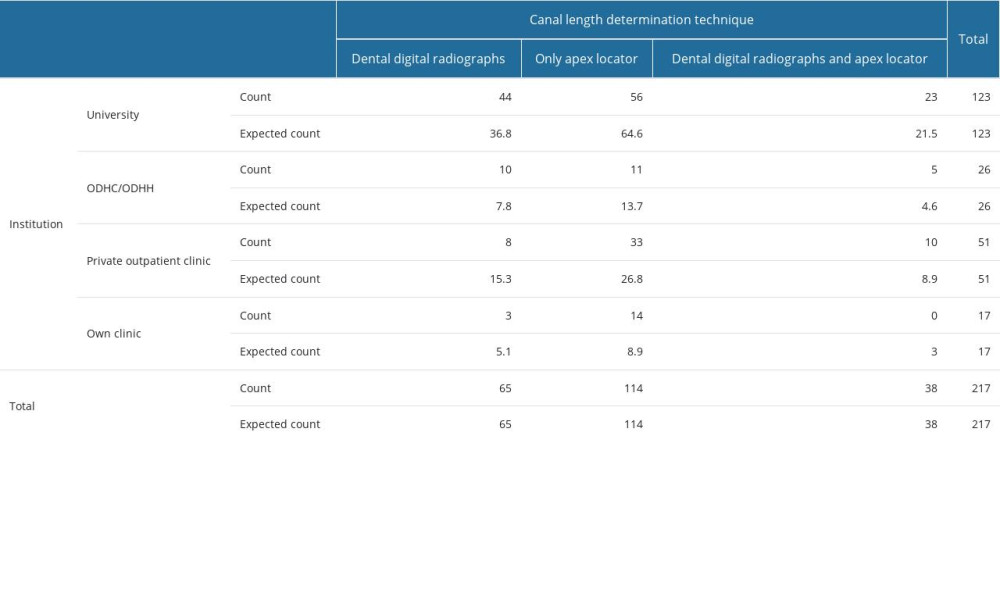 Table 3. Comparison of the file systems that the participants used when they were students and the file systems they currently use.
Table 3. Comparison of the file systems that the participants used when they were students and the file systems they currently use. Table 4. Comparison of the canal irrigation solution preferences of the participants with the final irrigation solution preferences.
Table 4. Comparison of the canal irrigation solution preferences of the participants with the final irrigation solution preferences.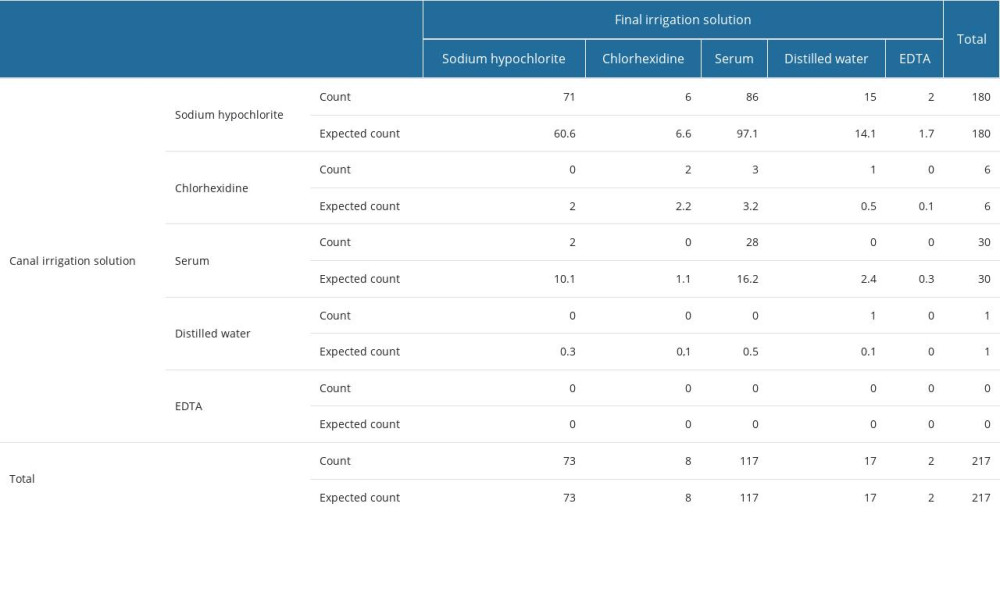
References
1. Fuks AB, Kupietzki A, Guelmann M, Pulp therapy for the primary dentition: Pediatric dentistry: Infancy through adolescence, 2013; 333-51, Elsevier Saunders Co.
