06 March 2024: Lab/In Vitro Research
Impact of Auxiliary Features on Retention of Short Dental Crowns: An In-Vitro Analysis of Box and Groove Preparations
Mohammed E. SayedDOI: 10.12659/MSM.943401
Med Sci Monit 2024; 30:e943401






Abstract
BACKGROUND: Several auxiliary features have been proposed to achieve sustainable retention for short-prepared dental crowns; however, achieving retention is challenging. This study aimed to assess the impact of increased total occlusal convergence and auxiliary preparation factors like box and groove on the retention form of short tooth preparations.
MATERIAL AND METHODS: Eighty resin machine-milled dies with a height of 3 mm and a deep chamfer margin of 1 mm were prepared to mimic the short-prepared molar. Initially, 2 teeth were prepared following the guidelines, and the total occlusal convergence was kept at 10° and 20°, respectively. Auxiliary features such as the proximal box and buccal groove were prepared on separate 20° dies. Eighty dies were prepared with 10 samples each for 10°, 20°, 20° with proximal box and 20° with buccal groove for zirconia (n=40) and metal crowns (n=40). Cementation was done with glass ionomer luting cement, and a pull-off test was conducted. Data were analyzed using one-way analysis of variance and post hoc fisher least significant difference test (P<0.05).
RESULTS: The highest mean was observed in the proximal box group with the metal crown (14.59), and the lowest in the group with 20° zirconia crowns (9.12). Within groups, the highest retentive values were found for the 20° taper with proximal box preparation; the lowest was for the 20° taper group.
CONCLUSIONS: Within the study limitations, it could be concluded that incorporating a proximal box or buccal groove in short tooth preparations with an increased total occlusal convergence improved retentive values.
Keywords: Dental Prosthesis Retention, Tooth Crown
Background
Dental crown retention, a fundamental aspect of prosthodontics, depends on tooth preparation, cement choice, and crown-tooth interface. Tooth preparation must include mechanical retention, and crown design must favor convergence angles and occlusal clearance for optimal dental results. Retention of the crown is significant for long-term effectiveness and functional rehabilitation in restorative dentistry. Retention is described as the prevention of dislodgment of the cast restoration along with its path of insertion, while resistance is the prevention of dislodgment by lateral forces [1,2].
Goodacre et al suggested the attributes that should be considered in the preparation of a tooth: a range of 10° to 20° of total occlusal convergence (TOC), a minimum occluso-cervical dimension of 4 mm for molars and 3 mm for all other teeth, and a height to base ratio of 0.4 or higher [3]. Empirical evidence indicates that a range of factors, such as the taper and form, dislodging forces, vertical forces, and type of cement used, can influence the retention of a dental crown. Modification techniques have been suggested to improve the retention of a dental crown when it is cemented to a tooth that has undergone standard preparation and when the tooth’s dimensions have been compromised.
TOC, as the literature suggests, is one of the most critical factors in preparing a tooth to receive a crown [4]. The amount of taper that can be attained through experimental and therapeutic means is not within the range of 2° to 5° but instead falls within the scope of 12° to 22° [2,4,5]. However, Jorgensen [6] and Kaufman et al [7] demonstrated an inverse relationship between increased TOC and retention. The optimum TOC in complete veneer preparations is influenced by several factors, including accessibility, morphology, proximal contacts between teeth, and operator expertise [8–10].
The literature suggests that 68.8% of cast restoration failure depends upon mechanical factors (crown preparation, cementation, and materials), while 28.8% of failure depends on biological factors (soft tissue support) [11]. Additionally, the primary causes of restoration failures were insufficient clinical crown length and the extent of tooth damage before treatment and debonding [12,13]. However, ongoing debate continues regarding the optimal material, most suitable cement, and most efficacious approach for enhancing retention in cases involving short clinical abutments [14].
Occluso-cervical height also plays a critical role in the retention of a crown. This can be compromised in conditions of morphological tooth wear, such as attrition, abrasion, and erosion, and in cases with extensive caries, fractures, occlusal discrepancy, developmental anomalies, and abfractions. Dentists can encounter challenges in achieving optimal retention and resistance forms during the preparation of these teeth. If the restoration is lost, it can impose various esthetic and functional challenges. In a significant majority of clinical cases, it was observed that short clinical abutments resulted in the dislodgement of crowns in around two-thirds of instances [15]. Ideally, 4 mm is the minimal preparation height recommended for posterior preparations, and in situations of short clinical crowns, achieving this is very difficult and adversely affects retention, which is of great concern [16–19]. In such situations, the alternatives are either crown lengthening surgery or the incorporation of various retentive features, such as grooves, boxes, and pins, in the preparation. Studies have evaluated the effect of these auxiliary features on the retention of the prosthesis [20–23].
Full coverage restorations are a treatment of choice whenever maximum retention and resistance forms are desired. Also, the addition of grooves and boxes has been advocated if heavy forces are anticipated in posterior teeth [24].
Published literature has shown the improvement of retention by creating cement locks and a groove, and further modifications with multiple grooves [25–27]. There exist numerous scholarly, and contentious, papers about the management of castings on clinical crowns of reduced height by the integration of supplementary retentive elements [18,22,27–30]. Grooves and boxes increase the entire restoration’s surface area, providing more space for luting cement [28]. Rajkumar et al [22] observed an insignificant increase in retention with the addition of a groove. However, using grooves to enhance retention was encouraged, as the retention was increased by 100% when the cast crown was extended into the groove rather than blocked off [11]. Compared with proximal boxes, proximal grooves yielded a notably increased retention, and including proximal grooves in short preparations resulted in retention comparable to that of a conventional preparation, with sufficient crown height [21]. The placement of grooves and boxes in compromised preparations was not effective when they possessed the same 20° TOC. The potential for reducing total occlusal convergence at the cervical level is also demonstrated to be promising [23] but has limited use. However, Tjan [31] showed that the presence of grooves can also affect the seating of the casting, making it more difficult, and difficulty increases with the increase in the number of grooves.
