20 December 2023: Clinical Research
High Prevalence of Musculoskeletal Disorders Among Dental Professionals: A Study on Ergonomics and Workload in Yemen
Basem H. Al-Huthaifi1ABCDEF, Mohammed M. Al MoaleemDOI: 10.12659/MSM.942294
Med Sci Monit 2023; 29:e942294






Abstract
BACKGROUND: Dentists frequently have work-related musculoskeletal disorder (MSD) diseases, which are the profession's second most common cause of disability. Awareness of dental ergonomics is necessary for controlling MSDs associated with dental workload. Dental professionals need additional training in dental ergonomics to reduce serious complications associated with dental workload. This questionnaire-based study aimed to evaluate the understanding of physical ergonomics and musculoskeletal disorders in 310 dental health professionals and students in Yemen.
MATERIAL AND METHODS: This was a cross-sectional study was conducted among 400 dental professionals working in various clinics and universities in Sana'a City, Yemen. They received a self-administered questionnaire that was developed from earlier studies. Five sections made up the questionnaire. The first section of the survey included questions about sex, age, and clinical professions; the second section focused on ergonomic awareness; the third section asked about work conditions; the fourth section asked about the prevalence of musculoskeletal disorders; and the fifth section asked about interventions used. Data were analyzed using SPSS version 25.0, and a P value of ≤0.05 was considered significant.
RESULTS: Only 310 questionnaires were completed. The participants'; level of understanding of ergonomics was low. One-way ANOVA showed a significant portion of respondents reported having MSDs, and they frequently reported pain related to workload. The neck, lower back, upper back, and shoulders experienced the highest levels of pain.
CONCLUSIONS: The prevalence of MSDs was high among dental professionals, especially in the lower back, upper back, and shoulder. This necessitates preventive measures like ergonomic positions, ergonomic equipment, regular exercise, and work breaks.
Keywords: Dentistry, ergonomics, musculoskeletal pain, Humans, Cross-Sectional Studies, Prevalence, Workload, Yemen, Musculoskeletal Diseases, Pain, Surveys and Questionnaires, Occupational Diseases, Dentists, Risk Factors
Background
Ergonomics is an applied science concerning employees and their relationship with their professional environment. It maintains the health of workers and improves their overall performance [1], and the application of ergonomics in dentistry can enhance optimum access and improve clinical practice [2].
The U.S. Centers for Disease Control and Prevention define musculoskeletal disorders (MSDs) as “injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs” [3]. MSDs are the most common causes of disability in occupations involving lifting, bending, twisting, sitting, or standing for long periods [3,4], particularly dentistry [4]. Dentists work while in uncomfortable positions, often moving their head forward and turning sideways with their arms drawn out from the body [5]. MSDs resulted in a 42.9% increase in disability from 1999 to 2010 [6].
Incorrect work posture and inappropriate position are the main causes of MS pain among dentists [7,8]. The risk of MSDs in dentistry can be minimized by applying ergonomic principles [1]. There is a strong association between physical ergonomics and MSDs and dental health professionals. Kumar et al reported that work-related MSDs and pain can be decreased through accurate operator-patient positioning, taking adequate breaks between patients, and preserving good physical health through standard exercises [9], and practitioners should improve their dental work environment [10]. Ergonomics should be involved in the dental educational system to decrease the risks of MSDs among dentists [11]. A recent review stated that in addition to ergonomic and socio-demographic characteristics, psychological factors can be involved, and this could have an impact on development of physical pain and MSDs [12].
The prevalence of work-related MSDs and their associated risk factors have been assessed in various countries, such as Taiwan [13], Iran [14], India [15], Brazil [16], and Australia [17], and the rates range from 40% to 70%. The rate in Poland is 60% [18], lower than that in Sweden (54%) [19] and slightly higher than that in Wales (64%) [20]. Other studies showed higher prevalence of MSDs in general practitioner dentists in Germany (95.8%) [21], Denmark (83%) [22], and Italy (91%) [23]. The global prevalence of MSDs in dental practitioners ranges from 64% to 93% [24]. Moreover, dental practice is highly challenging in terms of physical and mental status and related specialties [25].
A study showed that 90.2% of 184 subjects in the United Arab Emirates (UAE) had MSDs; the incidence of lower back pain increased with age and was associated with the amount of time spent with patients, whereas shoulder pain was strongly correlated with year of experience [26]. In 2022, Hussein et al found that dentists in the UAE had a similar percentage (90.4%) of work-related MSDs, but MSDs were linked to high levels of stress in the workplace. In general, pain in various body regions is linked to many factors, including gender, age, monthly income, job experience, number of patients treated each day, and use of an ergonomic dental chair [27]. Hamdan et al found that almost 50% of dental interns and students in Saudi Arabia (SA) had received instructions about preventing work-related MSDs, and 73% were aware of the risk of work-related MSDs but did not know about methods or therapies [28]. Nearly 78% of dentists in the Ha’il Region of SA reported having MSDs [29].