2. Alkilzy M, Shaaban A, Altinawi M, Splieth ChH, Epidemiology and aetiology of malocclusion among Syrian paediatric patients: Euro J Paediatr Dent, 2007; 8(3); 131-35
3. George S, Anandaray S, Issac JS, Rotary endodontics in primary teeth – a review: Saudi Dental J, 2016; 28(1); 12-17
4. Asgary S, Fazlyab M, Endodontic management of an infected primary molar in a child with agenesis of the permanent premolar: Iran Endod J, 2017; 12(1); 119-22
5. Kirmizigül İ, Demir P, Usage of rotary instruments in root canal therapy of deciduous teeth-review: Cumhuriyet Dental Journal, 2019; 22(3); 351-57
6. Ng Y, Spratt D, Sriskantharajah S, Gulabivala K, Evaluation of protocols for field decontamination before bacterial sampling of root canals for contemporary microbiology techniques: J Endod, 2003; 29(5); 317-20
7. Ali A, Aslam A, Rehman B, Tariq A, Rubber dam use by general dental practitioners-prevalence and obstacles to its use: Pakistan Oral & Dental Journal, 2016; 36(3); 468-71
8. Zeren AE, Şaziye S, Süt dişlerinde kanal çalişma boyu ölçümünde kullanilan güncel yöntemler: Dijital radyografi ve elektronik apeks bulucular: Acta Odontologica Turcica, 2014; 31(1); 49-53
9. Zehnder M, Root canal irrigants: J Endod, 2006; 32(5); 389-98
10. Waterhouse PJ, Whitworth JM, Pediatric endodontics: Endodontic treatment for the primary and young permanent dentition: Cohen’s pathways of the pulp, 2016, Canada, Elsevier
11. Angker L, Swain MV, Kilpatrick N, Micro-mechanical characterisation of the properties of primary tooth dentine: J Dent, 2003; 31(4); 261-67
12. European Society of Endodontology, Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology: Int Endod J, 2006; 39(12); 921-30
13. Peters OA, Current challenges and concepts in the preparation of root canal systems: A review: J Endod, 2004; 30(8); 559-67
14. Canoglu H, Tekcicek MU, Cehreli ZC, Comparison of conventional, rotary, and ultrasonic preparation, different final irrigation regimens, and 2 sealers in primary molar root canal therapy: Pediatr Dent, 2006; 28(6); 518-23
15. Barr ES, Kleier DJ, Barr NV, Use of nickel-titanium rotary files for root canal preparation in primary teeth: Pediatr Dent, 2000; 21(7); 453-54
16. Katge F, Ghadge S, Poojari M, Comparative evaluation of cleaning efficacy of Prime Pedo™ and DXL-Pro™ Pedo rotary files with conventional h files in root canals of primary teeth: An in vitro study: Journal of Clinical & Diagnostic Research, 2019; 13(7); ZC06-09
17. Kuo C, Wang Y-L, Chang H, Application of Ni-Ti rotary files for pulpectomy in primary molars: Journal of Dental Sciences, 2006; 1(1); 10-15
18. Panchal V, Jeevanandan G, Subramanian E, Comparison of instrumentation time and obturation quality between hand K-file, H-files, and rotary Kedo-S in root canal treatment of primary teeth: A randomized controlled trial: J Indian Soc Pedod Prev Dent, 2019; 37(1); 75-79
19. Haapasalo M, Shen Y, Qian W, Gao Y, Irrigation in endodontics: Dental Clin North Am, 2010; 54(2); 291-312
20. Agrawal Vineet S, Rajesh M, Sonali K, Mukesh P, A contemporary overview of endodontic irrigants – a review: J Dent App, 2014; 1(6); 105-15
21. Hülsmann M, Heckendorff M, Lennon A, Chelating agents in root canal treatment: Mode of action and indications for their use: Int Endod J, 2003; 36(12); 810-30
22. Mancini M, Armelin E, Casaglia A, A comparative study of smear layer removal and erosion in apical intraradicular dentine with three irrigating solutions: A scanning electron microscopy evaluation: J Endod, 2009; 35(6); 900-3