While there are multiple perspectives on the matter, the precise advantages of such supplementary characteristics remain ambiguous. The objective of the present investigation was to assess the impact of auxiliary preparation factors like box and groove preparation on the retention form of short-prepared teeth. The null hypothesis posited that including a buccal groove or proximal box along with increased total occlusal convergence would increase the retention form of a complete zirconia and metal crowns on the molar tooth with short preparations.
Material and Methods
FABRICATION OF TEST SAMPLES:
Two identical typhodont teeth (Practicon, Greenville, NC, USA) # 36 (mandibular left first molar) were prepared to simulate short crown preparations following general preparation guidelines, with specifics of the occluso-cervical height of 3 mm and a deep chamfer margin of 1 mm. Two plane reductions were followed for functional cusps. A 10° TOC was given to the first model and 20° to the second model. The dental procedures involved the use of a high-speed air rotor handpiece (manufactured by KaVo do Brazil Ind. Com. Ltd., Joinville, SC, Brazil), which was securely connected to a dental cast surveyor (3005 Surveyor Type A, produced by Dental Farm). The preparations were conducted using a round-end fissure diamond bur (102 R Shofu), which was tapered at angles of 10° and 20°. All the standardized preparations were checked with the help of a putty index sectioned in multiple directions (Affinis, Coltène/Whaledent). The anatomical preparations were rounded off and made without any lines or sharp points. Prior to printing the functional models, the taper was measured and verified using a computer system made up of a stereomicroscope with a USB CCD camera attached (Amscope, Irvine, CA, USA), a desktop computer, and a suitable measurement program (Version No. 3.7.12924) (Figure 1).
Modifications of the master model to include auxiliary features, 3-dimensional (3D) printed replica models, were generated from the 20° TOC master model so that the standardized taper and the preparations remained the same for the remaining groups. Verification was done in the same manner as for typhodont teeth. For scanning these models, a Bench Top Scanner (model number 4) manufactured by 3 Shape (Copenhagen, Denmark) was used. The working model from each group was 3D printed using the different 3D print resin liquid (Denta Model, Asiga, Alexandria, Australia), a digital light processing 3D printing machine (Asiga 3D printer, Alexandria, Australia, serial number 70B3D5362C6A, model number PN01233), and printing parameters of 50 micrometer layer thickness, 2.975 s exposure time, and 0° printing orientation after the models had been scanned. The base’s design was modified so that it was compatible with the dimensions and arrangement of the holding clamp used by the universal testing machine. A mid-buccal groove was provided on one of the printed working models and had dimensions of 1-mm width and depth and terminated 0.5 mm above the finish line. A 1-mm diameter cylindrical diamond bur was oriented vertically and was used to provide the groove. Another printed model was used to provide a proximal box on the distal side and had the same details as the groove, but the width increased to 3 mm (Figure 2). All the preparation and modifications were done by a single operator (A.P.) after practicing on many models. All the working models were generated from these 4 master models, with different features. The study comprised 8 groups, each containing 10 samples (Table 1).
All the working models (40 for zirconia and 40 for metal) were 3D printed with changes in taper and the auxiliary features. Before being used in the study, each resin die sample was examined for appropriateness and integrity, and the model was scanned to create an STL file, which was then processed separately. After creating an occlusal ring with an external diameter of 5.5 mm and an interior diameter of 3.5 mm, the margin was set with a cement spacing of 50 μm and 40 samples of 3D-milled zirconia crowns (10 per group) were fabricated. Monolithic zirconia was used for the fabrication of the zirconia crowns (Ceramill Zolid PS, Amann Girrbach, ref 760257, lot 1708000, North America, LP, Charlotte, NC, USA). Forty samples of metal crowns (10 per group) were fabricated via the lost wax technique. CAD/CAM wax patterns with an occlusal ring of similar dimensions were made and 3D printed, and the printed model was invested and casted using the lost wax technique. Metal used for fabricating metal crowns were nickel-chromium alloys (Wiron Light, ref 50270, lot 73784, BEGO Bremer Goldschlägerei Wilh. Herbst GmbH & Co. KG., Bremen, Germany). The fit of each definitive crown was examined and verified on their respective models. All the crowns fabricated were checked for any inaccuracies and were replaced by new ones if found faulty.
CEMENTATION OF DEFINITIVE CROWNS:
Glass ionomer cement (RIVA Glass Ionomer luting cement, SDI Germany GmbH, Cologne, Germany, lot M210815) was the material of choice for the cementation process. The crowns (n=10) of each subgroup were cemented to the corresponding models and were secured for 5 min with a force of about 2.5 kg. Once the initial setting had been completed, extra cement was taken out with an explorer (Figure 3).
AGEING OF SAMPLES AND PULL-OFF TESTING:
The thermocycling equipment (Model 1100, SD Mechatronik, Bayern, Germany) was used to thermocycle the cemented definitive crowns for 10 000 cycles between baths held at 5°C and 55°C (15 s each), with a dripping period of 10 s and a transfer time of 5 s, to simulate a year in the oral environment (Figure 4).
A universal testing device (Instron System ID 5967L1040; model number 5967, Norwood, MA, USA) was then used to evaluate retention under tension with a crosshead speed of 5 mm/min on all samples (Figure 5). Pull-off testing was performed on all 80 samples until crowns were dislodged, and the tensile force in newtons (N) was recorded. In other research [32,33], the retention of crowns was tested using a comparable crown pull-off test with universal testing equipment. The retentive strength of crowns was evaluated based on a variety of characteristics in a few earlier studies [34,35]. These earlier studies used standardized metal dies that were comparable to the models that were 3D printed for this investigation.