Nevertheless, no studies have investigated the prevalence and awareness of work-related MSDs in dental practitioners in Yemen. Therefore, this questionnaire-based study aimed to evaluate the understanding of physical ergonomics and musculoskeletal disorders in 310 dental health professionals in Yemen.
Material and Methods
STUDY DESIGN AND SAMPLE SIZE CALCULATION:
This study was approved by the Medical Ethics Committee of Dental Faculty in the University of Science and Technology, Sana’a, Yemen under number MEC/AD004 at 06/08/2023. This descriptive cross-sectional study was conducted on dental practitioners working in different dental clinics in Sana’a City, Yemen from January to February 2022, using a self-administered questionnaire. The study was conducted in accordance with the standards of the World Medical Association’s Declaration of Helsinki [30]. Additional details of the current study were discussed with the contributors before the distribution of questionnaires and collection of answers. All subjects signed a written consent. The study sample was determined according to the number of general practitioners in Sana’a City, Yemen. A population size of about 305 was verified using G*Power (http://www.gpower.hhu.de/en.html). The level of confidence was adjusted to 80%, and power was adjusted to 85%.
STUDY SETTING, STUDY CRITERIA, AND SUBJECTS:
To produce a homogeneous distribution, dentists were selected randomly from different parts of Sana’a City, Yemen. Participation was completely voluntary. A total of 400 questionnaires written in Arabic and English were distributed to different dental professionals. Male and female Yemeni dental practitioners were included in the study, but dental professionals with a history of orthopedic injury or congenital malformation (of the neck, back, or upper extremities) were excluded. A team composed of dental students was organized after they were trained. They served as investigators and distributed the questionnaires to the participants. After a brief explanation of the study, the respondents were given the questionnaire to complete under supervision of the investigators, who also collected informed consent forms and answered inquiries about the questions in the questionnaire.
QUESTIONNAIRE:
The questionnaire was self-administered and was distributed directly to the dentists, and the participants were required to complete it. The questionnaire was especially created for this study, and its content was validated on the basis of studies conducted in Asia [13–15], Europe [18–23], and Arab countries [26–29]. The questionnaire had 5 main sections and 22 questions, which were written in Arabic and English. It was the primary data collection instrument for the current study.
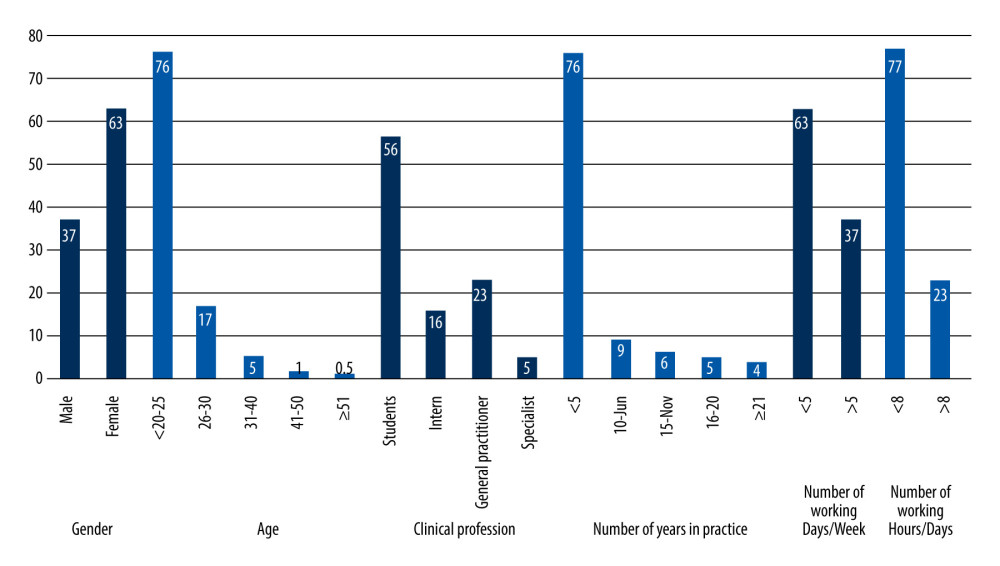
The first part of the questionnaire consisted of 6 questions related to the participants’ demographic characteristics and features: gender, age, clinical profession, year of practice, number of work hours per day and per week.
The second part was about awareness of ergonomics and its importance in dental practice. It consisted of 5 questions about the knowledge and application of dental ergonomics: Do you feel exhausted after work? Is dental work physically demanding? Can ergonomics enhance daily clinical dental performance? All the questions required a yes or no response. The third part contained 5 questions related to the work conditions: body position, presence of a dental assistant, number of patients treated per day, taking a break between patients, and the duration of this break.
The fourth part of the study was about the prevalence of MSD pain and its association with workload demand. It consisted of 4 questions about the presence or absence of pain, associated MSD pain before initiation of dental operation, associated MSD pain characteristics such as painful body site, and pain severity. The final part was about knowledge of participants regarding commonly used techniques to prevent MSDs. It included 2 questions: whether daily physical stretching exercises are performed, and techniques used to reduce MSD pain (physical activities, medications, or yoga).