23. Küçük M, Kermeoğlu F, Kalender A, Endodontide kullanilan güncel irrigasyon solüsyonlari, sistem ve cihazlari: Annals of Health Sciences Research, 2016; 5(1); 29-37
24. Ekim ŞA, Erdemir A, Endodontide irrigasyon aktivasyon yöntemleri: Atatürk Üniversitesi Diş Hekimliği Fakültesi Dergisi, 2015; 25; 98-104
25. Sari S, Okte Z, Success rate of Sealapex in root canal treatment for primary teeth: 3-year follow-up: Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2008; 105(4); e93-e96
26. Chen X, Liu X, Zhong J, Clinical and radiographic evaluation of pulpectomy in primary teeth: A 18-months clinical randomized controlled trial: Head Face Med, 2017; 13(1); 12
27. Nayak UA, Wadhwa S, Kasyap N, Knowledge and practice of, and attitudes toward, pulp therapy in deciduous teeth among pediatric dentists in India: J Investig Clin Dent, 2018; 9(1); e12284
28. Boreak N, Hanbashi A, Otayf H, Dentist’s attitudes, practice, and barriers toward the use of rubber dam during operative and endodontic treatments: An online questionnaire survey: World, 2021; 12(4); 306-10
29. Alqahtani SM, Chaturvedi S, Alshahrani AA, Online questionnaire-based study to evaluate the attitudes and use of rubber dental dams by Saudi dental practitioners: Med Sci Monit, 2023; 29; e938672
30. Marshall K, Page J, The use of rubber dam in the UK. A survey: Br Dent J, 1990; 169(9); 286-91
31. Angelis FD, D’Arcangelo C, Chella F, Patients’ attitude to rubber dam use: A questionnaire survey: Dental Cadmos, 2021; 89(01); 53-57
32. Stewardson D, McHugh E, Patients’ attitudes to rubber dam: Int Endod J, 2002; 35(10); 812-19
33. Vanhee T, Tassignon C, Porta P, Behavior of children during dental care with rubber dam or cotton roll isolation, a randomized study: Dent J (Basel), 2021; 9(8); 89
34. Pol S, Katge F, Krishna V, Effect of rubber dam on objective and subjective parameters of stress during dental treatment of children: Indian Journal of Oral Health and Research, 2018; 4(1); 16-20
35. American Academy of Pediatric Dentistry, Pulp therapy for primary and immature permanent teeth: The Reference Manual of Pediatric Dentistry, 2021; 399-407, Chicago, Ill., American Academy of Pediatric Dentistry
36. Shashirekha G, Jena A, Maity AB, Panda PK, Prevalence of rubber dam usage during endodontic procedure: A questionnaire survey: J Clin Diagn Res, 2014; 8(6); ZC01-3
37. Csinszka K-IA, Monea M, Pop M, Prevalence of rubber dam usage among dental practitioners and final year students in Tirgu Mures: A questionnaire survey: Acta Marisiensis-Seria Medica, 2015; 61(3); 188-91
38. Govindaraju L, Jeevanandan G, Subramanian E, Knowledge and practice of rotary instrumentation in primary teeth among indian dentists: A questionnaire survey: Journal of International Oral Health, 2017; 9(2); 45-48
39. Karthikeson P, Vignesh R, Knowledge and attitude of general dentists and dentists of other specialties toward endodontic treatment of primary teeth: Dru Inv Today, 2019; 11(6); 1372-77
40. Akshaya K, Ravindran V, Pandurangan SM, Pediatric dentists’ preference on usage of hand files or rotary files for pulpectomy of primary molars-a retrospective study: International Journal of Research in Pharmaceutical Sciences, 2020; 11(3); 1500-5
41. Lakshmanan L, Mani G, Jeevanandan G, Assessing the quality of root canal filling and instrumentation time using kedo-s files, reciprocating files and k-files: Brazilian Dental Science, 2020; 23(1); 7
42. Garg S, Dengree A, Namdev A, Namdev R, Kedo-SG pediatric rotary files: A boon for rotary endodontics in primary teeth: International Journal of Applied Dental Sciences, 2019; 5(3); 391-93