STATISTICAL ANALYSIS:
All tensile force values recorded during the tests for all specimens were recorded in a Microsoft Excel sheet (Microsoft Excel, USA). Subsequently, the collected data underwent a process of refinement and coding before being loaded into the statistical program SPSS Version 25.0 (IBM Corp., Armonk, NY, USA). The retentive strengths of all definitive crowns, along with crown tapers and auxiliary features, were evaluated using one-way ANOVA). The post hoc Fisher least significant difference test was used to compare groups A1 to B4 between themselves. A 95% confidence interval calculation was also made. In all compared statistical tests, a significance level of
Results
The present study was conducted to visualize the effect of the change in TOC as well as the effect of the auxiliary features, namely, buccal groove or proximal box, on the retentive competencies of the definitive zirconia and metal crowns. Table 2 demonstrates the means and standard deviations (SDs) of all groups. The mean difference was highest in group B4 (mean=14.59 and SD=0.85), while it was lowest in group A2 (mean=9.12 and SD=0.93). The result of one-way ANOVA found a statistically significant difference among the groups (
Table 3 presents the results indicating mean differences between the groups and multiple comparisons using the post hoc least significant difference test. Significant differences were observed in retention values between the groups, as indicated by the pull-off test. A strong negative correlation was found between groups A1, B3, and B4, while a positive correlation was identified between groups A1 and A2. Additionally, a statistically significant relationship was observed between groups A2 and A1
The box plot in Figure 6 depicts comparisons between the groups using the post hoc least significant difference test. The figure indicates that the maximum retentive value was observed in groups A4 and B4 with a 20° taper, both with proximal boxes in both metal and zirconia crowns. However, the 20° taper without box preparation showed lower retentive values. Figure 7 shows the confidence interval between the groups of zirconia and metal crowns. The result of this study showed that tooth preparation with a taper of 20° and a box preparation had the highest retentive value.
Discussion
STRENGTH AND LIMITATIONS:
This study was limited by factors such as single-tooth preparation and the lack of consideration of clinical factors, for example, tooth support or periodontal ligament support. Additionally, a single type of alloy was used. The rationale behind using resin material in this study was the high compressive strength and resilience of the base. Glass ionomer cement was used as a luting agent for resin material. However, the use of other cement might have changed the outcome. Hence, future in vitro studies should focus on the comparison of various cements in evaluating the retention of metal/ceramic crowns with a greater number of samples.
Conclusions
Within the limitations of the study, it can be concluded that increasing the TOC from 10° to 20° reduced the retentive quality of a complete coverage crown. Adding auxiliary features, such as grooves and boxes, increased the retentive values in a short-prepared tooth with a TOC of 20°. Box preparation on the proximal surface provided better retentive values than the groove on the buccal surface. Metal crowns provided better retentive values than zirconia crowns, based on the die-cement-crown material interface. Incorporating proximal box preparation in an increased TOC of 20° improved the retentive values even better than the 10° TOC tooth with no modifications.
Figures
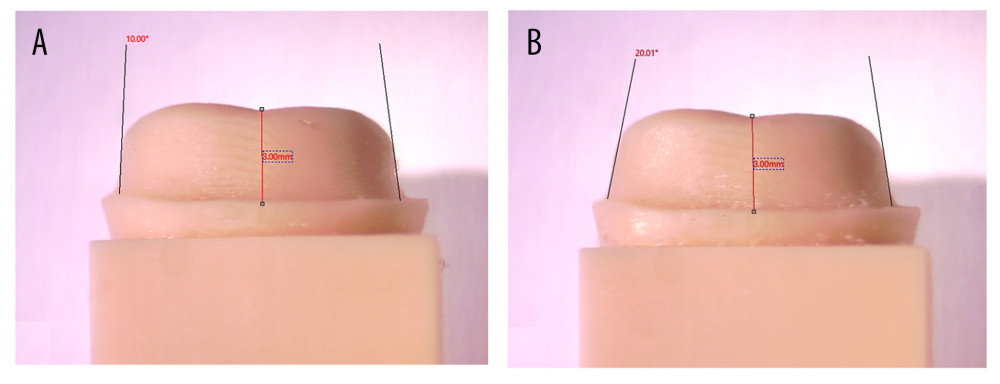 Figure 1. (A) 10° total occlusal convergence (taper) measured via stereomicroscope with a connected USB CCD camera. (B) 20° total occlusal convergence (taper) measured via stereomicroscope with a connected USB CCD camera. (The figure was generated using Microsoft Snip and Sketch version 10.2008.30001.0 and then compiled on MS PowerPoint, version 20H2 (OS build 19042.1466) on Windows 11 Pro, developed by Microsoft Corporation).
Figure 1. (A) 10° total occlusal convergence (taper) measured via stereomicroscope with a connected USB CCD camera. (B) 20° total occlusal convergence (taper) measured via stereomicroscope with a connected USB CCD camera. (The figure was generated using Microsoft Snip and Sketch version 10.2008.30001.0 and then compiled on MS PowerPoint, version 20H2 (OS build 19042.1466) on Windows 11 Pro, developed by Microsoft Corporation). 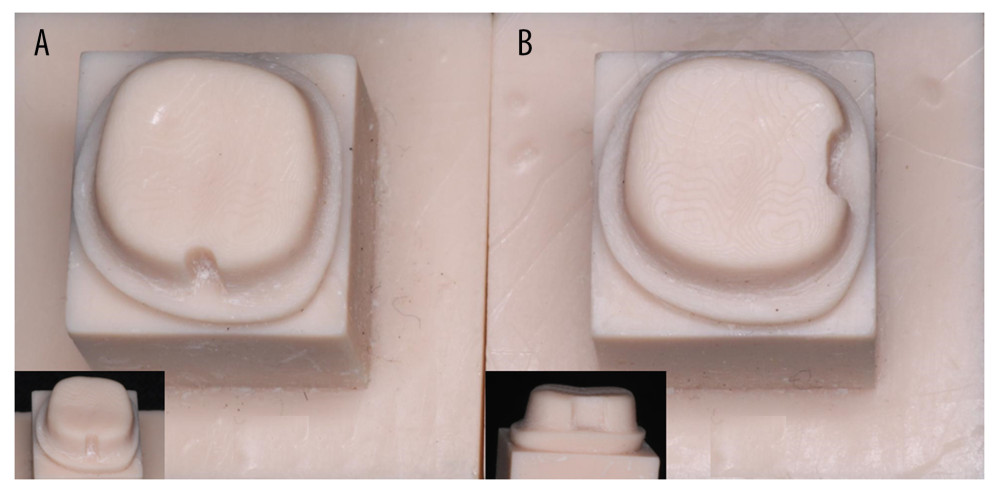 Figure 2. Standardized resin dies after typhodont teeth preparations with 20-degree taper along with mid-buccal groove and distal proximal box. (A, B) insets showing close view of the groove and the box preparations. The photograph was captured with a Canon EOS 700D digital single-lens reflex camera equipped with a 100-mm macro lens. A ring flash may have been used, and the photograph was then compiled using MS PowerPoint, version 20H2, on Windows 11 Pro, developed by Microsoft Corporation.
