16 November 2024: Review Articles
Surgical Advances in the Treatment of Acromioclavicular Joint Injury: A Comprehensive Review
Yingkai Ma1BC, Zhenwen Ma2EG, Jiangrong Guo1DE, Xinnan Ma1A, Songcen LV1BC, Shi Cheng1EF*DOI: 10.12659/MSM.942969
Med Sci Monit 2024; 30:e942969






Abstract
ABSTRACT: In this article, we aim to review the diagnosis, classification, and treatment of acromioclavicular joint injury by mainly describing the progress of surgical treatment for acromioclavicular joint injury, providing a reference for clinical diagnosis and treatment. Acromioclavicular joint injury is a common sports injury, which is more common in male than in female patients. The mechanism of the injury is mainly caused by direct or indirect violence, which can be clearly diagnosed by radiography. According to the time after injury, it can be divided into acute injury and chronic injury. The Rockwood classification is the most commonly used classification in research. For Rockwood types V to VI, we treat with surgery, while the treatment options for type III are controversial and no consensus has been reached. Surgical treatment can be divided into open surgery and shoulder arthroscopy. The methods of open surgery can be divided into 3 categories: direct acromioclavicular joint fixation, coracoclavicular space suspension device fixation, and coracoclavicular ligament reconstruction. The shoulder arthroscopy method involves reconstruction of the coracoclavicular ligament under arthroscopy, combined with suture-button suspension fixation. For patients with Rockwood classification III and IV-VI, who have significant movement needs, surgery is the preferred treatment for acute acromioclavicular dislocation within 3 weeks. For patients with a chronic acromioclavicular dislocation or who do not respond to nonsurgical treatment, it is recommended to use wire suspension fixation combined with ligament to repair the damage. This article aims to review advances in the management of acromioclavicular joint injury.
Keywords: Acromioclavicular Joint, Anatomy, Diagnosis, Classification, Therapeutics, Humans, Arthroscopy, Male, Female
Introduction
The acromioclavicular (AC) joint is an articulation connecting the distal end of the clavicle with the acromion that plays a pivotal role in shoulder movement. Injuries to the AC joint are prevalent among athletes and the younger population, accounting for over 40% of all shoulder injuries [1,2]. Annually, there are 9.2 cases per 1000 individuals [1]. Most of those affected are between the ages of 20 and 40, with the incidence rate in male patients being 5 to 10 times higher than that in female patients [1,3]. This discrepancy in incidence rates may be attributed to males engaging in high-risk sports. While minor injuries are often not associated with significant long-term morbidity, more severe grades can lead to considerable loss of shoulder strength and function [1,3]. To date, there is an ongoing debate regarding the most effective treatment approach for AC joint injuries, including the necessity of surgery and the optimal surgical technique. In this article, we seek to explore recent advancements in the management of AC joint injuries.
Anatomy
The distal clavicle and the acromion form the AC joint. On the surface of the joint is hyaline cartilage, and within the joint are fibrous disks capable of horizontal sliding and rotation, which gradually denature with age [4]. The primary function of the AC joint is to provide an expanded range of scapulothoracic rotation for the scapula, facilitating the adjustment of the scapula to conform to the thorax during arm movements. Additionally, it enables the transmission of force from the upper extremities to the clavicle, serving as a crucial junction for upper body mechanics and stability [5]. Complexes of the joint capsule, AC ligament, and coracoclavicular (CC) ligament are required for the stability of the AC joint. The AC joint capsule is extremely thin and surrounded by the AC ligament, which consists of the anterior, posterior, upper, and lower parts. The primary role of the 2 sections is to resist the horizontal movement force of the AC joint and to control the axial torsion force of the clavicle in a posterior direction [6]. The CC ligament is composed of conus ligaments and trapezoid ligaments, which are located anteromaterally and posterolaterally. These ligamentous elements offer static support to prevent anterior movement of the AC joint and maintain the joint’s vertical stability. The trapezoidal ligament serves as the primary function [7]. This ligament complex controls the rotational stability of the clavicle, as well as the stability of the lifting and contraction of the scapula [8].