43. Bahrololoomi Z, Tabrizizadeh M, Salmani L, In vitro comparison of instrumentation time and cleaning capacity between rotary and manual preparation techniques in primary anterior teeth: Frontiers in Dentistry, 2007; 4(2); 59-62
44. Seraj B, Ramezani G, Ghadimi S, In-vitro comparison of instrumentation time and cleaning capacity between endodontic handpiece and manual preparation techniques in primary molar teeth: Minerva Stomatol, 2013; 62(1–2); 17-22
45. Mohamed RH, Abdelrahman AM, Sharaf AA, Evaluation of rotary file system (Kedo-S-Square) in root canal preparation of primary anterior teeth using cone beam computed tomography (CBCT)-in vitro study: BMC Oral Health, 2022; 22(1); 1-10
46. Ghadge S, Katge F, Poojari M, Clinical evaluation and comparison of obturation quality using pediatric rotary file, rotary endodontic file and H file in root canal of primary molars: a double blinded randomized controlled trial: International Journal of Research and Reports in Dentistry, 2020; 3(4); 12-19
47. Sharma S, Khanduja R, Masih U, Gupta S, Comparative evaluation of clinical and radiographical assessment of manual and rotary technique during pulpectomy procedure in primary teeth-In vivo study: JIDA: Journal of Indian Dental Association, 2019; 13(9); 25059
48. Bargale S, Padmanabh Davangere SK, Kariya PB, Knowledge, attitude, and practice regarding standardized treatment protocol for pulp therapy in deciduous dentition among general dental practitioners of Vadodara, Gujarat, India: J Indian Soc Pedod Prev Dent, 2019; 37(4); 327-32
49. Sruthi MA, Ravindran V, An observational study on the materials and techniques commonly adopted by pediatric dentists for single visit pulpectomy: International Journal of Research In Pharmaceutical Sciences, 2020; 11(3); 1574-80
50. Silva MF, Wambier LM, Gevert MV, Rodrigues Chibinski AC, Effectiveness of iodoform-based filling materials in root canal treatment of deciduous teeth: A systematic review and meta-analysis: Biomater Investig Dent, 2022; 9(1); 52-74
51. Najjar RS, Alamoudi NM, El-Housseiny AA, A comparison of calcium hydroxide/iodoform paste and zinc oxide eugenol as root filling materials for pulpectomy in primary teeth: A systematic review and meta-analysis: Clin Exp Dent Res, 2019; 5(3); 294-310
52. Meschi N, EzEldeen M, van Gorp G, Lambrechts P, Materials and clinical techniques for endodontic therapy of deciduous teeth: Endodontic Materials in Clinical Practice, 2021; 263-87
53. Fuks AB, Kupietzky A, Guelmann M, Pulp therapy for the primary dentition, in Pediatric dentistry: Elsevier, 2019; 329-351.e1
54. Ritwik P, A review of pulp therapy for primary and immature permanent teeth: J Calif Dent Assoc, 2013; 41(8); 585-95
55. Pandranki J, Vanga NR, Chandrabhatla SK, Zinc oxide eugenol and Endoflas pulpectomy in primary molars: 24-month clinical and radiographic evaluation: J Indian Soc Pedod Prev Dent, 2018; 36(2); 173-80
56. Chris Noel T, Vignesh R, Suresh V, Assessment of commonly used irrigants during pulpectomy in primary teeth in a hospital based setting - a retrospective study: International Journal of Research in Pharmaceutical Sciences, 2020; 11(SPL 3); 1587-91
57. Hatipoğlu FP, Hatipoğlu Ö, Aricioğlu B, Türk dişhekimlerinin endodontik tedavi prosedürlerindeki yaklaşimlarinin incelenmesi: Süleyman Demirel Üniversitesi Sağlik Bilimleri Dergisi, 2020; 11(1); 54-64
58. Basir L, Abdi R, Hashemi E, Cleaning efficacy of various root canal irrigants in primary teeth: A scanning electron microscopic study: Gen Dent, 2022; 70(5); 29-33