Figure 2. Standardized resin dies after typhodont teeth preparations with 20-degree taper along with mid-buccal groove and distal proximal box. (A, B) insets showing close view of the groove and the box preparations. The photograph was captured with a Canon EOS 700D digital single-lens reflex camera equipped with a 100-mm macro lens. A ring flash may have been used, and the photograph was then compiled using MS PowerPoint, version 20H2, on Windows 11 Pro, developed by Microsoft Corporation. 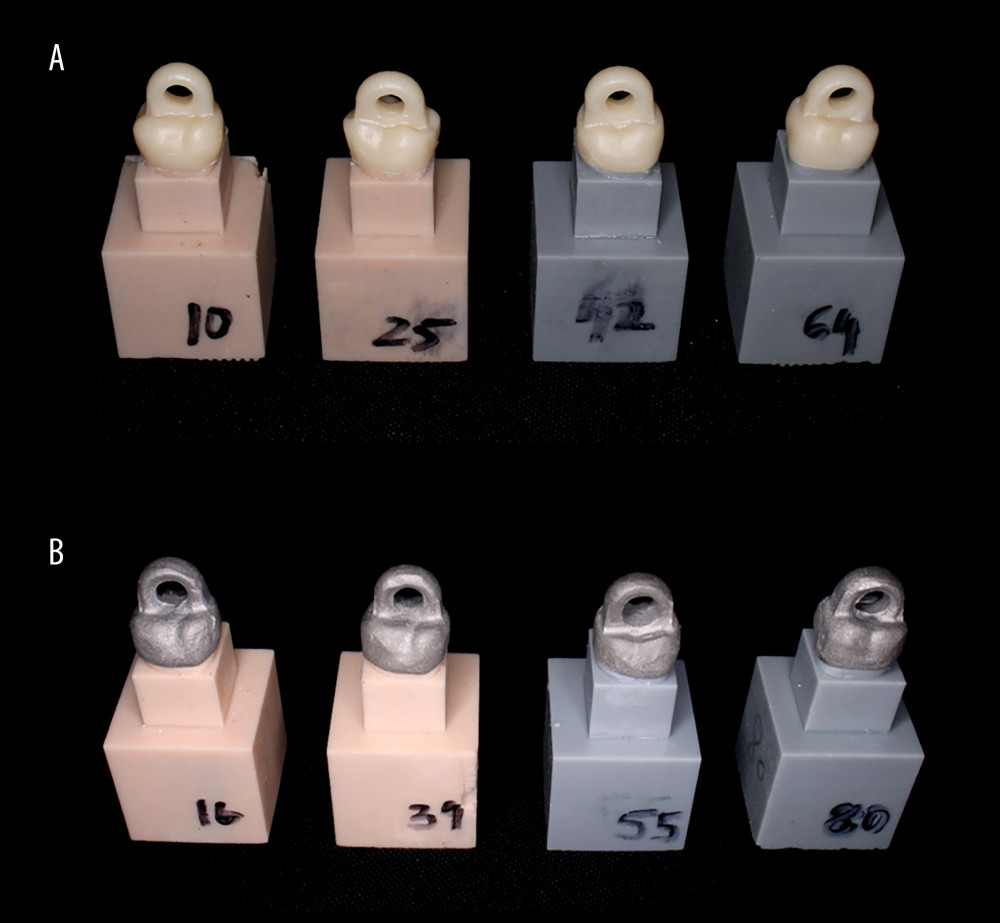 Figure 3. (A) Cemented definitive zirconia crowns on resin models of all groups. (B) Cemented definitive metal crowns on resin models of all groups.
Figure 3. (A) Cemented definitive zirconia crowns on resin models of all groups. (B) Cemented definitive metal crowns on resin models of all groups.  Figure 4. Thermocycling unit showing thermocycling of cemented metal crowns (10000 cycles between baths held at 5°C and 55°C). The image was captured using a Canon EOS 700D digital single-lens reflex camera equipped with a 100-mm macro lens, either with or without a ring flash.