Injury Mechanism and Classification
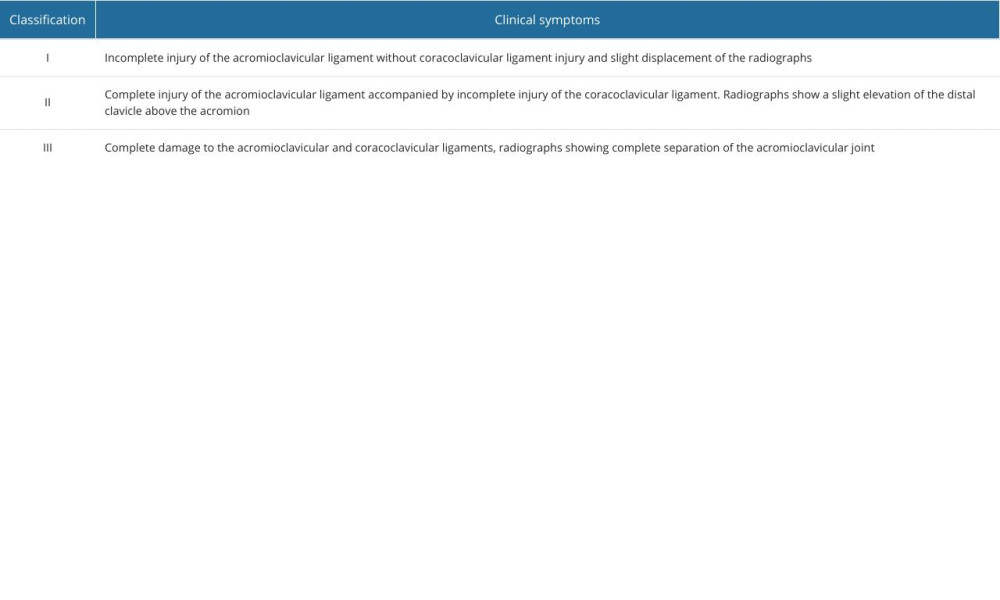
Direct or indirect violent trauma is the main cause of AC joint injury, and direct violent trauma is the most frequent factor. Indirect injuries typically have a relationship to the site of the injury, where the sternoclavicular joint transmits force to the AC joint, end of the clavicle, and nearby supporting ligaments, injuring the AC ligament and CC ligament [9]. The AC ligament is more susceptible to injury because the CC ligament has a broader range of motion than the AC ligament and can endure a wide range of movement [10]. Tossy et al [11] first presented the categorization of AC joint damage in 1963 (Table 1). Currently, the most popular classification is the Rockwood classification, a 6-type classification created in 1984 by Professor Rockwood based on the refinement of the original Tossy classification [12]. The displacement of the damaged shoulder joint was characterized after comparison with the contralateral shoulder joint and categorized based on anteroposterior X-ray imaging of the shoulder joint [13] (Table 2). Currently, the Rockwood categorization is frequently used as a therapy guide. The following is a detailed introduction to Rockwood classification: type I: AC ligament sprain with intact CC ligaments, stable AC joint, normal X-ray findings, and magnetic resonance imaging can show signs of AC joint sprain; type II: complete rupture of the AC ligament, damage to the CC ligaments, subluxation of the AC joint, and X-ray shows an increase in the acromial space less than 25% of normal; type III: complete rupture of both AC and CC ligaments, complete dislocation of the AC joint, and X-ray shows an increase in the acromial space between 25% and 100% of normal; type IV: complete rupture of both AC and CC ligaments, with posterior displacement of the distal clavicle, even penetrating into the trapezius muscle and fixed within it; type V: complete rupture of both AC and CC ligaments, and X-ray shows an increase in the acromial space between 100% and 300% of normal, with the clavicle located subcutaneously; and type VI: complete dislocation of the AC joint, and complete rupture of both AC and CC ligaments, with distal clavicle displacement to the coracoid process.
Diagnosis
Injuries to the AC joint are primarily diagnosed with X-rays, although magnetic resonance imaging can also be used. X-ray images are used to classify AC joint injuries according to the Rockwood classification [14] (Figure 1). If a Rockwood type III injury is detected, additional testing and treatment options are necessary [15].
Bontempo et al used the Zanca posture to acquire X-ray images of the AC joint in order to assess the degree of injury to the AC joint [16]. The AC joint is shot at 10 to 15 degrees from the shoulder joint’s horizontal surface in the Zanca position photography [16]. Alexander et al used Y-position shoulder joint X-ray to assess the distance between the clavicle and coracoidclavicle on both sides of the shoulder joint in order to identify AC joint damage [17].
Barnes et al [18] reported the use of cross-thoracic adduction radiographs, also known as the Basamania position, to assess AC joint stability in patients with suspected Rockwood type III injury. The International Society of Arthroscopy and Knee Surgery classified Rockwood type III injuries as IIIA and IIIB [19]. The Rockwood classification has been the standard for classifying and managing AC joint injuries; however, it has limitations. In clinical practice, the association between injury type and pain, range of motion, and functionality is low, and Rockwood categorization is more dependent on X-rays.