DATA ANALYSIS AND INTERPRETATION:
SPSS version 25.0 was used to code data obtained from the surveys and conduct statistical analysis. Cronbach’s alpha was used to assess internal consistency of different sets of questions for each group, yielding a value of 0.7, which indicated an acceptable level. The normality test was applied for all parameters and showed that those parameters were normally distributed. Along with the percentage responses for each question, the overall response rate was computed using this database. Frequency analysis was used to assess the demographics and level of awareness and knowledge regarding dental ergonomics and MSDs associated with dental practice. One-way ANOVA was performed, and
Results
AWARENESS OF ERGONOMICS AND ITS IMPORTANCE IN DENTAL PRACTICE:
Table 1 shows the levels of awareness of ergonomics and its importance to dental practice. About 34% of the participants knew about ergonomics, and only 30% of the total had applied ergonomics to their dental practice. We found that 86% of respondents felt exhausted after clinical dental work and 87% thought that dental work is physically demanding and exhausting. Finally, 79% thought that ergonomics could improve their daily performance in dental clinics. No significant differences were found among variables (P values >0.050).
WORK CONDITIONS AND THE NUMBER IF TREATED PATIENTS:
Table 2 represents work conditions and the number of treated patients. Most dentists in the present study indicated that they preferred working sitting and standing, and 47.4% had worked with an assistant. Most participants (54.5%) reported that they did not take enough breaks between patients, and those who took breaks usually had taken less than 10-minute breaks between patients. No significant difference was found among these variables (P values >0.050). The survey found that 70.6% of dentists treated 1–3 patients per day, and 20.6% treated 4–6 per day (P=0.035).
PREVALENCE OF MSDS AND ITS ASSOCIATION WITH WORKLOAD:
The prevalence of MSDs and its association with workload demand are presented in Table 3. More than half of the participants (63.2%) experience no pain associated with the MS system before starting dental practice. Almost 73% experienced pain associated with the MS system and caused by dental workload, and pain was mostly experienced in the neck (57.33%), lower back (48.88%), and upper back (43.11%). Significant differences were observed, as indicated by P values of 0.049 and 0.028. Nearly 42% experienced mild pain.
COMMONLY USED PROPHYLACTIC REMEDIES TO AVOID MSDS:
Regarding questions that assessed the knowledge of participants regarding commonly used techniques to prevent MSDs, Table 4 shows that only 30% performed physical stretching activities. The commonly used techniques for treating or decreasing the symptoms of MSDs included physical activity (46%), analgesics (29%), yoga (6%), and other methods (18%). All parameters showed significant differences (P values of 0.034 and 0.048).
Discussion
To the best of our knowledge, this is the first study to investigate the association between ergonomics and MSDs in Yemeni dental professionals with a self-administered questionnaire. This type of questionnaire is a valid and reliable instrument for determining the prevalence of MSDs [13–15,18–23,26–29]. The occurrence of MSDs in Yemeni dental students has not been reported, and the incidence of work-related MS pain in dental students and the awareness of the great importance of ergonomics in the reduction of MSD have not been explored. Thus, this descriptive cross-sectional study was conducted to investigate the prevalence of MSDs and their association with dental ergonomics in Yemeni dentists and dental students.
Several factors contribute to the high prevalence of MSDs in dental professionals. The prevalence of work-related MSDs is higher in dentistry than in other occupations [27,31]. The increased use of heavy forces at work, long time spent in the same uncomfortable position, and static position are the main causes of MS problems [32–34]. However, the high risk of MSDs in dentistry may be decreased by applying ergonomic concepts [7].
Applying dental ergonomics is a crucial step in lowering the incidence of MSDs related to dental work. Using an ergonomic dental chair, having more years of experience, seeing more patients each day, and taking medication to treat work-related MSDs have significant associations with the number of affected body regions [27]. Another study reported that students who used an ergonomic dental chair adopted a better posture than those who used a traditional dental chair [35]. The present study revealed that the participants had a low level of awareness regarding the importance of ergonomics. About 34% of the participants knew ergonomics as a concept, and 30% used it in dental practice. This finding is inadequate compared with the findings of previous studies. A study in Riyadh, SA demonstrated that the participants’ levels of knowledge according to their job and profession were high overall and were higher in female dentists [7]. To prevent the emergence of subsequent issues, ergonomics is necessary and should be emphasized, and awareness of it should be increased as early as possible, particularly in dental students.
In the present study, 86% of the participants reported that they felt exhausted after work. Similarly, 87% believed that performing dental work is physically demanding and exhausting. This finding is consistent with a study showing that male and female dentists experience fatigue after a clinical workday [36,37].