Figure 4. Thermocycling unit showing thermocycling of cemented metal crowns (10000 cycles between baths held at 5°C and 55°C). The image was captured using a Canon EOS 700D digital single-lens reflex camera equipped with a 100-mm macro lens, either with or without a ring flash. 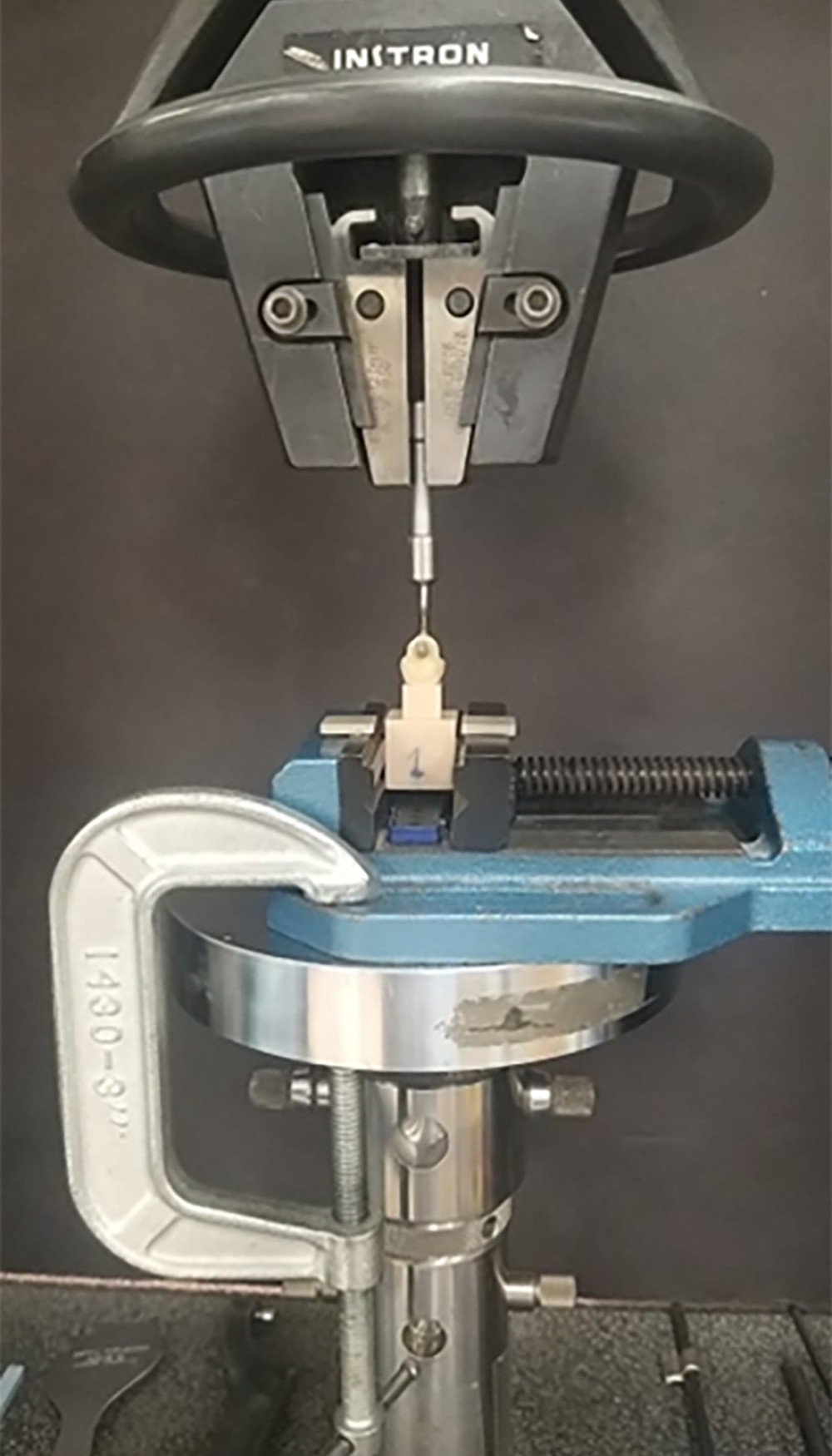 Figure 5. The universal testing machine demonstrates the connection of the test samples for the pull-off test, where the handles of the zirconia crowns are positioned to align with the sample handle in a perpendicular manner to the direction of the pulling force. The image was captured using a Canon EOS 700D digital single-lens reflex camera equipped with a 100-mm macro lens, either with or without a ring flash.
Figure 5. The universal testing machine demonstrates the connection of the test samples for the pull-off test, where the handles of the zirconia crowns are positioned to align with the sample handle in a perpendicular manner to the direction of the pulling force. The image was captured using a Canon EOS 700D digital single-lens reflex camera equipped with a 100-mm macro lens, either with or without a ring flash. ![Retentive force values (in newtons [N]) using post hoc least significant difference test shown via box plot.](https://jours.isi-science.com/imageXml.php?i=medscimonit-30-e943401-g006.jpg&idArt=943401&w=1000) Figure 6. Retentive force values (in newtons [N]) using post hoc least significant difference test shown via box plot.
Figure 6. Retentive force values (in newtons [N]) using post hoc least significant difference test shown via box plot. 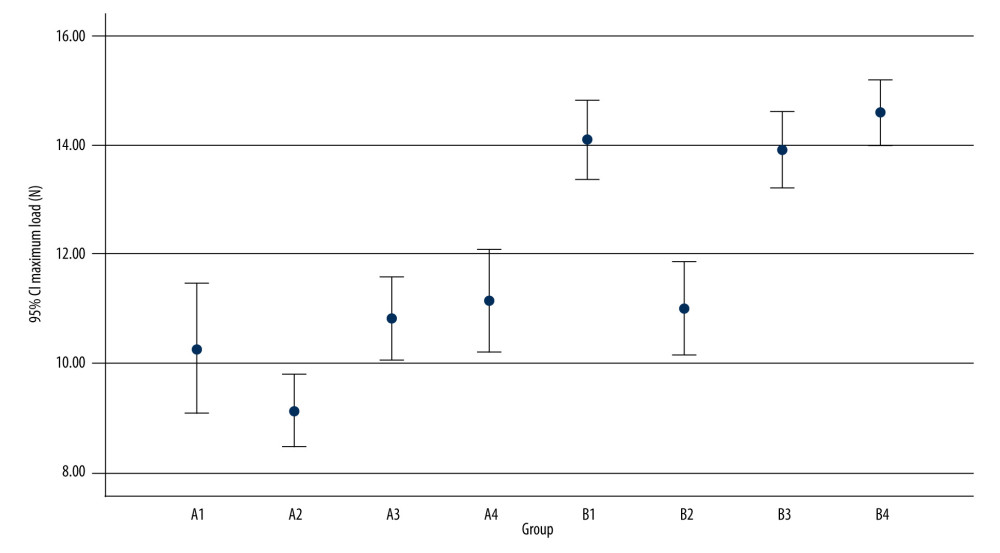 Figure 7. A comparison using the 95% confidence interval between test groups of zirconia and metal crowns in relation to pull-off force.