Choice of Treatment
Weinstein et al [20] concluded that the 3 weeks following an AC ligament injury is the most important time for recovery. If the AC and CC ligaments do not mend biologically, the displaced joint will have inadequate mechanical stability. Acute AC joint injury is defined as occurring within 3 weeks, and chronic AC joint injury is described as occurring over 6 weeks [21]. There is no consensus regarding the optimal time for surgery. Some evidence supports surgical treatment at an early stage. Rolf et al compared the effects of early surgery with those of delayed surgery in terms of Constant score, surgical effect, patient satisfaction, and complications and concluded that early surgery has a superior effect [22]. In a study comparing early and late AC joint dislocation, Song et al [23] concluded that the efficacy of early surgery was superior to that of delayed surgery. However, Krul et al reported that 21 patients with Rockwood type V were treated nonsurgically, and 11 of the 18 patients that were followed up for 90 days achieved good clinical outcomes and were able to move freely without any restrictions, for a 61% success rate. Consequently, nonsurgical treatment can be used initially [24]. Consequently, high-quality randomized controlled studies are still required to establish the optimal time of surgery.
Currently, most research concludes that nonsurgical treatment is suggested for Rockwood types I–II, surgical treatment is necessary for Rockwood types IV–VI, and the treatment of Rockwood type III is contentious [25]. According to one study, nonsurgical therapy of acute Rockwood type V injuries can recover normal movement [24]. Consequently, there is no consensus about the surgical procedures and timing of various types of injuries [4].
According to The International Society of Arthroscopy and Knee Surgery, type IIIA damage is a stable harm, whereas type IIIB is unstable damage that can progress to type V [19]. The lack of consensus regarding the management of Rockwood type III is due to the preference for surgical treatment during the acute phase (<3 weeks) or nonsurgical treatment for 12 weeks. According to the findings of Schlegel et al [26], 80% of AC joint injuries treated nonsurgically can achieve good clinical outcomes and patients can return to normal activities. Similarly, Ceccarelli et al [27] believed that surgical treatment of type III AC dislocation is required only if nonsurgical treatment is inadequate and favorable results are also possible. Nevertheless, other researchers suggest that the treatment effect of chronic injury may be inferior to that of acute injury [28]. Korsten et al [29] believe that the influence of a patient’s lifestyle and exercise requirements should be considered, and that patients with a high level of exercise and demand should be treated with early surgery. To participate in shoulder-related activities, such as push-ups and bench presses, it is necessary to undergo surgery as soon as feasible [30]. Therefore, the Rockwood type III injury should be treated by evaluating the AC joint’s stability and the patient’s functional needs [29].
Conservative Treatment
Nonsurgical treatment treatments consist of pain management, ice therapy, and brace and sling protection. The duration of protection is between 6 and 12 weeks.
Surgical Treatment
Surgical treatment of AC dislocation can be divided into 3 types. The first type is the direct fixation of the AC joint, represented by Kirschner wire fixation, and later the clavicular plate fixation with hook. The second type is fixation of the CC ligament, which is represented by the earliest Bosworth screw. In addition, there is the TightRope loop fixation with titanium plate [31]. The third type is ligament reconstruction technology, which is represented by the earliest reconstruction of the CC ligament by the Weaver-Dunn method. Additional methods include ligament insertion anatomical reconstruction, autologous tendon transplantation reconstruction, and artificial ligament reconstruction.
Direct Fixation of the AC Joint
Kirschner wire fixation of AC joint is now not commonly used. The Kirschner wire is passed between the acromion of the scapula and the distal clavicle, when it is used for fixation. To prevent proximal movement of the fixation, the later end of the Kirschner wire is partially left outside the skin. All postoperative patients are bandaged for 3 weeks at the shoulder joint. They can begin vertical wall climbing on the first day following surgery, and after 3 weeks they can begin active and passive activities. Six weeks following surgery, the abductive shoulder joint reaches 90 degrees, and the shoulder joint is removed 6 weeks after Kirschner wire fixation [32].
Kaiser et al [33] were the first to report the treatment of AC dislocation with clavicular hook plate fixation technology and the restoration of the CC ligament with surgical sutures. Mlasowsky et al conducted a follow-up study of 39 out of 54 cases of AC dislocation treated with clavicular hook plate for an average of 34 months; 35 patients had no postoperative complications and limited joint mobility, while the remaining patients experienced only discomfort in the shoulder region when holding heavy objects and during weather changes [34]. Kezunovic et al compared the clinical efficacy of hooked plate fixation and Bosworth screw fixation and found that hooked plate fixation had a lower incidence of postoperative adverse reactions, greater patient satisfaction, and higher Constant score. They also discovered that its postoperative effect was superior than that of Bosworth screw fixation [35]. This difference, however, lessens over time. To prevent subacromial impingement following internal fixation, it is suggested that the hook plate be removed after 3 months [36]. Compared with the loop suspension fixation approach, the clavicular hook plate fixation technique results in less postoperative pain and a low incidence of complications [37].