In the current study, most dentists stated that they prefer working sitting and standing. This finding differed from that of a study showing that most dentists from various specializations prefer to sit rather than to stand when working [5,19]. The time spent by the dentist with each patient and taking insufficient breaks between appointments are strongly associated with MSDs. Al-Mohrej et al showed that performing dental work continuously for more than 2 hours without a break can cause neck and lower back pain [31]. Dental visits lasting 10–60 minutes accounted for over 90% of a dentist’s time [37], and the length of patient treatment time is strongly correlated with MSDs [38]. The present study showed that most participants reported that they did not take adequate breaks between patients. This situation may serve as a trigger for MSD development. Less than 10 minutes are often taken by those who take breaks between patients. A similar finding was reported by Chikumarn, who found that only 41.7% of dentists took a 5-minute break between patients [39].
About 73% of the participants experienced symptoms of MSDs during their practice for the last 12 months (Table 3). This rate was lower than the rates obtained in Germany (95.8%) [21], Italy (91%) [23], and the UAE (90.4%) [27], but lesser than the rates obtained in the UAE (48.5%) [26] and Taiwan (48.5%) [9]. Hashim et al and Aljanakh et al reported rates of 77.9% and 68.3%, respectively, and found that an association between the prevalence of MSD in during the 12 months of follow-up period [26,29].
In addition, Table 3 shows the percentages of MSD in the neck (57.33%), lower back (48.88%), and upper back (43.11%). Those findings were consistent with a study showing that the lower back, upper back, neck, and shoulder were the body parts most frequently affected by work-related MSDs [13–16,18,19,21–23,29]. Overloading of the spine during work can affect these body parts. Dentists frequently bow their heads and position their bodies awkwardly when they are seated. They may adopt improper positions when standing and twisting their lumbar spine. They may have neck pain because of a key etiological factor that involves prolonged static strain due to persistent muscular activation in the sternocleidomastoid or trapezius muscles [40]. A study found that 67% of participants had neck pain followed by lower back and shoulder pain [26]. The evidence presented above indicates that the neck, lower back, and shoulders are the body regions most commonly affected by work-related MSDs. A possible reason is the high workload placed on these body parts during intraoral operations, particularly when dentists sit with a tilted pelvis, a forward tilt of the neck, and an agitated repeated shoulder movement.
The muscles that were most affected by MSDs were in the neck, lower back, upper back, and shoulder in the present study. The prevalence of neck-related pain in the previous 12-month period in Yemeni dental practitioners was lower than that reported in Germany (78.4%) and SA (66.0%) [21,29], but was similar to that in the UAE (58.8%), Poland (56.3%), and Denmark (50.0%) [27,18,22] and higher than that in Italy (30.6%) and Brazil (15.7%) [23,16]. The prevalence of lower back pain in dental professionals was lower than that in SA (73.5%), Taiwan (66.0%), Poland (60.1%), and the UAE (55.4%) [29,13,18,27], but was considerably higher than in Brazil (15.7%). The prevalence of upper back pain was lower than that of neck and lower back pain in Yemeni dental practitioners, although similar percentages were recorded in dentists in Taiwan (45.0%) and Germany (42.2%) [13,21], and a higher percentage was reported in the UAE (28.4%) [27]. The prevalence of shoulder pain was lower than that of neck, lower back, and upper back pain in Yemeni dental practitioners; higher rates were recorded in dentists in Germany (66.2%), Taiwan (75.0%), the UAE (44.1%), and SA (43.3%) [21,13,26,29]. A lower percentage was reported in Brazil (12.7) [16], but similar percentages were recorded in Italy (25.0%) and Poland (27.2%) [18,23,14,19].
Finally, the lowest prevalence of MSDs was observed in the knees (4%), hips or thighs (7%), and feet or ankles (11%) in the current study. This finding was consistent with the findings of many studies worldwide. Table 5 shows the overall MSDs in relation to body region, country, and year of publication in dental practitioners in different countries and the results of the current study.
In this present study, most respondents engaged in physical stretching exercises to reduce symptoms. They believed that doing so might minimize the severity of symptoms. Others employed other techniques, including yoga and medication. This finding was comparable to the findings in SA [28,29]. Al Wazzan et al hypothesized that years of practice plays an important role in the occurrence of MSDs, although young and old dentists have reported the same symptoms [41]. Some participants often worked for over 8 hours a day (Figure 1). This practice causes the premature occurrence of MSDs. Madaan reported that 81% of dental students experienced MS pain [7], and Diaz-Caballero reported 80% of dental students attending clinical practice had muscular pain [8]. Our results agree with these findings. As many as 63% of the participants experienced pain related to the MS system before starting dental practice, and 73% experienced pain as a result of their workloads. The highest level of pain was experienced in the lower back, followed by the upper back and shoulders. Those findings were in line with the results of previous studies showing that shoulder and lower back pain are commonly reported in dental students [21–23,27,29].
The limitation of this study is the possibility of response bias because participants’ responses may not accurately represent their real actions. Hence, bias was minimized as much as possible. Moreover, the collected samples represented only 1 city, there was no comparison between genders, and most of our participants were students and had less than 5 years of clinical practice. We strongly recommend compliance with the instructions of ergonomics during preclinical and clinical teaching in undergraduate studies to minimize the prevalence of work-related MSDs.