Figure 7. A comparison using the 95% confidence interval between test groups of zirconia and metal crowns in relation to pull-off force. Tables
Table 1. Description of zirconia and metal crown groups involving different preparation features in the study.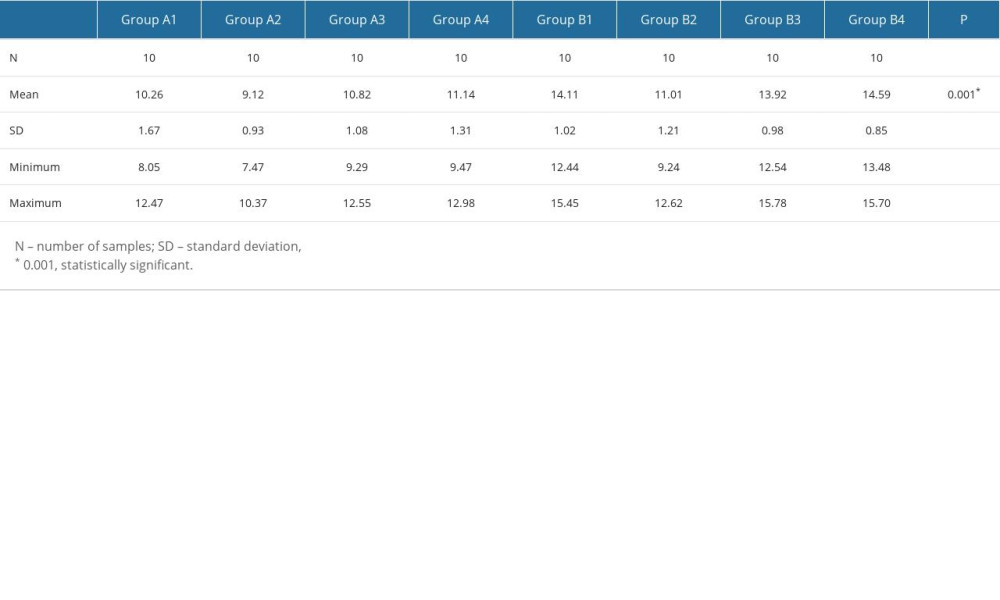 Table 2. One-way analysis of variance showing inter-group comparison (in zirconia and metal crown groups) for retentive force values (in newtons).
Table 2. One-way analysis of variance showing inter-group comparison (in zirconia and metal crown groups) for retentive force values (in newtons).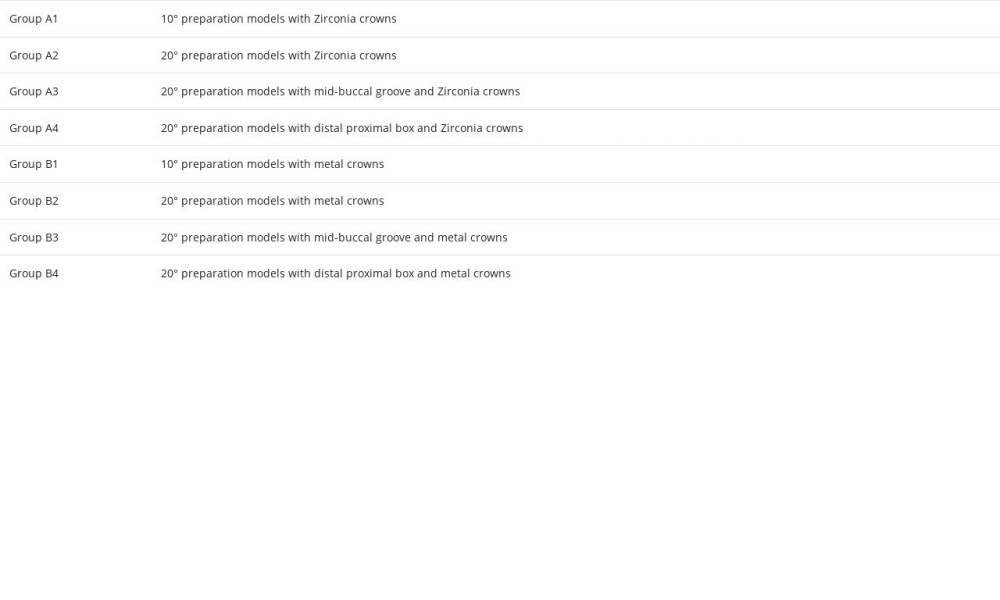 Table 3. Post hoc Fisher least significant difference test showing differences in zirconia (A) and metal crown (B) group means and multiple comparison of pull-off force values (N).