CC Ligament Fixation
Bosworth screws are regarded as a viable approach for the fixation of grade III, IV, and V injuries due to their fast operation time and good fixation. The AC interjoint region is cleaned, the injured CC ligament is repaired with No. 2 non-absorbable suture, the AC joint is reduced, and a tunnel is created between the clavicular and coracoid process. The guide wire penetrates half of the coracoid cortex. The Bosworth screw penetrates the double coracoid cortex, and pressure is applied. The reduced clavicle position is maintained. After 10 weeks of screw fixation, the screw is removed under local anesthetic. After removing the external fixation, a 90-degree exercise can be done [32]. Ammon et al studied this technique from a biomechanical standpoint, and their research showed that the titanium Bosworth screw’s fixation strength was comparable to that of the complete AC ligament [38]. A clinical study, with an average follow-up period of 8 years, revealed that the Bosworth screw technique was superior to small-incision Kirschner wire fixation in terms of fixation strength, reduction effect, pain relief, infection rate in early and late postoperative wounds, and the treatment effect of AC joint dislocation [32].
The first obvious advantages of Endobutton suspension fixation in the treatment of AC joint injury are that the incision is small and the internal fixation need not be removed. Mori et al reported the use of an Endobutton with a single tunnel for the restoration of the CC ligament in the treatment of acute AC joint dislocation. Good follow-up results were observed after 10 years of treatment, and the fracture risk caused by many tunnels was minimized [39].
Mori’s surgical procedure is roughly as follows: After receiving anesthesia, the patient assumes the beach chair position, a 3-cm incision is created inside the AC joint, and the incision is then directed toward the coracoid process. The trapezius muscle and deltoid muscle fascia are opened, and the deltoid muscle is separated from the anterior clavicle. The surgeon confirms the ligament injury in the coracoid process region. With a 3.5-mm hollow drill, the coracoid process is drilled through the cortex, and a 4.5-mm drill is used to drill through the coracoid process. Coracoid process fractures are avoided with caution. The traction suture guides the Endobutton through the coracoid process tunnel, after which the Endobutton is flipped linearly, the AC joint is anatomically reduced, and both ends of the ligament are pulled vertically to determine the optimal position of the clavicular tunnel at 25 mm inside the lateral end of the clavicle. A 3.5-mm clavicular tunnel is created, and another Endobutton is inserted into the tail line. The AC joint is reduced and stabilized in a surgical knot, and the stability is evaluated by passively moving the shoulder joint. The injured CC ligament can be repaired if necessary with a 2-0 suture (Figure 2) [39].
In addition, Menge et al used a fixed tightrope device to avoid the irritation of knotting and fixation. Tendon grafts around the clavicle and coracoid process is done in lieu of bone tunnel fixation, which uses a smaller bone tunnel and can reduce fracture risk while achieving good initial stability [40].
Wu et al described in detail the surgical approach of using the TightRope device for the fixation of acute AC joint dislocation and performed a comparative study with the use of Endobutton fixation technology. The results demonstrated that the symptoms of both groups were alleviated and the curative efficacy was satisfactory; however, there were no postoperative problems in TightRope group. In addition, the Endobutton group had the benefits of a small incision, quick duration, and less blood loss [41].
CC Ligament Reconstruction Technique
Recent research suggests that anatomical repair of the CC ligament is the most effective method for restoring normal CC and AC ligaments [42]. However, it is difficult to determine the exact anatomical restoration of the AC ligament. According to studies, restoration of the CC ligament using soft-tissue tendons yields superior biomechanical outcomes [43].
Weaver and Dunn were the first to describe the Weaver-Dunn reconstruction technique, which involves the transposition of the coracoshoulder ligament to the distal clavicle and the distal clavicular resection [44]. Rauschning et al [45] conducted a follow-up analysis on 18 patients who underwent Weaver-Dunn surgery, demonstrating its clinical efficacy. Kawabe et al successfully treated 41 patients with Rockwood III AC dislocation with Weaver-Dunn surgery [46]. This approach is now used less frequently.
In acute and chronic AC joint dislocation, hamstring tendons are routinely used as simple tendon grafts. The repair of the chronic AC joint damage with autologous tendon transplantation has more benefits, as it can promote healing and enhance biological stability [47]. According to studies [43,48], the biomechanical strength of free-tendon transplantation is superior to that of Weaver-Dunn surgery. It is similar to the biomechanical strength of suture-button suspension fixation [47]. Wang et al reported the treatment of AC joint dislocation by the reconstruction of the AC ligament and CC ligament with tendon transplantation and compared the treatment of the AC joint with hook-plate fixation and tendon transplantation fixation, concluding that there was no statistically significant difference between the two [49]. However, using tendons to repair ligaments requires a second operation to remove the internal fixator. In the surgical procedure used by Wang et al to reconstruct ligaments associated with AC joint dislocation with tendons, the front of the shoulder enters the medial side of the AC joint from the coracoid process, the deltoid muscle is opened, the clavicle, AC joint, and coracoid process are peeled off, and during the procedure, after confirming the ligament injury, a soft-tissue tunnel is created around the coracoid process, and the AC joint is reduced and temporarily maintained. A bone tunnel is created 20 mm and 40 mm from the distal clavicle, which are the attachment locations of the trapezoidal and conical ligaments. The trapezoidal ligament insertion tunnel diameter is 4.0 mm, the conical ligament insertion tunnel diameter is 3.5 mm, and a 3.5-mm tunnel is established at the AC insertion 15 mm from the AC joint. The transplanted tendon is bathed in antibiotics for 30 min. The prepared tendon enters at A, encircles the coracoid process, passes through the tunnel B, passes supraclavicular through the acromion tunnel C, loops back under the clavicle, passes back through the mouth B, ties the 2 tail ends together, and then fixes the tendon’s end with non-absorbable sutures while maintaining maximum tension. The trapezius and deltoid fascia are restored, and incisions are closed [49].