Conclusions
The frequency of MSDs in Yemeni dentists and dental students was high, particularly in the lower back, upper back, and shoulder. Less than one-third of the participants used medication for MSDs pain. Thus, measures must be taken to prevent MSDs. These severe occupational health issues may be prevented by maintaining appropriate ergonomic positions, utilizing ergonomic equipment, taking adequate breaks, and exercising regularly.
Tables
Table 1. Awareness of ergonomics and its importance in dental practice (n=310).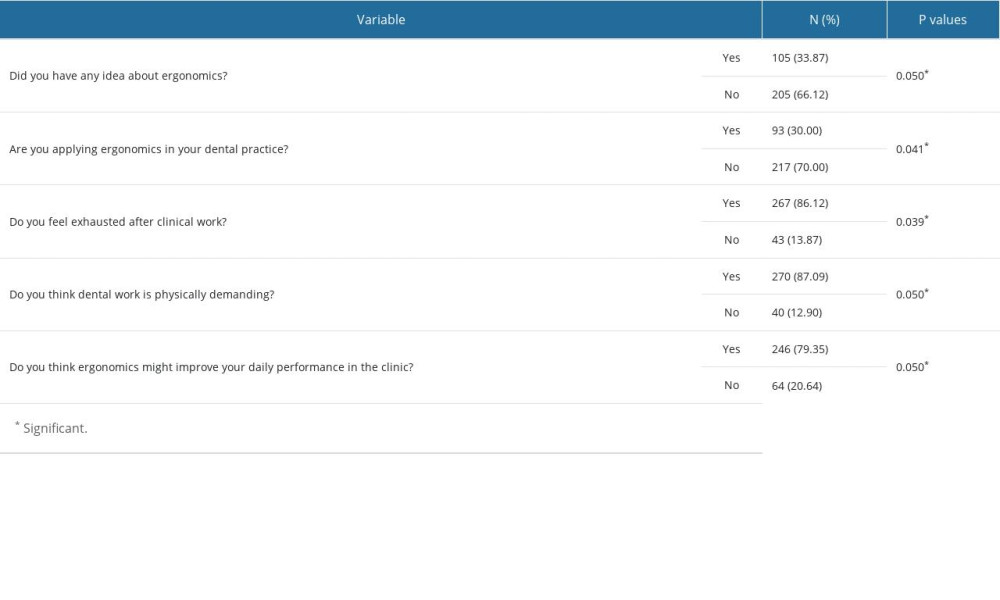 Table 2. Work conditions and the number of treated patients (n=310).
Table 2. Work conditions and the number of treated patients (n=310). Table 3. Prevalence of musculoskeletal disorders and their association with workload demand (n=310).
Table 3. Prevalence of musculoskeletal disorders and their association with workload demand (n=310).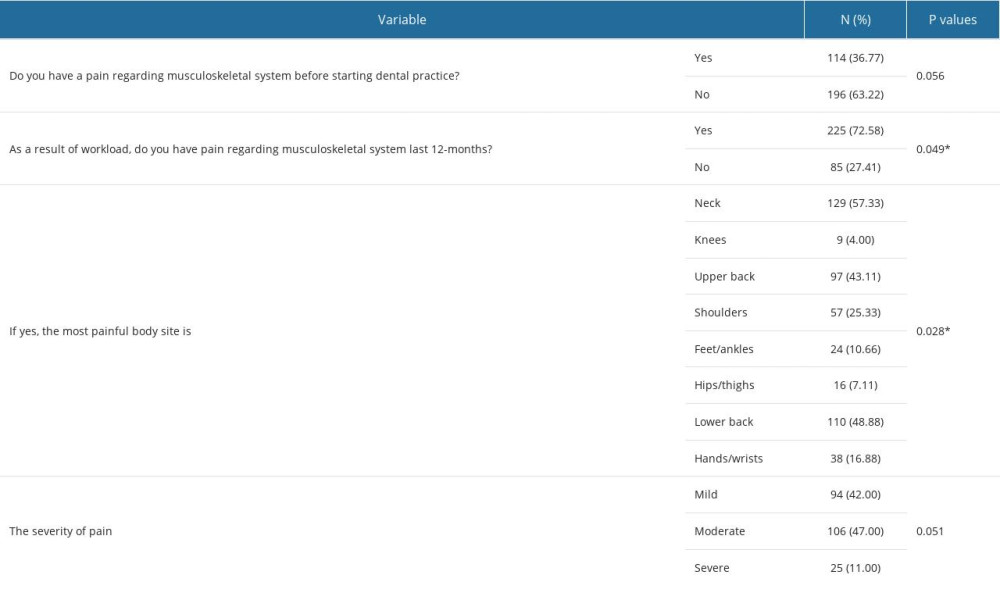 Table 4. Knowledge of participants regarding proper commonly used prophylactic remedies to avoid musculoskeletal disorders (n=310).