Table 3. Post hoc Fisher least significant difference test showing differences in zirconia (A) and metal crown (B) group means and multiple comparison of pull-off force values (N).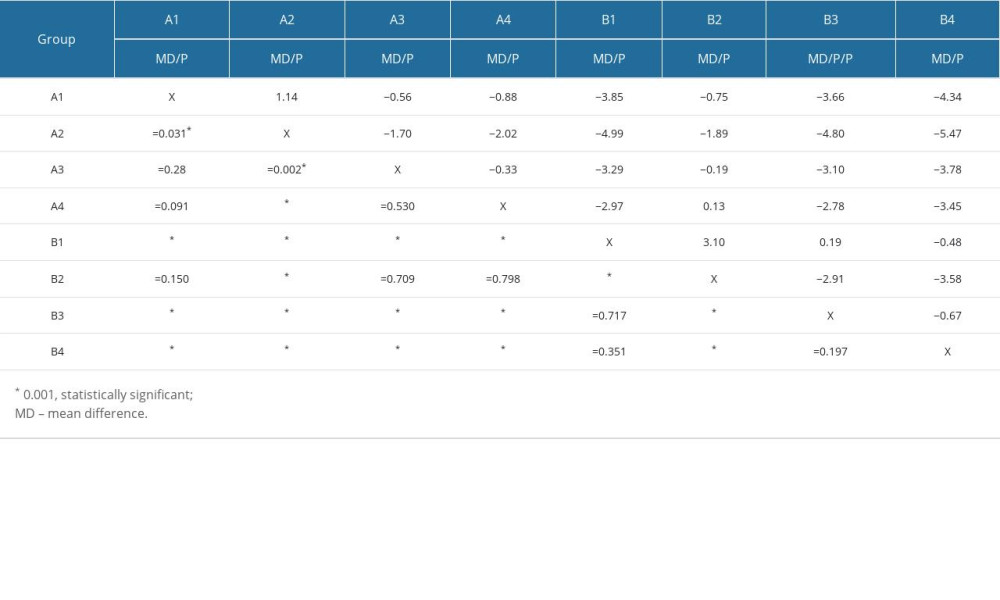
References
1. Sakaguchi RL, Powers JM: Craig’s restorative dental materials-e-book, 2011, Elsevier Health Sciences
2. Shillingburg HT, Hobo S, Whitsett LD, Fundamentals of fixed prosthodontics: Preparations for cast gold restorations, 2012; 143-85, Chicago, Quintessence Publishing
3. Goodacre CJ, Campagni WV, Aquilino SA, Tooth preparations for complete crowns: An art form based on scientific principles: J Prosthet Dent, 2001; 85; 363-76
4. Tiu J, Al-Amleh B, Waddell JN, Duncan WJ, Clinical tooth preparations and associated measuring methods: A systematic review: J Prosthet Dent, 2015; 113(3); 175-84
5. Chan KC, Hormati AA, Boyer DB, Auxiliary retention for complete crowns provided by cement keys: J Prosthet Dent, 1981; 45(2); 152-55
6. Jørgensen KD, The relationship between retention and convergence angle in cemented veneer crowns: Acta Odontol Scand, 1955; 13(1); 35-40
7. Kaufman EG, Coelho DH, Colin L, Factors influencing the retention of cemented gold castings: J Prosthet Dent, 1961; 11(3); 487-502
8. Dodge WW, Weed RM, Baez RJ, Buchanan RN, The effect of convergence angle on retention and resistance form: Quintessence Int, 1985; 16(3); 191-94
9. Al-Moaleem M, Shariff M, Porwal A, Evaluation of the degree of taper and convergence angle of full ceramo-metal crown preparations by different specialists centers at Assir Region, Saudi Arabia: Saudi J Med Med Sci, 2015; 3(3); 198-203
10. AL-Moaleem M, Ahmad M, Porwal A, Evaluation of tooth preparation by dental students in Jazan University during pre-clinical training: J Oral Health Dent Manag, 2014; 13(4); 1166-70
11. AlShaarani F, Alaisami RM, Aljerf L, An auxiliary factor for increasing the retention of short abutments: Heliyon, 2019; 5(10); e02674
12. Kopperud SE, Tveit AB, Gaarden T, Longevity of posterior dental restorations and reasons for failure: Eur J Oral Sci, 2012; 120(6); 539-48
13. Uy JN, Neo JC, Chan SH, The effect of tooth and foundation restoration heights on the load fatigue performance of cast crowns: J Prosthet Dent, 2010; 104(5); 318-24
14. Goldstein GR, The longevity of direct and indirect posterior restorations is uncertain and may be affected by a number of dentist-, patient-, and material-related factors: J Evid Based Dent Pract, 2010; 10(1); 30-31
15. Kent WA, Shillingburg HT, Duncanson MG, Taper of clinical preparations for cast restorations: Quintessence Int, 1988; 19(5); 339-45
16. Seol HW, Koak JY, Kim SK, Heo SJ, Full mouth rehabilitation of partially and fully edentulous patient with crown lengthening procedure: A case report: J Adv Prosthodont, 2010; 2(2); 50-53
17. Anoop S, Crown lengthening surgery: A periodontal makeup for anterior esthetic restoration: J Interdiscip Dent, 2018; 8(3); 132-36
18. Dhanraj M, Jain AR, Management of short abutments receiving complete veneer crowns – a cross sectional survey: Biomed Pharmacol J, 2017; 10(3); 1569-76
19. Sharma A, Rahul GR, Poduval ST, Shetty K, Short clinical crowns (SCC) – treatment considerations and techniques: J Clin Exp Dent, 2012; 4(4); e230-36
20. Pai V, Shetty P, Joseph M, Comparative evaluation of effect of auxiliary retentive features on retention of complete cast crowns in teeth with adequate and inadequate crown height. An invitro study: Indian J Dent Res, 1999; 10(1); 5-10
21. Vinaya K, Rakshith H, Prasad KD, To evaluate and compare retention of complete cast crown in natural teeth using different auxiliary retentive features with two different crown heights an in vitro study: Int J Biomed Sci, 2015; 11; 99-106
22. Rajkumar K, Bhat AM, Krishna PD, Effect of axial groove and resin luting cements on the retention of complete cast metal crowns: Dent Res J, 2009; 6(1); 39
23. Proussaefs P, Campagni W, Bernal G, The effectiveness of auxiliary features on a tooth preparation with inadequate resistance form: J Prosthet Dent, 2004; 91(1); 33-41
24. Rosenstiel SF, Land MF, Fujimoto J, Principles of tooth preparation: Contemporary fixed prosthodontics, 1995; 2; 135-67, St. Louis, Mosby-Year Book, Inc
25. Leong EW, Choon Tan KB, Nicholls JI, The effect of preparation height and luting agent on the resistance form of cemented cast crowns under load fatigue: J Prosthet Dent, 2009; 102(3); 155-64
26. Lewinstein I, Block L, Lehr Z, An in vitro assessment of circumferential grooves on the retention of cement-retained implant-supported crowns: J Prosthet Dent, 2011; 106(6); 367-72
27. O’Kray H, Marshall TS, Braun TM, Supplementing retention through crown/preparation modification: an in vitro study: J Prosthet Dent, 2012; 107(3); 186-90
28. Bowley JF, Lai WF, Surface area improvement with grooves and boxes in mandibular molar crown preparations: J Prosthet Dent, 2007; 98(6); 436-44
29. Kojic D, Singhal S, Shah S, CAD-CAM ceramic crown retention of resin cements: J Biotechnol Biomater, 2014; 4(1); 1-7
30. Roudsari RV, Satterthwaite JD, The influence of auxiliary features on the resistance form of short molars prepared for complete cast crowns: J Prosthet Dent, 2011; 106(5); 305-9
31. Tjan AH, Sarkissian R, Miller GD, Effect of multiple axial grooves on the marginal adaptation of full cast-gold crowns: J Prosthet Dent, 1981; 46(4); 399-403
32. Heintze SD, Crown pull-off test (crown retention test) to evaluate the bonding effectiveness of luting agents: Dent Mater, 2010; 26(3); 193-206