Millett et al considered that the use of tendon transplantation alone to repair the CC ligament would result in the failure of AC joint reduction after a long term. Therefore, they reported a method of using soft-tissue tendon anatomy to reconstruct the CC ligament with the aid of arthroscopy, combined with the use of suture-button suspension fixation to reduce the CC joint in order to treat the AC joint injury. They achieved good results [50].
Under the arthroscopy field of the shoulder via the posterior approach, the subcoracoid space is separated by an extra anterolateral approach, and the subcoracoid arch and subcoracoid space are divided by a 70-degree observation. After confirming the coracoid process, the subcoracoid surface is roughened, and a vertical clavicle incision is performed around 2.0 cm within the AC joint line, at 3.5 cm. The position is validated using C-arm fluoroscopy after a 2.4-mm hollow drill is passed through the distal clavicle and coracoid process. The wire guides the suture button plate at the tail through the bone tunnel. After the suture-button plate is turned over, an 8.25-mm hollow drill is used to create a soft-tissue tunnel within and outside the coracoid process. From the rear of the clavicle to the inside of the coracoid process, the conical ligament is reconstructed, and from the front of the clavicle to the outside of the coracoid process, the conical ligament is reconstructed. The AC joint is reduced and the CC ligament is repaired with an autologous or allograft tendon measuring 8.0 mm. The AC joint is shortened and the CC ligament is repaired with an autologous or allograft tendon measuring 8.0 mm. The ends of the 4 non-absorbable super-strong suture lines are fixed in the upper clavicular cortex with the suture-button plate. After being tied and fixed, the ends of the transplanted ligaments are tied and fixed on the clavicular bone. The abductor tension sling must be maintained for 4 to 6 weeks following surgery, after which active exercise can be started, and the intensity of physical activity can be increased after 8 weeks [50].
In the treatment of AC dislocation, synthetic materials have become increasingly popular in recent years. Carbon fiber, polytetrafluoroethylene (GoreTex®), and polyethylene terephthalate fiber (LARS®; Dacron®) are common materials. These materials can provide good initial stability and promote healing by inducing fibroblasts into the materials [51]. Fraschini et al stated that LARS had a success rate of 93.3% and a complication rate of 3.3% [52]. Tiefenboeck et al [53] showed that after LARS ligament treatment, 47 patients, with an average follow-up of 7.4 years, saw positive therapeutic outcomes. Although alternative synthetic materials have obtained pretty good clinical results, the danger of severe rejection must be considered when utilizing them [54]. Fauci et al examined postoperative stability and imaging results using biological allografts or synthetic ligaments and reported that, in patients with chronic AC joint injury instability, biological grafts gave better clinical and imaging outcomes than synthetic ligaments [55].
Shortcomings and Future Directions
At present, the controversy after AC joint injury mainly focuses on the treatment of patients with Rockwood III classification, and the use of conservative treatment or surgical treatment needs to be further explored. For now, most surgical treatments have shown positive clinical outcomes, but a minority of patients continue to have poor postoperative functional response. Scheibel et al observed that the postoperative effect of AC dislocation is worse when lateral instability occurs, compared with vertical stability [56]. But there is no consensus on the assessment and diagnosis of transverse instability of the AC joint [57]. Future surgical technique research should begin to concentrate on restoring the integrity of the AC joint capsule and ligament, as well as on restoring transverse stability [58].
As shoulder arthroscopic technology advances, an increasing number of people are attempting to use it to treat AC joint issues. Surgeons believe that arthroscopic treatments have better outcomes for both chronic and acute AC joint injuries, due to internal visualization, smaller trauma, smaller incision, and other advantages of arthroscopy. The use of the TightRope [59] system under arthroscopy is one of the new choices for arthroscopic surgery. Two titanium buttons are connected by a FibreWire suture and are introduced through a CC drill hole with a special guiding device. The inferior subcoracoid button is flipped, and the TightRope is secured by tying a knot over the clavicle [60]. Some surgeons also found that the arthroscopic DogBone® double endobutton technique has better outcomes than the conventional AC brace technique in acute AC joint injury [55].