Table 4. Knowledge of participants regarding proper commonly used prophylactic remedies to avoid musculoskeletal disorders (n=310).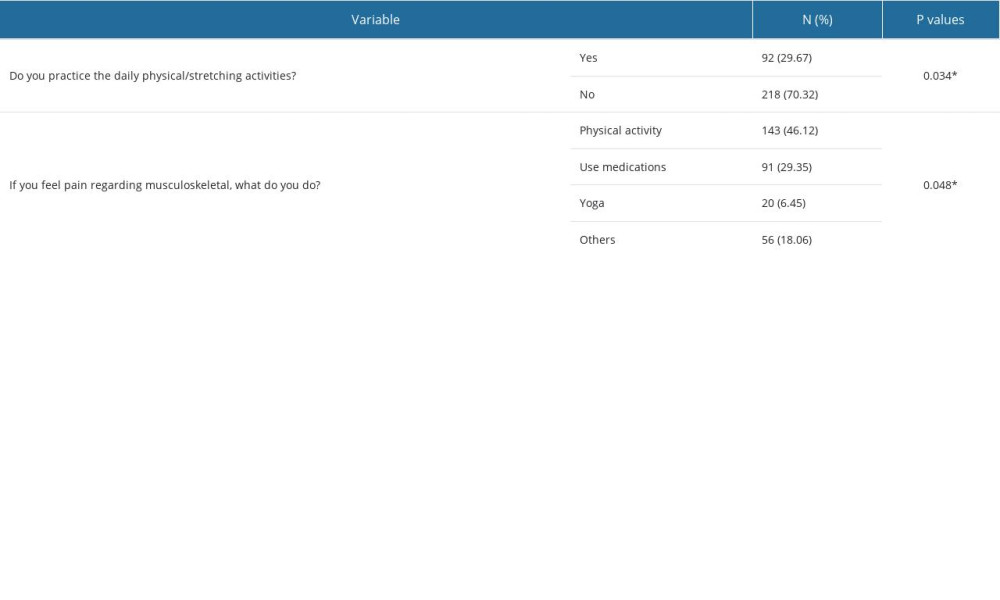 Table 5. Overall prevalence of musculoskeletal disorders among dental practitioners worldwide by body region, country, and year of publication.
Table 5. Overall prevalence of musculoskeletal disorders among dental practitioners worldwide by body region, country, and year of publication.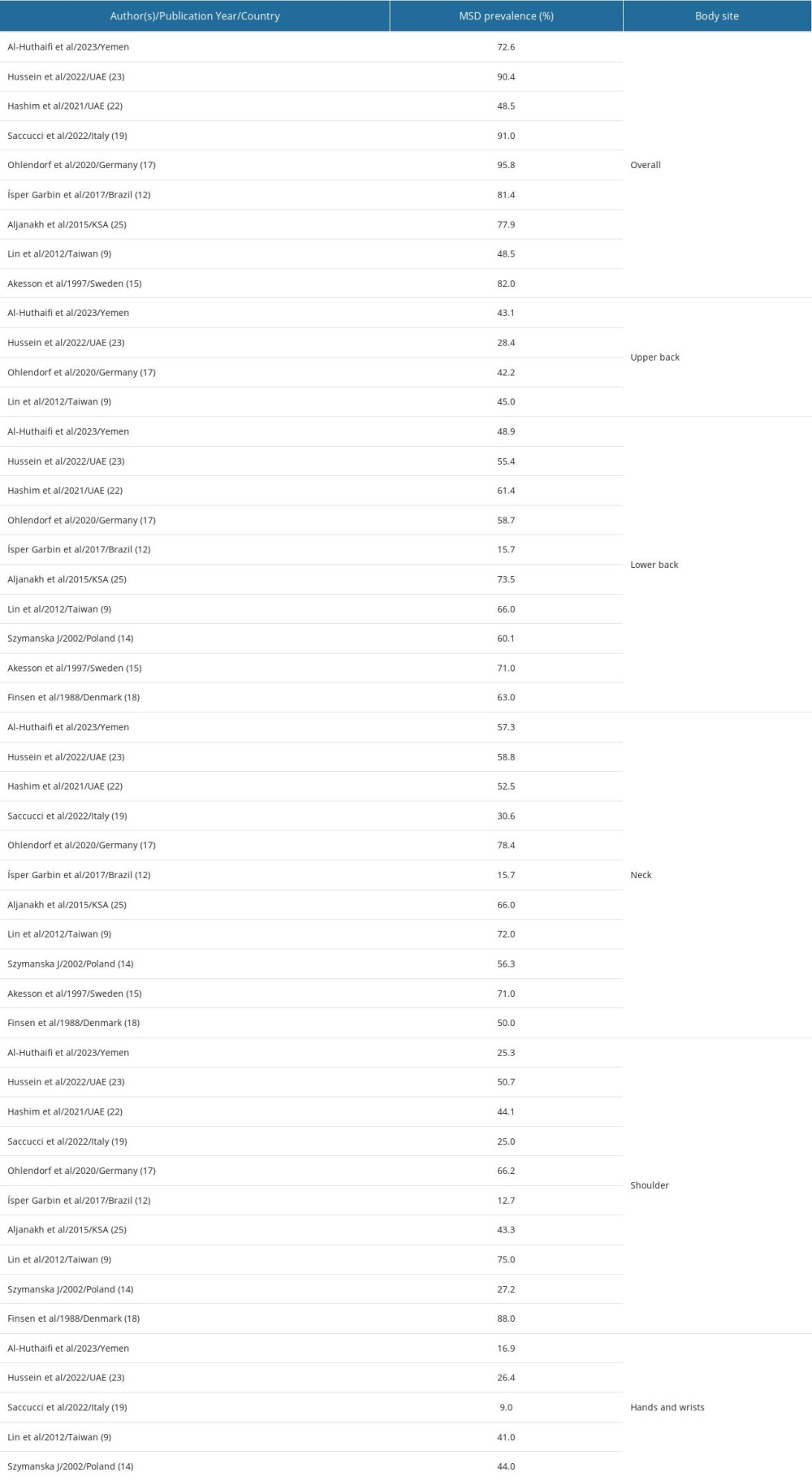
References
1. Movahhed T, Ajami B, Soltani M, Musculoskeletal pain reports among Mashhad dental students, Iran: Pak J Biol Sci, 2013; 16(2); 80-85
2. Pollack R, Dental office ergonomics: How to reduce stress factors and increase efficiency: J Can Dent Assoc, 1996; 62(6); 508-10
3. Central for Disease Control and Prevention: Work-related musculoskeletal disorders and ergonomics https//www.cdc.gov/workplacehealthpromotion/health-strategies/musculoskeletal-disorders/index.html
4. Alghadir A, Zafar H, Iqbal ZA, Work-related musculoskeletal disorders among dental professionals in Saudi Arabia: J Phys Ther Sci, 2015; 27(4); 1107-12
5. Alyahya F, Algarzaie K, Alsubeh Y, Khounganian R, Awareness of ergonomics & work-related musculoskeletal disorders among dental professionals and students in Riyadh, Saudi Arabia: J Phys Ther Sci, 2018; 30(6); 770-76
6. Vos T, Flaxman AD, Naghavi M, Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010: Lancet, 2012; 380(9859); 2163-96
7. Madaan V, Chaudhari A, Prevalence and risk factor associated with musculoskeletal pain among students of MGM Dental College: A cross-sectional survey: J Contemp Dent, 2012; 2(2); 22-27
8. Diaz-Caballero AJ, Gómez-Palencia IP, Díaz-Cárdenas S, Ergonomic factors that cause the presence of pain muscle in students of dentistry: Med Oral Patol Oral Cir Bucal, 2010; 15(6); e906-11
9. Kumar M, Pai KM, Vineetha R, Occupation-related musculoskeletal disorders among dental professionals: Med Pharm Rep, 2020; 93(4); 405-9
10. Gupta A, Bhat M, Mohammed T, Ergonomics in dentistry: Int J Clin Pediatr Dent, 2014; 7(1); 30-34
11. Gopinadh A, Devi KN, Chiramana S, Ergonomics and musculoskeletal disorder: As an occupational hazard in dentistry: J Contemp Dent Pract, 2013; 14(2); 299-303
12. Kawtharani AA, Chemeisani A, Salman F, Neck and musculoskeletal pain among dentists: A review of literature: Cureus, 2023; 15(1); e33609
13. Lin TH, Liu YC, Hsieh TY, Prevalence of and risk factors for musculoskeletal complaints among Taiwanese dentists: J Dent Sci, 2012; 7(1); 65-71
14. Borhan Haghighi A, Khosropanah H, Vahidnia F, Association of dental practice as a risk factor in the development of carpal tunnel syndrome: J Dent (Shiraz, Iran), 2013; 14(1); 37-40