59. Camp J, Pediatric endodontics, endodontic treatment for the primary and young permanent dentition: Pathways of the Pulp, 2002; 833-39
60. Vitali FC, Santos PS, Cradoso M, Are electronic apex locators accurate in determining working length in primary teeth pulpectomies? A systematic review and meta-analysis of clinical studies: Int Endod J, 2022; 55(10); 989-1009
61. Shibin J, Prathima GS, Suganya M, Evaluation of the working length determination accuracy by cone-beam computed tomography in primary teeth: Int J Clin Pediat Dent, 2022; 15(Suppl 1); S92-96
62. Nellamakkada K, Patil SS, Kakanur M, A clinical evaluation of two electronic apex locators and conventional radiography in working length determination in primary molar and its influence on children’s behavioral responses: J Indian Soc Pedod Prev Dent, 2020; 38(2); 158-63
63. Patil PD, Katge AF, Rusawat DB, Knowledge and attitude of pediatric dentists, general dentists, postgraduates of pediatric dentistry, and dentists of other specialties toward the endodontic treatment of primary teeth: Journal of Orofacial Sciences, 2016; 8(2); 96-101
64. da Costa CC, Kunert GG, da Costa Filho LC, Kunert IR, Endodontics in primary molars using ultrasonic instrumentation: J Dent Child (Chic), 2008; 75(1); 20-23
65. Singh R, Barua P, Kumar M, Effect of ultrasonic instrumentation in treatment of primary molars: J Contemp Dent Pract, 2017; 18(9); 750-53
66. Alowi WA, Maganur PC, Manoharan V, Knowledge and practice of rotary instrumentation in primary teeth among Saudi Arabian dentists: A cross-sectional study: Int J of Clin Pediatr Dent, 2022; 15(Suppl 1); S97-S102
67. Kim I-H, Cho H, Song JS, Assessment of real-time active noise control devices in dental treatment conditions: Int J Environ Res Public Health, 2022; 19(15); 9417
68. Vitale MC, Gallo M, Pascadapoli M, Local anesthesia with SleeperOne S4 computerized device vs traditional syringe and perceived pain in pediatric patients: A randomized clinical trial: J Clin Pediatr Dent, 2023; 47(1); 82-90
69. Ramakrishnan M, Dhanalakshmi R, Subramanian E, Survival rate of different fixed posterior space maintainers used in paediatric dentistry – a systematic review: Saudi Dental J, 2019; 31(2); 165-72
70. Rapeepattana S, Thearmontree A, Suntornlohanakul S, Etiology of malocclusion and dominant orthodontic problems in mixed dentition: A cross-sectional study in a group of Thai children aged 8–9 years: J Int Soc Prev Community Dent, 2019; 9(4); 383-89
71. Canbulatel O: 31 bin 477 çocuğa 1 uzman diş hekimi (1 pediatric dentist for 31 thousand 477 children), 2016 [Accessed: 01.01.2023]; Available from: https://www.aa.com.tr/tr/saglik/31-bin-477-cocuga-1-uzman-dis-hekimi/514520
Tables
Table 1. Responses of the participants to the questions.Table 2. Distribution of canal length determination technique preferences by institutions.Table 3. Comparison of the file systems that the participants used when they were students and the file systems they currently use.Table 4. Comparison of the canal irrigation solution preferences of the participants with the final irrigation solution preferences.Table 1. Responses of the participants to the questions.Table 2. Distribution of canal length determination technique preferences by institutions.Table 3. Comparison of the file systems that the participants used when they were students and the file systems they currently use.Table 4. Comparison of the canal irrigation solution preferences of the participants with the final irrigation solution preferences. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387