There is still a long way to go in the field of material research. Dyrna demonstrated in a biomechanical study that all AC joint strengthening techniques could improve the stability of the AC joint against translational and rotational stability, but none of the tested suture structures could restore the complete capsule and ligament structures of the AC joint [61]. One study demonstrated that the reconstruction of the AC joint capsule and ligament with patch on the basis of CC ligament reconstruction can effectively restore translational and axial stability of the AC joint to a level close to normal [62]. However, no specific treatment plan has been created as of yet.
Conclusions
Current research findings suggest, that for patients with Rockwood III and IV–VI classification with significant exercise requirements, surgery is the preferred treatment for acute AC joint dislocation within 3 weeks, and fixation of the CC space with a clavicular hook plate or suture-button suspension can achieve good therapeutic results. Suture-button suspension fixation with ligament restoration is advised for patients with chronic AC dislocation or for those who have failed to respond to nonsurgical treatment. Future studies should concentrate on lateral instability following AC joint damage treatment.



References
1. de Groot C, Verstift DE, Heisen J, Management of acromioclavicular injuries – current concepts: Orthop Res Rev, 2023; 15; 1-12
2. Gorbaty JD, Hsu JE, Gee AO, Classifications in brief: Rockwood classification of acromioclavicular joint separations: Clin Orthop Relat Res, 2017; 475(1); 283-87
3. Kiel J, Taqi M, Kaiser K, Acromioclavicular joint injury. [Updated 2022 Sep 24]: StatPearls [Internet], 2024, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK493188/
4. Nolte PC, Lacheta L, Dekker TJ, Optimal management of acromioclavicular dislocation: Current perspectives: Orthop Res Rev, 2020; 12; 27-44
5. Dyrna F, Imhoff FB, Haller B, Primary stability of an acromioclavicular joint repair is affected by the type of additional reconstruction of the acromioclavicular capsule: Am J Sports Med, 2018; 46(14); 3471-79
6. Fukuda K, Craig EV, An KN, Cofield RH, Chao EY, Biomechanical study of the ligamentous system of the acromioclavicular joint: J Bone Joint Surg Am, 1986; 68(3); 434-40
7. Lee S, Bedi A, Shoulder acromioclavicular joint reconstruction options and outcomes: Curr Rev Musculoskelet Med, 2016; 9(4); 368-77
8. Mazzocca AD, Spang JT, Rodriguez RR, Biomechanical and radiographic analysis of partial coracoclavicular ligament injuries: Am J Sports Med, 2008; 36(7); 1397-402
9. Johansen JA, Grutter PW, McFarland EG, Petersen SA, Acromioclavicular joint injuries: Indications for treatment and treatment options: J Shoulder Elbow Surg, 2011; 20(2 Suppl); S70-82
10. Willimon SC, Gaskill TR, Millett PJ, Acromioclavicular joint injuries: Anatomy, diagnosis, and treatment: Phys Sportsmed, 2011; 39(1); 116-22
11. Tossy JD, Mead NC, Sigmond HM, Acromioclavicular separations: Useful and practical classification for treatment: Clin Orthop Relat Res, 1963; 28; 111-19
12. Tuxun A, Keremu A, Aila P, Abulikemu M, Combination of clavicular hook plate with coracoacromial ligament transposition in treatment of acromioclavicular joint dislocation: Orthop Surg, 2022; 14(3); 613-20
13. Sirin E, Aydin N, Mert Topkar O, Acromioclavicular joint injuries: Diagnosis, classification and ligamentoplasty procedures: EFORT Open Rev, 2018; 3(7); 426-33
14. Schaefer FK, Schaefer PJ, Brossmann J, Experimental and clinical evaluation of acromioclavicular joint structures with new scan orientations in MRI: Eur Radiol, 2006; 16(7); 1488-93
15. Cisneros LN, Reiriz JS, Management of chronic unstable acromioclavicular joint injuries: J Orthop Traumatol, 2017; 18(4); 305-18
16. Bontempo NA, Mazzocca AD, Biomechanics and treatment of acromioclavicular and sternoclavicular joint injuries: Br J Sports Med, 2010; 44(5); 361-69
17. Alexander OM, Radiography of the acromioclavicular articulation: Med Radiogr Photogr, 1954; 30(2); 34-39
18. Barnes CJ, Higgins LD, Major NM, Basamania CJ, Magnetic resonance imaging of the coracoclavicular ligaments: Its role in defining pathoanatomy at the acromioclavicular joint: J Surg Orthop Adv, 2004; 13(2); 69-75