33. Graf T, Erdelt KJ, Güth JF, Influence of pre-treatment and artificial aging on the retention of 3D-printed permanent composite crowns: Biomedicines, 2022; 10(9); 2186
34. Chan DC, Wilson AH, Barbe P, Effect of preparation convergence on retention and seating discrepancy of complete veneer crowns: J Oral Rehabil, 2005; 32(1); 58-64
35. Ayad MF, Johnston WM, Rosenstiel SF, Influence of tooth preparation taper and cement type on recementation strength of complete metal crowns: J Prosthet Dent, 2009; 102(6); 354-61
36. Johnson GH, Lepe X, Patterson A, Schäfer O, Simplified cementation of lithium disilicate crowns: Retention with various adhesive resin cement combinations: J Prosthet Dent, 2018; 119(5); 826-32
37. Weed RM, A comparison of methods for increasing retention of complete veneer crowns: Int J Exp Dent Sci, 2010; 4(2); 95-98
38. Naik VA, Jurel SK, Comparative analysis of auxiliary retentive factors affecting retention of complete cast metal crown: Int J Stomat Occ Med, 2010; 3(4); 195-99
39. Veerabadhran MM, Reddy V, Nayak UA, The effect of retentive groove, sandblasting and cement type on the retentive strength of stainless steel crowns in primary second molars – an in vitro comparative study: J Indian Soc Pedod Prev Dent, 2012; 30(1); 19-26
40. Haritha J, Rao MRN, Padmaja BI, Management of short clinical crowns by utilizing horizontal groove retentive technique in crown/tooth or both with different luting cements – an analysis on extracted teeth: J Family Med Prim Care, 2020; 9(3); 1640-46
41. Gavelis JR, Morency JD, Riley ED, Sozio RB, The effect of various finish line preparations on the marginal seal and occlusal seat of full crown preparations: J Prosthet Dent, 1981; 45(2); 138-45
Figures
Figure 1. (A) 10° total occlusal convergence (taper) measured via stereomicroscope with a connected USB CCD camera. (B) 20° total occlusal convergence (taper) measured via stereomicroscope with a connected USB CCD camera. (The figure was generated using Microsoft Snip and Sketch version 10.2008.30001.0 and then compiled on MS PowerPoint, version 20H2 (OS build 19042.1466) on Windows 11 Pro, developed by Microsoft Corporation).Figure 2. Standardized resin dies after typhodont teeth preparations with 20-degree taper along with mid-buccal groove and distal proximal box. (A, B) insets showing close view of the groove and the box preparations. The photograph was captured with a Canon EOS 700D digital single-lens reflex camera equipped with a 100-mm macro lens. A ring flash may have been used, and the photograph was then compiled using MS PowerPoint, version 20H2, on Windows 11 Pro, developed by Microsoft Corporation.Figure 3. (A) Cemented definitive zirconia crowns on resin models of all groups. (B) Cemented definitive metal crowns on resin models of all groups.Figure 4. Thermocycling unit showing thermocycling of cemented metal crowns (10000 cycles between baths held at 5°C and 55°C). The image was captured using a Canon EOS 700D digital single-lens reflex camera equipped with a 100-mm macro lens, either with or without a ring flash.Figure 5. The universal testing machine demonstrates the connection of the test samples for the pull-off test, where the handles of the zirconia crowns are positioned to align with the sample handle in a perpendicular manner to the direction of the pulling force. The image was captured using a Canon EOS 700D digital single-lens reflex camera equipped with a 100-mm macro lens, either with or without a ring flash.Figure 6. Retentive force values (in newtons [N]) using post hoc least significant difference test shown via box plot.Figure 7. A comparison using the 95% confidence interval between test groups of zirconia and metal crowns in relation to pull-off force. Tables
Table 1. Description of zirconia and metal crown groups involving different preparation features in the study.Table 2. One-way analysis of variance showing inter-group comparison (in zirconia and metal crown groups) for retentive force values (in newtons).Table 3. Post hoc Fisher least significant difference test showing differences in zirconia (A) and metal crown (B) group means and multiple comparison of pull-off force values (N).Table 1. Description of zirconia and metal crown groups involving different preparation features in the study.Table 2. One-way analysis of variance showing inter-group comparison (in zirconia and metal crown groups) for retentive force values (in newtons).Table 3. Post hoc Fisher least significant difference test showing differences in zirconia (A) and metal crown (B) group means and multiple comparison of pull-off force values (N). In Press
12 Mar 2024 : Database Analysis
Risk Factors of Age-Related Macular Degeneration in a Population-Based Study: Results from SHIP-TREND-1 (St...Med Sci Monit In Press; DOI: 10.12659/MSM.943140
12 Mar 2024 : Clinical Research
Preoperative Blood Transfusion Requirements for Hemorrhoidal Severe Anemia: A Retrospective Study of 128 Pa...Med Sci Monit In Press; DOI: 10.12659/MSM.943126
12 Mar 2024 : Clinical Research
Tissue Inhibitors of Metalloproteinase 1 (TIMP-1) and 3 (TIMP-3) as New Markers of Acute Kidney Injury Afte...Med Sci Monit In Press; DOI: 10.12659/MSM.943500
12 Mar 2024 : Review article
Optimizing Behçet Uveitis Management: A Review of Personalized Immunosuppressive StrategiesMed Sci Monit In Press; DOI: 10.12659/MSM.943240
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952