15. Prasad DA, Appachu D, Kamath V, Prasad DK, Prevalence of low back pain and carpal tunnel syndrome among dental practitioners in Dakshina Kannada and Coorg District: Indian J Dent Res, 2017; 28(2); 126-32
16. Ísper Garbin AJ, Barreto Soares G, Moreira Arcieri R, Musculoskeletal disorders and perception of working conditions: A survey of Brazilian dentists in São Paulo: Int J Occup Med Environ Health, 2017; 30(3); 367-77
17. Sakzewski L, Naserud-Din S, Work-related musculoskeletal disorders in Australian dentists and orthodontists: Risk assessment and prevention: Work, 2015; 52(3); 559-79
18. Szymanska J, Disorders of the musculoskeletal system among dentists from the aspect of ergonomics and prophylaxis: Ann Agric Environ Med, 2002; 9(2); 169-73
19. Akesson I, Johnsson B, Rylander L, Musculoskeletal disorders among female dental personnel – clinical examination and a 5-year follow-up study of symptoms: Int Arch Occup Environ Health, 1999; 72(6); 395-403
20. Marshall ED, Duncombe LM, Robinson RQ, Kilbreath SL, Musculoskeletal symptoms in New South Wales dentists: Aust Dent J, 1997; 42(4); 240-46
21. Ohlendorf D, Naser A, Haas Y, Prevalence of musculoskeletal disorders among dentists and dental students in Germany: Int J Environ Res Public Health, 2020; 17(23); 8740
22. Finsen L, Christensen H, Bakke M, Musculoskeletal disorders among dentists and variation in dental work: Appl Ergon, 1998; 29(2); 119-25
23. Saccucci M, Zumbo G, Mercuri P, Musculoskeletal disorders related to dental hygienist profession: Int J Dent Hyg, 2022; 20(3); 571-79
24. Hayes M, Cockrell D, Smith DR, A systematic review of musculoskeletal disorders among dental professionals: Int J Dent Hyg, 2009; 7(3); 159-65
25. Halkai KR, Halkai R, Sulgante S, Work-related musculoskeletal disorders among dentists and their prevention through ergonomic interventions- a systematic review: Inte J Occup Safety Health, 2022; 12(2); 125-39
26. Hashim R, Salah A, Mayahi F, Haidary S, Prevalence of postural musculoskeletal symptoms among dental students in United Arab Emirates: BMC Musculoskelet Disord, 2021; 22; 30
27. Hussein A, Mando M, Radisauskas R, Work-related musculoskeletal disorders among dentists in the United Arab Emirates: A cross-sectional study: Medicina (Kaunas), 2022; 58(12); 1744
28. Hamdan HM, Saudi dental graduates educational experiences and awareness about work-related musculoskeletal disorders prevention: J Res Med Dent Sci, 2021; 9(8); 361-66
29. Aljanakh M, Shaikh S, Siddiqui AA, Prevalence of musculoskeletal disorders among dentists in the Ha’il Region of Saudi Arabia: Ann Saudi Med, 2015; 35(6); 456-61
30. Ploicy WMA: WMA declaration of Helsinki-ethical principles for medical research involving human subjects, 2013, Brazil, World Medical Association https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/