19. Beitzel K, Mazzocca AD, Bak KUpper Extremity Committee of ISAKOS, ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries: Arthroscopy, 2014; 30(2); 271-78
20. Weinstein DM, McCann PD, McIlveen SJ, Surgical treatment of complete acromioclavicular dislocations: Am J Sports Med, 1995; 23(3); 324-31
21. Flint JH, Wade AM, Giuliani J, Rue JP, Defining the terms acute and chronic in orthopaedic sports injuries: A systematic review: Am J Sports Med, 2014; 42(1); 235-41
22. Rolf O, Hann von Weyhern A, Acromioclavicular dislocation Rockwood III–V: Results of early versus delayed surgical treatment: Arch Orthop Trauma Surg, 2008; 128(10); 1153-57
23. Song T, Yan X, Ye T, Comparison of the outcome of early and delayed surgical treatment of complete acromioclavicular joint dislocation: Knee Surg Sports Traumatol Arthrosc, 2016; 24(6); 1943-50
24. Maleitzke T, Maziak N, Plachel F, Can an acute high-grade acromioclavicular joint separation be reduced and stabilized without surgery? A surgeon’s experience: Arch Orthop Trauma Surg, 2020; 140(12); 2021-27
25. Allemann F, Halvachizadeh S, Waldburger M, Different treatment strategies for acromioclavicular dislocation injuries: A nationwide survey on open/minimally invasive and arthroscopic concepts: Eur J Med Res, 2019; 24(1); 18
26. Schlegel TF, Burks RT, Marcus RL, Dunn HK, A prospective evaluation of untreated acute grade III acromioclavicular separations: Am J Sports Med, 2001; 29(6); 699-703
27. Ceccarelli E, Bondì R, Alviti F, Treatment of acute grade III acromioclavicular dislocation: a lack of evidence: J Orthop Traumatol, 2008; 9(2); 105-8
28. Cook JB, Shaha JS, Rowles DJ, Clavicular bone tunnel malposition leads to early failures in coracoclavicular ligament reconstructions: Am J Sports Med, 2013; 41(1); 142-48
29. Korsten K, Gunning AC, Leenen LP, Operative or conservative treatment in patients with Rockwood type III acromioclavicular dislocation: A systematic review and update of current literature: Int Orthop, 2014; 38(4); 831-38
30. Schlegel TF, Burks RT, Marcus RL, Dunn HK, A prospective evaluation of untreated acute grade III acromioclavicular separations: Am J Sports Med, 2001; 29(6); 699-703
31. Beitzel K, Cote MP, Apostolakos J, Current concepts in the treatment of acromioclavicular joint dislocations: Arthroscopy, 2013; 29(2); 387-97
32. Cetinkaya E, Arıkan Y, Beng K, Bosworth and modified Phemister techniques revisited. A comparison of intraarticular vs extraarticular fixation methods in the treatment of acute Rockwood type III acromioclavicular dislocations: Acta Orthop Traumatol Turc, 2017; 51(6); 455-58
33. Kaiser W, Ziemer G, Heymann HTreatment of acromioclavicular dislocations with the Balser hook plate and ligament suture: Chirurg, 1984; 55(11); 721-24 [in German]
34. Mlasowsky B, Brenner P, Düben W, Heymann H, Repair of complete acromioclavicular dislocation (Tossy stage III) using Balser’s hook plate combined with ligament sutures: Injury, 1988; 19(4); 227-32
35. Kezunović M, Bjelica D, Popović S, Comparative study of surgical treatment of acromioclavicular luxation: Vojnosanit Pregl, 2013; 70(3); 292-97
36. Broos P, Stoffelen D, Van de Sijpe K, Fourneau ISurgical management of complete Tossy III acromioclavicular joint dislocation with the Bosworth screw or the Wolter plate. A critical evaluation: Unfallchirurgie, 1997; 23(4); 153-59 [in German]
37. Arirachakaran A, Boonard M, Piyapittayanun P, Post-operative outcomes and complications of suspensory loop fixation device versus hook plate in acute unstable acromioclavicular joint dislocation: A systematic review and meta-analysis: J Orthop Traumatol, 2017; 18(4); 293-304
38. Ammon JT, Voor MJ, Tillett ED, A biomechanical comparison of Bosworth and poly-L lactic acid bioabsorbable screws for treatment of acromioclavicular separations: Arthroscopy, 2005; 21(12); 1443-46
39. Mori D, Yamashita F, Kizaki K, Anatomic coracoclavicular ligament reconstruction for the treatment of acute acromioclavicular joint dislocation: Minimum 10-year follow-up: JB JS Open Access, 2017; 2(3); e0007
40. Menge TJ, Tahal DS, Katthagen JC, Millett PJ, Arthroscopic acromioclavicular joint reconstruction using knotless coracoclavicular fixation and soft-tissue anatomic coracoclavicular ligament reconstruction: Arthrosc Tech, 2017; 6(1); e37-e42
41. Wu M, Yan S, Yu Y, Wang JMinimally invasive reconstruction of coracoclavicular ligament with adjustable locking TightRope for Rockwood type III acromioclavicular joint dislocation: Chin J Traumatol, 2019; 35(7); 631-37 [in Chinese]
42. Nolte PC, Lacheta L, Dekker TJ, Optimal management of acromioclavicular dislocation: Current perspectives: Orthop Res Rev, 2020; 12; 27-44
43. Mazzocca AD, Santangelo SA, Johnson ST, A biomechanical evaluation of an anatomical coracoclavicular ligament reconstruction: Am J Sports Med, 2006; 34(2); 236-46
44. Weaver JK, Dunn HK, Treatment of acromioclavicular injuries, especially complete acromioclavicular separation: J Bone Joint Surg Am, 1972; 54(6); 1187-94
45. Rauschning W, Nordesjö LO, Nordgren B, Resection arthroplasty for repair of complete acromioclavicular separations: Arch Orthop Trauma Surg (1978), 1980; 97(3); 161-64
46. Kawabe N, Watanabe R, Sato M, Treatment of complete acromioclavicular separation by coracoacromial ligament transfer: Clin Orthop Relat Res, 1984(185); 222-27
47. Wellmann M, Kempka JP, Schanz S, Coracoclavicular ligament reconstruction: Biomechanical comparison of tendon graft repairs to a synthetic double bundle augmentation: Knee Surg Sports Traumatol Arthrosc, 2009; 17(5); 521-28
48. Thomas K, Litsky A, Jones G, Bishop JY, Biomechanical comparison of coracoclavicular reconstructive techniques: Am J Sports Med, 2011; 39(4); 804-10
49. Wang G, Xie R, Mao T, Xing S, Treatment of AC dislocation by reconstructing CC and AC ligaments with allogenic tendons compared with hook plates: J Orthop Surg Res, 2018; 13(1); 175
50. Millett PJ, Warth RJ, Greenspoon JA, Horan MP, Arthroscopically assisted anatomic coracoclavicular ligament reconstruction technique using coracoclavicular fixation and soft-tissue grafts: Arthrosc Tech, 2015; 4(5); e583-87
51. Fauci F, Merolla G, Paladini P, Surgical treatment of chronic acromioclavicular dislocation with biologic graft vs synthetic ligament: A prospective randomized comparative study: J Orthop Traumatol, 2013; 14(4); 283-90
52. Fraschini G, Ciampi P, Scotti C, Surgical treatment of chronic acromioclavicular dislocation: Comparison between two surgical procedures for anatomic reconstruction: Injury, 2010; 41(11); 1103-6
53. Tiefenboeck TM, Boesmueller S, Popp D, The use of the LARS system in the treatment of AC joint instability – long-term results after a mean of 7.4 years: Orthop Traumatol Surg Res, 2018; 104(6); 749-54
54. Sinagra ZP, Kop A, Pabbruwe M, Foreign body reaction associated with artificial LARS ligaments: A retrieval study: Orthop J Sports Med, 2018; 6(12); 2325967118811604
55. Renaud M, Caubrière M, Lancigu R: Orthop Traumatol Surg Res, 2024; 110(1); 103635
56. Scheibel M, Dröschel S, Gerhardt C, Kraus N, Arthroscopically assisted stabilization of acute high-grade acromioclavicular joint separations: Am J Sports Med, 2011; 39(7); 1507-16
57. Aliberti GM, Kraeutler MJ, Trojan JD, Mulcahey MK, Horizontal instability of the acromioclavicular joint: A systematic review: Am J Sports Med, 2020; 48(2); 504-10
58. Haber DB, Golijanin P, Stone GL, Primary acromioclavicular-coracoclavicular reconstruction using 2 allografts, TightRope, and stabilization to the acromion: Arthrosc Tech, 2019; 8(2); e147-e52
59. Zhang LF, Yin B, Hou S, Arthroscopic fixation of acute acromioclavicular joint disruption with TightRope™: Outcome and complications after minimum 2 (2–5) years follow-up: J Orthop Surg (Hong Kong), 2017; 25(2); 2309499016684493
60. Phadke A, Bakti N, Bawale R, Singh B, Current concepts in management of ACJ injuries: J Clin Orthop Trauma, 2019; 10(3); 480-85
61. Dyrna F, Imhoff FB, Haller B, Primary stability of an acromioclavicular joint repair is affected by the type of additional reconstruction of the acromioclavicular capsule: Am J Sports Med, 2018; 46(14); 3471-79
62. Morikawa D, Mazzocca AD, Obopilwe E, Reconstruction of the acromioclavicular ligament complex using dermal allograft: A biomechanical analysis: Arthroscopy, 2020; 36(1); 108-15
Figures
In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387