31. Al-Mohrej OA, Al-Kenani NS, Chronic ankle instability: Current perspectives: Avicenna J Med, 2016; 6(4); 103-8
32. Pandis N, Pandis BD, Pandis V, Eliades T, Occupational hazards in orthodontics: A review of risks and associated pathology: Am J Orthod Dentofacial Orthop, 2007; 132(3); 280-92
33. Morse T, Bruneau H, Dussetschleger J, Musculoskeletal disorders of the neck and shoulder in the dental professions: Work, 2010; 35(4); 419-29
34. Melis M, Abou-Atme YS, Cottogno L, Pittau R, Upper body musculoskeletal symptoms in Sardinian dental students: J Can Dent Assoc, 2004; 70(5); 306-10
35. Gandavadi A, Ramsay JR, Burke FJ, Assessment of dental student posture in two seating conditions using RULA methodology – a pilot study: Br Dent J, 2007; 203(10); 601-5
36. Alexopoulos EC, Stathi IC, Charizani F, Prevalence of musculoskeletal disorders in dentists: BMC Musculoskelet Disord, 2004; 5; 16
37. Feng B, Liang Q, Wang Y, Prevalence of work-related musculoskeletal symptoms of the neck and upper extremity among dentists in China: BMJ Open, 2014; 4(12); e006451
38. Ylipaa V, Arnetz BB, Benko SS, Physical and psychosocial work environments among Swedish dental hygienists: Risk indicators for musculoskeletal complaints: Swed Dent J, 1997; 21; 111-20
39. Chaikumarn M, Working conditions and dentists’ attitude towards proprioceptive derivation: Int J Occup Saf Ergon, 2004; 10(2); 137-46
40. Heng W, Wei F, Liu Z, Physical exercise improved muscle strength and pain on neck and shoulder in military pilots: Front Physiol, 2022; 13; 973304
41. Al Wazzan KA, Almas K, Al Shethri SE, Al-Qahtani MQ, Back and neck problems among dentists and dental auxiliaries: J Contemp Dent Pract, 2001; 2(3); 17-30
Tables
Table 1. Awareness of ergonomics and its importance in dental practice (n=310).Table 2. Work conditions and the number of treated patients (n=310).Table 3. Prevalence of musculoskeletal disorders and their association with workload demand (n=310).Table 4. Knowledge of participants regarding proper commonly used prophylactic remedies to avoid musculoskeletal disorders (n=310).Table 5. Overall prevalence of musculoskeletal disorders among dental practitioners worldwide by body region, country, and year of publication.Table 1. Awareness of ergonomics and its importance in dental practice (n=310).Table 2. Work conditions and the number of treated patients (n=310).Table 3. Prevalence of musculoskeletal disorders and their association with workload demand (n=310).Table 4. Knowledge of participants regarding proper commonly used prophylactic remedies to avoid musculoskeletal disorders (n=310).Table 5. Overall prevalence of musculoskeletal disorders among dental practitioners worldwide by body region, country, and year of publication. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387